
Abstract
Introduction
As the identification of Lewy body dementia (LBD) is often confirmed postmortem, there is a paucity of evidence on the progression of disease antemortem. This study aimed to comprehensively assess the course of LBD over time across cognitive, functional, and neuropsychiatric outcomes using real-world data.
Methods
Adults with at least one visit to an Alzheimer’s Disease Center with a diagnosis of mild cognitive impairment/dementia (index date), indication of LBD, and at least one follow-up visit were identified in the National Alzheimer’s Coordinating Center database (September 2005–June 2020). Participant characteristics, medication use, comorbidities, and changes in outcomes were assessed over a 5-year follow-up period and stratified by disease severity based on the Clinical Dementia Rating (CDR®) Dementia Staging Instrument-Sum of Boxes (CDR-SB) score at index.
Results
A total of 2052 participants with LBD (mean age at index 73.4 years) were included (mild, 219; moderate, 988; severe, 845). Mean annualized increase over 5 years was 0.9 points for CDR-Global Score, 5.6 points for CDR-SB, 10.4 points for the Functional Activities Questionnaire, and 2.0 points for the Neuropsychiatric Inventory-Questionnaire. Disease progression was greater among participants with moderate and severe LBD at index compared with those with mild LBD.
Conclusion
Participants with LBD experienced decline across all outcomes over time, and impairment increased with disease severity. Findings highlight the substantial clinical burden associated with LBD and the importance of earlier diagnosis and effective treatment. Further research is needed to understand the predictors of cognitive and functional decline in LBD which may help inform clinical trials.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Progression of Lewy body dementia (LBD) over time across cognitive, functional, and neuropsychiatric outcomes is not well understood. |
Previous studies on clinical outcomes among people with LBD have mainly focused on a single outcome or focused on smaller cohorts. |
This retrospective study reported participant characteristics, medication use, comorbidities, and changes in outcomes over a 5-year follow-up period. |
What was learned from the study? |
Participants with LBD experienced significant decline in cognitive, functional, and neuropsychiatric outcomes over time, and impairment increased with disease severity. |
These findings highlight the substantial clinical burden associated with LBD and the importance of earlier diagnosis and effective treatment. |
Introduction
Lewy body dementia (LBD) accounts for 5% to 10% of all dementia cases [1] and is characterized by progressive cognitive decline, neuropsychiatric symptoms, and motor symptoms consistent with Parkinson’s disease (PD) [2,3,4]. LBD encompasses dementia with Lewy bodies (DLB) and PD dementia (PDD) [5], and as a result of its progressive nature, the disease is associated with a substantial clinical burden. People with LBD experience lower quality of life [6], higher and earlier mortality [7, 8], higher hospitalization rates [9], and greater variability in cognitive decline relative to patients with Alzheimer’s disease (AD) [10], as well as high healthcare resource utilization and costs [11].
LBD is often underdetected and misdiagnosed. Despite the availability of specific diagnostic criteria, accurate diagnosis of LBD remains challenging, particularly at early stages, because of various factors including overlapping pathologies with AD and vascular dementia, atypical disease presentation, underuse of biomarkers, and insufficient neuropsychological evaluation [4, 12]. Furthermore, for patients diagnosed with LBD, there are currently no disease-modifying therapies available and treatments indicated for LBD target specific symptoms [13,14,15]. Other treatments have been used off-label to manage LBD-related symptoms (e.g., memantine, anti-Parkinson agents, quetiapine), though evidence regarding their overall effectiveness is limited [13, 16]. As a result, there is a substantial unmet clinical need among people with LBD.
Prior studies on clinical outcomes among people with LBD have generally focused on a single outcome such as decline in cognition [10, 17,18,19,20], functional activities [21, 22], or neuropsychiatric symptoms [23, 24]. A large, longitudinal international study found that the mean annual decline in Mini-Mental State Examination (MMSE) score in people with DLB was approximately 2 points [20]; notably, a decrease of 1–3 points is indicative of clinically meaningful decline [25, 26]. Over a 5-year follow-up period even people diagnosed with mild DLB reported a 4.4-point decline in the MMSE score, which occurred faster in DLB compared with AD [17]. In a different study, Vik-Mo and colleagues reported that LBD was associated with greater neuropsychiatric and psychotic symptoms than other forms of dementia, including AD [24]. Within the LBD cohort, people with DLB presented with more severe and widespread cognitive dysfunction than those with PDD based on MMSE and Montreal Cognitive Assessment (MoCA), particularly in attention, visuospatial and executive function, and language domains [19], highlighting the severity of disease.
As the identification of LBD is often confirmed postmortem, there is a paucity of evidence documenting the progression of disease antemortem [27, 28]. In particular, broad, real-world assessments that comprehensively capture the heterogeneous disease course of LBD across multiple cognitive, functional, and neuropsychiatric domains are scarce. Such insight has the potential to assist healthcare stakeholders to optimize care as well as inform clinical trials aimed at developing novel therapies for this difficult-to-treat patient population. Therefore, this study sought to assess the clinical features of LBD, including disease characteristics, medication use, comorbidities, and progression trajectories in terms of changes in cognition, function, and neuropsychiatric symptoms over time using real-world data. The results were reported for the cohort of patients with LBD overall, and also stratified by disease severity based on the Clinical Dementia Rating (CDR®) Dementia Staging Instrument Sum of Boxes (CDR-SB) score at the time of initial cognitive decline diagnosis.
Methods
Data Source
This study used data from 30 Alzheimer's Disease Centers (ADCs) through the US National Alzheimer’s Coordinating Center (NACC) Uniform Data Set (UDS) and the neuropathology (NP) dataset. Since 1999, the NACC has collected data from past and present ADCs supported by the US National Institute on Aging/National Institutes of Health [29]. The UDS includes participants with a range of cognitive status and contains information on demographics, medical and family history, as well as clinical information on cognitive, motor, functional, and neuropsychiatric status. Data for UDS are collected prospectively on an approximately annual basis and recorded directly by trained clinicians. Data were de-identified and compliant with the patient confidentiality requirements of the Health Insurance Portability and Accountability Act; as a result, approval from an ethics committee was not required.
The NP dataset contains autopsy data for a subset of participants from the UDS. In addition to age and date of death, the NP dataset includes information regarding the presence of neuropathological features for most major dementias [30].
Sample Selection
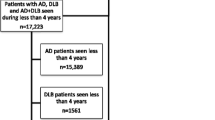
The study population included NACC participants with at least one ADC visit between September 2005 and June 2020 with a diagnosis of mild cognitive impairment (MCI) or dementia. The index date was defined as the date of the first visit with an indication of cognitive impairment. Participants were required to have an indication of LBD on or after the index date defined as any of the following: (1) primary, contributing, or non-contributing LBD etiology; (2) biomarker evidence of LBD on a dopamine transporter (DAT) scan (i.e., decreased striatal dopamine binding); or (3) evidence of LBD pathology postmortem. Additionally, participants were required to have at least one follow-up visit after the index date with non-missing data for the outcomes of interest in order to assess changes in disease progression over time (Fig. 1). The overall LBD cohort was stratified into three subgroups based on the CDR-SB score on the index date: mild (CDR-SB score 0–0.5); moderate (CDR-SB score 1–4); severe (CDR-SB score ≥ 4.5), in accordance with validated threshold values for identifying dementia in patients with PD [31].

Sample selection. CDR-GS Clinical Dementia Rating Global Score, CDR-SB Clinical Dementia Rating Sum of Boxes, LBD Lewy body dementia, MCI mild cognitive impairment, MoCA Montreal Cognitive Assessment, NPI-Q Neuropsychiatric Inventory-Questionnaire. LBD indication was defined as the presence of LBD etiology (primary, contributing, or non-contributing), biomarker evidence of LBD on a dopamine transporter (DAT) scan, or presence of LBD pathology postmortem. The index date was defined as the date of the first visit with indication of cognitive impairment (based on the earliest visit with clinician’s documentation of presence of cognitive decline, or the date of MCI/dementia diagnosis during subsequent visits, whichever occurred first). Participants were required to have non-missing data on at least one follow-up visit after the index date for CDR-GS, CDR-SB, MoCA, NPI-Q, changes in falls, tremors, and slowness
Study Measures and Outcomes
Participant characteristics were evaluated on the index date and included demographics (e.g., age, sex, race, ethnicity), select comorbidities, APOE ε4 genotype status, and self-reported medication use. Cognitive characteristics included age at onset of cognitive decline based on clinician assessment, clinical assessment of symptoms, CDR-Global Score (CDR-GS), CDR-SB score, and MoCA score (which replaced MMSE in the NACC database in March 2015) [32,33,34]. For patients with only MMSE scores available in the data, MMSE scores were mapped into MoCA scores using a published conversion algorithm validated in people with PD to generate uniform summary measures across the different time periods [35]. If one MMSE score could be mapped onto multiple MoCA scores, the lower MoCA score was used.
Functional outcomes that were analyzed included the Functional Assessment Questionnaire (FAQ) score (which quantifies participants’ ability to perform essential daily activities, such as preparing meals and managing personal finances; a score of ≥ 9 indicates impaired function [36]), level of independence, and PD symptoms (e.g., bradykinesia, gait disorder, posture instability). Neuropsychiatric outcomes that were analyzed included the total Neuropsychiatric Inventory-Questionnaire (NPI-Q) severity score (higher scores indicating greater symptom severity [37,38,39,40]) and the proportions of participants with specific neuropsychiatric symptoms included in the NPI-Q (e.g., delusions, hallucinations, depression). Outcomes were assessed at each visit after the index visit.
Statistical Analysis
Participant characteristics and outcomes were summarized descriptively using means and standard deviations for continuous variables and frequencies and percentages for categorical variables. The assessment of outcomes at each follow-up visit was conducted among participants with non-missing values for the outcome at the given visit. For the stratified analyses by CDR-SB score at index, statistical differences were evaluated using chi-square tests for categorical variables and Wilcoxon rank-sum tests for continuous variables for all characteristics except for cognitive assessments because they differed across the three subgroups by design. Mean changes in outcomes during the follow-up visits and the annualized mean change from the index date were described for each CDR-SB subgroup. While ADC visits are typically 12 months apart, some participants had variable time between visits. For example, 21% of the sample had visits that were 6–11 months apart and 9% had visits 18 months or more apart. To account for this variability, the annualized change was calculated using linear extrapolation or interpolation of the change in scores between visits. To explore the implications of sample attrition over time, a sensitivity analysis was conducted whereby the overall LBD cohort was restricted to participants with complete information for all outcomes of interest except FAQ for at least five visits. All analyses were conducted using SAS Enterprise Guide version 7.15 and R version 3.6.1.
Results
A total of 2052 participants met all inclusion criteria and among them, 219 (10.7%) had mild LBD, 988 (48.1%) had moderate LBD, and 845 (41.2%) had severe LBD (Fig. 1).
Characteristics at Index Visit
Characteristics among participants with LBD overall and stratified by CDR-SB score at index are summarized in Table 1. Most participants were male (67.5%) and the mean age on the index date was 73 years. Participants with mild LBD were significantly older than participants with moderate and severe LBD (76 vs. 73 and 73 years, respectively; p < 0.001). Less than half (42.7%) of the participants had a primary LBD etiology, 35.2% were identified with LBD pathology postmortem, 22.1% had a contributing or non-contributing LBD etiology, or biomarker evidence of LBD on a DAT scan. Most participants either had no copy of APOE ε4 (44.8%) or had one copy (33.4%), 9.4% had two copies, and 12.4% had an unknown number.
The three most common comorbid conditions were hypercholesterolemia (53.3%), hypertension (50.1%), and depression (48.3%). The proportion of participants with LBD using AD medications increased with disease severity. The use of memantine among participants with mild, moderate, and severe LBD was 5.9%, 16.4%, and 37.8%, respectively; the use of cholinesterase inhibitors was 16.9%, 48.6%, and 69.2%, respectively. Other medications that were common during the baseline period were antidepressants (mild, 25.1%; moderate, 40.3%; severe, 44.1%) and anti-Parkinson agents (mild, 14.6%; moderate, 20.0%; severe, 13.4%).
Clinical outcomes at the index visit are summarized in Table 2. The mean age at onset of cognitive decline was slightly higher among participants with mild LBD compared with those with moderate and severe (mild, 73; moderate, 69; severe, 68 years).
In general, participants with mild LBD had better cognitive, functional, and neuropsychiatric performance at index relative to participants with moderate and severe LBD as indicated by a higher mean MoCA score and lower mean CDR-GS, CDR-SB, FAQ, and NPI-Q scores (Table 2). The proportion of participants with impaired function (FAQ score ≥ 9) was almost 20 times lower among those with mild vs. severe LBD (mild, 3.2%; moderate, 21.2%; severe, 58.2%). The proportion of participants requiring some assistance with basic or complex activities was also the lowest for mild LBD (mild, 10.5%; moderate, 52.6%; severe, 83.8%). More than half of participants in each subgroup had any PD symptoms present at baseline (mild, 55.7%; moderate, 64.4%; severe, 65.1%).
Study Outcomes
Outcome assessments at follow-up visits 1, 3, and 5 after the index visit are summarized in Supplementary Material Table S1. Overall, hypertension, hypercholesterolemia, and depression remained the most common comorbid conditions post-index. The use of memantine and cholinesterase inhibitors remained stable over the 5-year follow-up period for the overall LBD cohort and was lowest among participants with mild relative to severe LBD. The use of anti-Parkinson agents was slightly higher among participants with mild and moderate LBD relative to those with severe LBD, while antidepressant use was lower among participants with mild LBD relative to those with moderate and severe LBD.
Cognitive, functional, and neuropsychiatric outcomes generally worsened over time for the overall LBD cohort and the deterioration was greater among participants with moderate and severe LBD compared with those with mild LBD. In particular, CDR-GS and CDR-SB scores increased over time for all subgroups and the magnitude of change was highest for participants with severe LBD at each follow-up visit post-index. The mean annualized increase in CDR-GS and CDR-SB over 5 years relative to the index visit increased with LBD severity (ranging from 0.4 to 1.2 and from 3.5 to 7.3, respectively). The mean annualized decrease in MoCA score over 5 years relative to the index visit was 5.5 for mild LBD, 6.5 for moderate LBD, and 6.1 for severe LBD (Fig. 2).

Change in a CDR-GS, b CDR-SB, and c MoCA scores over time stratified by CDR-SB at index. CDR Clinical Dementia Rating, CDR-GS Clinical Dementia Rating Global Score, CDR-SB Clinical Dementia Rating Sum of Boxes, MCI mild cognitive impairment, MoCA Montreal Cognitive Assessment. Participants with CDR-SB score of 0–0.5 on the index date were considered to have impairment of mild severity (“mild LBD”), while those with CDR-SB scores of 1–4 and ≥ 4.5 were considered to have impairment of greater severity (“moderate LBD” and “severe LBD”, respectively) [31]
Overall, the proportion of participants classified as having impaired function (FAQ score of ≥ 9) increased from visit 1 to 5 post-index from 8.2% to 35.6% for those with mild LBD, 35.4% to 56.0% for those with moderate LBD, and 66.5% to 83.0% for those with severe LBD. The mean annualized increase in the total FAQ score over 5 years relative to the index visit was 10.0, 12.5, and 7.5 for mild, moderate, and severe LBD. The proportion of participants classified as completely dependent also increased with disease severity from visit 1 to 5 post-index from 0.9% to 6.7% for mild, 2.7% to 20.9% for moderate, and 14.2% to 62.6% for severe LBD (Fig. 3). The cumulative proportion of participants experiencing meaningful changes in falls, tremors, and slowness was also higher for those with severe LBD: 50.3%, 47.6%, and 75.5% by visit 5 post-index, respectively. The proportion of participants with any PD symptoms post-index was stable among those with mild LBD (57.1–57.8% from visit 1 to 5 post-index) and declined for those with moderate and severe LBD from 68.3% to 49.8% and from 71.7% to 38.1%, respectively. The mean annualized increase in the total NPI-Q score over 5 years relative to the index visit was 1.6, 2.2, and 1.9 for mild, moderate, and severe LBD, indicating slightly increased severity of neuropsychiatric symptoms (Fig. 4). The proportion of participants with specific neuropsychiatric symptoms was relatively stable over time across the three LBD subgroups (Supplementary Material Table S1).

Change in a FAQ score ≥ 9, b total FAQ score, and c dependence in daily activities over time stratified by CDR-SB at index. CDR-SB Clinical Dementia Rating Sum of Boxes, FAQ Functional Activities Questionnaire. Participants with CDR-SB score of 0–0.5 on the index date were considered to have impairment of mild severity (“mild LBD”), while those with CDR-SB scores of 1–4 and ≥ 4.5 were considered to have impairment of greater severity (“moderate LBD” and “severe LBD”, respectively) [31]. FAQ score of ≥ 9 (dependent in ≥ 3 activities) was used to indicate impaired function [36]

Change in NPI-Q score over time stratified by CDR-SB at index. CDR-SB Clinical Dementia Rating Sum of Boxes, MCI mild cognitive impairment, NPI-Q Neuropsychiatric Inventory-Questionnaire. Participants with CDR-SB score of 0–0.5 on the index date were considered to have impairment of mild severity (“mild LBD”), while those with CDR-SB scores of 1–4 and ≥ 4.5 were considered to have impairment of greater severity (“moderate LBD” and “severe LBD”, respectively) [31]
The number of participants with available data on outcomes after the first follow-up visit post-index declined over time, with approximately 41%, 28%, and 17% of participants remaining in the mild, moderate, and severe subgroups, respectively, by visit 5. Findings from the sensitivity analysis in participants with complete information for outcomes of interest for at least five visits (n = 287) were consistent with the annualized mean change in outcomes for the overall LBD cohort (Supplementary Material Figs. S1–S6).
Discussion
This comprehensive study reported participant characteristics, treatment patterns, and progression over time among a diverse cohort of older adults with LBD in the USA. Participants with LBD experienced decline in multiple cognitive, functional, and neuropsychiatric outcomes over time. The worsening in cognition and function based on CDR-GS, CDR-SB, MoCA, and FAQ scores was largest among participants with moderate and severe LBD at the time of diagnosis relative to those with mild LBD, indicating potential acceleration of cognitive and functional decline as the disease progresses. Approximately 5 years following the index date, 60.2% of all participants with LBD had impaired function based on their FAQ score. Additionally, the level of dependence increased over time with disease severity, such that over half of participants required assistance with both basic and complex activities and 30% were completely dependent at visit 5 post-index. The proportion of participants with specific neuropsychiatric symptoms remained relatively stable across the three LBD subgroups over time, though the total NPI-Q score worsened slightly relative to the index visit, indicating an increased severity of neuropsychiatric symptoms. The annualized mean change in outcomes was consistent with the main results for the overall LBD cohort and showed decline in different domains, further highlighting the progressive nature of LBD across a wide spectrum of clinical features. These findings also illustrate the need for therapies that address the wide range of symptoms specific to LBD or help slow disease progression.
The demographic characteristics and comorbidity profiles of the LBD cohort overall and stratified by disease severity based on the CDR-SB score at the index visit were largely similar. The age at onset of cognitive decline was slightly higher among participants with mild LBD compared with those with moderate and severe, which could be likely driven by a higher proportion of participants with PDD vs. DLB in the mild group or potentially greater AD co-pathology in the severe group. About a third of participants were identified with LBD pathology postmortem, and the proportion was slightly higher among those with severe LBD, highlighting the challenges of early and accurate diagnosis of people with LBD. Previous findings from autopsy studies have suggested that DLB pathology occurs in about 20–25% of dementia cases in older adults [41]. While the clinical diagnosis of LBD is largely based on obtaining accurate clinical history and timeline of symptoms, postmortem autopsy is currently the only way to make a conclusive diagnosis and even then overlapping pathology is often seen [12].
Despite more than half of participants having PD symptoms present at the time of initial cognitive decline diagnosis, the use of anti-Parkinson agents was low, and remained so over time. This finding is likely driven by concerns about the limited benefit of dopaminergic medications in LBD, including low likelihood of motor improvement and risk of psychosis exacerbation [42]. The most commonly used medications at index among the overall LBD cohort were cholinesterase inhibitors (53.7%) and antidepressants (40.3%). The use of memantine and cholinesterase inhibitors increased with disease severity both at index and during the follow-up period and was generally higher among participants with severe LBD. The low use of symptomatic treatments in this population also highlights the need for improved therapies focusing on the treatment of symptoms specific to LBD [43], as well as those targeting the pathological mechanisms of the disease, potentially before symptoms and clinical signs develop [44]. While about half of the overall LBD cohort had any PD symptoms present during the follow-up period, a decrease was observed for the severe LBD subgroup from 71.7% to 38.1% at visits 1 to 5 post-index, respectively. This is likely driven by attrition of participants over time, suggesting that those with severe LBD and motor impairments may be more likely to be lost to follow-up because of the severity of their condition. Indeed, in the sensitivity analysis, the proportion of participants with LBD who had PD symptoms increased from 53.0% to 66.2% at visits 1 to 5 post-index, respectively.
This is one of the few studies to comprehensively document the disease progression trajectories with respect to cognitive, functional, and neuropsychiatric outcomes among people with LBD. While most of the previous literature on LBD focused on single outcomes [10, 17, 20, 21], aspects of our findings are consistent with prior studies. Previous research evaluating annual decline in MMSE scores reported a similar decline of 2 to 4 points among patients with LBD [17, 20]. In terms of functional decline, we found that the 1-year change in FAQ score ranged from 1 to 3 points, which is consistent with findings from Gill and colleagues [21].
It is well documented that decline in cognitive, functional, and neuropsychiatric function may potentially have a negative impact on other outcomes. For example, a recent health state transition model evaluating LBD disease progression found that reducing the annual risk of transitioning from mild to severe DLB by 40% decreased time institutionalized and increased time to death [45]. Further studies are needed to assess how different rates of progression in cognitive, functional, and neuropsychiatric outcomes by disease severity at initial assessment may affect healthcare resource use, costs, and survival over time as well as to evaluate the disease burden of LBD compared with other neurodegenerative diseases such as AD or PD or a control cohort. It is also important to understand the predictors of cognitive and functional decline among people with LBD overall and any differences in the underlying pathological processes between DLB and PDD subtypes. Such information may help in defining more homogenous groups of participants with LBD for recruitment in clinical trials targeting specific disease mechanisms [46]. Nevertheless, taken together, our study findings provide valuable insights into the disease trajectories of older adults with LBD under the current standard of care and highlight the need for better diagnostic tools to identify LBD in early stages. These observations could in turn inform future clinical trials for potential disease-modifying treatments for LBD as well as policy interventions to improve care management for older adults with LBD in the USA.
This study was subject to certain limitations. Although the study utilized data from a diverse set of participants across 30 ADCs in the USA, the results may not be generalized to the entire US population as NACC participants represent a clinic-based convenience sample and tend to be highly educated. Furthermore, individual ADCs recruit and enroll participants according to their own protocols and the varying inclusion/exclusion criteria may introduce bias into the sample. More than a third of participants in the LBD cohort were identified with LBD pathology postmortem and did not have a formal LBD diagnosis antemortem. As a result, the study sample may not adequately reflect the broader population of people with LBD encountered in real-world clinical practice. Additionally, the study sample was broadly categorized as having LBD based on clinician assessment of the dementia etiology recorded in the database. However, it was not feasible to differentiate between DLB and PDD—two related yet distinct subtypes of LBD which may result in different disease progression trajectories than the overall LBD cohort. The proportion of participants with available data declined considerably over time. Although the precise reason for attrition is unavailable in the data, participants with worsening cognitive impairment, neuropsychiatric symptoms, and difficulty with functional activities may be more likely to be lost to follow-up [47]. Consequently, the long-term decline in all outcomes, particularly in later years following the index date, may be underestimated. In addition, the medication use assessed in this study is self-reported (or informant-reported) and therefore should be interpreted with caution. Finally, all analyses were descriptive and did not adjust for differences in participants’ baseline characteristics or compare outcomes relative to participants without LBD. Further research is warranted to investigate factors associated with disease progression over time using multivariate models such linear mixed models.
Conclusion
Findings from this study highlight the substantial clinical burden associated with LBD. The demographic characteristics and comorbidity profiles of the LBD cohort overall and stratified by disease severity were largely similar and a third of participants were identified with LBD pathology postmortem. Participants with LBD experienced progression across several cognitive, functional, and neuropsychiatric outcomes, including CDR-GS, CDR-SB, MoCA, FAQ, NPI-Q, and dependence in daily activities. The decline was particularly pronounced for measures of function and cognition and was even greater among participants with moderate and severe LBD compared with those with mild LBD. While the use of cholinesterase inhibitors and memantine increased with disease severity, the proportion of patients using anti-Parkinson agents remained low over time. Timely and accurate diagnosis of LBD and better understanding of the disease trajectory may help improve patient care and also inform clinical trials aimed at developing disease-modifying and improved symptomatic therapies for this patient population.
References
Alzheimer's Association: about Lewy body dementia. https://www.alz.org/alzheimers-dementia/what-is-dementia/types-of-dementia/lewy-body-dementia Accessed July 15, 2021.
Tahami Monfared AA, Meier G, Perry R, Joe D. Burden of disease and current management of dementia with Lewy bodies: a literature review. Neurol Ther. 2019;8(2):289–305. https://doi.org/10.1007/s40120-019-00154-7.
Cromarty RA, Elder GJ, Graziadio S, et al. Neurophysiological biomarkers for Lewy body dementias. Clin Neurophysiol. 2016;127(1):349–59. https://doi.org/10.1016/j.clinph.2015.06.020.
Chin KS, Teodorczuk A, Watson R. Dementia with Lewy bodies: challenges in the diagnosis and management. Aust N Z J Psychiatry. 2019;53(4):291–303. https://doi.org/10.1177/0004867419835029.
Gomperts SN. Lewy body dementias: dementia with Lewy bodies and Parkinson disease dementia. Continuum (Minneap Minn). 2016;22(2):435–63. https://doi.org/10.1212/CON.0000000000000309.
Boström F, Jönsson L, Minthon L, Londos E. Patients with dementia with Lewy bodies have more impaired quality of life than patients with Alzheimer disease. Alzheimer Dis Assoc Disord. 2007;21(2):150–4. https://doi.org/10.1097/WAD.0b013e318065c4a9.
Mueller C, Soysal P, Rongve A, et al. Survival time and differences between dementia with Lewy bodies and Alzheimer’s disease following diagnosis: a meta-analysis of longitudinal studies. Ageing Res Rev. 2019;50:72–80. https://doi.org/10.1016/j.arr.2019.01.005.
Price A, Farooq R, Yuan JM, Menon VB, Cardinal RN, O’Brien JT. Mortality in dementia with Lewy bodies compared with Alzheimer’s dementia: a retrospective naturalistic cohort study. BMJ Open. 2017;7(11):e017504. https://doi.org/10.1136/bmjopen-2017-017504.
Mueller C, Perera G, Rajkumar AP, et al. Hospitalization in people with dementia with Lewy bodies: frequency, duration, and cost implications. Alzheimers Dement (Amst). 2018;10:143–52. https://doi.org/10.1016/j.dadm.2017.12.001.
Giil LM, Aarsland D. Greater variability in cognitive decline in Lewy body dementia compared to Alzheimer’s disease. J Alzheimers Dis. 2020;73(4):1321–30. https://doi.org/10.3233/JAD-190731.
Espinosa R, Davis M, Johnson S, Cline S, Weintraub D. Direct medical costs of dementia with Lewy bodies by disease complexity. J Am Med Dir Assoc. 2020;21(11):1696–704. https://doi.org/10.1016/j.jamda.2020.06.006.
Sanford AM. Lewy body dementia. Clin Geriatr Med. 2018;34(4):603–15. https://doi.org/10.1016/j.cger.2018.06.007.
Tahami Monfared AA, Desai M, Hughes R, Lucherini S, Yi Y, Perry R. Treatment options for dementia with Lewy bodies: a network meta-analysis of randomised control trials. Neurol Ther. 2020;9(2):521–34. https://doi.org/10.1007/s40120-020-00198-0.
U.S. Food and Drug Administration: Exelon®: Highlights of prescribing information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2007/022083lbl.pdf Accessed July 15, 2021.
European Medicines Agency: Rivastigmine Actavis. https://www.ema.europa.eu/en/medicines/human/EPAR/rivastigmine-actavis Accessed July 15, 2021.
Palermo G, Ceravolo R, Bonuccelli U. Advances in the pharmacotherapeutic management of dementia with Lewy bodies. Expert Opin Pharmacother. 2018;19(15):1643–53. https://doi.org/10.1080/14656566.2018.1519548.
Rongve A, Soennesyn H, Skogseth R, et al. Cognitive decline in dementia with Lewy bodies: a 5-year prospective cohort study. BMJ Open. 2016;6(2):e010357. https://doi.org/10.1136/bmjopen-2015-010357.
Matar E, Shine JM, Halliday GM, Lewis SJG. Cognitive fluctuations in Lewy body dementia: towards a pathophysiological framework. Brain. 2020;143(1):31–46. https://doi.org/10.1093/brain/awz311.
Martini A, Weis L, Schifano R, et al. Differences in cognitive profiles between Lewy body and Parkinson’s disease dementia. J Neural Transm (Vienna). 2020;127(3):323–30. https://doi.org/10.1007/s00702-019-02129-2.
Kramberger MG, Auestad B, Garcia-Ptacek S, et al. Long-term cognitive decline in dementia with Lewy bodies in a large multicenter international cohort. J Alzheimers Dis. 2017;57(3):787–95. https://doi.org/10.3233/JAD-161109.
Gill DP, Hubbard RA, Koepsell TD, et al. Differences in rate of functional decline across three dementia types. Alzheimers Dement. 2013;9(5 Suppl):S63-71. https://doi.org/10.1016/j.jalz.2012.10.010.
Gill DP, Koepsell TD, Hubbard RA, Kukull WA. Risk of decline in functional activities in dementia with Lewy bodies and Alzheimer disease. Alzheimer Dis Assoc Disord. 2011;25(1):17–23. https://doi.org/10.1097/WAD.0b013e3182037edf.
Vik-Mo AO, Giil LM, Borda MG, Ballard C, Aarsland D. The individual course of neuropsychiatric symptoms in people with Alzheimer’s and Lewy body dementia: 12-year longitudinal cohort study. Br J Psychiatry. 2020;216(1):43–8. https://doi.org/10.1192/bjp.2019.195.
Vik-Mo AO, Giil LM, Ballard C, Aarsland D. Course of neuropsychiatric symptoms in dementia: 5-year longitudinal study. Int J Geriatr Psychiatry. 2018;33(10):1361–9. https://doi.org/10.1002/gps.4933.
Andrews JS, Desai U, Kirson NY, Zichlin ML, Ball DE, Matthews BR. Disease severity and minimal clinically important differences in clinical outcome assessments for Alzheimer’s disease clinical trials. Alzheimers Dement (N Y). 2019;5:354–63. https://doi.org/10.1016/j.trci.2019.06.005.
Watt JA, Veroniki AA, Tricco AC, Straus SE. Using a distribution-based approach and systematic review methods to derive minimum clinically important differences. BMC Med Res Methodol. 2021;21(1):41. https://doi.org/10.1186/s12874-021-01228-7.
Jellinger KA. Dementia with Lewy bodies and Parkinson’s disease-dementia: current concepts and controversies. J Neural Transm (Vienna). 2018;125(4):615–50. https://doi.org/10.1007/s00702-017-1821-9.
Skogseth R, Hortobagyi T, Soennesyn H, et al. Accuracy of clinical diagnosis of dementia with Lewy bodies versus neuropathology. J Alzheimers Dis. 2017;59(4):1139–52. https://doi.org/10.3233/JAD-170274.
Besser L, Kukull W, Knopman DS, et al. Version 3 of the National Alzheimer’s Coordinating Center’s uniform data set. Alzheimer Dis Assoc Disord. 2018;32(4):351–8. https://doi.org/10.1097/wad.0000000000000279.
Besser LM, Kukull WA, Teylan MA, et al. The revised National Alzheimer’s Coordinating Center’s neuropathology form-available data and new analyses. J Neuropathol Exp Neurol. 2018;77(8):717–26. https://doi.org/10.1093/jnen/nly049.
Wyman-Chick KA, Scott BJ. Development of clinical dementia rating scale cutoff scores for patients with Parkinson’s disease. Mov Disord Clin Pract. 2015;2(3):243–8. https://doi.org/10.1002/mdc3.12163.
Morris JC. The clinical dementia rating (CDR): current version and scoring rules. Neurology. 1993;43(11):2412–4. https://doi.org/10.1212/wnl.43.11.2412-a.
Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–9. https://doi.org/10.1111/j.1532-5415.2005.53221.x.
Monsell SE, Dodge HH, Zhou XH, et al. Results from the NACC uniform data set neuropsychological battery crosswalk study. Alzheimer Dis Assoc Disord. 2016;30(2):134–9. https://doi.org/10.1097/WAD.0000000000000111.
Lawton M, Kasten M, May MT, et al. Validation of conversion between mini-mental state examination and Montreal cognitive assessment. Mov Disord. 2016;31(4):593–6. https://doi.org/10.1002/mds.26498.
Pfeffer RI, Kurosaki TT, Harrah CH Jr, Chance JM, Filos S. Measurement of functional activities in older adults in the community. J Gerontol. 1982;37(3):323–9. https://doi.org/10.1093/geronj/37.3.323.
Morris JC, Weintraub S, Chui HC, et al. The uniform data set (UDS): clinical and cognitive variables and descriptive data from Alzheimer disease centers. Alzheimer Dis Assoc Disord. 2006;20(4):210–6. https://doi.org/10.1097/01.wad.0000213865.09806.92.
Weintraub S, Besser L, Dodge HH, et al. Version 3 of the Alzheimer Disease Centers’ neuropsychological test battery in the uniform data set (UDS). Alzheimer Dis Assoc Disord. 2018;32(1):10–7. https://doi.org/10.1097/wad.0000000000000223.
Weintraub S, Salmon D, Mercaldo N, et al. The Alzheimer’s Disease Centers’ uniform data set (UDS): the neuropsychologic test battery. Alzheimer Dis Assoc Disord. 2009;23(2):91–101. https://doi.org/10.1097/WAD.0b013e318191c7dd.
Kaufer DI, Cummings JL, Ketchel P, et al. Validation of the NPI-Q, a brief clinical form of the Neuropsychiatric Inventory. J Neuropsychiatry Clin Neurosci. 2000;12(2):233–9. https://doi.org/10.1176/jnp.12.2.233.
Galasko D. Lewy body disorders. Neurol Clin. 2017;35(2):325–38. https://doi.org/10.1016/j.ncl.2017.01.004.
Goldman JG, Goetz CG, Brandabur M, Sanfilippo M, Stebbins GT. Effects of dopaminergic medications on psychosis and motor function in dementia with Lewy bodies. Mov Disord. 2008;23(15):2248–50. https://doi.org/10.1002/mds.22322.
Taylor JP, McKeith IG, Burn DJ, et al. New evidence on the management of Lewy body dementia. Lancet Neurol. 2020;19(2):157–69. https://doi.org/10.1016/S1474-4422(19)30153-X.
Walker Z, Possin KL, Boeve BF, Aarsland D. Lewy body dementias. Lancet. 2015;386(10004):1683–97. https://doi.org/10.1016/S0140-6736(15)00462-6.
Espinosa R, Davis M, Johnson S, Cline S, Weintraub D. A model to assess the outcomes associated with dementia with Lewy bodies. Alzheimer Dis Assoc Disord. 2021;35(1):68–74. https://doi.org/10.1097/wad.0000000000000412.
Goldman JG, Forsberg LK, Boeve BF, et al. Challenges and opportunities for improving the landscape for Lewy body dementia clinical trials. Alzheimers Res Ther. 2020;12(1):137. https://doi.org/10.1186/s13195-020-00703-5.
Burke SL, Hu T, Naseh M, et al. Factors influencing attrition in 35 Alzheimer’s disease centers across the USA: a longitudinal examination of the National Alzheimer’s Coordinating Center’s uniform data set. Aging Clin Exp Res. 2019;31(9):1283–97. https://doi.org/10.1007/s40520-018-1087-6.
Acknowledgements
Funding
This study was funded by Eli Lilly. The study sponsor also funded the journal’s Rapid Service Fee.
Medical Writing Assistance
Medical writing assistance was provided by Loraine Georgy, PhD, an employee of Analysis Group, Inc. which received consulting fees from the study sponsor to conduct this research, and by Gloria DeWalt, PhD, who was an employee of Analysis Group, Inc. at the time this study was conducted. The NACC database is funded by NIA/NIH Grant U01 AG016976. NACC data are contributed by the NIA-funded ADCs: P30 AG019610 (PI Eric Reiman, MD), P30 AG013846 (PI Neil Kowall, MD), P30 AG062428-01 (PI James Leverenz, MD), P50 AG008702 (PI Scott Small, MD), P50 AG025688 (PI Allan Levey, MD, PhD), P50 AG047266 (PI Todd Golde, MD, PhD), P30 AG010133 (PI Andrew Saykin, PsyD), P50 AG005146 (PI Marilyn Albert, PhD), P30 AG062421-01 (PI Bradley Hyman, MD, PhD), P30 AG062422-01 (PI Ronald Petersen, MD, PhD), P50 AG005138 (PI Mary Sano, PhD), P30 AG008051 (PI Thomas Wisniewski, MD), P30 AG013854 (PI Robert Vassar, PhD), P30 AG008017 (PI Jeffrey Kaye, MD), P30 AG010161 (PI David Bennett, MD), P50 AG047366 (PI Victor Henderson, MD, MS), P30 AG010129 (PI Charles DeCarli, MD), P50 AG016573 (PI Frank LaFerla, PhD), P30 AG062429-01(PI James Brewer, MD, PhD), P50 AG023501 (PI Bruce Miller, MD), P30 AG035982 (PI Russell Swerdlow, MD), P30 AG028383 (PI Linda Van Eldik, PhD), P30 AG053760 (PI Henry Paulson, MD, PhD), P30 AG010124 (PI John Trojanowski, MD, PhD), P50 AG005133 (PI Oscar Lopez, MD), P50 AG005142 (PI Helena Chui, MD), P30 AG012300 (PI Roger Rosenberg, MD), P30 AG049638 (PI Suzanne Craft, PhD), P50 AG005136 (PI Thomas Grabowski, MD), P30 AG062715-01 (PI Sanjay Asthana, MD, FRCP), P50 AG005681 (PI John Morris, MD), P50 AG047270 (PI Stephen Strittmatter, MD, PhD).
Author Contributions
Julie Chandler, Kevin Biglan, Mihaela Georgieva, Urvi Desai, and Noam Kirson contributed to the study design. Formal analyses were conducted by Henry Lane, Ben Westermeyer, and Hoi Ching Cheung. All authors contributed to the critical interpretation of data as well as drafting/editing the manuscript, have approved the final version of this manuscript, and take responsibility for the integrity of this research study.
Disclosures
Julie Chandler and Kevin Biglan are employees of Eli Lilly and minor stockholders. Mihaela Georgieva, Urvi Desai, Noam Kirson, and Henry Lane are employees of Analysis Group, Inc., which received consulting fees from the study sponsor to conduct this research. Hoi Ching Cheung and Ben Westermeyer were employees of Analysis Group, Inc. at the time this study was conducted. Hoi Ching Cheung is currently a Regional Associate with Clinton Health Access Initiative, Inc. Ben Westermeyer is pursuing doctoral studies in statistics at University of Washington.
Compliance with Ethics Guidelines
Data were de-identified and compliant with the patient confidentiality requirements of the Health Insurance Portability and Accountability Act; as a result, approval from an ethics committee was not required.
Data Availability
The datasets analyzed during the current study are not publicly available, as they are subject to a data use agreement between Analysis Group, Inc., and the National Alzheimer’s Coordinating Center (NACC). Information about the data used in this study, including detailed descriptions and the process for obtaining them, is available at https://www.alz.washington.edu/.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Chandler, J., Georgieva, M., Desai, U. et al. Disease Progression and Longitudinal Clinical Outcomes of Lewy Body Dementia in the NACC Database. Neurol Ther 12, 177–195 (2023). https://doi.org/10.1007/s40120-022-00417-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40120-022-00417-w