
Abstract
Introduction
Infection with hepatitis A virus (HAV) is often asymptomatic in young children, but most adolescents and adults will have symptoms ranging from nausea and tiredness to acute liver failure and even death. The risk of severe disease is higher in older adults and people with pre-existing liver disease. Immunization is recommended in regions with low HAV endemicity levels, i.e., where people get infected later in life. In the Philippines, recent epidemiologic data on HAV infection are lacking. The objective of this study was to assess age-specific seroprevalence and evaluate risk factors associated with HAV seropositivity.
Methods
People from two geographic areas (urban and rural) were recruited/enrolled and stratified by age group. HAV-specific immunoglobulin G (IgG) antibodies were measured with a chemiluminescent microparticle immunoassay. Sociodemographic parameters, hepatitis medical history, disease knowledge, hygiene measures and sanitation were assessed via a purpose-made questionnaire. Age at midpoint of population immunity (AMPI) was estimated using Kaplan-Meier curves. Logistic regression analyses were carried out to determine factors that were statistically significantly associated (p < 0.05) with HAV seropositivity.
Results
Overall, 1242 participants were included in the analysis; 250/602 (41.5%) participants from urban regions and 283/640 (44.2%) participants from rural regions tested positive for HAV IgG antibodies. AMPI was 35 and 37 years for the rural and urban region, respectively. Higher education was associated with lower HAV seropositivity prevalence ratios, while not living in the same region for the last 5 years, regularly consuming street food and lack of handwashing after defecation were associated with a higher likelihood of HAV seropositivity.
Conclusion
Results suggest that HAV endemicity is low in the Philippines. Factors associated with HAV seropositivity were traveling, consuming street food and lack of basic hygienic gestures. Immunization might be an option to protect vulnerable populations against severe hepatitis A disease.
Plain Language Summary
Hepatitis A virus (HAV) is transmitted via the fecal-oral route through consumption of contaminated food or water or by close contact with an infected person. In children, HAV is usually of no concern, but in adults and people with existing liver disease, HAV infection can lead to severe symptoms and even death. In areas where most people get hepatitis during childhood (high endemicity), vaccination is not required, since people acquire life-long immunity after infection. In regions with low and intermediate HAV endemicity, people may remain at risk of infection later in life and vaccination could be considered to prevent severe HAV disease and its associated complications. In the Philippines, the current endemicity level is unknown. The goal of this study was to determine the endemicity level in the Philippines and to determine risk factors for HAV infection. We measured the proportion of people (by age group) who had previously been infected with HAV. Results showed that by age of 5 years < 20% of the study population was infected by HAV. By the age of 37 years in the urban population and 35 years in the rural population, 50% of people tested positive for HAV antibodies, indicating previous infection. This means that the Philippines has low HAV endemicity. Risk factors for HAV seropositivity were traveling, regularly eating street food and not washing hands after defecation. Vaccination against HAV might be of benefit in the Philippines, especially early in life to prevent most severe outcomes in adulthood.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? | |
Hepatitis A virus (HAV) can lead to severe hepatitis, especially in older age groups and people with pre-existing liver disease | |
The benefit of HAV vaccination depends on age-specific seroprevalence and endemicity level in a given region | |
The goal of the study was to determine seroprevalence in the Philippines in two distinct regions (urban and rural) | |
What was learned from the study? | |
The average seroprevalence is 41.5% and 44.2% in urban and rural regions, respectively | |
The age at midpoint of population immunity (AMPI) is 35 and 37 years for the rural and urban region, respectively | |
HAV endemicity is low in the Philippines; immunization strategies could be envisaged to protect vulnerable populations against severe HAV disease |
Introduction
Hepatitis A is an infectious disease caused by the hepatitis A virus (HAV), which is an RNA virus belonging to the picornavirus family, and infects primarily humans as its only natural host [1]. HAV is transmitted primarily by the fecal-oral route, through either close contact with infected individuals or ingestion of contaminated food and water. Infected individuals may develop symptoms of hepatitis, including fever, malaise, abdominal discomfort, diarrhea, loss of appetite, dark-colored urine and jaundice [2, 3]. While young children often remain asymptomatic, most older children and adults will develop symptoms [2, 4, 5]. HAV infection does not cause chronic liver disease; however, in rare cases, acute liver failure occurs, and a small proportion of patients die from fulminant hepatitis [6]. Risk factors for severe disease are older age (> 40 years) and pre-existing liver conditions [6]. Case fatality rate increases from 0.1% in children < 15 years of age to 1.8–5.4% in individuals ≥ 50 years old [2].
The global burden of hepatitis A disease was estimated at 159 million acute infections and 39,000 deaths in 2019 [5, 7]. The highest burden was observed in low- to middle-income countries, in particular in Southeast Asia, where 42 million acute hepatitis A cases and 24,000 deaths were reported, corresponding to 60% of deaths worldwide [5].
HAV survives several weeks outside of its host and is highly resistant to environmental conditions [5]. Contaminated drinking water or food processed under non-hygienic conditions represents a common source of infection. After HAV infection, people develop virus-specific antibodies that confer life-long immunity. The presence of HAV-specific immunoglobulin G (IgG) antibodies can be easily measured, and age-specific seroprevalence is used to categorize regions into endemicity levels [8]. The latter have been defined by the World Health Organization (WHO) as high: ≥ 90% seroprevalence by the age of 10 years; intermediate: ≥ 50% seroprevalence by the age of 15 years; low: ≥ 50% seroprevalence by the age of 30 years, respectively [5].
Due to improved sanitation and access to clean drinking water, hepatitis A infection in children has decreased worldwide, including in Southeast Asia, leading to an epidemiologic shift from high to intermediate or low endemicity [9,10,11]. Therefore, the proportion of adolescents and adults susceptible to HAV infection increases in regions with intermediate to low endemicity [8, 9, 11,12,13]. The downside of this trend is increased morbidity and mortality due to a more severe disease course in older age groups [14]. For example, in the US, incidence of HAV infection declined between 1999 to 2011 from 6.0/100,000 people to 0.4/100,000 people [15]. At the same time, mean age at HAV infection increased from 36.0 to 45.1 years, and the proportion of people being hospitalized increased from 7.3 to 24.5%. These numbers emphasize the risk of hepatitis A outbreaks in intermediate/low endemicity regions and the need for specific vaccination strategies considering local endemicity and risk factors [16].
Tailoring preventive strategies against HAV infection requires current knowledge of region-specific endemicity levels and risk factors for HAV infection. In the Philippines, surveillance of hepatitis A disease is not mandatory, and seroprevalence data are scarce [12]. A seroprevalence study carried out in 1996 in Metro Manila showed that 42% of inhabitants were seropositive before the age of 15 years, and ≥ 50% were seropositive before the age of 20 years, corresponding to an intermediate-endemicity status [17]. This pattern has likely changed in the last 2 decades, similar to shifts reported in other countries of the Southeast Asian region [10,11,12].
The objective of this study was to assess age-specific HAV seroprevalence in the Philippines in two distinct geographic regions and to identify associations between sociodemographic parameters and HAV seroprevalence.
Methods
This was a cross-sectional, observational study to determine age-specific HAV IgG seroprevalence in inhabitants of the Philippines. The primary objective was to determine age-specific prevalence of HAV infection. Other objectives were to calculate the age at midpoint of population immunity (AMPI), i.e., the age at which 50% of the population has been infected with HAV. A secondary objective was to evaluate the association with known risk factors with HAV infection.
Two distinct geographic areas were selected, one rural and one urban, to obtain a representative estimate of the national seroprevalence.
Lumban municipality in the province of Laguna was selected as the rural site. Subjects were recruited from 14 Barangays. Age-stratified enrollment was coordinated by study staff and community health officers responsible for the area.
For the urban area, mass invitations were sent via a single institution, the UERM Memorial Medical Center located in Quezon City, which serves several cities and municipalities in Metro Manila and the Greater Manila area. A full list of cities considered by the recruitment process is provided in Supplementary information (SI) Table S1. To enhance recruiting into pre-specified age groups and increase the distribution of participants, community officials assisted in the recruitment process by inviting community members to participate in the study.
The study was conducted in accordance with the Declaration of Helsinki and Ethical Guidelines for Health-related Research Involving Humans, Council for International Organizations of Medical Sciences. The protocol and related documents were approved by the UERMMMCI Ethics Review Committee, and the protocol was registered in the Philippines Health Research Registry (PHRR211106-004046) [18].
Population
Children and adults aged 1 to 80 years, who had been residents in the selected geographic areas for ≥ 6 months, could be included in the study if they or their legal representative were willing to participate and to sign the informed consent form. Subjects who had specific medical conditions that would put them at risk during the study were excluded, such as subjects with contraindication for blood drawing, recipients of blood-derived products, and those with immunodeficient conditions, terminal or psychiatric illness. Only one subject from the same household could be enrolled. A full list of inclusion and exclusion criteria is provided in SI.
The study population was stratified into 11 pre-defined age groups based on WHO categories for hepatitis A endemicity study age groups (1–2, 3–4, 5–9, 10–14, 15–19, 20–24, 25–29, 30–34, 35–39, 40–49, ≥ 50 years) [5].
Outcomes
The primary outcome was HAV immune status. HAV-specific IgG antibodies in peripheral blood samples were measured with a Food and Drug Administration-approved, validated serologic test using a chemiluminescent microparticle immunoassay (CMIA, Abbot Architect) [19]. Test results are interpreted according to a system-specific calibration cutoff to be either reactive for HAV IgG antibodies (signal to cutoff ratio ≥ 1.00) or unreactive (signal to cutoff ratio < 1.00) [19].
Exposure was derived from participant’s age at enrollment. Additional outcomes were collected with a purpose-built questionnaire that had to be completed by participants or the legal guardian of participants with the help of trained interviewers. The questionnaire consisted of 44 questions divided into five sections including (1) sociodemographic information, (2) knowledge of disease, (3) past medical history of hepatitis, (4) drinking water safety and (5) hygiene food intake (SI). Questions were based on published risk factors for HAV infection, the WHO and United Nations Children’s Fund (UNICEF) questionnaire ‘Core questions on drinking-water and sanitation for household surveys’ and the water/sanitation, assets, maternal education and income (WAMI) index [6, 20, 21]. During the pilot phase, study interviewers were trained, and potential issues related to formulation or translation to the local language were identified. Interviewers were instructed to read the questions in a way to reduce induction bias, i.e., without suggesting a given response.
Blood Sample Collection and Processing
Peripheral blood samples were collected from study participants by skilled study staff in serum-gel or EDTA tubes. Samples were labeled and registered by the study field coordinator. All samples were refrigerated at 4 °C until they were transported on ice to the designated central laboratory and processed within 36 h from sample collection. Blood samples were processed according to local laboratory standardized procedures, and serum could be stored at − 20 °C up to 3 months until HAV IgG antibody testing.
Data Management
Interviewers used a standardized paper-based questionnaire to collect participants’ responses in the field. Individual results were entered into a centralized database in an anonymized fashion using a unique participant identification code. Data were entered in duplicate, and internal quality checks were put in place to avoid typing errors and to ensure consistency of data capture.
Sample Size
Sample size was determined based on age-specific seroprevalence data obtained in Thailand between 1999 and 2004 and assuming that this country is ahead of a general endemic shift to lower HAV infections observed in Southeast Asia [11]. Precision was set to 5% for prevalence estimates ≤ 10% and to 10% for higher prevalence estimates together with 90% confidence intervals (CIs). The population pyramid of the Philippines was considered in conjunction with pre-specified age groups to determine the sample size for each age group required to obtain the seroprevalence estimate at the desired precision. For each region, the calculated sample size was 572 participants requiring 640 participants to be enrolled assuming an attrition rate of 10% (Table S2). A stopping rule was applied to each age group in case a sufficient number of participants had been enrolled.
The sample size was adequate to assess the strength of association between selected factors and HAV seropositivity with a statistical power of 80% and 95% CIs.
Statistical Analysis
Descriptive statistics were used to calculate seroprevalence by age group. Classification of HAV endemicity according to WHO criteria were used for interpretation of results: high: > 90% seropositivity by the age of 10 years; intermediate: seroprevalence ≥ 50% by the age of 15 but < 90% by the age of 10 years; low: seroprevalence ≥ 50% by the age of 30 but < 50% by the age of 15 years; very low: < 50% by the age of 30 years [5].
Kaplan-Meier analysis was used to determine AMPI overall and for each geographical region. A statistical comparison between urban and rural AMPI scores was done using chi-square test.
Descriptive statistics were used to summarize participants’ responses to the purpose-made questionnaire. Statistical significance of differences between urban and rural regions was assessed using chi-square or Fisher’s exact test.
Bivariate and multivariate analyses were carried out to determine whether there was a statistically significant association between risk factors for HAV infection and past (current) exposure to HAV. The strength of association was first estimated with univariate log-binomial models. Factors showing a potential association with HAV exposure (p < 0.20) were subsequently included in multivariate log-binomial models. Logistic regression analysis with backward elimination using Wald’s test and likelihood ratio test (p < 0.05 for both tests) was used to build the final model. Prevalence ratios and 95% CIs were calculated for variables that reached statistical significance.
Results
Overall, 1242 participants were included in the analysis, 602 participants from urban areas and 640 from rural regions.
Sociodemographic characteristics were significantly different between rural and urban populations in terms of education, years of schooling of the mother, profession, number of habitable rooms and building materials used on walls and floors (Table 1). Age and gender distribution were similar.
Components of the WAMI index were statistically significantly different between rural and urban populations (Table 2). Maximum score in water sanitation was observed for 99.5% of participants in urban areas compared with 90.8% in rural regions. The average number of household assets (i.e., refrigerator, bank account, iron, desktop/laptop, radio, sofa, sewing machine) was higher for participants living in cities compared to their rural counterparts. Maternal education and income were significantly lower in rural areas compared with city dwellers.
HAV Seroprevalence
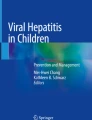
Overall prevalence of HAV seropositivity was 41.5% for urban and 44.2% for rural regions. None of the participants tested positive for HAV IgM antibodies, suggesting no active or recent infection (Table 3). HAV IgG seropositivity increased with increasing age in both regions; however, seroconversion followed a different pattern showing higher seroprevalence in urban areas in younger age groups (up to 19 years) and higher seroprevalence in rural regions in older age groups (20 years and older) (Fig. 1).

HAV seroprevalence by age group. HAV, hepatitis A virus; IgG, immunoglobulin G; y, years
AMPI
In the overall population, estimated AMPI was 36 years. Region-specific AMPIs were 35 and 37 years in the rural and urban populations, respectively (Fig. 2). The difference in AMPI between regions was not statistically significant (p = 0.8840).

Kaplan-Meier curves for AMPI, overall (A) and by region (B). CI, confidence interval; AMPI, age at midpoint of population immunity
Risk Factors
Responses from each section of the participants’ questionnaire were compared between rural and urban regions to identify differences in potential risk factors for HAV infection between urban and rural regions. For each response section of the questionnaire, factors that were statistically significantly associated with HAV IgG seropositivity were identified through multivariate logistic regression analysis.
Sociodemographic Parameters
Statistically significant differences in sociodemographic parameters between the two geographic regions have been presented above and are summarized in Table 1.
Upon multivariate regression analysis, age group and education were statistically significantly associated with HAV seropositivity. Taking the 1–2-year age group as reference, seroprevalence was significantly lower in the 3–4-year age group and significantly higher in the ≥ 20–24-year age groups (Fig. 3).

Factors Correlating with HAV seropositivity—final logistic regression model. CI, confidence interval; HAV, hepatitis A virus; p, p-value; y, year
Higher education level was associated with lower prevalence ratios, reaching statistical significance for graduate/post-graduate education (prevalence ratio regarding middle school: 0.21, 95% CI 0.05, 0.66, p = 0.004) (Fig. 3).
Hepatitis-related Medical History
Few participants reported a medical history of hepatitis, but those who did were more likely to live in cities (Table S3). A higher proportion of rural participants lived in the same area over the previous 5 years compared with their urban peers (93.1% vs 84.0%). More urban participants claimed to be vaccinated against HAV compared with rural participants (102 vs 2 participants in the urban and rural area, respectively). Among urban participants, vaccination could be confirmed in 25/102 (24.5%) participants based on vaccination cards (Table S3). Among those with confirmed vaccination, 92% were reactive to IgG anti-HAV. In the rural areas, among the two individuals who claimed to be vaccinated, only one was confirmed and non-reactive to IgG anti-HAV. Based on combined urban and rural data, 41% of people with unconfirmed HAV vaccination were reactive to IgG anti-HAV compared with 88.5% of confirmed vaccination cases.
In multivariate regression analysis, two variables were shown to be statistically significantly related to HAV seropositivity (p < 0.05): people who have not lived in the same region during the past 5 years had a 1.41-fold higher prevalence (95% CI 1.19, 1.62); on the other hand, people who had no confirmed HAV vaccination had a lower prevalence (prevalence ratio regarding vaccinated: 0.77; p = 0.008) (Fig. 3).
Water Safety Access
There were statistically significant differences between urban and rural regions regarding water sources used for drinking water and other purposes (Table S4). Most participants from urban regions used bottled water (81.2%) and piped water into dwellings (18.1%) for drinking water, while in rural regions, participants used mainly bottled water (34.4%) and tubewells/bore holes (30.8%). Most sources were considered improved in both regions according to WHO standards [22]. In urban areas, most participants used water piped into the dwelling (97.8%) for other purposes, while in rural regions different sources were used for non-drinking water (tubewell/bore hole: 43.4%; water piped into dwelling: 24.7%; public tap/standpipe: 15.1%; protected dug well: 12.3%).
Pour-flush toilets were the most common type of facilities used (65.4% and 96.9% in urban and rural areas, respectively). Approximately a third of urban dwellers had flush toilets. Most toilets flushed into a septic tank. Flush/pour was considered improved according to WHO criteria in 99.7% and 94.4% of urban and rural households, respectively.
In the multivariate logistic regression model, only the presence of improved flush/pour was associated with HAV seropositivity; prevalence ratio in households using unimproved pour/flush was 0.42 (95% CI 0.21, 0.78; p < 0.003) (Fig. 3).
Hygienic Food Intake Practices
Significant differences were observed in all aspects of food preparation and intake between urban and rural regions (Table S5).
A dedicated surface for preparing food was available in most urban households (78.5%) but less common in rural places (45%). Meals were mostly taken at home in both urban and rural areas, and street food was only occasionally consumed. Washing of hands prior to food handling, eating and after defecation was more strictly applied in urban than rural regions. Overall, most people responded that they washed their hands ‘always’ or ‘most of the time’ before handling or eating food and after defecation. In urban areas, kitchens were more likely to be free of insects and rodents according to participant responses.
In multivariate analyses, regular street food consumption (‘always’) was associated with an increase in prevalence ratio vs no street food consumption (prevalence ratio = 1.72; 95% CI 1.31, 2.03; p < 0.001). Washing hands after defecation most of the time (rather than always) was associated with higher prevalence of HAV seropositivity (prevalence ratio = 1.33; 95% CI 1.07, 1.59; p < 0.013) (Fig. 3).
Knowledge about Hepatitis A Disease
Knowledge about hepatitis A differed significantly between urban and rural areas (Table S6).
More participants from urban regions indicated having heard of hepatitis A compared with those in rural regions (80.6% vs 45.9%). Among these participants, 56.7% and 44.2% of urban and rural participants correctly identified hepatitis as a communicable disease. More than 70% of respondents knew that it could be transmitted by contaminated food and water. Classic symptoms associated with hepatitis A, which were known by > 50% of participants in both geographic areas, included yellowish discoloration of eyes, fever, abdominal pain and dark tea-colored urine. Approximately 45% of participants overall thought that a vaccine against HAV was available in the Philippines, while 15.4% of urban participants and 23.8% of rural participants believed that no HAV vaccine was available in the Philippines.
Upon multivariate regression analysis, knowledge regarding hepatitis A transmission was associated with HAV seropositivity: prevalence ratio was lower in participants not knowing that the disease was communicable (prevalence ratio: 0.75; 95% CI 0.58, 0.93; p = 0.007) and in those that identified ‘talking to the ill’ as a risk factor for contagion (prevalence ratio: 0.80; 95% CI 0.66, 0.96; p = 0.015) (Fig. 3).
Discussion
In 1996, the Philippines had intermediate HAV endemicity with more than half of people being seropositive at the age of 20 years [17]. Recent epidemiologic data on hepatitis A disease for the Philippines are lacking. Results from this study showed a shift in seroconversion towards older age groups (median age at conversion: 36 years), suggesting that the Philippines has transitioned to a low HAV endemicity level as observed in other Southeast Asian countries [10, 23].
Several East Asian countries have witnessed a shift in hepatitis A epidemiology to intermediate/low endemicity. In Thailand, AMPI increased from 4.5 years in 1971 to 42.0 years in 2014 [11]. Recent cross-sectional studies carried out in Laos, Indonesia, Vietnam and the Philippines also pointed towards an increase in age at seroconversion compared with earlier studies [23,24,25].
In this study, age-specific seroprevalence showed a distinct pattern depending on geographic location: seroprevalence was lower in rural regions compared with urban areas in young age groups up to 19 years, but it was higher in older age groups. Rural to urban migration may have confounded age-specific seroprevalence by region and artificially increased seroprevalence rates in urban regions. Indeed, not living in the same region during the last 5 years significantly correlated with seroprevalence. Another explanation might be that urban children are more likely to receive vaccination and in turn be reactive for HAV IgG antibodies. However, due to the limited number of participants with confirmed vaccination status, this hypothesis could not be confirmed based on our study results. Importantly, both regions witnessed an increase in age at seroconversion, pinpointing the important sanitary improvements achieved in recent decades. A recent report showed that as of 2019, 91% of the Philippine population has access to basic sanitation services, up from 68% in 2000 [26]. The AMPI was similar in rural and urban regions (median age at conversion: 35 and 37 years, respectively), confirming the low endemicity status. Several sociodemographic factors and behaviors in hygiene and food preparation/consumption were associated with HAV seroprevalence.
Several studies have shown that hepatitis A endemicity correlated with socioeconomic factors, with high endemicity observed in developing countries and low endemicity in high-income countries [8, 12, 13, 27]. Socioeconomic status is linked to access to clean drinking water and sanitation, educational level and income. Besides age group, factors that statistically significantly correlated with seroprevalence in this study were educational level, disease knowledge, living in the same area for the last 5 years, vaccination status, street food consumption and hygienic factors (washing hands after defecation and improved pour/flush toilets). The impact of eating habits and observation of hygienic gestures corroborates the fecal-oral route of HAV transmission. HAV-contaminated food or water represents the main source of infection and may lead to hepatitis A outbreaks even in regions with low endemicity [28]. The increased seroprevalence observed in people who moved during the last 5 years is likely due to an increased risk of transmission for travelers to endemic regions [14, 29]. Educational level and disease knowledge are indicators of socioeconomic status, access to clean water and sanitation, and awareness of disease transmission. In this study, people with the lowest seroprevalence ratio had a graduate or postgraduate degree in agreement with other studies reporting lower seroprevalence in people with higher educational level [30,31,32]. However, some factors appeared counterintuitive; for example, people knowing that hepatitis was a communicable disease had a higher prevalence ratio. This result suggests that disease knowledge is not sufficient to prevent infection but needs to be accompanied by supportive actions. Finally, vaccination status also correlated with HAV IgG positivity. Most people who received hepatitis A vaccines will have detectable HAV-specific IgG antibodies, even years after vaccination; therefore, seroprevalence is higher in the vaccinated population compared with unvaccinated individuals [5, 33].
In regions with low endemicity, a sizeable proportion of adolescents and adults remains susceptible to HAV infection, which may lead to hepatitis A outbreaks often linked to more severe disease and increased healthcare resource use [34, 35]. This situation leads to the so-called paradox of hepatitis A epidemiology where disease burden is higher in low endemicity regions [5, 14]. Hepatitis A is a vaccine-preventable disease; both inactivated and live attenuated vaccines exist, which are highly immunogenic and well tolerated [33]. Immunization strategies vary across countries from partial immunization programs in high-risk groups to universal childhood immunization [36]. Vaccination is not recommended in high-endemicity regions; however, in countries with intermediate to low endemicity, WHO recommends universal childhood immunization if there is (1) an increase of acute and/or severe hepatitis A cases, including adolescents and adults, (2) a shift in epidemiology from high to intermediate endemicity and (3) if cost-effectiveness analyses favor introduction of universal hepatitis A vaccination. While results from this study demonstrated a shift in endemicity in the Philippines, the study did not assess the incidence of acute cases and healthcare resource use due to hepatitis A disease. Future studies are required to monitor HAV-related healthcare resource use and hepatitis-related burden of disease. Such information may inform cost-effectiveness models to estimate the value of hepatitis A vaccination in the Philippine context. In Indonesia, which experienced a similar shift in hepatitis A epidemiology, cost-effectiveness analysis suggested that universal childhood hepatitis A immunization would be cost-effective [37].
There are several limitations to this study. Findings are based on an age-stratified convenience sample from two geographic regions, and this might limit generalizability to the entire Philippine population. People could refuse to participate in the study, and this could have led to selection bias. However, the implication of community health officers from different Barangay(s) in the enrollment of participants and the use of mass invitations in urban areas ensured inclusion of participants with diverse sociodemographic backgrounds. Networking and collaborations among governing medical institutions and regional health offices aimed at increasing diversity among enrolled subjects thereby improving generalizability of results.
Some questions asked for information that could be perceived as sensitive or embarrassing by of participants, such as income, eating habits and hygienic behavior. This may have led to response bias or measurement error since participants might be inclined to provide more socially acceptable answers [38]. Finally, documentation of vaccines received was often missing, and vaccination status might be underreported.
Conclusion
An epidemiologic shift has occurred in the Philippines towards low HAV endemicity. People tend to get infected later in life leaving a large proportion of adolescents and adults at risk of infection and potentially more severe disease. Risk factors for HAV infection include frequent traveling, consumption of street food and insufficient hygienic measures. Vaccination strategies against HAV should be considered early in life to prevent hepatitis A outbreaks and severe disease in high-risk groups.
Data Availability
Additional data are available via the Supplemental Material. Requests for the anonymized aggregated database can be directed to GSK and UERMMMCI via a formal request to the corresponding author.
References
McKnight KL, Lemon SM. Hepatitis A virus genome organization and replication strategy. Cold Spring Harb Perspect Med. 2018;8(12).
Lemon SM, Ott JJ, Van Damme P, Shouval D. Type A viral hepatitis: a summary and update on the molecular virology, epidemiology, pathogenesis and prevention. J Hepatol. 2017;S0168-8278(17)32278-X.
Shin EC, Jeong SH. Natural history, clinical manifestations, and pathogenesis of hepatitis A. Cold Spring Harb Perspect Med. 2018;8(9).
Hollinger FB, Bell B, Levy-Bruhl D, Shouval D, Wiersma S, Van Damme P. Hepatitis A and B vaccination and public health. J Viral Hepat. 2007;14(Suppl 1):1–5.
World Health Organization. WHO position paper on hepatitis A vaccines–october 2022. Wkly Epidemiol Rec. 2022;40(97):493–512.
Thébault A, Roque-Afonso A-M, Kooh P, Cadavez V, Gonzales-Barron U, Pavio N. Risk factors for sporadic hepatitis A infection: a systematic review and meta-analysis. Microb Risk Anal. 2021;17:100155.
The Institute for Health Metrics and Evaluation. Global Burden of Disease Study 2019. 2019 [cited 2023 July]. Available from: https://ghdx.healthdata.org/gbd-2019
Melnick JL. History and epidemiology of hepatitis A virus. J Infect Dis. 1995;171(Supplement 1):S2–8.
Mohd Hanafiah K, Jacobsen KH, Wiersma S. Challenges to mapping the health risk of hepatitis A virus infection. Int J Health Geograph. 2011;10(57).
Barzaga BN. Hepatitis A shifting epidemiology in South-East Asia and China. Vaccine. 2000;18(Suppl 1):S61–4.
Sa-nguanmoo P, Posuwan N, Vichaiwattana P, et al. Declining trend of Hepatitis A seroepidemiology in association with improved public health and economic status of Thailand. PLoS One. 2016;11(3): e0151304.
Gripenberg M, Aloysia D’Cor N, L’Azou M, Marsh G, Druelles S, Nealon J. Changing sero-epidemiology of hepatitis A in Asia Pacific countries: a systematic review. Int J Infect Dis. 2018;68:13–7.
Jacobsen KH, Wiersma ST. Hepatitis A virus seroprevalence by age and world region, 1990 and 2005. Vaccine. 2010;28(41):6653–7.
Chakravarti A, Bharara T. Epidemiology of Hepatitis A: past and current trends. In: Streba C, editor. Hepatitis A and Other Associated Hepatobiliary Diseases: IntechOpen; 2019.
Ly KN, Klevens RM. Trends in disease and complications of hepatitis A virus infection in the United States, 1999–2011: a new concern for adults. J Infect Dis. 1015;212(2):176–82.
Chi V, Cleary S, Bocchini JAJ. In pursuit of control and elimination: update on hepatitis A and B epidemiology and prevention strategies. Curr Opin Pediatr. 2018;30(5):689–97.
Barzaga NG, Florese RH, Roxas JR, Francisco ZT. Seroepidemiology of hepatitis A virus among filipinos living in selected communities in and around metro manila. Philip J Microbiol Infect Dis. 1996:39–47.
Philippine Health Research Registry. Seroprevalence of hepatitis A in 3 South East Asian countries: Indonesia, Philippines and Vietnam. 2021 [cited 2023 June]. Available from: https://registry.healthresearch.ph/index.php/registry?view=research&layout=details&cid=4046
Abbott Laboratories. ARCHITECT System—HAVAb-IgG 2004 [cited 2023 Jan]. Available from: https://www.ilexmedical.com/files/PDF/HAVAb-IgG_AEC.pdf
Ariyarathna N, Abeysena C. Risk factors for viral hepatitis A infection in Gampaha District, Sri Lanka: an unmatched case control study. BMC Public Health. 2020;20(1):357.
World Health Organization, United Nations Children's Fund (UNICEF). Core questions on drinking-water and sanitation for household surveys. In: Organization WH, editor. UNICEF. WHO, Geneva. 2006.
World Health Organization. Improved sanitation facilities and drinking-water sources: WHO. 2023 [cited 2023 June]. Available from: https://www.who.int/data/nutrition/nlis/info/improved-sanitation-facilities-and-drinking-water-sources
Hernandez-Suarez G, Saha D, Lodrono K, et al. Seroprevalence and incidence of hepatitis A in Southeast Asia: a systematic review. PLoS One. 2021;16(12): e0258659.
Khounvisith V, Xaiyaphet X, Chanthavilay P, et al. Hepatitis A virus in Lao people’s democratic Republic: seroprevalence and risk factors. Am J Trop Med Hyg. 2020;103(1):164–8.
Kwon JC, Chang HY, Kwon OY, et al. Seroepidemiology of hepatitis viruses and hepatitis B genotypes of female marriage immigrants in Korea. Yonsei Med J. 2018;59(9):1072–8.
Global Council for the promotion of interanational trade (GCPIT). Improving water, sanitation, and hygiene in Philippines: challenges, solutions, and entrepreneurial opportunities 2023 [cited 2023 Sep]. Available from: https://gcpit.org/improving-water-sanitation-and-hygiene-in-philippines-challenges-solutions-and-entrepreneurial-opportunities/#:~:text=As%20of%202019%2C%2091%25%20of,up%20from%2087%25%20in%202000.
Jacobsen KH, Koopman JS. The effects of socioeconomic development on worldwide hepatitis A virus seroprevalence patterns. Int J Epidemiol. 2005;34(3):600–9.
Fore AE. Hepatitis A Transmitted by food. Clin Infect Dis. 2004;38:705–15.
Balogun O, Brown A, Angelo KM, et al. Acute hepatitis A in international travellers: a GeoSentinel analysis, 2008–2020. J Travel Med. 2022;29(2):taac013.
Merat S, Rezvan H, Nouraie M, et al. Seroprevalence and risk factors of hepatitis A virus infection in Iran: a population based study. Arch Iran Med. 2010;13(2):99–104.
Ayouni K, Kharroubi G, Mallekh R, et al. Seroprevalence of hepatitis A virus infection in Central-West of Tunisia. J Med Virol. 2021;93(6):3666–71.
de Alencar Ximenes RA, Martelli CM, Merchan-Hamann E, et al. Multilevel analysis of hepatitis A infection in children and adolescents: a household survey in the Northeast and Central-west regions of Brazil. Int J Epidemiol. 2008;37(4):852–61.
Herzog C, Van Herck K, Van Damme P. Hepatitis A vaccination and its immunological and epidemiological long-term effects - a review of the evidence. Hum Vaccin Immunother. 2021;17(5):1496–519.
Hofmeister MG, Yin S, Aslam MV, Teshale EH, Spradling PR. Hepatitis A hospitalization costs, United States, 2017. Emerg Infect Dis. 2020;26(5):1040–1.
Guzman-Holst A, Luna-Casas G, Burguete Garcia A, et al. Burden of disease and associated complications of hepatitis a in children and adults in Mexico: a retrospective database study. PLoS One. 2022;17(5):e0268469.
Zhang L. Hepatitis A vaccination. Hum Vaccin Immunother. 2020;16(7):1565–73.
Suwantika AA, Beutels P, Postma MJ. Cost-effectiveness of hepatitis A vaccination in Indonesia. Hum Vaccin Immunother. 2014;10(8):2342–9.
Tourangeau R, Yan T. Sensitive questions in surveys. Psychol Bull. 2007;133(5):859–83.
Funding
GlaxoSmithKline Biologicals SA funded this study (EPI-HAV-013 BOD APA SUPP—eTrack ID: 216938) and was involved in all stages of study conduct, including analysis of the data. GlaxoSmithKline Biologicals SA also covered all costs associated with the development and publication of this manuscript, including the journal’s Rapid Service Fee.
Author information
Authors and Affiliations
Contributions
Adriana Guzman-Holst, Gustavo Hernandez-Suarez, Maria Peñafrancia L. Adversario, Vinna Marie T. Quinones, Jangail C. Songco, Donaliz R. Garcia, Ma. Christina C. Blanco, Jacqueline D. Bernabe, Hyacinth Claire T. Chacon, Ronald Alvin C. Ascue, Jayme Natasha K. Paggao, Lous Ohsana P. Comendador, Josefina C. Carlos, Jennifer M. Nailes, Michelle G. Cacayorin, May Priscilla V. Cero, Ma. Paula Aleta Benedicto-Delfin, and Nadjah S. Natividad participated in the design or implementation or analysis, and interpretation of the study; and the development of this manuscript. All authors had full access to the data and gave final approval before submission.
Corresponding author
Ethics declarations
Conflict of Interest
Adriana Guzman-Holst and Gustavo Hernandez-Suarez are employed by and hold shares in GSK. These authors declare no other financial and non-financial relationships and activities. Maria Peñafrancia L. Adversario, Vinna Marie T. Quinones, Jangail C. Songco, Donaliz R. Garcia, Ma. Christina C. Blanco, Jacqueline D. Bernabe, Hyacinth Claire T. Chacon, Ronald Alvin C. Ascue, Jayme Natasha K. Paggao, Lous Ohsana P. Comendador, Josefina C. Carlos, Jennifer M. Nailes, Michelle G. Cacayorin, May Priscilla V. Cero, Ma. Paula Aleta Benedicto-Delfin and Nadjah S. Natividad declare no financial and non-financial relationships and activities and no conflicts of interest.
Medical Writing, Editorial and Other Assistance
The authors thank Dr. Sison for his involvement as scientific contributor who critically reviewed the study protocol and participated in data collection. The authors thank Dr. Rubi for valuable input during conception of the manuscript. The authors also thank Business & Decision Life Sciences Medical Communication Service Center for editorial assistance and manuscript coordination, on behalf of GSK. Katrin Spiegel, on behalf of GSK, provided medical writing support.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and Ethical Guidelines for Health-related Research Involving Humans, Council for International Organizations of Medical Sciences. The protocol and related documents were approved by the UERMMMCI Ethics Review Committee, and the protocol has been registered in the Philippines Health Research Registry (PHRR211106-004046).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Carlos, J.C., Quinones, V.M.T., Adversario, M.P.L. et al. Seroprevalence and Shifting Endemicities of Hepatitis A Virus Infection in Two Different Geographical Areas in the Philippines. Infect Dis Ther 13, 1019–1035 (2024). https://doi.org/10.1007/s40121-024-00955-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40121-024-00955-w