
Abstract
Background
Children under the age of 3 years have been diagnosed with complex regional pain syndrome (CRPS). They were found to be functionally disadvantaged and psychologically distressed in relation to children with other painful conditions.
Case presentation
An 18-month-old baby girl was referred to the pain clinic with a history of severe right lower limb pain that had begun 2 months earlier. The parents were unable to recall any trauma before the painful situation. Pain and allodynia were severe and extended from the toes to the gluteus area. She was low weight for her age (6700 g). The patient was on the maximum doses of gabapentin and amitriptyline accepted for her body weight and did not have the possibility to start rehabilitation due to severe pain and allodynia. After discussing the risks and potential benefits of a planned lumbar sympathetic block (LSB), the parents approved the interventional procedure. This is the first case report describing the LSB technique at such a young age.
Method
A lumbar sympathetic block was carried on at the third lumbar vertebral level, fluoroscopy-guided, and under general anesthesia (GA) initiated with ketamine iv. A 4-cm needle was introduced using a tunneled vision approach in an oblique view at the L3 level until adequate depth was confirmed in the lateral position. Safety considerations were taken in relation to the radiation dose and all drugs injected with dose adjustment to her body weight. The block was successful (the skin temperature increased by 2.8 °C) and was uneventful. Pain and allodynia were completely alleviated in the recovery room. At the follow-up after 3 and 8 weeks, the parents reported an 80% improvement in pain and allodynia, a 70% improvement in sleep, a weight gain of 900 g, and that she had started rehabilitation.
Conclusions
Lumbar sympathetic blocks can be considered at a very young age to treat CRPS if other non-invasive measures fail.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Complex regional pain syndromes (CRPS) are best managed with a sympathetic block. |
The patient described had a long-lasting case of CRPS, significantly limiting the ability to care for her well-being. |
Considering her extremely young age (18 months), the decision to treat her pain with a sympathetic block was made after a long-lasting, non-successful, pharmacological therapy. |
A sympathetic block was executed with every possible caution to prevent any potential unwanted effects. |
Considering the brilliant results, and the exceptionality of the case, the authors have decided to publish this case report. |
Introduction
Both adults and children may experience chronic pain sympathetically mediated, known as complex regional pain syndrome (CRPS). CRPS type I is more common in girls than in boys in the pediatric population [1]. The mean age at diagnosis is 12 years, and the lower extremities are more affected than the upper [1]. Based on case reports, children as young as 3 years old have been diagnosed with CRPS [2]. The youngest case of CRPS ever reported in the literature involved an upper limb ailment in a young girl aged two and half years [3].
The diagnosis of CRPS in such young ages is challenging since the specific causes of the syndrome are commonly unknown. Studies on the pediatric age group are generally lacking both for origin, pathophysiology, and the clinical aspects of CRPS. However, the pathogenesis of pediatric CRPS is not necessarily identical to that of adults [1]. CRPS is commonly attributed to a previous trauma that might be very minor like a sprain or twist and in some cases no obvious injury can be recalled. Unless trauma has been witnessed by the parents, diagnosis of such trauma in very young non communicating children cannot be confirmed, adding difficulties in the diagnosis [4]. Very young non-communicating children cannot give a full history of trauma (unless witnessed) and as well they cannot describe the characteristics of their pain [1].
Signs of CRPS can vary very much. They include hyperalgesia, allodynia, swelling with or without changes in skin color of the affected limb, dry skin, mottled skin, hyperhidrosis, and trophic changes of the nails and hair [4]. Children diagnosed with CRPS are functionally more impaired and psychologically distressed than children with other pain conditions [5]. Management of CRPS in children requires the utilization of interdisciplinary treatment programs, which incorporate cognitive behavioral therapy (CBT) with physical and occupational rehabilitation [6].
To date, there are no specific pharmacological management techniques recommended for pediatric CRPS, [1] and, to the best of our knowledge, there are no large-scale clinical trials in progress. Limited studies described the use of non-steroidal anti-inflammatory drugs (NSAIDs), amitriptyline, and a few case reports described the use of gabapentin for the treatment of pediatric CRPS patients.
Ketamine is an anesthetic with analgesic effect. It is a NMDA receptor antagonist. In addition, ketamine also acts on other non-NMDA pathways that affect pain and mood regulation [7]. It acts as an antagonist of nicotinic and muscarinic cholinergic receptors. There are several studies in the adult population on the efficacy of intravenous ketamine infusions for CRPS, including case reports of resistant cases [7, 8].
Invasive pain management intervention with single sympathetic blocks was the most used to treat CRPS in pediatrics, followed by epidural catheters and continuous sympathetic blocks [9]. Regarding the outcome of these interventions, reports showed improvement in pain intensity and functional disability scores in most patients. However, outcomes were seldom assessed with validated tools. Zernikow et al. [9] concluded that there is a weak level of evidence for the use of invasive interventions for the treatment of CRPS in children.
Long-term prognosis of pediatric CRPS is unknown and studies to date have yielded contradictory results [6]. CRPS-1 in childhood seems to be milder than in adults, with less atrophy and with a good short-term prognosis. The long-term prognosis needs further evaluation [9]. This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Case Description
Method
Collection and publication of patient data were approved by the IRB of Dar Al Fouad Hospital, Giza, Egypt (DAF2023-19). Written informed consent was obtained from the father for both the intervention and the publication.
An 18-month-old baby girl was referred to the pain clinic with a history of severe lower limb pain that started 2 months earlier. Her parents were unable to recall any trauma before the onset of the pain syndrome. Before the incidental onset of pain, the girl had her normal growth in all aspects. She was able to take her first few steps while walking without assistance, with no known previous diseases or allergies.
The mother reported that the girl gradually started crying and pointing to her right knee. Over the next 2 weeks, the pain increased to cover the entire lower limb, and spread to the gluteus area by the third week. The mother informed us that the girl experienced continuous stinging pain for 24 hours, and diaper changes became problematic due to the severe pain. Due to a lack of sleep and poor appetite, the baby started losing weight. When she arrived at the pain clinic, her weight was 6700 g, significantly less than the mean normal weight at her age. The parents described the pain as excruciating and no one could touch her skin, especially around the right knee up to the gluteus area and down to the big toe.
During the first week they consulted the pediatrician who initially prescribed paracetamol 10 mg/kg oral syrup/6 hourly PRN. He then added ibuprofen syrup, 6 mg/kg every 8 h, and referred her to a pediatric orthopedic specialist. The specialist examined her with marked difficulty as severe allodynia and partial contraction of the right knee were present. He could not extend the patient’s leg. Hence, he ordered an X-ray image of the right lower limb and knee to exclude any bone lesions. All of the X-ray images were normal. She was suspected of having CRPS and was referred to the pediatric neurology department. Pediatric neurologists agreed on the suspect of CRPS, but as it is an exclusion syndrome, they did not have the possibility of an EMG that is usually performed in such a condition, to exclude nerve injuries. The exam would have been extremely difficult for the young patient without general anesthesia, which could have affected the results. Neurologists prescribed oral gabapentin 25 mg/day that was gradually escalated to 100 mg on three divided doses/day. They also added amitriptyline 5 mg that was increased to 10 mg at bedtime. The drugs' oral regimen represented the maximum possible dose for that age. The patient showed some improvement in sleep, and the pain appeared reduced and more localized around the knee. Still, she could not extend her knee, which was a little swollen and in a persistent condition of contraction at 45 degrees. The patient was referred for rehabilitation that could not be performed because of marked allodynia. The neurologist referred the patient to the pain clinic for a potential interventional treatment.
Therefore, the patient came to our attention after a journey of 2 months in the described conditions. She appeared emaciated and underweight (her body weight was 6700 g). She was also apprehensive, and showed an exaggerated fear of strangers, especially those in white coats. The pain score at rest was 8 out of 10 utilizing the FLACC scale [10]. Her right knee was semi-flexed at 45 degrees. She had marked allodynia in the right lower limb but mostly around the knee. There were not many dysautonomic signs (color and temperature changes) apart from mild edema around the knee. The parents could recall color changes in the form of redness, hotness, and edema, which accompanied the breakthrough bouts of pain. The right knee was permanently in a state of contracture at 45 degrees, without any possibility of passive extension. She could contract it more to some degree but could not extend it at all. She lost the ability to walk, as she could not perform any weight-bearing on her partially flexed right leg. There was no other abnormality. After discussing the risks and potential benefits of the planned intervention and the limitations in the literature regarding similar extremely young cases, the parents approved the trial procedure to save the limb of their baby girl and restore its function. Written informed parental consent was obtained for the intervention and the use of the patient’s anonymized data for the publication of this case report.
Case Management
The patient was introduced to the preparation room by her mother. An intravenous line was established after local anesthesia using EMLA cream. Sedation with intravenous midazolam (0.05 mg/kg) was initiated as per our hospital protocol. Standard monitors were used, including pulse oximetry, noninvasive blood pressure measurements, and ECG. The patient was transferred to the intervention room accompanied by her mother. Premedication with i.v. 0.02 mg/kg atropine was administered followed by intravenous ketamine at a dose of 2 mg/kg to initiate general anesthesia. A face mask was used with sevoflurane 1–2%, followed by laryngeal airway mask (LAM) application. At this point, the mother was requested to leave the room. Prone position with a soft roll under the pelvis was achieved and a skin temperature probe was applied to the right calf muscle area. Spontaneous breathing of 50% oxygen mixed with air and sevoflurane 1% was aided by manually assisted ventilation, if needed.
Intervention
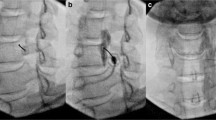
Under strict aseptic conditions and fluoroscopy guidance, L3 vertebrae was visualized (Fig. 1). The C-arm was placed in the oblique plane until the end of the transverse process was aligned with the anterior aspect of the vertebral body (Fig. 2). For the intervention, we used a 4-cm-long trocar of a 22G cannula, which was shorter than any available spinal needle. A needle was introduced and tunneled vision was obtained (Fig. 3). Once the trajectory was confirmed, a lateral view was obtained to determine the depth of the needle (Fig. 4). Needle advancement was checked every 1–2 mm depth, and we aimed to keep contact with the vertebral body as much as possible and slipped along the vertebral body to ensure correct placement. When the required depth was achieved, an A-P view was obtained to confirm the correct position of the needle tip no deeper than the mid-pedicular position. After suction, 1 ml of iohexol (180 mgI/ml) over 20 s was injected to ensure proper needle placement (Figs. 5, 6). For the anesthetic block, we used a mixture of bupivacaine 2 mg/kg with dexamethasone 0.2 mg/kg, confirmed by adequate spread of the dye by fluoroscopy (Fig. 7).

A-P view of lumbar vertebrae

Oblique view with the end of the transverse process aligned with the anterior aspect of the vertebral body

Needle introduced in tunneled vision

Lateral view obtained to determine the depth of the needle

Proper needle position, with dye (iohexol) injection to confirm accurate needle position in the antero-posterior (A-P) view

Proper needle position, with dye (iohexol) injection to confirm accurate needle position in the lateral view

Adequate dye spread after injecting the local anesthetic and steroid
Injectate Volume Calculation
There are no established guidelines recommending the volume of injectate for this technique in pediatrics. Therefore, we used the guidelines for epidural dosing in pediatrics as a proportional reference. If we know that the lumbar epidural volume for pediatrics ranges from 0.25 to 0.0.5 ml/kg [11], we agreed to have a reduced volume for our case because the point of injection is not in a closed space like the epidural space. We injected a total volume of 2 ml, confirmed by the dye spread after injection, which was satisfactory with no evidence of epidural, intravascular, or lateral spread.
Radiation Dose
The radiation dose from recorded images and number of images recorded during the procedure were reduced to attain optimum clarity and quality of the images without ignoring the safety of the patient or the procedure.
Accumulated values measured by the machine were as follows: radiation time: 00.00.38 (38 s); dose area product (DAP): 12.67 µGy∙m2 (reference air kerma (mGy) 0.30.
At this point, the patient was turned in a supine position. The general anesthesia was terminated, and the LMA was removed after securing adequate reflexes. The lower limb temperature was checked upon arrival in the recovery room. An elevation of 2.9 °C was achieved, confirming an adequate sympathetic block. The hemodynamic values showed no significant differences. The mother was invited to join the daughter in the recovery room. The first general impression was that there was no allodynia, and the child was trying to extend her knees. After complete recovery, she was discharged from the recovery room, and after another 3 h, she was discharged, and referred to the pediatric rehabilitation department.
Follow-up
After 3 and 8 weeks, in a follow-up visit, the parents reported overall improvement. Pain and allodynia were reported to be improved by 80%, and 70% respectively, with noticeable improvement in sleep, mood, and activity. On examination, there was almost no allodynia. However, the knee was still contracted. The patient had gained 900 g of body weight at the 3-week follow-up visit, and the parents reported a better appetite. During a follow-up phone call 4 months later, the patient’s mother expressed her satisfaction for the significant improvement of pain and sleep, indicating these were no longer issues. However, she did note a delay in rehabilitation progress. On a positive note, the patient can now step over her feet, has started walking, and is able to bear weight on her affected knee.
Discussion
CRPS has been reported in literature before the age of 3 years [3]. This case is the first reported in the literature to be diagnosed at such a young age (18 months). To the best of our knowledge, the youngest previously described case of CRPS was an upper limb ailment in a two-and-a-half-year-old girl [3]. Diagnosis of CRPS early in life is extremely difficult, as the patients cannot communicate. So, there is no real description of their pain. A previous publication stated that the psychological and functional effects of CRPS are more intense in children than in adults, [12] which is consistent with this case. However, the literature on the criteria for CRPS diagnosis is not solid, especially in children. Based on the Budapest Criteria [13], our patient suffered from continuous pain disproportionate to any stimulation. Symptoms and signs included sensory alterations, allodynia, sudomotor, edema around the knee, and motor abnormalities, made evident by the decreased range of movement and motor dysfunction. Hence, there was no other possible diagnosis explaining the signs and symptoms better.
Measurement of pain or functional impairment is usually based on self-reporting, even in children. However, it was not possible in our patient. Any instrumental investigation (like EMG) was impossible in this case because, as previously stated, it would have required general anesthesia, which would have altered the result. However, X-rays and MRI of the right knee were performed and resulted negative.
The LSB technique itself was not different from the technique used in adults, but we had to make some adaptations to meet the challenges of this very young patient. Among them, there was the choice of the needle length, and the needle advancement that was done very prudently (advancements of 1–2 mm max). As far as we know, this is the first report describing in detail the LSB technique at such a young age.
Radiation exposure was a major concern, as there were no previously described fluoroscopy-guided pain management interventions at such a young age and at very low body weight. Due to the limited data from clinical practice on calculating radiation doses for this age group, particularly those with low weight for age, and in comparison to other procedures and radiological examinations performed on the pediatric population (such as colonography and micturating cystourethrography), the ALARA (As Low As Reasonably Achievable) principle was adopted, as recommended by the Society of Pediatric Radiology [14,15,16]. Radiation dose from the recorded images and the number of images recorded during the procedure were reduced to attain optimum clarity and quality of the images without ignoring the safety of the patient. By comparing the radiation dose area product (DAP) of our patient to data published in similar procedures, our data were on the low limits, ensuring adequate protection [14, 16]. Lead protection could not be applied because the weight of any lead protective tool was too heavy for such a small patient.
Squaring of the images of the vertebral bodies was difficult due to the lack of ossification of the apophyses that is not completed until adulthood. The epiphyseal plates appeared not squared and soft [17]. Also, because of the small size of the patient, having the minimal cephalad or caudad tilt in the C-arm angle caused a significant change in angle of the image. Considering we were concerned about radiation exposure of such a small patient, we agreed to use the least number of images to achieve a reasonably accepted visualization, as previously described.
Ketamine injection was an addition to our management. It has contributed to the induction of general anesthesia, and it might have contributed to the management of CRPS, as suggested in previous reports on adults [7]. We commonly use it in our unit for pediatric pain management interventions that require light general anesthesia or monitored anesthesia care. It is known to be an NMDA receptor antagonist [8]. In addition, ketamine acts on other non-NMDA pathways that affect pain and mood regulation. It acts as an antagonist of nicotinic and muscarinic cholinergic receptors. It also blocks sodium and potassium channels. Ketamine activates high-affinity D2 dopamine receptors and type 1 voltage-gated calcium channels, promotes γ-aminobutyric acid A (GABA-A) signaling, and enhances descending modulatory pathways. There are several studies on the effectiveness of intravenous ketamine infusion for the management of CRPS in the adult population including reports of resistant cases [7, 8].
The calculation of dose and volume of local anesthetics was a further challenge, especially when it comes to injection volumes for an intervention at such a young age, but we have tried to link previous case reports with comparisons of the volumes used in epidural injections for children [18,19,20]. A number of previous reports of the technique have been conducted in children aged 8 to 12, and stated their maximum volumes being of 6 ml [18].
The psychological effect of CRPS on children is generally very strong and it was very evident in our case. This factor received great attention and we did our best to make the experience of the intervention acceptable. The child and mother separation was not carried out until the patient was under GA, as recommended in the literature [20]. The most overwhelming problem in this case was the level of functional and psychological disability of such a fragile patient. So, the intervention here was not only to save her limbs but also to guarantee a better quality of life.
Limitations
A limitation in our case study was that none of the established indicators or metrics for allodynia were possible to assess allodynia in this specific patient because of the considerable intensity of pain, her vulnerability, and the absence of direct communication. We relied exclusively on the observations made by the patient’s mother. However, we were able to identify the affected region of allodynia (which was as basic as sensitivity to light touch) and utilized the FLACC scale to evaluate the level of pain at rest prior to treatment, which was recorded as being as high as 8 out of 10.
Conclusions
CRPS can be diagnosed very early in life. For management, lumbar sympathetic blocks have also proven useful at a very young age when performed with extreme caution, particularly if other non-invasive measures have failed. Until clear guidelines for doses, techniques, and procedures are established, general rules should be followed, and all protective measurements must be taken.
References
Low AK, Ward K, Wines AP. Pediatric complex regional pain syndrome. J Pediatr Orthop. 2007;27(5):567–72. https://doi.org/10.1097/BPO.0b013e318070cc4d.
Weissmann R, Uziel Y. Pediatric complex regional pain syndrome: a review. Pediatr Rheumatol Online J. 2016;14(1):29. https://doi.org/10.1186/s12969-016-0090-8.
Güler-Uysal F, Başaran S, Geertzen JH, Göncü K. A 2 1/2-year-old girl with reflex sympathetic dystrophy syndrome (CRPS type I): case report. Clin Rehabil. 2003;17(2):224–7. https://doi.org/10.1191/0269215503cr589oa.
Kachko L, Efrat R, Ben Ami S, Mukamel M, Katz J. Complex regional pain syndromes in children and adolescents. Pediatr Int. 2008;50(4):523–7. https://doi.org/10.1111/j.1442-200X.2008.02625.x.
Logan DE, Williams SE, Carullo VP, et al. Children and adolescents with complex regional pain syndrome: more psychologically distressed than other children in pain? Pain Res Manag. 2013;18(2):87–93. https://doi.org/10.1155/2013/964352.
Harden RN, Oaklander AL, Burton AW, et al. Complex regional pain syndrome: practical diagnostic and treatment guidelines. Pain Med. 2013;14(2):180–229. https://doi.org/10.1111/pme.12033.
Israel JE, St Pierre S, Ellis E, et al. Ketamine for the treatment of chronic pain: a comprehensive review. Health Psychol Res. 2021;9(1):25535. https://doi.org/10.52965/001c.25535.
Chitneni A, Patil A, Dalal S, et al. Use of ketamine infusions for treatment of complex regional pain syndrome: a systematic review. Cureus. 2021;13(10): e18910. https://doi.org/10.7759/cureus.18910 PMID:34820225; PMCID:PMC8601938.
Zernikow B, Wager J, Brehmer H, et al. Invasive treatments for complex regional pain syndrome in children and adolescents. Anesthesiology. 2015;122(3):699–707. https://doi.org/10.1097/ALN.0000000000000573. (PMID: 25539076).
Peng T, Qu S, Du Z, et al. A systematic review of the measurement properties of face, legs, activity, cry and consolability scale for pediatric pain assessment. J Pain Res. 2023;16:1185–96. https://doi.org/10.2147/JPR.S397064.
Sawardekar A, Szczodry D, Suresh S. Neuraxial anaesthesia in paediatrics. Anaesth Intensive Care Med. 2013;14(6):251–4. https://doi.org/10.1016/j.mpaic.2013.03.007.
Logan DE, Williams SE, Carullo VP, et al. Children and adolescents with complex regional pain syndrome: more psychologically distressed than other children in pain? Pain Res Manag. 2013;18(2):87–93. https://doi.org/10.1155/2013/964352. (PMID: 23662291; PMCID: PMC3718058).
Harden RN, Bruehl S, Stanton-Hicks M, Wilson PR. Proposed new diagnostic criteria for complex regional pain syndrome. Pain Med. 2007;8:326–31. https://doi.org/10.1111/j.1526-4637.2006.00169.x. (PMID: 17610454).
Livingstone RS, Eapen A, Chiramel GK. Radiation dose to paediatric patients undergoing fluoroscopic examinations performed using digital imaging system. Radiography. 2008;14(1):17–23. https://doi.org/10.1016/j.radi.2006.06.004.
Strauss KJ, Kaste SC. The ALARA (as low as reasonably achievable) concept in pediatric interventional and fluoroscopic imaging: striving to keep radiation doses as low as possible during fluoroscopy of pediatric patients-a white paper executive summary. Pediatr Radiol. 2006;36(2):110–2. https://doi.org/10.1007/s00247-006-0184-4. (PMID: 16862422; PMCID: PMC2663649).
Earl VJ, Potter AO, Perdomo AA. Effective doses for common paediatric diagnostic general radiography examinations at a major Australian paediatric hospital and the communication of associated radiation risks. J Med Radiat Sci. 2022;70(1):30–9. https://doi.org/10.1002/jmrs.632. (PMID:36453696).
Jaremko JL, Siminoski K, Firth GB, et al. Canadian STOPP Consortium National Pediatric Bone Health Working Group Common normal variants of pediatric vertebral development that mimic fractures: a pictorial review from a national longitudinal bone health study. Pediatr Radiol. 2015;45(4):593–605. https://doi.org/10.1007/s00247-014-3210-y.
Meier PM, Zurakowski D, Berde CB, Sethna NF. Lumbar sympathetic blockade in children with complex regional pain syndromes: a double blind placebo-controlled crossover trial. Anesthesiology. 2009;111(2):372–80. https://doi.org/10.1097/ALN.0b013e3181aaea90.
Doolan LA, Brown TCK. Reflex sympathetic dystrophy in a child. Anaesth Intens Care. 1984;12:70–2. https://doi.org/10.1177/0310057X8401200117. (PMID: 6703323).
Cruz N, O’Reilly J, Slomine BS, Salorio CF. Emotional and neuropsychological profiles of children with complex regional pain syndrome type-I in an inpatient rehabilitation setting. Clin J Pain. 2011;27:27–34. https://doi.org/10.1097/AJP.0b013e3181f15d95. (PMID: 20842016).
Funding
No funding or sponsorship was received for this study or publication of this article.
Author information
Authors and Affiliations
Contributions
Compilation of the first draft: Amany E. Ayad. Liaison with fellow authors: Amany E. Ayad. Obtainment of patient consent: Nora Amr Agiza. Review of manuscript, from first to final drafts, providing suggestions to improve the text: Nora Amr Agiza, Amany E. Ayad, and Giustino Varrassi. Review of manuscript from neurological viewpoint: Marian Yosry Girgis. All the authors have reviewed and approved the final manuscript before submission.
Corresponding author
Ethics declarations
Conflict of Interest
The authors (Amany Ezzat Ayad, Nora Amr Agiza, Amr Hashem Elrifay, Ahmed Mortada, Marian Yosry Girgis, and Giustino Varrassi) declare that they have no conflicts of interest. Author Giustino Varrassi is an Editor-in-Chief of Pain and Therapy Journal. We confirm that he was not involved in the selection of peer reviewers for the manuscript nor any of the subsequent editorial decisions.
Ethical Approval
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Ayad, A.E., Agiza, N.A., Elrifay, A.H. et al. Lumbar Sympathetic Block to Treat CRPS in an 18-Month-Old Girl: A Breaking Barriers Case Report and Review of Literature. Pain Ther (2024). https://doi.org/10.1007/s40122-024-00650-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40122-024-00650-1