
Abstract
Introduction
Chronic pain (CP) and depression/anxiety often coexist, worsening each other's symptoms. Treating this comorbidity is challenging. Tricyclic antidepressants and serotonin noradrenaline reuptake inhibitors are the first-line treatment options for this comorbidity, although sometimes they are not effective and/or well tolerated by patients, and there is little clinical evidence that selective serotonin reuptake inhibitors are useful for controlling CP. The antidepressant vortioxetine, with a multimodal mechanism that may help reduce pain, has proven clinical efficacy in patients with major depressive disorder (MDD). This study investigated vortioxetine's effectiveness for MDD and CP in clinical practice.
Methods
This was a 3-month, multicenter, prospective, open-label, non-interventional pharmacoepidemiologic study. Patients (n = 64) with MDD (9-item Patient Health Questionnaire [PHQ-9] score ≥ 15) and CP (visual analogue scale [VAS] score ≥ 4) were treated with vortioxetine for 3 months (initiated with 10 mg/day, with flexible dosing thereafter [5–20 mg/day]). VAS, Clinical Global Impression (CGI), and Patient Global Impression (PGI) scales were used at baseline and at 1 and 3 months. Brief Pain Inventory (BPI), PHQ-9 scale, and Satisfaction with Medicines Questionnaire (SATMED-Q) were used at baseline and at 3 months. Adverse Events (AEs) were recorded. Descriptive statistics, chi-square tests, and Student's t-tests were used for paired data.
Results
MDD patients showed a statistically significant improvement in VAS from baseline (mean [standard deviation (SD)]: 7.42 [0.69]) to 1 month (mean [SD]: 6.1 [0.81], P < 0.001) and 3 months (mean [SD]: 5.09 [1.26], P < 0.0001). Similarly, BPI and PHQ-9 scores showed significant improvement from baseline (mean [SD]: 6.20 [0.80] and 16.63 [1.47], respectively) to 3 months (mean [SD]: 4.73 [0.98] and 7.30 [2.60], P < 0.0001, respectively). Patients showed clinical improvement with CGI and PGI scales and reported being satisfied with the treatment in the SATMED-Q. A few mild EAs were registered.
Conclusion
Vortioxetine can relieve depressive and pain symptoms, with a good safety profile, in patients with MDD and CP.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Why carry out this study? |
Chronic pain (CP) and depression frequently coexist as comorbidities that are challenging to treat |
Current treatments for depression associated with CP based on tricyclic antidepressants or serotonin noradrenaline reuptake inhibitors are sometimes not effective and/or not well tolerated; therefore, it is important to explore the efficacy and tolerability of novel therapeutic agents |
The antidepressant vortioxetine is effective in Major Depressive Disorder (MDD) and presents a new multimodal mechanism of action that could make it a good alternative treatment for patients with MDD and CP |
What was learned from the study? |
The treatment of vortioxetine and pain medication in patients with MDD and CP alleviates both CP and depressive symptoms, with a good safety profile and improvement in their quality of life |
Introduction
Chronic pain (CP) is defined as persistent or recurrent pain lasting > 3 months. This condition is a major source of suffering for patients and therefore requires specific management [1]. CP constitutes a stress state that is a critical factor in determining depression [2]. Thus, depression is considered one of the most frequent psychiatric complications in patients with CP [3, 4].
CP affects 20% of the global population [5]. Depression is one of the most disabling mental disorders worldwide and has been reported to be the third leading cause of the global burden of disease [6, 7]. The prevalence of pain in cohorts of patients with depression and of symptoms of serious depression in cohorts of patients with CP is higher than the prevalence of these two conditions individually [8]. Approximately 65% of patients with depression experience one or more pain complaints, whereas depression can be present in 5–85% of patients with CP, depending on the study setting [8].
Depression in patients with CP is associated with a reduced pain threshold, increased pain perception, greater functional limitations, and worse analgesic response [3]. Likewise, the presence of pain reduces the chance of recovery from depression and is related to more intense symptoms in these patients [8], including impaired sleep, enhanced anxiety, and impaired cognition [9]. Furthermore, in some cases, the presence of depression in patients with CP is a predictor of non-response to antidepressants [10]. Thus, this comorbidity exacerbates the symptoms of both conditions, making treatment more difficult and complicating the management of these patients. Furthermore, CP is considered a predictor of major depression and worsening of anxiety symptoms [11, 12], and the severity of depression and anxiety is also linked to a lack of response to the treatment [13]. Thus, a relationship has been found between the magnitude of pain complaints and the intensity of depressive and anxious manifestations [9, 11].
Of note, the neuronal pathways that are modulated in response to pain and mood disorders involve the same brain regions, including the insular cortex, prefrontal cortex, anterior cingulate, thalamus, hippocampus, and amygdala [14]. Similarly, both pain and depression have been associated with abnormalities in the levels of different substances, including brain-derived neurotrophic factor (BDNF), the neurotransmitters serotonin (5-hydroxytryptamine or 5-HT) and norepinephrine (NE; also known as noradrenaline, NA) [9], and disturbances in noradrenergic and serotonergic neurotransmission in the central nervous system [15]. These observations are consistent with the idea that there is an overlap between the mechanisms that support pain- and depression-induced neuroplasticity, which facilitates the development of CP-induced depression [2].
The mechanism of action of most antidepressants is based on the regulation of the neurotransmitters 5-HT and NE [8, 16]. Tricyclic antidepressants (TCAs) and serotonin noradrenaline reuptake inhibitors (SNRIs) are effective treatment options for patients with depression, anxiety, and other psychosomatic disorders [16]. At the same time, they have also been shown to be useful in the management of concomitant chronic and neuropathic pain [9, 15, 17, 18]. However, in a significant number of patients suffering chronic or neuropathic pain, these treatments have been shown to be ineffective [10, 13, 19]. In addition, some patients have poor tolerability to these two drug classes so, in these cases, selective serotonin reuptake inhibitors (SSRIs) are an alternative to obtain a good antidepressant response [17, 20]. However, SSRIs are not effective in the treatment of neuropathic pain [21].
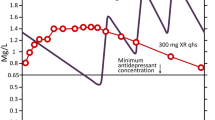
Vortioxetine (approved for marketing in Europe in 2013 and marketed as Brintellix®) is an antidepressant with a multimodal mechanism of action indicated for major depressive disorder (MDD) in adults. Its clinical efficacy has been demonstrated in the short and long term, with beneficial effects on affective [22], physical [23], and anxiety symptoms [24,25,26] and remarkable efficacy in improving cognitive dysfunction associated with unipolar depression [22, 27,28,29,30] and dementia [28]. Furthermore, vortioxetine has shown a good safety and tolerability profile, and unlike other antidepressants, it does not produce cardiovascular alterations, significant weight gain, or sexual dysfunction [31, 32]. However, its combination with opioids is not recommended to avoid the possibility of serotonergic syndromes. [33]. Likewise, several preclinical and clinical studies have recently demonstrated the effectiveness of vortioxetine in managing CP [15, 34,35,36,37], although more evidence is needed.
Vortioxetine inhibits the release of GABA, the main inhibitory neurotransmitter in the organism, through stimulation of the 5-HT1A receptors, and this secondarily triggers the release of dopamine (DA), noradrenaline (NA), histamine (HA), and acetylcholine (Ach) in the prefrontal cortex.
Vortioxetine binds with high affinity to the serotonin transporter (SERT, Ki 1.6 nM), thereby inhibiting its activity and increasing 5-HT levels. This is believed to be the principal mechanism underlying the antidepressant effects of vortioxetine and numerous other antidepressants [38]. Evidence suggests that serotonergic pathways are involved in the inhibitory control of pain, although the effect of 5HT on pain modulation in the spinal cord may be inhibitory or facilitatory, depending on which receptor subtypes are preferentially activated [3]. Vortiotexine also regulates multiple 5-HT receptor subtypes related to pain transmission at the same time: it exerts agonist action at 5-HT1A receptors (Ki = 15 nM), hastening its desensitization and making 5-HT release occur faster [39]; partial agonist action at 5-HT1B receptors (Ki = 33 nM) and antagonist action at 5-HT1D (Ki = 54 nM) and 5HT7 (Ki = 19 nM) receptors, inhibiting the serotonin release brake [39]; and antagonist action at 5HT3 (Ki = 3.7 nM) receptor, involved in 5HT-induced hyperalgesia [39, 40]. The multiple sites of action of vortioxetine also result in increased levels of dopamine (DA), NA, histamine (HA), and acetylcholine (Ach) [3]. In addition, pharmacological studies have shown that 5-HT7 receptors are involved in 5HT-induced analgesia, while 5-HT3 receptors are involved in hyperalgesia [41]. Thus, vortioxetine is a serotonergic transmission enhancer and powerful inhibitor of 5-HT3 receptors. SSRIs are ineffective in treating neuropathic pain because they induce the disinhibition of serotoninergic neurons, which may result in maladaptive changes in the descending serotonin pathways, resulting in nociceptive sensitization and chronic pain [42,43,44]. Considering that 5-HT3 receptors are involved in 5HT-induced hyperalgesia, the ability of vortioxetine to inhibit 5-HT3 receptors and other 5-HT receptors, modulating rather than only promoting serotoninergic transmission [39], makes it an interesting candidate for CP treatment [3, 34].
Considering all previous findings, this observational study aimed to investigate, in the context of common clinical practice, improvements in depressive symptoms and pain in patients with MDD and CP treated with vortioxetine.
Methods
Study design and patients
This was a 3-month, multicenter, prospective, open-label, non-interventional pharmacoepidemiologic study conducted at four centers in Barcelona, Spain, from November 5, 2020, to February 23, 2023. The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. Fundació Unio Catalana Hospitals local ethics committee approved the study (code CEI 19/33), and it was accepted by all the sites. All patients provided written informed consent before study participation.
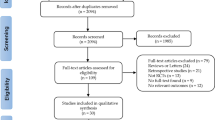
Eligible participants were those who attended pain units on an outpatient basis, showed an ineffective response to the long-lasting medication for depression they were receiving at that time, and/or had considerable adverse effects to the antidepressants. The inclusion criteria were male or female participants, aged ≥ 18 years, already diagnosed with MDD, with a 9-item Patient Health Questionnaire (PHQ-9) score ≥ 15, with an associated CP condition (visual analogic scale [VAS] score ≥ 4), and having concomitant medication to treat habitual pain, with no changes during the study. This analgesic medication consists of minor opioids, nonsteroidal anti-inflammatory drugs (NSAIDs), paracetamol, and/or metamizole (any of them inducing undesirable effects such as drowsiness, dry mouth, constipation, and disorientation). Patients were required to read and understand the Patient Information sheet and sign an Informed Consent form. Patients with any contraindications specified in the Vortioxetine SPC, cognitive impairment that mades it impossible for them to sign the informed consent form, or suffering from significant acute or unstable disease or unstable medical condition that could compromise their participation in the study according to the investigator's judgment were ineligible for study participation. Patients who were members of the staff involved in the study or their immediate family, or a subordinate (or an immediate family member of a subordinate) of the staff involved in the study, who were previously enrolled in this study, or who participated in another ongoing clinical trial were also excluded. In addition, patients who had been receiving treatment with major opioids or, in the opinion of the investigator, were unable to comply with the study protocol were not considered.
To reduce the risk of selection bias, the following measures were implemented: (1) patients were consecutively included in the study; (2) investigators were trained to respect the protocol and remain neutral during the evaluation of the patients to be included in the study; (3) several centers were included to reflect the diverse range of practices, which was expected to reduce bias linked to systematic errors; (4) a very specific sample was chosen with little variability in baseline characteristics.
Vortioxetine baseline treatment was 10 mg/day. Fifteen days after the first dose, patients received a phone call to evaluate their clinical evolution, and the dose could be increased to the maximum therapeutic dose (20 mg/day) or decreased to 5 mg/day based on individual patient response at the investigator’s judgment. All patients continued with pain medication during the study, as per common clinical practice. Study assessments and follow-ups were performed at three visits: at baseline, 1 month (± 2 weeks), and 3 months (± 2 weeks) of vortioxetine treatment (visits 1, 2, and 3, respectively).
Study Assessments
The primary objective was to assess the improvement in depressive symptoms using the 9-item Patient Health Questionnaire (PHQ-9). PHQ-9 consists of nine items with Likert-type responses ranging from 0 to 3, relative to the last two weeks. A total score between 0 and 27 is obtained:1–4, 5–9, 10–14, 15–19, and 20–27 represent minimal, mild, moderate, moderately severe, and severe depression, respectively [45].
Secondary objectives were to assess improvement in pain and treatment satisfaction in the patients. To this aim we used the following tests:
Visual analogic scale (VAS) [46] helps determine the intensity of pain to be measured with maximum reproducibility between observers. It consists of a 10-cm horizontal line, the ends of which are the extreme expressions of a symptom. The left end shows the absence of pain or lowest intensity, and the right end shows the highest intensity. The patient is asked to mark the point on the line indicating the intensity, which is measured with a millimeter ruler in centimeters or millimeters. Thus, a total measure between 0 and 10 is obtained: 0–3, 4–7, and 8–10 represent mild, moderate, and severe pain, respectively. Patients with a VAS score < 4 suffer from mild pain, which thus should not lead to major depression. Consequently, they were excluded from this study.
Brief Pain Inventory (BPI) [47] consists of 10 items. It is a multidimensional pain assessment instrument that provides information on pain intensity and its interference with activities of daily living. It also assesses the description, location, and level of pain relief associated with the treatment.
The Chronic Pain Coping Inventory (in Spanish, “Cuestionario de Afrontamiento del Dolor” [CAD]) [48] is a questionnaire on strategies to cope with pain, built using an entirely Spanish sample of patients with CP. It consists of 31 items grouped into six dimensions: self-affirmation, readiness to find information, religion, distraction, catharsis, and mental self-control. Religion and catharsis dimensions are grouped into “passive” pain coping and the remaining dimensions into “active” pain coping. The items are assessed on a 5-point agree/disagree scale.
Clinical Global Impression (CGI) Scale [49] was used to assess the overall disease severity and clinical improvement. In the current study, the Improvement (CGI-I) clinician-rated subscale was used. The Patient Global Impression Improvement (PGI-I) scale [50] consists of a single question asking the patient to rate the relief obtained with treatment. Both scales range from 1 (very much improved) to 7 (very much worse).
Satisfaction with Medicines Questionnaire (SATMED-Q) [51] is a 17-item questionnaire with six dimensions: treatment effectiveness, convenience of use, impact on daily activities, medical care, global satisfaction, and undesirable side effects. It measures the level of patient satisfaction with health care and treatment.
Adverse events (AEs) associated with vortioxetine were described during treatment. The summary included the dates of start and end, outcome, causality relationship, and severity criteria.
BPI scale and PHQ-9, CAD, and SATMED-Q questionnaires were administered at baseline and at 3 months and VAS, CGI, and PGI scales at baseline and at 1 and 3 months.
Statistical Analysis
The sample size was calculated based on the primary variable of the study: the change from baseline to month 3 in the PHQ-9 total score. With an SD of 5, the objective was to recruit 100 patients to obtain a 95% confidence interval (95% CI) with an accuracy error of ≤ 1.
The evaluable population comprised all eligible patients who had taken at least one dose of vortioxetine and had at least one post-baseline datum on the primary endpoints, including those patients with protocol violations or who discontinued the study. The safety population included all patients who received at least one dose of the study treatment.
Descriptive statistical analyses were performed for all variables. Continuous variables were described by the number of valid cases, mean, standard deviation (SD), median, 25th and 75th percentiles (P25-P75), and minimum and maximum. On the other hand, categorical variables were described by absolute and relative frequencies of each category over the total number of valid values (N). In case of missing values, the number per group was described. Comparisons of categorical variables were made using ANOVA, chi-square test, or Fisher's exact test, as applicable. For continuous variables, the Student t-test for paired data or the Mann-Whitney U-test was used depending on the type of data. A bilateral statistical significance level of 0.05 was used for all comparisons.
Statistical analysis was performed following the principles specified in the ICH E9 guidelines as well as in the standards of good clinical practice. Statistical analysis was performed using SAS (Statistical Analysis System), version 9.4, on a Windows platform.
Results
Study Population
Much of the study was conducted under the health restrictions imposed by the SARS-CoV-2 pandemic. Therefore, only four of the seven centers initially included participated in the recruitment, and only 64 patients out of the 100 initially planned were enrolled in the study. All (64 patients, 100%) signed the informed consent form. The 64 participants (100%) completed the study.
Baseline demographics and disease characteristics are shown in Table 1. The mean age of the participants was 63.6 years, and most were women (81.3%). Only two participants (3.1%) were on medical leave. Most patients (92.2%) reported at least one comorbidity (the most frequent being hypertension and osteoporosis), and all were previously receiving several analgesics (with paracetamol, NSAIDs, and tramadol being the most common) and treatment for depression (escitalopram [32.8%] and duloxetine [18.8%] in most cases) (see Table 1).
All patients were diagnosed with MDD. Most patients (92.2%) suffered from severe pain, with a mean intensity of pain (SD) of 7.64 (0.68) (lasting > 3 months and < 12 months in 40.6% and between 2 and 5 years for 25%). Patients had already developed a coping strategy to deal with pain, with readiness to find information and catharsis being the most frequent (see Table S1 in the Electronic Supplementary Material for details). Pain was located in the lower extremities and lower back in 68.8% and 67.2% of the participants, respectively, and the type of pain most commonly suffered was mixed (92.2%). Pain was mainly caused by lumbosciatica (45.3%), osteoarthritis (32.8%), and degenerative spinal problems (35.9%). Patients’ baseline clinical assessments are presented in Table 2 and showed moderate to severe pain with interference with daily life activities and moderately severe to severe depressive symptoms.
None of the participants had previously received vortioxetine treatment. The starting dose was 10 mg/day for all patients and was increased up to 20 mg/day at visit 2 in six patients. Mean (SD) vortioxetine dose was 10.00 (0.0) mg/day at baseline and 10.94 (2.94) mg/day at 3 months (Table 3).
Effect of Vortioxetine Depressive Symptoms
Statistically significant clinical improvement in the severity of depressive symptoms, as measured by the PHQ-9 score, was observed at 3 months (P < 0.0001) (Fig. 1). The PHQ-9 score changed from a mean (SD) of 16.63 (1.47) at baseline to 7.30 (2.60) at 3 months (Fig. 1a), with most patients reporting mild depression (n = 50, 78.1%), followed by moderate (n = 10, 15.6%) and minimal (n = 4, 6.3%) depression (Fig. 1b). At 3 months, the PHQ-9 score was < 15 for all patients, indicating a general improvement in depressive symptoms.

Effect of treatment with vortioxetine in the PHQ-9 score of patients at baseline and 3 months expressed as a mean PHQ-9 score ± SD and b number and percentage of patients according to the severity of depression at each timepoint. ***p < 0.0001 with respect to baseline. SD standard deviation
Effect of Vortioxetine on Pain and Overall Disease Severity
The VAS score showed a sustained improvement in patients' pain during the 3 months of treatment, with significant changes from baseline at 1 and 3 months (mean [SD] 7.42 [0.69], 6.31 [0.81], and 5.09 [1.6], respectively [P < 0.0001]) (Fig. 2a). At baseline, patients had moderate to severe pain (54.7% and 45.3%, respectively); at 1 month, most of them had moderate pain (96.9%); at 3 months, they had mild to moderate pain (9.4% and 89.1%, respectively) (Fig. 2b), indicating a decrease in the intensity of the pain. Only one patient (1.6%) reported severe pain at 3 months. Similar results were obtained with the BPI scale (Fig. 2c), which showed a significant decrease in the severity of pain in patients at 3 months from baseline (mean [SD] 6.20 (0.80) at baseline and 4.73 (0.98) at 3 months [P < 0.0001]). Furthermore, this improvement was accompanied by a significant decrease in pain interference with daily activities (Fig. 2d), with a change in the BPI score mean [SD] that ranged from 7.02 (0.85) at baseline to 4.79 (1.23) at 3 months (P < 0.0001).

Pain variations from baseline to 3 months measured by VAS (a and b) and BPI (c and d) scores: a mean VAS score ± SD; b number and percentage of patients according to intensity of pain, based on VAS score at each timepoint; c intensity of pain and d interference of pain in daily activities, according to BPI scale ± SD at each time point. ***p < 0.0001 with respect to the baseline. BPI Brief Pain Inventory; SD standard deviation; VAS visual analogue scale
An overall significant (P < 0.0001) improvement in patient condition was observed with the CGI score from baseline to 1 and 3 months (P < 0.0001 at all time points) (Fig. 3a and b). While at baseline the mean (SD) was 3.00 (0.00), it was 2.05 (0.21) at 1 month and 1.91 (0.39) at 3 months. At 3 months, 84.4% of patients were perceived as better and 12.5% as much better. According to the PGI (Fig. 3c and d), at baseline, the mean (SD) was 3.00 (0.00), showing a significant (P < 0.0001) improvement at both 1 month (2.44 [0.64]) and 3 months (1.98 [0.33]). At 3 months, 89.1% of the patients reported feeling better, and 6.3% reported feeling much better.

Improvement of the patients from baseline to 1 and 3 months according to CGI (a and b) and PGI (c and d) scores: a mean CGI score ± SD; b number and percentage of patients according to the improvement of the patient observed by the clinician at each time point; c mean PGI score ± SD; d number and percentage of patients who reported an improvement at each timepoint. ***p < 0.0001 with respect to the baseline. CGI clinical global impression; PGI patient global impression; SD standard deviation
Safety, Tolerability, and Acceptance
Vortioxetine was well tolerated, and only 18.8% and 17.2% of patients showed AEs at 1 and 3 months, respectively (See Table S2 in the electronic supplementary material). Three types of AEs were reported and ranked, at both times, as follows: drowsiness (10 patients [15.6%] and 6 patients [9.4%], respectively), dry mouth (2 patients [3.1%] and 4 patients [6.3%], respectively), and nausea (1 patient [1.6%] at week 2). All AEs were mild. No other AEs were reported.
The results from the SATMED-Q questionnaire showed that patients were satisfied with vortioxetine treatment, and no safety concerns were detected (See Table S3 in the electronic supplementary material for details).
Discussion
Comorbid medical conditions, particularly chronic systemic disorders, are often found in patients with major depression, with CP being frequently reported in depression and anxiety [2, 3, 9]. Discrimination between these conditions is difficult, and treating them individually is inconvenient owing to the low efficacy of this approach [8]. Although TCAs and SNRIs are the first-line treatment options for this comorbid condition [9, 15, 17], they have been shown to be ineffective in a significant number of patients [10, 13, 19]. As there is little evidence that SSRIs are useful in CP [21], new treatment alternatives are needed for this comorbidity.
Vortioxetine has shown clinical efficacy in the treatment of MDD in adults and recently in relieving pain and depression in patients with burning mouth syndrome [36, 37]. These properties, together with its good safety profile and fewer side effects, make it an interesting alternative for treating patients with MDD and CP.
The population in the current study comprised outpatients attending pain units diagnosed with MDD, experiencing any kind of associated CP (Table 1), and receiving concomitant medication to treat pain but never treated before with vortioxetine. Vortioxetine was administered at the same doses approved for MDD (10–20 mg/daily) [33]. Although of the 100 patients initially planned only 64 were finally included because of pandemic sanitary restrictions, this number of patients allowed us to obtain statistically significant data. The results showed a good safety profile and efficacy of this drug in patients with this comorbid condition in terms of pain relief and depressive symptoms. At baseline, patients suffered from moderately severe to severe depressive symptoms, accompanied by severe pain with interference in daily life activities, and had already developed a pain coping strategy. Nevertheless, at 3 months, most patients reported an improvement in depressive symptoms and pain, with a reduction in clinical parameters. Improvement in depressive symptoms with vortioxetine has been reported previously [27, 28, 30, 37, 52], and as expected, all patients showed an improvement in the PHQ-9 questionnaire mean score from baseline to 3 months of approximately 9 points, which was < 15 for depressive symptoms in all patients. These results are interesting, as a greater effectiveness of vortioxetine in reducing depressive symptoms was observed in these patients compared to the depression medication they were previously taking. Thus, vortioxetine appears to be effective in the treatment of depression with inadequate response to previous antidepressants, which is comorbid with chronic pain, similar to that noted in patients without coexisting pain disorders [53, 54].
Regarding pain relief, a 2-point reduction in the VAS score for pain severity was observed, as previously reported [36, 37]. This means that patients experienced a change in the category of pain they felt, which implies an improvement. Thus, while at baseline patients reported moderate to severe pain (54.7% and 45.3%, respectively), at 1 month, most had moderate pain (96.9%), and at 3 months, they had mild to moderate pain (9.4% and 89.1%, respectively). Similarly, the BPI scale showed an improvement in the mean score from baseline to 3 months of approximately 1.5 and 2.25 points, respectively. This change implies that the intensity of the pain experienced by the patient has decreased and is having less interference with daily activities. These results suggest that vortioxetine could be effective in reducing pain in patients with depression. Furthermore, clinical efficacy was evaluated using both the CGI and PGI scales, showing a decrease in the scores, indicating the improvement of the participants perceived by both clinicians and patients in overall disease severity and in the impact on global functioning. The use of the two scales, which show both the physician's and the patient's perspectives, is a methodological strength that reinforces the results obtained in the clinical improvement of the patients. Improvements in CGI score have already been observed in studies on vortioxetine pain treatment [37].
Considering the above, we must also consider that before being included in the study, the participants were already on medication consisting of an antidepressant plus pain medication. The results obtained with the change in their depression treatment, thus accompanying their pain medication with vortioxetine instead of other antidepressants, seem to imply that vortioxetine could play a role in relieving the pain and depression symptoms of patients. Furthermore, it was accompanied by a general improvement in the participants, perceived by both clinicians and patients, and with general satisfaction with the treatment reported by the subjects, which could improve their quality of life. Taken together, these results reinforce the hypothesis that vortioxetine could be an interesting alternative to other antidepressants for treating pain in patients with depression. However, it would be interesting to conduct longer clinical studies to check whether the measured parameters continue to improve or remain unchanged over time.
Limitations
The limitations of the study are that it is a single-arm, with no control group, non-randomized study with a small sample of patients and a short duration. However, this study of real clinical practice showed very good results in the treatment of pain in patients with comorbid medical conditions, including MDD and CP.
Conclusion
This observational study, performed in the context of clinical practice, has shown that the treatment of vortioxetine and pain medication in patients with MDD and CP can improve both depressive symptoms and CP, with a good efficacy and safety profile and patient satisfaction. This also shows that vortioxetine may be an interesting treatment for the management of CP, not only for depression.
Although further research is needed, this study opens the door to new, longer clinical trials in which the efficacy of vortioxetine in relieving CP can be compared with that of antidepressants already indicated for patients with MDD and CP.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Treede RD, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, et al. A classification of chronic pain for ICD-11. Pain. 2015;156:1003–7.
Sheng J, Liu S, Wang Y, Cui R, Zhang X. The link between depression and chronic pain: neural mechanisms in the brain. Neural Plast. 2017;2017:1–10.
Alcántara Montero A, Pacheco de Vasconcelos SR. of vortioxetine in the treatment of neuropathic pain. Rev Esp Anestesiol Reanim. 2022;69:640–8.
Gerrits MMJG, Van Oppen P, Van Marwijk HWJ, Penninx BWJH, Van Der Horst HE. Pain and the onset of depressive and anxiety disorders. Pain. 2014;155:53–9.
Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health. 2011;11:770.
Whiteford HA, Degenhardt L, Rehm J, Baxter AJ, Ferrari AJ, Erskine HE, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. 2013;382:1575–86.
Collins PY, Patel V, Joestl SS, March D, Insel TR, Daar AS, et al. Grand challenges in global mental health. Nature. 2011;475:27–30.
Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity. Arch Intern Med. 2003;163:2433–45.
Arango-Dávila CA, Rincón-Hoyos HG. Depressive disorder, anxiety disorder and chronic pain: multiple manifestations of a common clinical and pathophysiological core. Rev Colomb Psiquiatr. 2018;47:56–64.
Krupa AJ, Korkosz M, Gorostowicz A, Nowakowski J, Kierzkowska I, Dudek D, et al. Predictors of treatment response to serotonin and noradrenaline reuptake inhibitors in fibromyalgia. Polish Arch Intern Med. 2023;133:1–9.
Clark LA. The anxiety and depressive disorders. In: Kendall P, Watson DE, editors. Descriptive psychopathology and differential diagnosis. San Diego: Anxiety Depress distinctive overlapping Featur; 1989.
Benatti C, Blom JMC, Rigillo G, Alboni S, Zizzi F, Torta R, et al. Disease-induced neuroinflammation and depression. CNS Neurol Disord Drug Targets. 2016;15:414–33.
Krupa AJ, Chrobak AA, Sołtys Z, Korkosz M, Nowakowski J, Dudek D, et al. Psychopathological symptoms in fibromyalgia and their associations with resistance to pharmacotherapy with SNRI. Psychiatr Pol. 2024;2674:1–18.
Meerwijk EL, Ford JM, Weiss SJ. Brain regions associated with psychological pain: implications for a neural network and its relationship to physical pain. Brain Imaging Behav. 2013;7:1–14.
Mohr P, Bitter I, Svestka J, Seifritz E, Karamustafalioglu O, Koponen H, et al. Management of depression in the presence of pain symptoms. Psychiatr Danub. 2010;22:4–13.
Khouzam HR. Psychopharmacology of chronic pain: a focus on antidepressants and atypical antipsychotics. Postgrad Med. 2016;128:323–30.
Finnerup NB, Sindrup SH, Jensen TS. The evidence for pharmacological treatment of neuropathic pain. Pain. 2010;150:573–81.
Moisset X, Bouhassira D, Attal N. French guidelines for neuropathic pain: an update and commentary. Rev Neurol (Paris). 2021;177:834–7.
Birkinshaw H, Friedrich CM, Cole P, Eccleston C, Serfaty M, Stewart G, et al. Cochrane library—Antidepressants for pain management in adults with chronic pain: a network meta-analysis. Cochrane Database Syst Rev. 2023. https://doi.org/10.1002/14651858.CD014682.pub2.
Haanpää ML, Gourlay GK, Kent JL, Miaskowski C, Raja SN, Schmader KE, et al. Treatment considerations for patients with neuropathic pain and other medical comorbidities. Mayo Clin Proc. 2010;85:15–25.
Saarto T, Wiffen PJ. Antidepressants for neuropathic pain: A Cochrane review. J Neurol Neurosurg Psychiatry. 2010;81:1372–3.
Cipriani A, Furukawa TA, Salanti G, Chaimani A, Atkinson LZ, Ogawa Y, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. 2018;391:1357–66.
Porreca F, Ossipov MH, Gebhart GF. Chronic pain and medullary descending facilitation. Trends Neurosci. 2002;25:319–25.
Baldwin DS, Florea I, Jacobsen PL, Zhong W, Nomikos GG. A meta-analysis of the efficacy of vortioxetine in patients with major depressive disorder (MDD) and high levels of anxiety symptoms. J Affect Disord. 2016;206:140–50.
Chokka P, Ge H, Bougie J, Ettrup A, Clerzius G. Anxiety symptoms in working patients with major depressive disorder treated with vortioxetine: associations with clinical and treatment outcomes in the AtWoRC study. Ther Adv Psychopharmacol Orig. 2021;11:1–12.
Adair M, Cronquist Christensen M, Florea I, Loft H, Fagiolini A. Vortioxetine in patients with major depressive disorder and high levels of anxiety symptoms: an updated analysis of efficacy and tolerability. J Affect Disord. 2023;328:345–54.
Alvarez E, Perez V, Artigas F. Pharmacology and clinical potential of vortioxetine in the treatment of major depressive disorder. Neuropsychiatr Dis Treat. 2014;10:1297–307.
Christensen MC, Schmidt SN, Grande I. Effectiveness of vortioxetine in patients with major depressive disorder and early-stage dementia: the MEMORY study. J Affect Disord. 2023;338:423–31.
Baune BT, Sluth LB, Olsen CK. The effects of vortioxetine on cognitive performance in working patients with major depressive disorder: a short-term, randomized, double-blind, exploratory study. J Affect Disord. 2018;229:421–8.
Vieta E, Sluth LB, Olsen CK. The effects of vortioxetine on cognitive dysfunction in patients with inadequate response to current antidepressants in major depressive disorder: a short-term, randomized, double-blind, exploratory study versus escitalopram. J Affect Disord. 2018;227:803–9.
Baldwin DS, Chrones L, Florea I, Nielsen R, Nomikos GG, Palo W, et al. The safety and tolerability of vortioxetine: analysis of data from randomized placebo-controlled trials and open-label extension studies. J Psychopharmacol. 2016;30:242–52.
Sanchez C, Asin KE, Artigas F. Vortioxetine, a novel antidepressant with multimodal activity: review of preclinical and clinical data. Pharmacol Ther. 2015;145:43–57.
EMA. Brintellix - Ficha técnica/resumen de las características del producto [Internet]. Eur. Med. Agency. 2018 [citado 15 de septiembre de 2023]. Recuperado a partir de: https://cima.aemps.es/cima/pdfs/es/p/113891010/P_113891010.html.pdf
Zuena AR, Maftei D, Alemà GS, Dal Moro F, Lattanzi R, Casolini P, et al. Multimodal antidepressant vortioxetine causes analgesia in a mouse model of chronic neuropathic pain. Mol Pain. 2018;14:1–9.
Micov AM, Tomić MA, Todorović MB, Vuković MJ, Pecikoza UB, Jasnic NI, et al. Vortioxetine reduces pain hypersensitivity and associated depression-like behavior in mice with oxaliplatin-induced neuropathy. Prog Neuropsychopharmacol Biol Psychiatry. 2020;103:109975.
Adamo D, Pecoraro G, Aria M, Favia G, Mignogna MD. Vortioxetine in the treatment of mood disorders associated with burning mouth syndrome: results of an open-label, flexible-dose pilot study. Oral Dis. 2018;24:1168–84.
Adamo D, Pecoraro G, Coppola N, Calabria E, Aria M, Mignogna M. Vortioxetine versus other antidepressants in the treatment of burning mouth syndrome: an open-label randomized trial. Oral Dis. 2021;27:1022–41.
Richelson E. The clinical relevance of antidepressant interaction with neurotransmitter transporters and receptors. J Clin Psychiatry. 2003;64:5–12.
Stahl SM. Modes and nodes explain the mechanism of action of vortioxetine, a multimodal agent (MMA): enhancing serotonin release by combining serotonin (5HT) transporter inhibition with actions at 5HT receptors (5HT1A, 5HT1B, 5HT1D, 5HT7 receptors). CNS Spectr. 2015;20:93–7.
Kelliny M, Croarkin PE, Moore KM, Bobo WV. Profile of vortioxetine in the treatment of major depressive disorder: an overview of the primary and secondary literature. Ther Clin Risk Manag. 2015;11:1193–212.
Dogrul A, Ossipov MH, Porreca F. Differential mediation of descending pain facilitation and inhibition by spinal 5HT-3 and 5HT-7 receptors. Brain Res. 2009;1280:52–9.
Attal N, Cruccu G, Baron R, Haanpää M, Hansson P, Jensen TS, et al. EFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revision. Eur J Neurol. 2010;17:1113-e88.
Dirksen R, Van Luijtelaar ELJM, Van Rijn CM. Selective serotonin reuptake inhibitors may enhance responses to noxious stimulation. Pharmacol Biochem Behav. 1998;60:719–25.
Patetsos E, Horjales-Araujo E. Treating chronic pain with SSRIs: what do we know? Pain Res Manag. 2016;2016:1–17.
Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13.
Couper MP, Tourangeau R, Conrad FG, Singer E. Evaluating the effectiveness of visual analog scales: a web experiment. Soc Sci Comput Rev. 2006;24:227–45.
Cleeland CS. The Brief Pain Inventory [Internet]. MD Anderson Cancer Cent. [citado 19 de septiembre de 2023]. Recuperado a partir de: https://www.mdanderson.org/research/departments-labs-institutes/departments-divisions/symptom-research/symptom-assessment-tools/brief-pain-inventory.html
Soriano J, Monsalve V. CAD: Cuestionario de afrontamiento ante el dolor crónico. Rev la Soc Esp del Dolor. 2002;9:13–22.
Busner J, Targum SD. Global impressions scale: applying a research tool in clinical practice. Psychiatry (Edgmont). 2007;4:28–37.
Guy W. ECDEU Assessment Manual for Psychopharmacology. Rev. ed. D. Rockville, MD: U.S. Department of Health, Education, andWelfare; Public Health Service; Alcohol, Drug Abuse, and Mental HealthAdministration; National Institute of Mental Health; PsychopharmacologyResearch Branch; Division of Extramural Research Programs; 1976.
Ruiz MA, Pardo A, Rejas J, Soto J, Villasante F, Aranguren JL. Development and validation of the «treatment satisfaction with medicines questionnaire» (SATMED-Q)©. Value Heal. 2008;11:913–26.
Mattingly GW, Ren H, Christensen MC, Katzman MA, Polosan M, Simonsen K, et al. Effectiveness of vortioxetine in patients with major depressive disorder in real-world clinical practice: results of the RELIEVE study. Front Psychiatry. 2022;13:1–12.
Montgomery SA, Nielsen RZ, Poulsen LH, Häggström L. A randomised, double-blind study in adults with major depressive disorder with an inadequate response to a single course of selective serotonin reuptake inhibitor or serotonin-noradrenaline reuptake inhibitor treatment switched to vortioxetine or agomelat. Hum Psychopharmacol. 2014;29:470–82.
Fagiolini A, Florea I, Loft H, Christensen MC. Effectiveness of vortioxetine on emotional blunting in patients with major depressive disorder with inadequate response to SSRI/SNRI treatment. J Affect Disord. 2021;283:472–9.
Acknowledgements
We thank the participants of this study.
Medical Writing, Editorial, and Other Assistance.
Medical writing assistance was provided by Fátima Rodríguez Fornés of Trialance and funded by H. Lundbeck A/S.
Funding
The study and Rapid Service Fee were funded by H. Lundbeck A/S. Vortioxetine, marketed as Brintellix®, is commercialize by H. Lundbeck A/S.
Author information
Authors and Affiliations
Contributions
Dr. Jordi Guitart Vela and Dr. Jordi Folch Ibáñez designed the study, and reviewed and edited the manuscript. All authors contributed to the work and were familiar with the primary data. Each author read the final version of the manuscript and approved its content. All authors agree to have their names added to the paper. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship of this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Corresponding author
Ethics declarations
Conflict of interest
The authors received research funding for this study from H. Lundbeck A/S.
Ethical Approval
This study was performed in accordance with the principles of the Declaration of Helsinki of 1964. The study was reviewed and approved by the Fundació Unio Catalana Hospitals local ethics committee (code CEI 19/33), and it was accepted by all the sites. All participants provided written informed consent prior to participation.
Additional information
Prior Presentation: This work is not based on work previously presented. However, the design of the study has been previously described in the following congresses: XVI Congreso de la Sociedad Española del Dolor. May 29–June 1, 2019, Zaragoza, Spain. Presentation: Poster. Results not presented. Sine Dolore European Pain Foundation Annual Meeting 2019. May 2–5, Menorca, Spain. Presentation: Poster. Results not presented. Sine Dolore European Pain Foundation Annual Meeting 2022. May 5–8, Menorca, Spain. Presentation: Round Table: "Depression and pain, seeking full functional recovery." Results not presented.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Folch Ibáñez, J., Vargas Domingo, M., Coma Alemany, J. et al. Effectiveness of Vortioxetine in Patients with Major Depressive Disorder Associated with Chronic Pain: An Observational Study in a Spanish Population. Pain Ther 13, 621–635 (2024). https://doi.org/10.1007/s40122-024-00597-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40122-024-00597-3