
Abstract
To enhance risk stratification in patients suspected of coronary artery disease, the assessment of coronary artery calcium (CAC) could be incorporated, especially when CAC can be readily assessed on previously performed non-gated chest computed tomography (CT). Guidelines recommend reporting on patients’ extent of CAC on these non-cardiac directed exams and various studies have shown the diagnostic and prognostic value. However, this method is still little applied, and no current consensus exists in clinical practice. This review aims to point out the clinical utility of different kinds of CAC assessment on non-gated CTs. It demonstrates that these scans indeed represent a merely untapped and underestimated resource for risk stratification in patients with stable chest pain or an increased risk of cardiovascular events. To our knowledge, this is the first review to describe the clinical utility of different kinds of visual CAC evaluation on non-gated unenhanced chest CT. Various methods of CAC assessment on non-gated CT are discussed and compared in terms of diagnostic and prognostic value. Furthermore, the application of these non-gated CT scans in the general practice of cardiology is discussed. The clinical utility of coronary calcium assessed on non-gated chest CT, according to the current literature, is evident. This resource of information for cardiac risk stratification needs no specific requirements for scan protocol, and is radiation-free and cost-free. However, some gaps in research remain. In conclusion, the integration of CAC on non-gated chest CT in general cardiology should be promoted and research on this method should be encouraged.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
This study aimed to describe the clinical utility of different kinds of visual coronary artery calcium (CAC) assessment on non-gated unenhanced chest computed tomography (CT), thereby providing an overview of the currently applied methods and an interpretive consensus for the clinical practice. |
Visual CAC on non-gated chest CT can be quantified based on the presence or absence of CAC, or on the number of vessels with visible CAC. Alternatively, it can also be quantified on an ordinal scale based on features of CAC (e.g., the total extent of calcification, the exact length of the calcified parts or the extent of “blooming” of calcification). These methods need no specific imaging requirements. |
Each of these methods has been proven diagnostically accurate and strongly predictive of coronary events or mortality. In terms of clinical utility, the vessel-specific extent-based ordinal score and the simple visual score seem most optimal. |
Reporting on accidental CAC on non-gated CT allows for early identification of high-risk individuals and early initiation of preventative therapy, hereby improving patients’ cardiovascular prognosis. |
When implemented optimally, incorporation of this method in standard care could lead to a cost reduction of downstream additional non-invasive imaging and can ensure a more personalized and evidence-based approach to patient care, as high-risk individuals are readily identified and unnecessary testing in low-risk individuals is avoided. |
Introduction
Coronary artery disease (CAD) has a great impact on the general practice of cardiology, affecting 20–40% of the general population and representing 27% of the economic cardiovascular disease (CVD) burden in Europe alone [1, 2]. Therefore, an accurate and streamlined clinical evaluation of patients suspected of having CAD is paramount. Guidelines [3, 4] recommend the assessment of coronary artery calcium (CAC) on cardiac computed tomography (CT) to determine patients’ CAD burden and prognosis. This method has been proven accurate and efficient in clinically evaluating both symptomatic and asymptomatic patients [5,6,7,8,9]. Furthermore, the clinical applicability of CAC for CVD risk estimation has been validated in both young and elderly patients [10,11,12].
Recent studies have proven that CAC can be readily assessed on non-cardiac directed CT as well [13,14,15,16]. These non-gated unenhanced chest CTs have been previously performed for evaluation of non-cardiac diseases (e.g., pulmonary diseases). Guidelines recommend reporting on patients’ extent of CAC on these non-cardiac-directed exams [17, 18].
As stated earlier, the global burden of CAD is not only a health issue but an economic challenge to healthcare systems that is expected to grow exponentially in future years. Henceforth, there is a rising need for simple clinically available information on cardiac risk factors. An inexpensive radiation-free method for the assessment of patients’ CAC would fit these criteria. The clinical value of this source of freely accessible risk information could be wide-ranging, for example in optimizing patient selection for advanced imaging procedures in symptomatic patients or for cardiovascular risk estimation in asymptomatic patients.
This review aims to provide an overview of the different methods for CAC evaluation on non-gated unenhanced chest CTs and to describe their clinical utility, and ultimately to promote the integration of CAC evaluation on non-gated CT in the general practice of cardiology.
Methods
In order to describe the clinical utility of evaluating CAC on non-gated unenhanced chest CTs, we performed a scoping review.
Literature Search
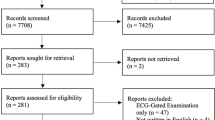
A search strategy in PubMed was implemented using terms related to “coronary calcium” and “non-gated”. Furthermore, terms related to the Medical Subject Headings (i.e., MeSH terms) “coronary artery disease”, and “thorax” were used, as depicted in Table 1. This search strategy yielded 536 articles, from which the literature applicable to our study was selected. Other studies were added using a snow-ball method to broaden the scope to determine in which aspects visual CAC assessment on non-gated chest CT could be of clinical value.
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Methods of CAC Assessment and Quantification on Non-Gated CT
Several methods of CAC quantification on non-gated chest CT have been explored.
The Agatston Score
The application of the Agatston score on routine chest CT can be limitedly generated due to the specific acquisition method. The Agatston score from cardiac-directed CT is the product of the within-slice CAC plaque area and the plaque-specific density factors (1, 2, 3, 4) summed for all slices. These density factors are based on increasing Hounsfield units (HU). To keep a strong agreement with the original Agatston score on 130-kV electron beam cardiac-directed CT, the HU threshold needs to be specifically altered when lower kV settings are applied [19]. Furthermore, studies have found that slice thickness > 3 mm can seemingly underestimate the total CAC score [20]. These features appear to be an inherent limitation of all Agatston scoring software systems [21] and form a problem on non-cardiac CT with often varying kV settings and slice thickness. In addition, specific software is required to compute the Agatston score, which not every physician can easily access.
Visual Assessment
Further quantification methods are visually performed. This can be simply based on the presence or absence of CAC, or on the number of vessels with visible CAC [22]. Alternatively, CAC can also be quantified on an ordinal scale based on features of CAC (e.g., the total extent of calcification, the exact length of the calcified parts or the extent of “blooming” of calcification). On coronary CT angiography (CCTA), calcifications can cause an illuminated white blurriness, which complicates grading the degree of occlusion of the coronary lumen. This is called “blooming”, a partial volume artifact caused by limited spatial resolution of CT scanners and complicates delineating the edges of high-density objects (i.e., bone or calcification) [23].
The Diagnostic and Prognostic Value of Visual CAC Quantification on Non-Gated CT
We evaluated the diagnostic and prognostic performance of the different CAC quantification methods on non-gated chest CT in CAD mentioned above. These methods are depicted in Figs. 1, 2, 3, and 4. Table 2 and Fig. 5 present an overview of these methods in terms of accuracy, intra-and interobserver agreement, and time efficiency.

The Total Visual Score and length based score as methods for visual CAC assessment. A The Total Visual Score for visual CAC assessment. B The length-based method for CAC assessment. LCA left coronary artery, LCx left circumflex, mm millimeters, RCA right coronary artery, LM left main, LAD left anterior descending

The Weston score for visual CAC assessment. LAD left anterior descending, LCx left circumflex, LM left main, mm millimeters, RCA right coronary artery, CAC coronary artery calcium

The segment-specific extent-based method for visual CAC assessment. A Qualitative type of the segment-specific extent-based method for visual CAC assessment. B Semi-quantitative type of the segment-specific extent-based method for visual CAC assessment. LAD left anterior descending, LCx left circumflex, LM left main, mm millimeters, RCA right coronary artery, CAC coronary artery calcium

Vessel-specific extent-based method of visual CAC assessment. LAD left anterior descending, LCx left circumflex, LM left main, mm millimeter, RCA right coronary artery, CAC coronary artery calcium

Overview of agreement, correlation, and evaluation time of different methods for visual CAC quantification. A Interobserver agreement with kappa-statistics. B Correlation with the Agatston score on gated cardiac CT. C Evaluation time for CAC quantification on non-gated CT, in seconds. CAC coronary artery calcium, TVS Total Visual Score, CT computed tomography
The Total Visual Score (TVS) and Length-Based Methods
The most exact and least subjective methods are the Total Visual Score (TVS) and length-based methods (Fig. 1), as they measure the exact length of CAC in mm [24,25,26]. Therefore, the intra-and interobserver agreement of these methods is excellent. For the length-based method, the interobserver agreement ranged from 0.80 to 0.90 and the intra-observer agreement ranged from 0.80 to 0.92 [25, 26]. For TVS, the interobserver agreement ranged from 0.80 to 0.92 [24]. In terms of prognosis, TVS could accurately predict all-cause mortality (odds ratio (OR) 1.3, 95% confidence interval (CI) 1.3–1.8, p < 0.001) and CVD mortality (OR 1.8, 95% CI 1.5–2.1, p < 0.001). Huang et al. [26] reported a negative predictive value of 98% for the absence of CAC and a positive predictive value of 98% for the presence of CAC with the length-based method. The sensitivity and specificity were resp. 92% and 98%. The downside of these methods is that they are relatively time-consuming compared to simpler and equally accurate methods (i.e., the vessel-specific extent-based method) [24] and less readily applied requiring multiple measurements.
The Weston Score
Another way to quantify patients’ CAC is to assess the extent of blooming, i.e., the Weston score (Fig. 2). When compared to the Agatston score on cardiac-directed CT, this method could determine patients’ CAC burden equally well (correlation, R = 0.81, p < 0.001) [27]. Furthermore, the Weston score showed a similar trend to the Kaplan–Meier curves for coronary event-free survival as the Agatston score [28]. Although this method has proven accurate in quantifying patients’ CAC and predictive of coronary events, it is relatively subjective and challenging for physicians untrained in this particular skill.
Segment-Specific Extent-Based Scores
This method comments on the extent of patients’ CAC based on the number of segments involved of the entire coronary tree, divided into either 9 or 27 segments (Fig. 3). This method of CAC quantification and localization is found to be less time-efficient compared to simpler methods. Suh et al. [29] reported that segment-specific CAC assessment was the most time-consuming and had an inferior interobserver agreement. Possibly, this method is found to be too detailed to be applied in the general population with natural variations of the coronary tree.
Vessel-Specific Extent-Based Score
The most extensively researched method of visual CAC quantification is the vessel-specific extent-based score (Fig. 4), which reports on the number of vessels involved [13,14,15,16, 21, 24, 25, 29,30,31,32]. According to expert consensus [33], reporting on the number of vessels involved is key information when analyzing patients’ CAC. Furthermore, literature describes this as the most time-efficient method of CAC quantification with a good interobserver agreement ranging from 0.70 to 0.97 [25, 29, 31]. Three studies reported an excellent sensitivity of 100% and a specificity of 100% [14, 21, 31]. When compared with the classic Agatston score, this method has shown a similar significant relationship between CAC score and odds of cardiovascular death [13, 30]. An increase in risk for CVD events of 25% was seen per 1 standard deviation (SD) increase of the vessel-specific CAC score, the risk for coronary events increased with 42% per 1 SD. Shemesh et al. [15] found that the vessel-specific ordinal CAC score of CAC ≥ 4 (i.e., severe calcification) was a significant predictor of CVD death with OR = 2.1 (p = 0.0002). A more recent study [34] reported a 2.9-fold increased risk of myocardial infarction, a 3.7-fold increased risk of stroke, and a 1.8-fold risk of all-cause mortality with severe CAC (i.e., CAC ≥ 4).
Simple Visual Score
Sensibly, the most readily applied and least time-consuming method is the simple visual score, which comments on the presence (or absence) of CAC. CAC severity is not quantified on an ordinal score, but based on clinical judgment. This method is the most subjective with a low interobserver agreement of only 0.50 [29]. Still, a study containing 410 patients with a chest CT as follow-up on long-nodules concluded that simply commenting on either the presence of CAC or on the number of arteries with CAC was of equal prognostic value as the Agatston score. The reported sensitivity was 100% and specificity was 93%. The c-statistics of the multivariable Kaplan–Meier Models were 0.80 vs. 0.81, respectively [22]. Chiles et al. [16] aimed to validate risk assessment with CAC quantification on non-gated chest CT for cardiac death and all-cause mortality in asymptomatic patients, incorporating several methods. The simple visual score was strongly associated with both cardiac death and all-cause mortality and demonstrated an increased risk of events with an increase in the CAC-severity category.
Coronary Artery Calcium Data and Reporting System (CAC-DRS)
To determine the prognosis of patients and adjust medical treatment, the Coronary Artery Calcium Data and Reporting System (CAC-DRS) is recommended [33]. Society of Cardiovascular Computed Tomography (SCCT) guidelines recommend this form of standardized reporting, as it highlights key imaging features (number of vessels involved) associated with increased patient risk.
Each method of visual CAC assessment described in this paragraph has proven to be diagnostically accurate and strongly predictive of coronary events or mortality. However, when comparing these methods in terms of clinical utility, the vessel-specific extent-based ordinal score and the simple visual score seem most optimal. These methods are most readily applied and both demonstrate a strong correlation and good agreement with the clinically validated Agatston score on electrocardiogram (ECG)-gated CT, as described in Table 2.
Imaging Requirements for Accurate CAC Assessment on Non-Gated CT
In terms of imaging requirements, different acquisition protocols for CAC quantification on non-gated chest CT have been explored. The first is the variating radiation dose of non-gated scans. CAC assessed on low-dose CT scans (1.5–2.57 mSv), ultra-low-dose CT scans (0.24 mSv), and standard-dose CTs (3.4–3.8 mSv) have shown an equally strong correlation with the classic Agatston score and were all strongly associated with CVD death and all-cause mortality [16, 31].
Another variating imaging feature is the slice thickness. In studies on ordinal calcium scoring, a great variety of slice thicknesses has been evaluated ranging from 1.25 to 6 mm, each proving diagnostically accurate [25, 30, 35].
Lastly, the admission of contrast variates with different non-gated CT protocols. A study by Fresno et al. [36] evaluated the accuracy of CAC assessment on both contrast-enhanced and non-contrast-enhanced non-gated CT as compared to the classic Agatston score. They reported a high sensitivity (89%) and even higher specificity (100%) for both scans. CAC on both scans was significantly associated with major adverse cardiovascular events (MACE). However, CAC severity was more often underestimated on contrast-enhanced CT versus non-contrast enhanced CT (41% vs. 26%, respectively). As contrast administration highlights the vessel lumen, the distinction between contrast and low-density calcifications could be complicated.
In terms of clinical utility, each type of radiation dose CT can be applied, each slice thickness, and both contrast-enhanced and non-contrast-enhanced CT have been found sufficient for the quantification of CAC.
CAC on Non-Gated CT in Asymptomatic and Symptomatic Patients
The clinical implication and value of CAC assessment is different in asymptomatic and symptomatic patients. In asymptomatic patients, CAC assessment on non-gated CT can be applied for cardiovascular risk management. Previous studies have demonstrated that evaluation of CAC on non-gated CT in asymptomatic patients can determine patients prognosis equally well as CAC on cardiac CT [16, 22, 24, 30]. For example, Blair et al. [30] performed a case–control study in 228 community-living individuals. Patients who died due to cardiovascular disease (n = 57) formed the cases and were matched 1:3 with 171 controls. They demonstrated a similar hazard ratio (HR) of CVD mortality for CAC on non-gated CT as on cardiac CT, respectively 1.57 (p = 0.05) vs. 1.66 (p = 0.04). Conversely, in CT in 410 patients who were evaluated for lung diseases, the absence of CAC on non-gated performed as a strong negative predictor of events [22]. The event-free survival of patients with CAC 0 on non-gated CT was similar to patients with CAC 0 on cardiac CT (96.1% and 95.9%, respectively).
In addition, CAC burden in asymptomatic patients is a more patient-specific risk indicator than cardiac risk factors (e.g., hypertension, diabetes). For example, a study amongst 740 hospital inpatients [37] demonstrated that CAC on non-gated CT was associated with a high hazard ratio for MACE, e.g., myocardial infarction of HR 6.0 (CI 13.7–9.7, p < 0.001). Even when adjusted for classic cardiovascular risk factors, the hazard ratio remained high, HR 3.2 (CI 1.8–5.6, p < 0.001). Additionally, Graby et al. [34] demonstrated that CAC alone had the highest HR for myocardial infarction compared to classic cardiovascular risk factors, CAC HR 8.6 (CI 4.6–16.2, p < 0.01) vs. diabetes HR 1.7 (CI 1.0–3.0, p = 0.04) and hypertension HR 2.8 (CI 1.9–4.2, p < 0.01).
Another important factor of CAC evaluation on non-gated CT in asymptomatic patients is the early identification of (severe) CAC. In terms of prognosis, this allows for early intervention with preventative therapy and early risk modification, thereby improving patients’ cardiovascular prognosis.
In symptomatic patients, CAC assessment on non-gated CT could generally be applied to rule out or diagnose CAD; unfortunately, studies have yet to explore this possibility.
Differences in CAC on Non-Gated CT Between Sexes and Age Strata
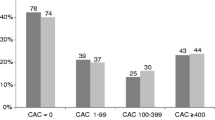
The extent and prevalence of CAC differs between male and female patients [38]. This could be explained by the difference in atherosclerotic plaque development [39]. On non-gated CT, the difference in CAC between sexes has been demonstrated by Shemesh et al. [15, 40]. They reported a constant higher prevalence of CAC and higher mean CAC score for men than women in the same age strata. Thus female patients have a generally lower CAC prevalence as male patients in the same age strata. Despite the difference in prevalence, the risk for cardiovascular death increases with rising CAC score in both women and men [15].
The prevalence of CAC variates between patients of different age strata as well. Graby et al. demonstrated an increasing CAC prevalence with older age (p < 0.001), ranging from 3% in patients < 40 years and 94% in patients ≥ 90 years old. Due to the demonstrated difference of CAC prevalence in age groups, the clinical value of CAC assessment in the young is questioned. Although CAC prevalence is low in younger individuals, the presence of CAC is associated with a severely increased risk of cardiovascular events [11]. Therefore, reporting on CAC on non-cardiac directed scans could identify patients at increased risk much earlier. Graby et al. [34] investigated the number needed to report for patients to benefit from a change in clinical management. They reported that the number needed to report accidental CAC on non-gated CT is only two in patients of < 40 years old.
CAC on Non-Gated CT as a Gatekeeper to Tailor Downstream Additional Imaging
The performance of additional non-invasive imaging in patients with stable chest pain is based on their pre-test likelihood of having obstructive CAD. Patients’ pre-test likelihood is estimated based on risk factors, age, sex type of complaints, or ECG abnormalities. These risk models have been proven to be very sensitive [41]; however, they appear to often overestimate patients’ risk of obstructive CAD [42]. This study by Rijlaarsdam et al. compared the National Institute for Health and Care Excellence (NICE) guidelines and the 2019 European Society of Cardiology (ESC) guidelines for diagnosing suspected stable angina. They reported that the majority of patients with an intermediate—high risk did not have obstructive coronary artery disease, respectively, 81% and 79%. The overestimation of patients’ actual risk of obstructive CAD leads to an over-performance of additional noninvasive imaging. With the current economic burden on healthcare systems, an extra tool to filter these patients more specifically would be desirable.
CAC on cardiac CT has played an evident role in patient-specific risk reclassification [42,43,44]. Recently, CAC on non-gated CT has been proven accurate and valuable as well [45]. As these scans were performed previous to patients CAD evaluation, this information would be available at the earliest convenience. An exploratory study by Chi et al. [14] reported that these scans are available in > 10% of patients who are evaluated for having coronary artery disease. Possibly, this tool could prove efficient in streamlining or tailoring downstream non-invasive imaging in patients with stable chest pain.
The Clinical Value of CAC on Non-Gated CT on Lifestyle Modification
An important aspect of coronary artery disease is the necessity of lifestyle- and risk-factor modification to prevent (re-)occurrence of events (e.g., myocardial infarction). Unfortunately, warranted lifestyle modifications are often not realized. Interestingly, CAC on non-gated CT could provide a solution. Patients’ CAD burden is easily visualized by the extent of coronary artery calcifications. In patients with a previously performed non-gated CT, this information would be available at the earliest consultation of a cardiologist or even general physician. Previous studies on CAC on cardiac CT have demonstrated that patients’ knowledge of their calcium score correlates with improved adherence and more effective lifestyle modification [46, 47]. This has yet to be proven with non-gated CT, though the effect would probably be the same.
The Clinical Value of CAC on Non-Gated CT on Medical Therapy
It would be interesting to evaluate the health benefit and clinical impact on therapy of reporting on accidental CAC on non-cardiac directed scans. If reported, primary prevention could be initiated in an early (subclinical) phase of patients’ coronary artery disease. The recent NOTIFY-1 (Incidental Coronary Calcification Quality Improvement Project) trial [48] explored this possibility in 173 patients who had a non-gated CT on which coronary artery calcium was observed. Patients were randomized to either the notification arm or standard-of-care arm. In the patients who were notified about their calcium score (n = 86), preventative therapy was significantly more initiated than in patients with standard care. As a result, low-density lipoprotein cholesterol levels were significantly lower in the notification arm as compared to the standard-of-care arm, respectively, 97.2 vs. 115.3 mg/dl (P = 0.005). For future perspectives, long-term follow-up and overall event-free survival of the notified patients could prove interesting.
Patients’ CAC burden has proven to be a more patient-specific indicator for medical therapy than risk factors. Phillips et al. demonstrated this in a population of 256 patients with breast cancer. These patients had an increased risk of CAD and by extension cardiovascular events. According to Phillips et al. [32], the vessel-specific ordinal score on non-gated CT reclassified 7% of patients with a low risk (according to risk factors), in a higher-risk category and identified them as patients who would benefit from statin therapy. The Risk Or Benefit IN Screening for CArdiovascular Diseases (ROBINSCA) trial [49] has demonstrated this for CAC on cardiac CT. Conversely, the absence of CAC in patients with risk-enhancing factors (e.g., diabetes or elevated levels of lipoprotein(a)) was associated with lower absolute event rates [50]. Therefore, despite risk-enhancing factors, statin therapy would not be indicated.
Noteworthy, statin therapy has shown to increase calcification of coronary plaques, i.e., the calcium density [51, 52]. Therefore, when preventative therapy and effective risk-factor treatment is initiated, the extent of patients CAC can increase while patients’ cardiovascular event risk decreases. This forms a problem with the performance of the Agatston score on cardiac CT, and physicians should keep this in mind when evaluating patients’ CAC. Possibly, the visual CAC assessment methods on non-gated CT are less affected by the increased density of calcification due to statin therapy, as these methods do not incorporate the density in their quantification (except for the Weston score).
Cost-Effectiveness of CAC Assessment on Non-Gated CT
With the current economic strain on health care systems, an inexpensive method for CAC evaluation for clinical decision-making would seem desirable. CAC assessment on these non-cardiac directed scans has been proven efficient in diagnosis and prognosis of CAD. The question remains whether this would be cost-effective as well. Imaginably, the incorporation of this method in standard care would not generate any extra costs. In addition, expenses could be spared when the performance of additional non-invasive testing is withheld in the absence of CAC. Gomes et al. [53] investigated the cost-effectiveness of CAC-guide strategy on cardiac CT in patients up for CAD evaluation. They concluded that CAC could form a gatekeeper for additional non-invasive imaging (i.e., CCTA) if society would be willing to pay €2172 for an additional correct diagnosis, in which case the use of CCTA would decrease by 50%. For future perspectives, a likewise evaluation for CAC on non-cardiac CT would be interesting.
CAC on Non-Gated CT in Patients with Cancer
As mentioned earlier, patients with cancer are evidently at risk for cardiovascular events. Data are plentiful on CVD in patients with cancer due to cardiotoxicity of several treatments [54] or synergistic risk factors for both cancer and CVD [55]. Furthermore, due to improved cancer therapies, patients have an increased survival. Simultaneously, they have an increased possibility of experiencing MACE based on delayed side effects of their cancer treatments. Armenian et al. [56] reported a significantly worse all-cause mortality of patients with cancer with CVD than patients with cancer without CVD and recommended early cardiovascular risk assessment in cancer survivors. For these reasons, patients with cancer would benefit from early cardiac screening and surveillance. In this population, non-gated CTs are often performed for cancer surveillance and disease follow-up (e.g., breast and lung cancer).
Guidelines [17, 18] advise the use of these scans for CAC assessment and the incorporation of this method for early CAD identification and risk estimation for prognosis. Several studies [16, 24, 29, 57] have explored the clinical utility of CAC assessment on these non-cardiac-directed scans. A recent multicenter trial, the ITALUNG trial [57], demonstrated that moderate-to-severe calcifications on non-gated CT were significantly associated with cardiovascular mortality in 1364 patients with lung cancer. Patients had a median follow-up of 11.4 (10.9–11.9) years and CAC was assessed visually and categorized as none, mild, moderate, or severe. CVD mortality increased significantly per CAC severity category (p = 0.015). Earlier, Chiles et al. [16] reported similar results in 1442 patients of the National Lung Screening Trial (NSLT), incorporating the extent-based vessel-specific score.
Automated Coronary Calcium Quantification on Non-Gated Chest CT
A possible future method of coronary calcium quantification is the direct or automatic quantification of CAC through artificial intelligence (AI). Several studies have explored a variety of techniques developed for this method of CAC quantification [58,59,60]. Although this development is most exciting for radiology and AI, the clinical utility in the general practice of cardiology is yet debatable, as simple visual estimation has already been proven accurate in determining CAD burden and patients’ prognosis.
Discussion
To our knowledge, this is the first review to describe the clinical utility of different kinds of visual CAC assessment on non-gated unenhanced chest CT. Although several studies have demonstrated the evident diagnostic and prognostic value, no current interpretive consensus exists in clinical practice. According to the literature on CAC evaluation on non-gated (i.e., non-cardiac) CT, each method has been proven diagnostically accurate and prognostically efficient. In our perspective, the simple visual score and the vessel-specific extent-based score are most readily applied (< 1 min), while remaining diagnostically and prognostically accurate. These methods would therefore be preferred to more detailed methods. CAC on non-gated CT has predominantly been investigated in asymptomatic populations and is equally efficient in both male and female patients. Reporting on accidental CAC on non-gated scans appears to have a clinical impact on therapy tailoring and initiation. In addition, this diagnostic tool plays a role in the contrast between low-risk and high-risk markers for coronary artery disease and the impact of different medical approaches. Low-risk markers, which are widespread, are the focus of preventive practitioners and public health measures due to their potential for significant survival improvement at a lower cost. Unfortunately, the medical profession tends to concentrate on high-risk markers, which appear to have a relatively low prevalence. This leads to unnecessary testing, high costs, and limited survival benefits for most patients. Calcium scoring is positioned in between the above-mentioned approaches. When implemented optimally, CAC can identify high-risk individuals while avoiding unnecessary tests and ensuring a more personalized and evidence-based approach to patient care. Finally, CAC on non-gated CT is especially clinically valuable for cardiac screening and surveillance in patients with cancer, as the prevalence of CAD and by extension the risk of cardiovascular events (e.g., myocardial infarction) increases in this population. This can be explained by the increasing survival of these patients with a simultaneous increase in adverse delayed side effects of their cancer treatments. In addition, in this specific population, non-gated CTs are often performed as a follow-up in patients with cancer.
Despite the above-mentioned evidence reported on the clinical utility of CAC evaluation on non-gated CT, a gap in research remains. For future perspectives, studies on the following subjects could prove valuable.
Firstly, the diagnostic power of CAC on non-gated CT for risk reclassification (i.e., negative predictive power, specificity, and sensitivity) and tailoring of downstream non-invasive imaging in symptomatic patients could be investigated. As optimization of this diagnostic tool and incorporation of this method in standard care could lead to cost reduction of downstream additional non-invasive imaging, as unnecessary testing is avoided and patient care is more personalized and evidence-based.
With the use of previously performed scans the clinical warranty of this information is questioned. For CAC on non-gated CT, this has yet to be determined. The warranty of the Agatston score on cardiac CT, however, has been extensively described [61,62,63]. Depending on age, sex, ethnicity, and risk factors, the warranty of CAC 0 on cardiac CT would be between 3 and 7 years. Still, Dzaye et al. [64] showed that it took 10 years before 15% of the population had CAC 0 converted to CAC > 100. Arguably, the warranty of CAC on non-gated CT would be similar to CAC on cardiac CT, as both methods are of equal prognostic value and describe the same feature of coronary atherosclerosis, i.e., calcification.
The biggest theoretical argument against performing CAC assessment as a risk classifier is the inability to identify “soft plaque” or “low-attenuation plaque”. Recent studies have identified this feature of patients’ plaque as a high-risk feature for myocardial infarction. However, what becomes clear from the extensive literature on plaque quantification is that the total “CAD burden” is eventually most defining of patients’ risk for events. Stone et al. showed that total plaque burden ≥ 70% gave the highest hazard ratio of 5.03 (p < 0.001) vs. 3.35 (p < 0.001) thin-cap atheroma. According to the Scottish Computed Tomography of the Heart (SCOTHEART) trial by Williams et al. [65], the “low-attenuation plaque burden” is the strongest predictor of fatal or nonfatal myocardial infarction. However, in their study, the median total plaque burden in patients with CAC 0–99 appeared to be 0%. Furthermore, the median CAC score in patients without myocardial infarction was 0 and the median CAC score in patients with myocardial infarction was > 0.
It should be noted that any kind of plaque burden was associated with an increased risk of cardiac events. Possibly, when looking specifically at patients with a high total plaque burden, the noncalcified feature is a higher-risk marker. However, for risk stratification of the vast majority of low-risk patients with stable chest pain, a rough estimate of disease burden is well above the mark. A study by Senoner et al. [66] reported that 26% of patients with a calcium score of 0 showed CAD on CCTA, with only 0.5% experiencing MACE, suggesting that for risk classification, non-calcified plaque might not be so worrisome.
Conclusions
To our knowledge, this is the first review to describe the clinical utility of different kinds of visual CAC assessment on non-gated unenhanced chest CT. We have observed an evident clinical utility of coronary calcium assessed on non-gated chest CT. This merely untapped resource for cardiac risk information needs no specific requirements for scan protocol, is radiation-free, and cost-free. In conclusion, the integration of CAC on non-gated chest CT for clinical evaluation of patients in the general practice of cardiology should be promoted. Still, further research on the clinical utility is warranted and should be encouraged.
Data Availability
As this is a scoping review, data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
References
Timmis A, Townsend N, Gale CP, Torbica A, Lettino M, Petersen SE, Mossialos EA, Maggioni AP, Kazakiewicz D, May HT, De Smedt D, Flather M, Zuhlke L, Beltrame JF, Huculeci R, Tavazzi L, Hindricks G, Bax J, Casadei B, Achenbach S, Wright L, Vardas P. European Society of Cardiology: cardiovascular disease statistics 2019. Eur Heart J. 2020;41:12–85.
Timmis A, Vardas P, Townsend N, Torbica A, Katus H, De Smedt D, Gale CP, Maggioni AP, Petersen SE, Huculeci R, Kazakiewicz D, de Benito RV, Ignatiuk B, Raisi-Estabragh Z, Pawlak A, Karagiannidis E, Treskes R, Gaita D, Beltrame JF, McConnachie A, Bardinet I, Graham I, Flather M, Elliott P, Mossialos EA, Weidinger F, Achenbach S. European Society of Cardiology: cardiovascular disease statistics 2021. Eur Heart J. 2022;43:716–99.
Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK, Blankstein R, Boyd J, Bullock-Palmer RP, Conejo T, Diercks DB, Gentile F, Greenwood JP, Hess EP, Hollenberg SM, Jaber WA, Jneid H, Joglar JA, Morrow DA, O’Connor RE, Ross MA, Shaw LJ. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation. 2021;144:e368–454.
Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, Prescott E, Storey RF, Deaton C, Cuisset T, Agewall S, Dickstein K, Edvardsen T, Escaned J, Gersh BJ, Svitil P, Gilard M, Hasdai D, Hatala R, Mahfoud F, Masip J, Muneretto C, Valgimigli M, Achenbach S, Bax JJ. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41:407–77.
Budoff MJ, Mayrhofer T, Ferencik M, Bittner D, Lee KL, Lu MT, Coles A, Jang J, Krishnam M, Douglas PS, Hoffmann U. Prognostic value of coronary artery calcium in the PROMISE study (prospective multicenter imaging study for evaluation of chest pain). Circulation. 2017;136:1993–2005.
Agha AM, Pacor J, Grandhi GR, Mszar R, Khan SU, Parikh R, Agrawal T, Burt J, Blankstein R, Blaha MJ, Shaw LJ, Al-Mallah MH, Brackett A, Cainzos-Achirica M, Miller EJ, Nasir K. The prognostic value of CAC zero among individuals presenting with chest pain: a meta-analysis. JACC Cardiovasc Imaging. 2022;15:1745–57.
Blaha M, Budoff MJ, Shaw LJ, Khosa F, Rumberger JA, Berman D, Callister T, Raggi P, Blumenthal RS, Nasir K. Absence of coronary artery calcification and all-cause mortality. JACC Cardiovasc Imaging. 2009;2:692–700.
Blaha MJ, Cainzos-Achirica M, Dardari Z, Blankstein R, Shaw LJ, Rozanski A, Rumberger JA, Dzaye O, Michos ED, Berman DS, Budoff MJ, Miedema MD, Blumenthal RS, Nasir K. All-cause and cause-specific mortality in individuals with zero and minimal coronary artery calcium: a long-term, competing risk analysis in the Coronary Artery Calcium Consortium. Atherosclerosis. 2020;294:72–9.
Rijlaarsdam-Hermsen D, Lo-Kioeng-Shioe MS, Kuijpers D, van Domburg RT, Deckers JW, van Dijkman PRM. Prognostic value of the coronary artery calcium score in suspected coronary artery disease: a study of 644 symptomatic patients. Neth Heart J. 2020;28:44–50.
Paixao AR, Ayers CR, El Sabbagh A, Sanghavi M, Berry JD, Rohatgi A, Kumbhani DJ, McGuire DK, Das SR, de Lemos JA, Khera A. Coronary artery calcium improves risk classification in younger populations. JACC Cardiovasc Imaging. 2015;8:1285–93.
Osei AD, Uddin SMI, Dzaye O, Achirica MC, Dardari ZA, Obisesan OH, Kianoush S, Mirbolouk M, Orimoloye OA, Shaw L, Rumberger JA, Berman D, Rozanski A, Miedema MD, Budoff MJ, Vasan RS, Nasir K, Blaha MJ. Predictors of coronary artery calcium among 20–30-year-olds: the coronary artery calcium consortium. Atherosclerosis. 2020;301:65–8.
Vliegenthart R, Oudkerk M, Hofman A, Oei HH, van Dijck W, van Rooij FJ, Witteman JC. Coronary calcification improves cardiovascular risk prediction in the elderly. Circulation. 2005;112:572–7.
Azour L, Kadoch MA, Ward TJ, Eber CD, Jacobi AH. Estimation of cardiovascular risk on routine chest CT: ordinal coronary artery calcium scoring as an accurate predictor of Agatston score ranges. J Cardiovasc Comput Tomogr. 2017;11:8–15.
Chi JM, Makaryus JN, Rahmani N, Shah AB, Shah RD, Cohen SL. Coronary CT calcium score in patients with prior nongated CT, is it necessary? Curr Probl Diagn Radiol. 2021;50:54–8.
Shemesh J, Henschke CI, Shaham D, Yip R, Farooqi AO, Cham MD, McCauley DI, Chen M, Smith JP, Libby DM, Pasmantier MW, Yankelevitz DF. Ordinal scoring of coronary artery calcifications on low-dose CT scans of the chest is predictive of death from cardiovascular disease. Radiology. 2010;257:541–8.
Chiles C, Duan F, Gladish GW, Ravenel JG, Baginski SG, Snyder BS, DeMello S, Desjardins SS, Munden RF. Association of coronary artery calcification and mortality in the national lung screening trial: a comparison of three scoring methods. Radiology. 2015;276:82–90.
Hecht HS, Cronin P, Blaha MJ, Budoff MJ, Kazerooni EA, Narula J, Yankelevitz D, Abbara S. 2016 SCCT/STR guidelines for coronary artery calcium scoring of noncontrast noncardiac chest CT scans: a report of the Society of Cardiovascular Computed Tomography and Society of Thoracic Radiology. J Cardiovasc Comput Tomogr. 2017;11:74–84.
Lopez-Mattei J, Yang EH, Baldassarre LA, Agha A, Blankstein R, Choi AD, Chen MY, Meyersohn N, Daly R, Slim A, Rochitte C, Blaha M, Whelton S, Dzaye O, Dent S, Milgrom S, Ky B, Iliescu C, Mamas MA, Ferencik M. Cardiac computed tomographic imaging in cardio-oncology: an expert consensus document of the Society of Cardiovascular Computed Tomography (SCCT). Endorsed by the International Cardio-Oncology Society (ICOS). J Cardiovasc Comput Tomogr. 2023;17:66–83.
Baron KB, Choi AD, Chen MY. Low radiation dose calcium scoring: evidence and techniques. Curr Cardiovasc Imaging Rep. 2016;9:12.
Hughes-Austin JM, Dominguez A 3rd, Allison MA, Wassel CL, Rifkin DE, Morgan CG, Daniels MR, Ikram U, Knox JB, Wright CM, Criqui MH, Ix JH. Relationship of coronary calcium on standard chest CT scans with mortality. JACC Cardiovasc Imaging. 2016;9:152–9.
Htwe Y, Cham MD, Henschke CI, Hecht H, Shemesh J, Liang M, Tang W, Jirapatnakul A, Yip R, Yankelevitz DF. Coronary artery calcification on low-dose computed tomography: comparison of Agatston and Ordinal Scores. Clin Imaging. 2015;39:799–802.
Shao L, Yan AT, Lebovic G, Wong HH, Kirpalani A, Deva DP. Prognostic value of visually detected coronary artery calcification on unenhanced non-gated thoracic computed tomography for prediction of non-fatal myocardial infarction and all-cause mortality. J Cardiovasc Comput Tomogr. 2017;11:196–202.
Pack JD, Xu M, Wang G, Baskaran L, Min J, De Man B. Cardiac CT blooming artifacts: clinical significance, root causes and potential solutions. Vis Comput Ind Biomed Art. 2022;5:29.
Watts JR Jr, Sonavane SK, Snell-Bergeon J, Nath H. Visual scoring of coronary artery calcification in lung cancer screening computed tomography: association with all-cause and cardiovascular mortality risk. Coron Artery Dis. 2015;26:157–62.
Lee S, Suh YJ, Nam K, Lee K, Lee HJ, Choi BW. Comparison of artery-based methods for ordinal grading of coronary artery calcium on low-dose chest computed tomography. Eur Radiol. 2021;31:8108–15.
Huang YL, Wu FZ, Wang YC, Ju YJ, Mar GY, Chuo CC, Lin HS, Wu MT. Reliable categorisation of visual scoring of coronary artery calcification on low-dose CT for lung cancer screening: validation with the standard Agatston score. Eur Radiol. 2013;23:1226–33.
Kirsch J, Buitrago I, Mohammed TL, Gao T, Asher CR, Novaro GM. Detection of coronary calcium during standard chest computed tomography correlates with multi-detector computed tomography coronary artery calcium score. Int J Cardiovasc Imaging. 2012;28:1249–56.
Bhatt SP, Kazerooni EA, Newell JD Jr, Hokanson JE, Budoff MJ, Dass CA, Martinez CH, Bodduluri S, Jacobson FL, Yen A, Dransfield MT, Fuhrman C, Nath H. Visual estimate of coronary artery calcium predicts cardiovascular disease in COPD. Chest. 2018;154:579–87.
Suh YJ, Lee JW, Shin SY, Goo JM, Kim Y, Yong HS. Coronary artery calcium severity grading on non-ECG-gated low-dose chest computed tomography: a multiple-observer study in a nationwide lung cancer screening registry. Eur Radiol. 2020;30:3684–91.
Blair KJ, Allison MA, Morgan C, Wassel CL, Rifkin DE, Wright CM, Criqui MH, Ix JH. Comparison of ordinal versus Agatston coronary calcification scoring for cardiovascular disease mortality in community-living individuals. Int J Cardiovasc Imaging. 2014;30:813–8.
Messerli M, Hechelhammer L, Leschka S, Warschkow R, Wildermuth S, Bauer RW. Coronary risk assessment at X-ray dose equivalent ungated chest CT: results of a multi-reader study. Clin Imaging. 2018;49:73–9.
Phillips WJ, Johnson C, Law A, Turek M, Small AR, Dent S, Ruddy TD, Beanlands RS, Chow BJW, Small GR. Comparison of Framingham risk score and chest-CT identified coronary artery calcification in breast cancer patients to predict cardiovascular events. Int J Cardiol. 2019;289:138–43.
Hecht HS, Blaha MJ, Kazerooni EA, Cury RC, Budoff M, Leipsic J, Shaw L. CAC-DRS: coronary artery calcium data and reporting system. An expert consensus document of the Society of Cardiovascular Computed Tomography (SCCT). J Cardiovasc Comput Tomogr. 2018;12:185–91.
Graby J, Soto-Hernaez J, Murphy D, Oldman J, Burnett TA, Charters PFP, Barrishi A, Thanaraaj T, Masterman BJ, Khavandi A, Rodrigues JCL. Coronary artery calcification on routine CT has prognostic and treatment implications for all ages. Clin Radiol. 2023;78:412–20.
Xia C, Vonder M, Pelgrim GJ, Rook M, Xie X, Alsurayhi A, van Ooijen PMA, van Bolhuis JN, Oudkerk M, Dorrius M, van der Harst P, Vliegenthart R. High-pitch dual-source CT for coronary artery calcium scoring: a head-to-head comparison of non-triggered chest versus triggered cardiac acquisition. J Cardiovasc Comput Tomogr. 2021;15:65–72.
Fresno CU, Tijmes FS, Thavendiranathan P, Akhtari S, Karur GR, Torres FS, Halankar J, Nguyen ET, Hanneman K. Visual ordinal scoring of coronary artery calcium on contrast-enhanced and non-contrast chest CT: a retrospective study of diagnostic performance and prognostic utility. AJR Am J Roentgenol. 2022;219:569–78.
Yu C, Ng ACC, Ridley L, Anjaria M, Meier S, Yiannikas J, Kritharides L, Naoum C. Incidentally identified coronary artery calcium on non-contrast CT scan of the chest predicts major adverse cardiac events among hospital inpatients. Open Heart. 2021;8: e001695.
Shaw LJ, Min JK, Nasir K, Xie JX, Berman DS, Miedema MD, Whelton SP, Dardari ZA, Rozanski A, Rumberger J, Bairey Merz CN, Al-Mallah MH, Budoff MJ, Blaha MJ. Sex differences in calcified plaque and long-term cardiovascular mortality: observations from the CAC Consortium. Eur Heart J. 2018;39:3727–35.
van Rosendael SE, Bax AM, Lin FY, Achenbach S, Andreini D, Budoff MJ, Cademartiri F, Callister TQ, Chinnaiyan K, Chow BJW, Cury RC, DeLago AJ, Feuchtner G, Hadamitzky M, Hausleiter J, Kaufmann PA, Kim YJ, Leipsic JA, Maffei E, Marques H, de Araújo Gonçalves P, Pontone G, Raff GL, Rubinshtein R, Villines TC, Chang HJ, Berman DS, Min JK, Bax JJ, Shaw LJ, van Rosendael AR. Sex and age-specific interactions of coronary atherosclerotic plaque onset and prognosis from coronary computed tomography. Eur Heart J Cardiovasc Imaging 2023;24(9):1180–1189
Shemesh J, Henschke CI, Farooqi A, Yip R, Yankelevitz DF, Shaham D, Miettinen OS. Frequency of coronary artery calcification on low-dose computed tomography screening for lung cancer. Clin Imaging. 2006;30:181–5.
Lopes PM, Albuquerque F, Freitas P, Rocha BML, Cunha GJL, Santos AC, Abecasis J, Guerreiro S, Saraiva C, Mendes M, Ferreira AM. The updated pre-test probability model of the 2019 ESC guidelines improves prediction of obstructive coronary artery disease. Rev Port Cardiol. 2022;41:445–52.
Rijlaarsdam-Hermsen D, van Domburg RT, Deckers JW, Kuijpers D, van Dijkman PRM. Comparison of guidelines for diagnosing suspected stable angina and the additional value of the calcium score. Int J Cardiol. 2021;344:1–7.
Zhou J, Li C, Cong H, Duan L, Wang H, Wang C, Tan Y, Liu Y, Zhang Y, Zhou X, Zhang H, Wang X, Ma Y, Yang J, Chen Y, Guo Z. Comparison of different investigation strategies to defer cardiac testing in patients with stable chest pain. JACC Cardiovasc Imaging. 2022;15:91–104.
Rijlaarsdam-Hermsen D, Lo-Kioeng-Shioe M, van Domburg RT, Deckers JW, Kuijpers D, van Dijkman PRM. Stress-only adenosine CMR improves diagnostic yield in stable symptomatic patients with coronary artery calcium. JACC Cardiovasc Imaging. 2020;13:1152–60.
Groen RA, Jukema JW, van Dijkman PRM, Timmermans PT, Bax JJ, Lamb HJ, de Graaf MA. Evaluation of clinical applicability of coronary artery calcium assessment on non-gated chest computed tomography, compared with the classic Agatston score on cardiac computed tomography. Am J Cardiol. 2023;208:92–100.
Kalia NK, Miller LG, Nasir K, Blumenthal RS, Agrawal N, Budoff MJ. Visualizing coronary calcium is associated with improvements in adherence to statin therapy. Atherosclerosis. 2006;185:394–9.
Wong ND, Hsu JC, Detrano RC, Diamond G, Eisenberg H, Gardin JM. Coronary artery calcium evaluation by electron beam computed tomography and its relation to new cardiovascular events. Am J Cardiol. 2000;86:495–8.
Sandhu AT, Rodriguez F, Ngo S, Patel BN, Mastrodicasa D, Eng D, Khandwala N, Balla S, Sousa D, Maron DJ. Incidental coronary artery calcium: opportunistic screening of previous nongated chest computed tomography scans to improve statin rates (NOTIFY-1 Project). Circulation. 2023;147:703–14.
van der Aalst CM, Denissen S, Vonder M, Gratama JWC, Adriaansen HJ, Kuijpers D, Vliegenthart R, van Lennep JER, van der Harst P, Braam RL, van Dijkman PRM, van Bruggen R, Oudkerk M, de Koning HJ. Screening for cardiovascular disease risk using traditional risk factor assessment or coronary artery calcium scoring: the ROBINSCA trial. Eur Heart J Cardiovasc Imaging. 2020;21:1216–24.
Patel J, Pallazola VA, Dudum R, Greenland P, McEvoy JW, Blumenthal RS, Virani SS, Miedema MD, Shea S, Yeboah J, Abbate A, Hundley WG, Karger AB, Tsai MY, Sathiyakumar V, Ogunmoroti O, Cushman M, Savji N, Liu K, Nasir K, Blaha MJ, Martin SS, Al RM. Assessment of coronary artery calcium scoring to guide statin therapy allocation according to risk-enhancing factors: the multi-ethnic study of atherosclerosis. JAMA Cardiol. 2021;6:1161–70.
Lee SE, Chang HJ, Sung JM, Park HB, Heo R, Rizvi A, Lin FY, Kumar A, Hadamitzky M, Kim YJ, Conte E, Andreini D, Pontone G, Budoff MJ, Gottlieb I, Lee BK, Chun EJ, Cademartiri F, Maffei E, Marques H, Leipsic JA, Shin S, Choi JH, Chinnaiyan K, Raff G, Virmani R, Samady H, Stone PH, Berman DS, Narula J, Shaw LJ, Bax JJ, Min JK. Effects of statins on coronary atherosclerotic plaques: the PARADIGM study. JACC Cardiovasc Imaging. 2018;11:1475–84.
Nakazato R, Gransar H, Berman DS, Cheng VY, Lin FY, Achenbach S, Al-Mallah M, Budoff MJ, Cademartiri F, Callister TQ, Chang HJ, Cury RC, Chinnaiyan K, Chow BJ, Delago A, Hadamitzky M, Hausleiter J, Kaufmann P, Maffei E, Raff G, Shaw LJ, Villines TC, Dunning A, Feuchtner G, Kim YJ, Leipsic J, Min JK. Statins use and coronary artery plaque composition: results from the International Multicenter CONFIRM registry. Atherosclerosis. 2012;225:148–53.
Gomes DA, Lopes PM, Albuquerque F, Freitas P, Silva C, Guerreiro S, Abecasis J, Santos AC, Saraiva C, Ferreira J, de Araújo Gonçalves P, Marques H, Mendes M, Ferreira AM. Coronary artery calcium score as a gatekeeper for further testing in patients with low pretest probability of obstructive coronary artery disease: a cost-effectiveness analysis. Rev Port Cardiol. 2023;42(7):617–624.
Khan S, Chen CL, Brady MS, Parameswaran R, Moore R, Hassoun H, Carvajal RD. Unstable angina associated with cisplatin and carboplatin in a patient with advanced melanoma. J Clin Oncol. 2012;30:e163-164.
Koene RJ, Prizment AE, Blaes A, Konety SH. Shared risk factors in cardiovascular disease and cancer. Circulation. 2016;133:1104–14.
Armenian SH, Xu L, Ky B, Sun C, Farol LT, Pal SK, Douglas PS, Bhatia S, Chao C. Cardiovascular disease among survivors of adult-onset cancer: a community-based retrospective cohort study. J Clin Oncol. 2016;34:1122–30.
Mascalchi M, Puliti D, Romei C, Picozzi G, De Liperi A, Diciotti S, Bartolucci M, Grazzini M, Vannucchi L, Falaschi F, Pistelli F, Gorini G, Carozzi F, Rosselli A, Carrozzi L, Paci E, Zappa M. Moderate-severe coronary calcification predicts long-term cardiovascular death in CT lung cancer screening: the ITALUNG trial. Eur J Radiol. 2021;145: 110040.
Isgum I, Prokop M, Niemeijer M, Viergever MA, van Ginneken B. Automatic coronary calcium scoring in low-dose chest computed tomography. IEEE Trans Med Imaging. 2012;31:2322–34.
Takx RA, de Jong PA, Leiner T, Oudkerk M, de Koning HJ, Mol CP, Viergever MA, Išgum I. Automated coronary artery calcification scoring in non-gated chest CT: agreement and reliability. PLoS One. 2014;9: e91239.
Waltz J, Kocher M, Kahn J, Dirr M, Burt JR. The future of concurrent automated coronary artery calcium scoring on screening low-dose computed tomography. Cureus. 2020;12: e8574.
Valenti V, B ÓH, Heo R, Cho I, Schulman-Marcus J, Gransar H, Truong QA, Shaw LJ, Knapper J, Kelkar AA, Sandesara P, Lin FY, Sciarretta S, Chang HJ, Callister TQ, Min JK. A 15-year warranty period for asymptomatic individuals without coronary artery calcium: a prospective follow-up of 9,715 individuals. JACC Cardiovasc Imaging. 2015;8:900–9.
Min JK, Lin FY, Gidseg DS, Weinsaft JW, Berman DS, Shaw LJ, Rozanski A, Callister TQ. Determinants of coronary calcium conversion among patients with a normal coronary calcium scan: what is the “warranty period” for remaining normal? J Am Coll Cardiol. 2010;55:1110–7.
Dzaye O, Dardari ZA, Cainzos-Achirica M, Blankstein R, Agatston AS, Duebgen M, Yeboah J, Szklo M, Budoff MJ, Lima JAC, Blumenthal RS, Nasir K, Blaha MJ. Warranty period of a calcium score of zero: comprehensive analysis from MESA. JACC Cardiovasc Imaging. 2021;14:990–1002.
Dzaye O, Dardari ZA, Cainzos-Achirica M, Blankstein R, Szklo M, Budoff MJ, Lima JAC, Blumenthal RS, Nasir K, Blaha MJ. Incidence of new coronary calcification: time to conversion from CAC = 0. J Am Coll Cardiol. 2020;75:1610–3.
Williams MC, Kwiecinski J, Doris M, McElhinney P, D’Souza MS, Cadet S, Adamson PD, Moss AJ, Alam S, Hunter A, Shah ASV, Mills NL, Pawade T, Wang C, Weir McCall J, Bonnici-Mallia M, Murrills C, Roditi G, van Beek EJR, Shaw LJ, Nicol ED, Berman DS, Slomka PJ, Newby DE, Dweck MR, Dey D. Low-attenuation non-calcified plaque on coronary computed tomography angiography predicts myocardial infarction: results from the multicenter SCOT-HEART trial (Scottish computed tomography of the HEART). Circulation. 2020;141:1452–62.
Senoner T, Plank F, Beyer C, Langer C, Birkl K, Steinkohl F, Widmann G, Barbieri F, Adukauskaite A, Friedrich G, Dichtl W, Feuchtner GM. Does coronary calcium score zero reliably rule out coronary artery disease in low-to-intermediate risk patients? A coronary CTA study. J Cardiovasc Comput Tomogr. 2020;14:155–61.
Funding
No funding or sponsorship was received for this study or publication of this article.
Author information
Authors and Affiliations
Contributions
Roos A. Groen, J. Wouter Jukema, Paul R.M. van Dijkman, Jeroen J. Bax, Hildo J. Lamb, M. Louisa Antoni and Michiel A. de Graaf all meet the ICMJE criteria for authorship. They all have (1) made substantial contributions to the conception or design of the work; (2) drafted the work or revised it critically for important intellectual content; (3) approved the final version to be published; and (4) agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflict of Interest
J. Wouter Jukema/his department has received research grants from and/or was speaker (with or without lecture fees) on a.o. (CME accredited) meetings sponsored/supported by Abbott, Amarin, Amgen, Athera,, Biotronik, Boston Scientific, Dalcor, Daiichi Sankyo, Edwards Lifesciences, GE Healthcare Johnson and Johnson, Lilly, Medtronic, Merck-Schering-Plough, Novartis, Novo Nordisk, Pfizer, Roche, Sanofi Aventis, the Netherlands Heart Foundation, CardioVascular Research the Netherlands (CVON), the Netherlands Heart Institute and the European Community Framework KP7 Programme. This funding was not applied to the current research. Roos A. Groen, Paul R.M. van Dijkman, Jeroen J. Bax, Hildo J. Lamb, M. Louisa. Antoni and Michiel A. de Graaf declare they have no conflicts of interest for the present manuscript.
Ethical Approval
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Groen, R.A., Jukema, J.W., van Dijkman, P.R.M. et al. The Clear Value of Coronary Artery Calcification Evaluation on Non-Gated Chest Computed Tomography for Cardiac Risk Stratification. Cardiol Ther 13, 69–87 (2024). https://doi.org/10.1007/s40119-024-00354-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40119-024-00354-9