
Abstract
Introduction
It is important to achieve good persistence and adherence to disease-modifying therapies (DMTs) to achieve the best outcomes in chronic diseases such as multiple sclerosis (MS). The BETACONNECT device is an electronic auto-injector for the DMT interferon beta-1b (Betaseron), designed to improve patients’ injection experience and to monitor adherence. This observational study aimed to assess patient adherence to and persistence with interferon beta-1b therapy as well as patient-reported satisfaction in a US population.
Methods
A prospective, observational, multicenter study was conducted in 146 adult patients with relapsing–remitting MS or clinically isolated syndrome, newly prescribed or currently established on interferon beta-1b therapy and naïve to the BETACONNECT device, and followed up during a 6-month observation period.
Results
Among the 91 patients who completed the study, the overall mean adherence rate was 82.5%, with 65.9% of patients adherent for at least 80% for the duration of the 6-month period. At 6 months, 98.9% of patients had less than a 60-day gap in therapy. Of the 115 patients who provided satisfaction data, 90.5% of patients were either very satisfied or satisfied with the BETACONNECT device.
Conclusion
This study shows that the BETACONNECT device was associated with high adherence to interferon beta-1b therapy in patients with MS. Patients also reported high degrees of satisfaction with the device. Therefore, this may be a viable delivery option to help with adherence and persistence, potentially leading to improved clinical outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? | |
Lack of adherence to disease-modifying therapy (DMT) regimens can lead to poorer outcomes for patients with multiple sclerosis (MS). | |
This study assessed the effect of an electronic auto-injector for interferon beta-1b (BETACONNECT) on patient adherence, persistence, and satisfaction. | |
What was learned from the study? | |
Results showed that the device may help to improve adherence to interferon beta-1b therapy in patients with MS, as demonstrated by the high adherence, persistence, and satisfaction rates in this study. | |
This research provides real-world evidence for the use of BETACONNECT for the delivery of interferon beta-1b therapy for patients with MS in a US setting, and the potential to result in improved clinical outcomes. |
Introduction
Multiple sclerosis (MS) is a chronic, debilitating autoimmune disease. The prevalence of MS in the United States (USA) is estimated at 338–363 per 100,000 population, resulting in nearly 1 million people living with MS [1]. Patients experience ongoing central nervous system (CNS) damage, including lesion formation, demyelination, and neuro-axonal damage [2].
Initially, patients may present with clinically isolated syndrome (CIS), which may progress to relapsing–remitting multiple sclerosis (RRMS) involving an increased frequency of CNS exacerbations (i.e. relapses), and up to 15% may develop progressive MS [3, 4]. Disease-modifying therapies (DMTs) are a key therapeutic option in MS, and may help to prevent long-term disability [2, 3]. Interferon beta-1b (Betaseron, Bayer US LLC, Whippany, NJ, USA) is a type of DMT for patients with CIS or RRMS.
Adherence to medical regimens is particularly important for the management of chronic diseases such as MS. Generally, adherence is defined as the percentage of doses taken as prescribed over a set time period for analysis, either from the first to last medication dispensing date or for a fixed follow-up duration [5]. Medication adherence measurements can be subjective or objective: objective measures include pill counts, electronic monitoring, secondary database analyses, and biochemical measures, while subjective measurements require a provider or patient’s evaluation of their medication-taking behavior [6]. Self-report and healthcare professional assessments are the most common tools used to measure the frequency at which patients take their medications, but patients tend to underreport this rate in order to avoid disapproval from healthcare providers [6]. Poor adherence to medication regimens can have substantial, direct effects, resulting in worse health outcomes, increased costs, increased morbidity, and lower quality of life [5, 7,8,9].
DMT adherence for patients with MS can be particularly poor. In a US retrospective cohort study involving 5735 patients over 2 years, 55.3% of MS patients on interferon beta or glatiramer acetate had a treatment gap of at least 60 days [10]. MS patients with low adherence may suffer from more frequent exacerbations [11], and those who did not take their study medication properly or regularly were found to have 4.6 times higher odds of a relapse than those with very good or good adherence [12]. Poor adherence leads to an increased likelihood of DMT discontinuation [13], likely driven by progression of disease activity as well as adverse events such as injection-site reactions. In addition, studies have demonstrated overreporting of adherence when comparing subjective and objective reporting measures. In a study evaluating adherence among MS patients, 6.98% of days were recorded as not covered on medication by an electronic medication event monitoring system (MEMS) compared with 5.85% of days recorded in medication diaries [14].
Adherence to DMTs is associated with better clinical and economic outcomes: fewer relapses, decreased use of healthcare resources (e.g. emergency room visits and hospitalizations), and lower medical costs [15, 16]. MS patients adherent to first-line DMT regimens had significantly lower disability scores and greater satisfaction with treatment and its effectiveness than patients who were not adherent [17]. Furthermore, compared with non-adherent patients, MS patients who are adherent to their DMT regimen reported better emotional health, energy, and social function, and less pain [18, 19].
The introduction of electronic auto-injectors is one way to improve adherence to injectable DMTs. Compared with mechanical auto-injectors, electronic auto-injectors are often safer and more reliable, and have additional features to allow patients more control, resulting in less injection discomfort and greater patient satisfaction [20, 21]. The BETACONNECT device is an electronic auto-injector designed to improve the injection experience and monitor adherence to the interferon beta-1b regimen. Its reporting mechanism is built directly into the device and does not require patient input, which may help to ensure accuracy. The objective of this study was to evaluate the use of the BETACONNECT device on interferon beta-1b therapy adherence, persistence, and satisfaction in MS patients, and to provide real-world evidence on use of the device in a US population.
Methods
This was a prospective, multicenter, observational study that took place in 19 US-based MS centers. Before being enrolled in the study, patients provided written consent to participate by signing an informed consent form. Ethics approval was obtained from multiple ethics committees (see Table S1 in the electronic supplementary material), and the study was conducted in accordance with ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. Inclusion and exclusion criteria for the study are outlined in Table 1.
The primary endpoints were as follows: adherence to interferon beta-1b therapy, measured as the proportion of actual-to-expected number of injections completed during 6 months of treatment (or up to the point of early termination for the patients who did not complete the study) as captured by the BETACONNECT device; percentage of patients adherent to interferon beta-1b (i.e. received 80% or more of their expected injections) from data obtained via the BETACONNECT device; and persistence, measured as the number of days between the initial interferon beta-1b administration with the BETACONNECT device and the earlier of either the last interferon beta 1-b administration with the BETACONNECT device or before a minimum 60-day gap in therapy. The secondary endpoint was patient-reported satisfaction, measured by a satisfaction survey administered via email through a web-based electronic data capture tool.
All analyses were performed for the US study population receiving at least one dose of interferon beta-1b. The primary endpoint analysis looked at absolute adherence, the proportion of patients adherent to the therapy regimen, and the proportion of patients who were persistent with the therapy regimen at both 6 weeks and 6 months. Patients were excluded from the primary endpoint analysis if there was device error, insufficient device data (including patients with < 4 viable injections using the BETACONNECT device), withdrawal of consent, or loss to follow-up. The secondary endpoint analysis looked at overall patient satisfaction at 6 weeks, and patients were excluded if they withdrew consent or did not provide complete responses for the patient satisfaction survey.
Descriptive statistics were provided for all measures, including categorical measures by absolute and relative frequencies, and continuous measures by mean, standard deviation, median, interquartile range, minimum, and maximum. All analyses were performed using SAS version 9.4 software (SAS Institute Inc., Cary, NC, USA). Covariates were included to indicate whether the patient was naïve to interferon beta-1b and whether the patient completed the study.
Results
Study Population
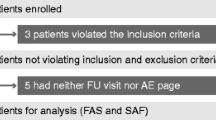
Of the 146 patients enrolled in the study, 102 patients were eligible for the primary endpoint analysis and 115 patients for the secondary endpoint analysis. A total of 44 patients were excluded from the primary endpoint analysis (36 patients were excluded owing to insufficient device data, nine withdrew consent, and four were excluded because of device error, non-adherence to medication titration, being non-English speaking, or not using the BETACONNECT device). Of the 31 patients excluded from the secondary analysis, 28 were because of insufficient survey data, and three were because of consent withdrawal. Some patients were excluded for multiple reasons, and thus counts for specific exclusion criteria are not mutually exclusive.
Among the 102 patients eligible for the primary endpoint analysis, the mean age was 52.2 years, 74.5% were female, patients were mostly classed as non-Hispanic (92.2%) or white (86.3%), and the majority were married (71.6%) (Table 2). For patients with a non-missing MS diagnosis date, the mean time since MS diagnosis was 10.3 years. For patients with CIS, the mean time since the first CIS event was 12.6 years. Of the 102 patients eligible for the primary endpoint analysis, 91 (89.2%) completed the study (i.e. did not leave the study before the expected 6 months of study participation) and were eligible for the final analysis. Those not included in the primary endpoint analysis (n = 11; 10.8%) were because of insufficient data (n = 7), device error (n = 1), incomplete BETACONNECT training (n = 1), non-adherence to the titration schedule (n = 1), and non-English speaking (n = 1). Of the 91 patients who were eligible for the final analysis, 80 patients (87.9%) were established on interferon beta-1b therapy while 11 patients (12.1%) were naïve to interferon beta-1b.
Adherence
Of the 91 patients who completed the study, the overall mean adherence rate was 82.5% (naïve patients, 96.9%; established patients, 80.6%; Table 3). A total of 65.9% (n = 60) (95% confidence interval [CI]: 56.2%, 75.7%) of patients were adherent to at least 80% of their expected injections at 6 months. Eleven (100%) of the patients naïve to interferon beta-1b therapy and 49 (61.3%) patients already established on interferon beta-1b therapy were considered adherent to their regimen at 6 months.
Persistence
Among patients who completed the study, 98.9% (95% CI 96.8%, 100%) were classed as persistent at 6 months; all of the naïve patients and 98.8% (95% CI 96.3%, 100%) of the established patients demonstrated persistence with their interferon beta-1b therapy using the BETACONNECT device. The mean overall time to non-persistence among completers was 169 days.
Satisfaction
Of the 115 patients who were eligible for the secondary endpoint analysis (17 naïve, 98 established) and provided satisfaction data, 73 (63.5%) reported being very satisfied with their BETACONNECT device, 31 (27.0%) being satisfied, nine (7.8%) being neither satisfied nor dissatisfied, and two (1.7%) being very dissatisfied (Fig. 1).

Patient satisfaction with the BETACONNECT device
Discussion
This study aimed to assess interferon beta-1b therapy adherence and persistence in patients, and patient-reported satisfaction, using the BETACONNECT electronic auto-injector. The results indicate that this device demonstrated high adherence and persistence rates over 6 months among adult patients with MS, whether naïve or established on interferon beta-1b therapy. Most patients reported being either very satisfied or satisfied with the BETACONNECT device.
The findings from the current study are similar to existing literature on other electronic auto-injector devices, although a formal head-to-head analysis has yet to be conducted. Similar studies were performed using RebiSmart (Merck KGaA, Darmstadt, Germany), an interferon beta-1a injection device; BRIDGE and RIVER were such studies in Italian RRMS patients receiving subcutaneous self-injections of interferon beta-1a with RebiSmart. BRIDGE showed high (> 85%) short-term adherence rates [22]. RIVER was a long-term adherence and safety assessment of BRIDGE (19–26 months) and showed that the overall adherence to the use of RebiSmart in the entire study cohort was 79.8% (median: 85.2%, range 16–100%) [23]. Additionally, the ScanSmart study was a prospective, single-arm, open-label, non-interventional, multicenter phase 4 study in Scandinavian patients to evaluate the rate that patients received treatment with subcutaneous interferon beta-1a; it showed that over 12 weeks, 89% (n = 48) of patients had ≥90% adherence to treatment [24]. (Note: the RebiSmart device is not available currently in the USA.)
Higher persistence rates were observed in the current publication than in other cohort studies, although a head-to-head analysis was not done. In a Canadian cohort study that followed 721 patients over 7.8 years, 451 patients (62.6%) discontinued their DMT during the study period, although 259 (57.4%) did resume/restart therapy [25]. The observed higher rate could be a potential benefit of the BETACONNECT device.
As was seen in our study, many patients also report being satisfied with the BETACONNECT device. High patient satisfaction rates with this electronic auto-injector have been reported in previous patient surveys, and patients have a positive impression of this device [20, 21, 26,27,28]. In addition, previous market surveys conducted to investigate patients’ ratings of subcutaneous interferon beta formulations with various devices (e.g. BETACONNECT, RebiSmart, ExtaviPro) showed that the BETACONNECT device was preferred [29]. Recently, a retrospective cohort study conducted in the USA found that after the introduction of BETACONNECT, adherence to interferon β-1b was higher than for patients taking interferon β-1a without an electronic auto-injector, and that more than 90% of patients using BETACONNECT had ≥ 90% medication possession ratio, a threshold commonly used to define good adherence [30]. In a further recent study, patient satisfaction with the BETACONNECT device was maintained over 2 years, with median scores of 9 out of 10 both at baseline and at the end of the study period [31].
It is also interesting to note that injection data collected by the BETACONNECT device can be paired with an app (myBETAapp), as observed in the ongoing PROmyBETAapp digital study (see below). Previous studies have shown that 92% of patients using the myBETAapp were very satisfied or satisfied with it [32]. Moreover, a digital observational study found that over a 6-month period, persistence with myBETAapp usage was 96%, mean compliance was 94% of injections completed, and adherence (persistence and ≥ 80% compliance) was 89% [33]. Among other functions to help patients manage their injections, myBETAapp allows patients to share their injection history with healthcare professionals and has a “wellness tracker” feature so they can record their well-being (for their own personal information). A prospective, observational, cohort study is currently underway to investigate medication use and patient-reported outcomes via myBETAapp in patients using the BETACONNECT auto-injector (ClinicalTrials.gov Identifier: NCT04356339). It is anticipated that the results of this study will provide a further perspective on issues covered in the current trial, such as adherence, persistence, and patient satisfaction.
The BETACONNECT device may be a promising and novel method to objectively measure rates at which patients take their MS treatment. Although subjective methodologies have their place, and demonstrate benefits such as ease of implementation and lower costs, objective measures have been shown to better reflect actual adherence and are thought to represent an improvement over subjective measures [6]. In addition, electronic measurements offer several advantages over more traditional adherence measures in MS, in part owing to their lack of dependence on human recall [6].
Some strengths of the current study include the incorporation of real-world evidence and patient perspective by taking patient satisfaction into consideration to assess patient adherence and persistence. Furthermore, this is the first study to look at these outcomes in a US population, and the 6-month time period adds to the robustness of results. However, this study has several limitations. First, the study design was non-randomized and uncontrolled, and since patients were self-selected to be included in this observational study, they may have been more likely to adhere to their medication. Patients were older in this population for both established RRMS and CIS, which may have influenced study results. It is possible that older patients could be more likely to adhere to their therapy, as a retrospective cohort study in patients with MS taking DMTs found that, compared with younger patients, those ≥ 45 years of age were between 13.7 and 18.6% more likely to be adherent to their regimen [34]. There could also be missing data from those patients who relapsed during the study period and were subsequently excluded, and the actual adherence rate could have been higher. Additionally, the definitions for the endpoints used in our study may have affected our findings. In our study, adherence was defined as the proportion of expected number of injections completed during 6 months of treatment or up to the point of early termination as captured by the BETACONNECT device and the percentage of patients who received ≥ 80% of their expected injections with the device. Persistence was defined as the number of days until the earlier of the last interferon beta-1b administration with the BETACONNECT device or before a minimum 60-day gap in therapy, reported as a percentage. However, adherence rates could differ, depending on whether the rate was defined as an average among a patient population or patients receiving a specific percentage of injections (e.g. > 80%). Lastly, only patients who had continuous access to interferon beta-1b treatment for the duration of the study and access to a personal computer were enrolled, possibly leading to selection bias. However, given that the results observed in this study were similar to those of other studies, we do not anticipate that these factors would significantly affect the results of this study.
It is also worth mentioning that the current investigation does not address any potential differences between oral and injectables DMTs, as this was beyond the scope of this observational study. However, it may also be important to note that published evidence in this respect is somewhat contradictory, and the way patients receive care may be as important as the route of DMT administration. Thus, although higher persistence and adherence rates were found with oral fingolimod than with injectable DMTs [35], comparable persistence rates have been found across oral and injectable DMTs [36], and another study found fewer missed doses with injectable than oral DMTs [37]. As most—perhaps as much as two-thirds—of non-adherence to MS therapies is caused by issues other than the route of drug administration, avoiding injectables, such as by the use of oral DMTs, will not completely solve the problem of non-adherence [38].
Conclusions
This study found that patients using the BETACONNECT device had high adherence to and persistence with interferon beta-1b therapy, and that adherence to and persistence with the BETACONNECT device were high in both naïve and established adult patients with MS receiving interferon beta-1b therapy. High satisfaction rates were also reported with this electronic auto-injector. Thus, the BETACONNECT device may be a viable delivery option for interferon beta-1b therapy that also tracks and reports adherence data. Further studies are underway to evaluate the use of the complete BETACONNECT system, including the use of an app (myBETAapp) to help ascertain adherence and persistence in conjunction with patient-reported outcomes (NCT04356339).
References
Wallin MT, Culpepper WJ, Campbell JD, et al. US Multiple Sclerosis Prevalence Workgroup. The prevalence of MS in the United States: a population-based estimate using health claims data. Neurology. 2019;92(10): e1029–40.
Reich DS, Lucchinetti CF, Calabresi PA. Multiple sclerosis. N Engl J Med. 2018;378(2):169–80.
Dobson R, Giovannoni G. Multiple sclerosis—a review. Eur J Neurol. 2019;26(1):27–40.
Lublin FD, Reingold SC, Cohen JA, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. 2014;83(3):278–86.
Menzin J, Caon C, Nichols C, White LA, Friedman M, Pill MW. Narrative review of the literature on adherence to disease-modifying therapies among patients with multiple sclerosis. J Manag Care Pharm. 2013;19(1 Suppl A):S24–40.
Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:217047.
Han E, Suh DC, Lee SM, Jang S. The impact of medication adherence on health outcomes for chronic metabolic diseases: a retrospective cohort study. Res Social Adm Pharm. 2014;10(6):e87-98.
Iuga AO, McGuire MJ. Adherence and health care costs. Risk Manag Healthc Policy. 2014;7:35–44.
Van Houtven C, Weinberger M, Carey T. Implications of nonadherence for economic evaluation and health policy. In: Bosworth HB, Oddone EZ, Weinberger M, editors. Patient treatment adherence concepts, interventions, and measurement. London: Lawrence Erlbaum Associates; 2006. p. 421–42.
Bonafede MM, Johnson BH, Wenten M, Watson C. Treatment patterns in disease-modifying therapy for patients with multiple sclerosis in the United States. Clin Ther. 2013;35(10):1501–12.
Bruce JM, Hancock LM, Lynch SG. Objective adherence monitoring in multiple sclerosis: initial validation and association with self-report. Mult Scler. 2010;16(1):112–20.
Hupperts R, Ghazi-Visser L, Martins Silva A, et al. The STAR Study: a real-world, international, observational study of the safety and tolerability of, and adherence to, serum-free subcutaneous interferon beta-1a in patients with relapsing multiple sclerosis. Clin Ther. 2014;36(12):1946–57.
Sabido-Espin M, Munschauer R. Reasons for discontinuation of subcutaneous interferon beta-1a three times a week among patients with multiple sclerosis: a real-world cohort study. BMC Neurol. 2017;17(1):57.
Bruce JM, Hancock LM, Arnett P, Lynch S. Treatment adherence in multiple sclerosis: association with emotional status, personality, and cognition. J Behav Med. 2010;33(3):219–27.
Steinberg SC, Faris RJ, Chang CF, Chan A, Tankersley MA. Impact of adherence to interferons in the treatment of multiple sclerosis: a non-experimental, retrospective, cohort study. Clin Drug Investig. 2010;30(2):89–100.
Tan H, Cai Q, Agarwal S, Stephenson JJ, Kamat S. Impact of adherence to disease-modifying therapies on clinical and economic outcomes among patients with multiple sclerosis. Adv Ther. 2011;28(1):51–61.
Saiz A, Mora S, Blanco J, En Representacion de los Investigadores del Estudio C. Therapeutic compliance of first line disease-modifying therapies in patients with multiple sclerosis. COMPLIANCE Study. Neurologia. 2015;30(4):214–22.
Treadaway K, Cutter G, Salter A, et al. Factors that influence adherence with disease-modifying therapy in MS. J Neurol. 2009;256(4):568–76.
Devonshire V, Lapierre Y, Macdonell R, et al. The global adherence project (GAP): a multicenter observational study on adherence to disease-modifying therapies in patients with relapsing–remitting multiple sclerosis. Eur J Neurol. 2011;18(1):69–77.
Weller I, Saake A, Schreiner T, Vogelreuter J, Petroff N. Patient satisfaction with the BETACONNECT autoinjector for interferon beta-1b. Patient Prefer Adherence. 2015;9:951–9.
Barone DA, Singer BA, Merkov L, Rametta M, Suarez G. Survey of US patients with multiple sclerosis: comparison of the new electronic interferon beta-1b autoinjector (BETACONNECT) with mechanical autoinjectors. Neurol Ther. 2016;5(2):155–67.
Lugaresi A, Florio C, Brescia-Morra V, et al. Patient adherence to and tolerability of self-administered interferon beta-1a using an electronic autoinjection device: a multicentre, open-label, phase IV study. BMC Neurol. 2012;12:7.
Lugaresi A, De Robertis F, Clerico M, et al. Long-term adherence of patients with relapsing–remitting multiple sclerosis to subcutaneous self-injections of interferon beta-1a using an electronic device: the RIVER study. Expert Opin Drug Deliv. 2016;13(7):931–5.
Pedersen ED, Stenager E, Vadgaard JL, et al. Adherence to subcutaneous interferon beta-1a treatment using an electronic injection device: a prospective open-label Scandinavian noninterventional study (the ScanSmart study). Patient Prefer Adherence. 2018;12:569–75.
Melesse DY, Marrie RA, Blanchard JF, Yu BN, Evans C. Persistence to disease-modifying therapies for multiple sclerosis in a Canadian cohort. Patient Prefer Adherence. 2017;11:1093–101.
Ziemssen T, Sylvester L, Rametta M, Ross AP. Patient satisfaction with the new interferon beta-1b autoinjector (BETACONNECT). Neurol Ther. 2015;4(2):125–36.
Kleiter I, Lang M, Jeske J, Norenberg C, Stollfuß B, Schürks M. Adherence, satisfaction and functional health status among patients with multiple sclerosis using the BETACONNECT® autoinjector: a prospective observational cohort study. BMC Neurol. 2017;17(1):174.
Patti F, Martínez Ginés ML, Norenberg C, Duarte Caron F. BetaEval Global: prospective, multinational, observational cohort study of patients using BETACONNECT®. Patient Prefer Adherence. 2020;14:771–9.
Limmroth V, Reischl J, Mann B, et al. Autoinjector preference among patients with multiple sclerosis: results from a national survey. Patient Prefer Adherence. 2017;11:1325–34.
Butler O, Heeg S, Holl K, Frenz AK, Wicklein EM, Rametta M, Yeo S. Real-world assessment of interferon-β-1b and interferon-β-1a adherence before and after the introduction of the BETACONNECT®autoinjector: a retrospective cohort study. Drugs Real World Outcomes. 2021;8(3):359–67.
Köhler W, Bayer-Gersmann K, Neußer T, Schürks M, Ziemssen T. Predictors of adherence among patients with multiple sclerosis using the BETACONNECT®autoinjector: a prospective observational cohort study. Front Neurol. 2021;12:643126.
Limmroth V, Bartzokis I, Bonmann E, Kusel P, Schreiner T, Schürks M. The BETACONNECT™ system: MS therapy goes digital. Neurodegener Dis Manag. 2018;8(6):399–410.
Limmroth V, Hechenbichler K, Müller C, Schürks M. Assessment of medication adherence using a medical app among patients with multiple sclerosis treated with interferon beta-1b: pilot digital observational study (PROmyBETAapp). J Med Internet Res. 2019;21(7):e14373.
Higuera L, Carlin CS, Anderson S. Adherence to disease-modifying therapies for multiple sclerosis. J Manag Care Spec Pharm. 2016;22(12):1394–401.
Bergvall N, Petrilla AA, Karkare SU, et al. Persistence with and adherence to fingolimod compared with other disease-modifying therapies for the treatment of multiple sclerosis: a retrospective US claims database analysis. J Med Econ. 2014;17(10):696–707.
Longbrake EE, Cross AH, Salter A. Efficacy and tolerability of oral versus injectable disease-modifying therapies for multiple sclerosis in clinical practice. Mult Scler J Exp Transl Clin. 2016;2:2055217316677868.
Dionne CA, Ganguly R, Camac A, Chaves C. Do oral disease modifying agents improve adherence to MS treatment? A comparison of oral and injectable drugs. In: 29th Annual meeting of the Consortium of Multiple Sclerosis Centers (CMSC), 27–30 May 2015, Indianapolis, USA. Abstract DX19.
Lugaresi A, Rottoli MR, Patti F. Fostering adherence to injectable disease-modifying therapies in multiple sclerosis. Expert Rev Neurother. 2014;14(9):1029–42.
Acknowledgements
The authors wish to acknowledge the patients, staff, and investigators at our clinical sites who participated in this study for their efforts.
Funding
This study was funded by Bayer Healthcare Pharmaceuticals, who also provided funding for the journal’s Rapid Service Fee.
Medical Writing, Editorial and Other Assistance
Bayer Healthcare Pharmaceuticals provided funding for medical writing and editorial support in the development of this manuscript. The authors thank Dr Richard Clark (Freelance Medical Writer, Dunchurch UK) for copyediting and styling the manuscript as per journal requirements, and his assistance with the manuscript submission process and help with addressing any peer-review comments.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Authors’ Contributions
All named authors contributed to the design of the study. Data collection was performed by Apryl Quillen and Kim McLeod. Data analysis and interpretation was performed by all authors. Apryl Quillen and Kim McLeod performed the statistical analyses. All authors participated in drafting/critically revising the manuscript.
Disclosures
Ryan Farej, Mark Rametta, and Anneliese LaRose are employees of Bayer US LLC, Whippany, New Jersey, United States. Apryl Quillen and Kim McLeod are employees of Xcenda LLC (AmerisourceBergen), Palm Harbor, Florida, United States.
Compliance with Ethics Guidelines
Before being enrolled in the study, patients provided written consent to participate by signing an informed consent form. Ethics approval was obtained from multiple ethics committees (see Table S1 in the electronic supplementary material), and the study was conducted in accordance with ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Data Availability
The datasets generated during and/or analyzed during the current study are not publicly available owing to the proprietorial nature of the data.
Author information
Authors and Affiliations
Corresponding authors
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Farej, R., Rametta, M., La Rose, A. et al. A Prospective, Observational, Multicenter Study Assessing Adherence to Interferon Beta-1b Therapy and Patient Satisfaction Using the BETACONNECT Auto-Injector. Neurol Ther 11, 373–384 (2022). https://doi.org/10.1007/s40120-022-00323-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40120-022-00323-1