
Abstract
Artificial intelligence (AI) technology is promising in the field of healthcare. With the developments of big data and image-based analysis, AI shows potential value in ophthalmology applications. Recently, machine learning and deep learning algorithms have made significant progress. Emerging evidence has demonstrated the capability of AI in the diagnosis and management of anterior segment diseases. In this review, we provide an overview of AI applications and potential future applications in anterior segment diseases, focusing on cornea, refractive surgery, cataract, anterior chamber angle detection, and refractive error prediction.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
The application of artificial intelligence (AI) in anterior segment diseases is promising. |
AI is capable of diagnosing and managing anterior segment diseases. |
Cornea, refractive surgery, cataract, anterior chamber angle detection and refractive error prediction are the most common fields of AI applications. |
AI methods still face potential challenges. |
Introduction
With the development of artificial intelligence (AI) technology, it is proving to be promising in the field of healthcare, including radiology, pathology, microbiology, electronic medical records, and surgery [1,2,3]. The potential value of AI in ophthalmology is expanding, especially in the areas relying on big data and image-based analysis [4, 5]. The cornea and the lens are the two most important refractive structures in the anterior segment [2]. Cataract and cornea opacity rank within the top five leading causes of blindness worldwide [6, 7]. Delayed recognition of anterior segment diseases may lead to severe complications and permanent vision loss. The diagnosis and treatment of anterior segment diseases often involve imaging analysis, including slit-lamp photography (SLP), anterior segment optical coherence tomography (AS-OCT), corneal tomography/topography (CT), ultrasound biomicroscope (UBM), specular microscopy (SM), and in vivo confocal microscopy (IVCM) [2,3,4]. Thus, AI algorithms, based on anterior segment images, are mostly committed to improving accuracy for disease screening and predicting possible outcomes after disease treatments, in combination with clinical data [2, 4, 5].
In this review, we detail the history and basic principles of AI algorithms in anterior segment diseases. In addition, we provide updated overview of AI applications and discuss the potential futures in anterior segment diseases, encompassing cornea, refractive surgery, cataract, anterior chamber angle detection, and refractive error prediction.
Methods
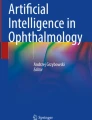
We performed the systematic review using the PubMed database, focusing on the most recent studies and clinical trials on the anterior segment diseases. The following keywords were searched: “artificial intelligence,” “machine learning,” “deep learning,” “cornea,” “keratitis,” “keratoplasty,” “corneal sub-basal nerve,” “corneal epithelium,” “corneal endothelium,” “refractive surgery,” “keratoconus,” “cataract,” “cataract surgery”, “intraocular lens,” “paediatric cataract,” “cataract surgery training,” “cataract surgery monitoring,” “anterior chamber angle,” “refractive error,” and “anterior segment diseases.” Articles published in English were included, which were manually screened for further relevant studies. This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors. The literature search is illustrated in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRIMSA) flowchart (Fig. 1).

Illustration of literature search strategy in PRISMA flowchart
History and Principle
McCarthy et al. first reported the concept of AI in 1955 [8]. In general, the core of AI algorithm is to mimic human behaviors in the real world and make human-like decisions by software programs [9]. The first generation of an AI algorithm relied on the curation of medical experts and the formulation of robust decision rules [10]. During the past 60 years, AI algorithms have improved considerably. Recent AI algorithms can manage more complex interactions, which include machine learning (ML) and deep learning (DL) as the two most common subfields [5, 9].
The ML algorithms contain two categories: supervised and unsupervised. Supervised ML methods are trained by input–output pairs (termed “ground truth”), which contain inputs and the desired output labels manually marked by human experts [5, 9, 10]. The algorithm learns to give the correct output for an input on new cases. Unsupervised ML methods are trained using unlabeled data to find subclusters of the original data, which may demonstrate something previously unknown to experts. There are common ML algorithms, such as logistic regression (LR), decision trees (DT), support vector machines (SVM), Gaussian mixture model (GMM), and random forests (RF), etc.
The DL algorithms, the latest incarnation of the artificial neural networks (ANN), can perform sophisticated multilevel data abstraction without manual feature engineering [9, 11]. The DL method consists of an input layer, an output layer, and a few hidden layers in between. An artificial neuron, such as a cortical neuron, responds to one element of the input layer and hidden layer. The “weight” of each input and hidden layer can be ascribed before passing to the next layer. Convolutional neural networks (CNN) and recurrent neural networks (RNN) are the progression of DL methods.
Cornea
Infectious Keratitis
Corneal blindness largely results from keratitis [6, 12]. Keratitis can get worse rapidly and even progress to corneal perforation without timely and correct diagnosis [12]. Early detection and appropriate treatment of keratitis can halt the disease progression and reach a better visual prognosis [12, 13]. However, the diagnosis of keratitis often requires a skilled ophthalmologist, the current clinical positive rate (33–80%) is far from ideal [14].
AI has been developed to recognize causes and improve diagnostic accuracy of keratitis. Saini et al. built an ANN classifier using 106 corneal ulcer subjects with laboratory evidence on smear or culture, and complete healing response to specific antibiotic or antifungal drugs [15]. Specificities of the ANN classifier for bacterial and fungal categories were 76.5% and 100%, respectively. Using 2008 IVCM images, Lv et al. tested a DL ResNet system to diagnose fungal keratitis [16]. The accuracy, specificity, and sensitivity were 0.9364, 0.9889, and 0.8256, respectively. Also, with 1870 IVCM images, Liu et al. trained an novel CNN framework (AlexNet) for the automatic diagnosis of fungal keratitis (accuracy = 99.95%) [17]. Kuo et al. designed a DL framework with DenseNet architecture, relying on 288 slit-lamp images, to diagnose fungal keratitis (sensitivity of 71%, specificity of 68%) [18]. Hung et al. developed deep learning models for identifying bacterial keratitis and fungal keratitis, with a highest average accuracy of 80.0% using slit-lamp images from 580 patients [19]. Ghosh et al. tested CNN models with the highest area under the curve (AUC) of 0.86 for rapidly discriminating between fungal keratitis and bacterial keratitis using slit-lamp images from 194 patients [20]. Li et al. built a DL algorithm, DenseNet121, based on 6567 slit-lamp images [21]. DenseNet121 achieved an AUC of 0.998, a sensitivity of 97.7%, and a specificity of 98.2% in keratitis detection.
To test the capability of distinguishing keratitis from other anterior diseases, AI methods have also proven to be workable. Based on 1772 slit-lamp images, Li et al. combined Visionome with a DL framework for dense annotation of the pathological features [22]. DL frameworks using ResNet and faster region-based CNN detected anterior disease, such as keratitis, conjunctival hyperemia, and pterygium, etc. Gu et al. proved that a novel DL network focusing on 5325 slit-lamp images, which contained a family of multitask and multilabel learning classifiers, was workable to diagnose infectious keratitis, noninfectious keratitis, corneal dystrophy or degeneration, and corneal neoplasm (AUC = 0.910) [23]. Loo et al. also proposed a DL algorithm for segmentation of ocular structures and microbial keratitis biomarkers [24]. Using slit-lamp images from 133 eyes, the DL algorithm is promising for the quantification of corneal physiology and pathology.
Keratoplasty
As reported by the Eye Bank, the demand for corneal graft tissue is increasing, which represents a significant financial and public health burden [25]. AI methods may help cornea surgeons to better decide on possibilities for performing keratoplasty and related procedures. Yousefi et al. introduced a ML approach, which was useful for identifying keratoconus and suspects (3495 subjects) who may be at higher risk for future keratoplasty using AS-OCT information [26]. Hayashi et al. built a DL model (AUC = 0.964) to judge the need for rebubbling after Descemet’s endothelial membrane keratoplasty (DMEK) using AS-OCT images from 62 eyes.
AI models have been tested for detecting and improving therapeutic effects of surgical procedures during keratoplasty. Hayashi et al. built a deep neural network model, Visual Geometry Group-16, to predict successful big-bubble (SBB) formation during deep anterior lamellar keratoplasty (DALK) [27]. Based on AS-OCT and corneal biometric values of 46 patients, the AUC of this model reached 0.75. Using AS-OCT images from 1172 subjects, Treder et al. evaluated a CNN classifier (accuracy = 96%) to detect graft detachment after DMEK [28]. Heslinga et al. developed a DL model to locate and quantify graft detachment after DMEK using 1280 AS-OCT scans [29]. Dice scores for the horizontal projections of all B-scans with detachments was 0.896. Pan et al. used a DL framework for augmented reality (AR)-based surgery navigation to guide the suturing in DALK [30]. The corneal contour tracking accuracy was 99.2% on average. Vigueras-Guillén et al. developed a DL method to estimate the corneal endothelium parameters from SM images of 41 eyes after Descemet stripping automated endothelial keratoplasty (DSAEK) [31]. The proposed DL method obtained reliable and accurate estimations.
Corneal Subbasal Nerve Neuropathy
Diabetic peripheral neuropathy (DPN) is the most common complication of both type 1 and 2 diabetes [32]. IVCM is capable of quantifying corneal subbasal plexus, which represents small nerve fiber damage and repair. Scarpa et al. used a CNN algorithm for the classification of IVCM images from 50 healthy subjects and 50 diabetic subjects with neuropathy [33]. This CNN algorithm provided a completely automated analysis for identifying clinically useful features for corneal nerves (accuracy = 96%). Focusing on corneal nerve fiber, Williams et al. applied a deep learning algorithm on IVCM images from 222 subjects, with a specificity of 87% and sensitivity of 68% for the identification of DPN [34]. Based on IVCM images from 369 subjects, Preston et al. utilized a CNN algorithm for corneal subbasal plexus detection to classify DPN, with the highest F1 score of 0.91 [35].
Cornea Epithelium and Endothelium Parameters
The epithelium is the outermost layer of the cornea, critical for refractive status and wound healing [36]. The most common examination method used by ophthalmologists is slit-lamp microscopy combined with different illuminations and eye staining techniques. Noor et al. reported that AI methods could differentiate abnormal corneal epithelium tissues using 25 hyperspectral imaging (HSI) images without eye staining [37]. SVM and CNN algorithms were used to extract image features with an accuracy of 100%.
Fuchs endothelial dystrophy (FED) comes with an increase in the thickness of the Descemet’s membrane, guttae, and a progressive loss of endothelial cells [38]. The guttae is a large deposition of extracellular matrix in the corneal endothelium. Vigueras-Guillén et al. developed DL methods to estimate the corneal endothelium parameters using 500 SM images with guttae [39]. The DL methods obtained lower mean absolute errors compared with commercial software.
Refractive Surgery
Early Keratoconus
Keratoconus (KC) is a noninflammatory corneal ectasia disorder, over 90% of reported KC is bilateral, and because of the progressive corneal thinning, the corneal protrusion and irregular corneal astigmatism induces poor visual performance in KC patients [40]. Early KC is a general concept of early stage KC, including subclinical KC, preclinical KC, KC suspects, and forme fruste KC (FFKC) [41]. Unlike KC, the visual performance of early KC patients is good, and there is no specific corneal topographic finding in early KC patients [42]. However, undetected early KC is known to be associated with iatrogenic keratectasia, which is the most severe and irreversible complication after laser in situ keratomileusis (LASIK) [43, 44]. Hence, discrimination of early KC from normal eyes is an urgent task for ophthalmologist and ophthalmology science.
Discriminating early KC from normal eyes by single anterior corneal topographic map is difficult; however, AI makes it possible to generate thousands of features to improve the accuracy of the discrimination power of early KC based on big data. In 1997, Smolek et al. introduced a neural network (NN) algorithm to discriminate early KC eyes from KC eyes by using corneal topography with a limited sample size [45]. After that, numerous studies have used ML algorithms to detect early KC eyes by using corneal topography. Accardo et al. used a NN method to discriminate early KC eyes from normal eyes, achieving sensitivity of 94.1% and specificity of 97.6% [46]. Saad et al. also used a NN method to detect early KC eyes, achieving sensitivity of 63% [47].
After the Scheimpflug camera became widely applied in ophthalmology clinics, multiple AI-related have studies used this system to detect early KC by collecting both anterior and posterior corneal surface information. Kovacs et al. [48] and Hidalgo et al. [49] both applied ML algorithms to detect early KC eyes by using a Scheimpflug camera, achieving sensitivities of 92% and 79.1%, respectively. Lopes et al. [50] and Smadja et al. [51] did similar studies to detect early KC eyes by using ML algorithms of RF and DT. Recently, Xie et al. used a DL algorithm to detect early KC eyes and achieved an accuracy of 95%, which was higher than achieved by senior ophthalmologists [52]. Further, Xu et al. combined raw data of the entire cornea (anterior curvature, posterior curvature, anterior elevation, posterior elevation, and pachymetry) to build a ML model called the KerNet [53]. The KerNet was helpful for distinguishing clinically unaffected eyes in patients with asymmetric KC from normal eyes (AUC = 0.985). Chen et al. reported a CNN model that combined color-coded maps of the axis, thickness, and front and back elevation [54]. The CNN model reached accuracy of 0.90 for recognizing healthy eyes and early stage KC. The outcomes of these studies show great potential for the application of AI in detecting early KC eyes by using a Scheimpflug camera, though the detection accuracy varies among studies. The limited information of low-resolution images captured by the Scheimpflug camera is one of the possible reasons.
In recent years, based on AI algorithms, several studies have tried to combine corneal information from multiple instruments to improve the detection accuracy of early KC. Hwang et al. [55] and Shi et al. [56] both combined Scheimpflug camera information and AS-OCT, which quantified corneal epithelial information to differentiate early KC eyes from normal eyes. The AUCs were 1.0 and 0.93, respectively. Perez-Rueda et al. combined biomechanical and corneal topographic information to detect early KC with an AUC of 0.951 [57]. These studies show that corneal information at different dimensions can improve the detection accuracy of early KC. AI will be a useful tool to detect early KC by generating numerous features from cornea.
Surgery Outcomes in Refractive Surgery
Predicting the outcomes of laser refractive surgery is important during clinical work. AI methods may enhance the quality of refractive surgical results by preventing the misdiagnosis in nomograms. Based on big data (17,592 cases and 38 clinical parameters for each patient), Achiron et al. developed ML classifiers to support clinical decision-making and lead to better individual risk assessment [58]. Cui et al. analyzed the ML technique for prediction of small incision lenticule extraction (SMILE) nomograms with 1465 eyes [59]. Compared with the experienced surgeon, the ML model showed significantly higher efficacy and smaller error of SE correction. However, the ML model was less predictable for eyes with high myopia and astigmatism. Park et al. tested ML algorithms using 3034 eyes composed of four categorical features and 28 numerical features accepted for SMILE surgery [60]. AdaBoost achieved the highest performance and accuracy for the sphere, cylinder, and astigmatism axis, respectively.
Lens
Age-Related Cataract
Cataract is the leading cause of blindness worldwide [6]. Approximately 32 million cataract surgeries have been performed globally up to 2020. With the global aging trend, public eye care demand is growing fast [6]. The clinical consultation and surgery for cataract patients will cause heavy burden for healthcare systems [61]. Thus, more precise diagnosis and treatment are in urgent need.
Age-related cataract always manifests as cortical cataract, nuclear sclerotic, and posterior subcapsular cataract. Slit-lamp microscopy and photography are mostly used to observe and capture cataract with diffuse, slit-beam, and retro-illumination techniques. In general, doctors usually diagnose and grade cataract according to subjective experience, based on the Lens Opacities Classification (LOCS) III and/or the Wisconsin cataract grading system, which might be inconsistent [62, 63]. Therefore, a unified and objective assessment of cataract is critical. AI technology based on big data is capable of this diagnostic and grading task. Using 37,638 slit-lamp photographs, Wu et al. built a ResNet model to capture mode recognition (AUC > 99%), cataract diagnosis (AUC > 99%), and detection of referable cataracts (AUC > 91%) [64]. To grade nuclear cataracts, Gao et al. built a CNN model using 5378 slit-beam images (mean absolute error = 0.304) [65]. Similarly, Xu et al. built a SVR model to grade nuclear cataracts using 5378 slit-beam images (mean absolute error = 0.336) [66]. Cheung et al. built a SVM model to grade nuclear cataracts using 5547 slit-beam images (AUC = 0.88–0.90) [67]. Keenan et al. developed a deep learning model called DeepLensNet to perform automated and quantitative classification of cataract severity for all three types of cortex, nuclear, and posterior subcapsular cataract. Compared with clinical ophthalmologists, the DeepLensNet performed significantly more accurately for cortex opacity (mean squared error = 13.1) and nuclear sclerosis (mean squared error = 0.23). For the least common posterior subcapsular cataract, the grading capability was similar between the DeepLensNet (mean squared error = 16.6) and clinical ophthalmologists [68]. Objectively, silt-lamp images of good quality require a certain amount of training to reduce inter-examiner deviation. Clinical grading labels for the training set may bring biases. Future work might focus on more objective grading algorithms combined with cortex, nuclear, and posterior subcapsular cataract, avoiding such errors of subjectivity.
AI models using fundus images to diagnose and grade cataract have also been developed. Xu et al. built a CNN model using 8030 fundus images to grade cataract (accuracy = 86.24%) [69]. Zhang et al. applied a SVM and CNN model using 1352 fundus images to grade cataract (accuracy = 94.75%) [70]. Xiong et al. utilized a DT model for cataract grading using 1355 fundus images (accuracy = 83.8%) [71]. Yang et al. developed an ensemble learning model for cataract grading using 1239 fundus images (accuracy = 84.5%) [72]. However, the fundus images do not directly capture the lenticular opacity. Along the visual axis, any opacity from cornea and vitreous or small pupil can blur the fundus images, leading to inaccurate diagnosis of cataract.
Moreover, Scheimpflug tomography was used to build an objective tool for nuclear cataract staging, called Pentacam Nucleus Staging (PNS). Based on the pixel intensity in the nucleus region, the PNS provided the severity value for nuclear sclerosis [73, 74]. Based on a deep learning algorithm, swept-source optical coherence tomography (SS-OCT) images have also been used to quantify cataract by lens pixels intensity. The sensitivity and specificity to detect cataract were 94.4% and 94.7%, respectively, for cortex, nuclear, and posterior subcapsular cataract detecting [75]. However, these images are potentially flawed by the limitations of themselves. All the AI-based models and tools are hypothesized based on the properties of each image device. Well-designed AI models may be further developed along the following criteria: objective grading, detection cataract of three types, specificity of lens opacity, interpretability of results, robustness to corneal disease, and limited inter-operator variability [75].
IOL Prediction
Intraocular lens (IOL) formulas are developed to improve IOL selection for cataract eye. New IOL formulas are applying big data and computational methodologies to achieve better prediction of targeted refraction and simplify the IOL selection process (Table 1).
Using the method of pattern recognition, the Hill-radial basis function (Hill-RBF) is developed based on AI and regression analysis of a very large database of actual postsurgical refractive outcomes to predict the IOL power [76]. The Hill-RBF can deal with the undefined factors in IOL power calculations. However, it is still an empirical algorithm that relies on the type of data and eye characteristics [77]. The Hill-RBF 2.0 is improved, with a larger database combined with expanded “in-bounds” biometry ranges [76]. Hill-RBF 3.0 included gender into the main metrics and further improved accuracy [78].
The Kane formula is a new IOL power formula combined AI with theoretical optics, which includes axial length, keratometry, anterior chamber depth, lens thickness, central corneal thickness, A-constant, and gender for IOL power prediction. Connell et al. found the Kane formula was more accurate than the Hill-RBF 2.0 Barrett Universal II for actual postoperative refraction [79].
In 2015, the concept of “super formula” was introduced with the integration of AI technology. This formula allowed the 3D analysis framework, including IOL power, axial length, and corneal power, to observe areas of similarities and disparities between IOL formulas [80]. The Ladas super formula consists of SRK/T, Hoffer Q, Holladay 1, Holladay with WK adjustment, and Haigis with the help of a complex DL algorithm. Kane et al. compared the Ladas formula with the new IOL formulas [77]. The study found that the Ladas super formula was less accurate than the Barrett Universal II, but was more accurate than Hill-RBF.
Based on the prediction of the internal lens position (TILP), the Pearl-DGS is a thick-lens IOL calculation formula using AI and linear algorithms [81]. The Pearl-DGS is currently an open-source tool for IOL power prediction. Clarke et al. reported a ML model (Bayesian additive regression trees) for IOL power calculation to optimize postoperation refractive outcomes, which had a median error close to the IOL manufacturer tolerance [82]. VRF formula is a vergence-based thin-lens formula. Based on theoretical optics with regression and ray-tracing principles, the VRF-G formula is a modification of VRF, including eight metrics: axial length, keratometry, anterior chamber depth, horizontal corneal diameter, lens thickness, preoperative refraction, central corneal thickness, and gender [83]. The FullMonte formula was built on mathematical neural networks combined with the Monte Carlo Markov Chain algorithm [84]. The Kamona method is based on ML algorithms using the mean K of anterior corneal surface, mean K of posterior corneal surface, axial length, anterior chamber depth, lens thickness, and white-to-white values [85].
Other AI-based IOL models have been tested to predict the IOL power. Li et al. developed a novel ML-based IOL power calculation method, the Nallasamy formula, based on a dataset of cataract patients [86]. They proved that the Nallasamy formula outperformed Barrett Universal II. Li et al. also developed a ML-prediction method to improve the performance of the ray-tracing IOL calculation, which showed more precise results in long eyes [87]. Sramka et al. evaluated the Support Vector Machine Regression model (SVM-RM) and the Multilayer Neural Network Ensemble model (MLNN-EM) for IOL power calculations, which achieved better results than the Barrett Universal II formula [88].
Li et al. incorporated a ML method for effective lens position (ELP) predictions, which is an important factor for IOL power formulas [89]. Brant et al. tested a ML algorithm to optimize the IOL inventory close to the target refractive status [90]. With the development of global databases and AI algorithms, more new IOL power calculators and models will achieve better IOL power prediction, especially for short eyes, long eyes, and post-refractive surgery eyes.
Pediatric Cataract
Although pediatric cataracts are relatively rare (1 per 3000), clinical manifestations are quite inconsistent [91]. Pediatric cataract will cause deprivation of visual stimuli, which is a big threat to visual development. Appropriate diagnosis and treatment will be helpful to reduce deprivation amblyopia and blindness [92, 93].
Recent developments in AI have shown their potential possibility for the diagnosis and management of pediatric cataract using slit-lamp images. Liu et al. built an AI model that combined CNN with SVM methods for qualitative and quantitative pediatric cataract detection using 886 slit-lamp images [94]. This model was validated for pediatric cataract diagnosis as classification (accuracy = 97.07%), area grading (accuracy = 89.02%), density (accuracy = 92.68%), and location (accuracy = 89.28%). Lin et al. created the Congenital Cataract-Cruiser (CC-Cruiser) to identify, stratify, and strategize treatment for images of pediatric cataract [95]. The accuracies of cataract diagnosis and treatment determination reached 87.4% and 70.8%, respectively. In addition, Long et al. developed a Congenital Cataract-Guardian (CC-Guardian) to accurately detect and address complications using internal and multiresource validation [96]. The CC-Guardian included three functional modules: a prediction module, a scheduling follow-up module, and a clinical decision module. The CC-Guardian provided real medical benefits for the effective management of congenital cataract. Combing the silt-lamp images and clinical information, Zhang et al. applied random forest (RF), Naïve Bayesian (NB), and association rules mining to build an AI model to predicate postoperative complications of pediatric cataract patients, with average classification accuracies over 75% [97]. In future studies, it is important to contain more clinical data and image results to improve the prognosis accuracy of pediatric cataract.
Cataract Surgery Training and Monitoring
Cataract surgery is the cornerstone operation to master for an eye surgeon. Video recording of cataract surgery is an effective way to collect surgical workflows, which are useful for surgical skill training and optimization. Combined with AI algorithms, this may extend applications to automatic report generation and real-time support. The Challenge on Automatic Tool Annotation for cataRACT Surgery (CATARACTS), in the context of a decision support algorithm, demonstrated that the annotation of cataract surgery was workable [98]. Yu et al. proved that a CNN-RNN algorithm inputted with instrument labels was accurate for identifying presegmented phases from cataract surgery videos [99]. Yeh et al. developed a CNN-RNN model that showed accurate predictions for routine steps of cataract surgery and estimated the possibility for complex cataract surgeries with advanced surgical steps [100]. Yoo et al. trained a CNN-based smart speaker (accuracy = 93.5%) for the timeout speech to confirm surgical information, such as right side, left side, cataract, phacoemulsification, and IOL [101]. Further improvements might offer more help in cataract surgery education and monitoring.
Primary Angle-Closure Glaucoma
Primary angle-closure glaucoma (PACG) accounts for 50% of global bilateral blindness due to glaucoma [102]. By 2040, the number of PACG will reach 32.04 million worldwide [103]. Objective and quantified assessments of anterior chamber depth (ACD) and anterior chamber angle (ACA) are important. To detect shallow anterior chamber, DL methods have been developed using anterior segment photographs (AUC = 0.86) [104] and fundus photographs (AUC = 0.987) [105]. Based on images obtained using ultrasound biomicroscope, automatic AI methods were applied for ACA analysis [106,107,108]. However, ultrasound biomicroscopy only shows the cross-section of localized ACA. The development of SS-OCT can capture the 3D structure of ACA. Combining AI algorithms with SS-OCT images, automatic classification for ACA evaluation is becoming more efficient for PACG diagnosis [109]. Using the SS-OCT images, Pham et al. developed a convolutional neural network (DCNN) for discrimination of scleral spur, iris, corneosclera shell, and anterior chamber, with a Dice coefficient of 95.7% [110]. In addition, Liu et al. tested the reproducibility of a DL algorithm to recognize scleral spur and anterior chamber angle [111]. The repeatability coefficients of were 0.049–0.058 mm for structure detection. Randhawa et al. tested the generalizability of DL algorithms to detect gonioscopic angle closure based on three independent patient populations, with AUCs of 0.894–0.992 [112]. Porporato et al. validated a DL algorithm for 360° angle assessment, with an AUC of 0.85 [113]. Li et al. proposed a DL method using SS-OCT images for classification of open angle, narrow angle, and angle closure (sensitivity = 0.989, specificity = 0.995) [114]. Similarly, Xu et al. tested a DL classifier for primary angle closure disease, the AUC of which reached 0.964 [115]. The incorporation of AI analysis and SS-OCT images might work as a useful tool for the management of angle-closure glaucoma.
Uncorrected Refractive Error
Uncorrected refractive error is associated with visual impairment worldwide [6]. The timely prediction of refractive error, including severe myopia and hyperopia, is essential for reducing the risks of retinal diseases, glaucoma, and amblyopia [116, 117]. Varadarajan et al. evaluated a DL method to extract information of refractive error from retinal fundus images. The mean absolute error of spherical equivalent (SE) was 0.56–0.91 diopters [118]. Yoo et al. evaluated a DL model to estimate uncorrected refractive error using posterior segment OCT (PS-OCT) images, which yielded an AUC of 0.813 for high myopia detection [119]. Chun et al. tested a DL-based system for refractive error using photorefraction images captured by a smartphone, with an overall accuracy of 81.6% [120]. With the application of ultrawide field fundus images, Yang et al. proved the feasibility of predicting refractive error in myopic patients with DL models [121]. Above all, for refractive error prediction, the AI analysis of fundus and PS-OCT images showed a clear focus of attention to the morphological changes of macular and optic nerve head. However, the accuracy of exact refractive error prediction might need further improvements considering more real-world factors.
Limitations and Future Applications
Combined with a considerable number of relevant data and images, AI shows significant promise in clinical diagnosis and decision-making. However, elaborating underlying features and classifying results of different diseases through the AI algorithms yet might be a black box, which is uncertainty whether agreeing with the real-world or not [5]. The Standard Protocol Items: Recommendations for Interventional Trials-AI (SPIRIT-AI) and Consolidated Standards of Reporting Trials-AI (CONSORT-AI) Steering Groups presented the need for consensus-based reporting guidelines for AI-related interventions [122]. These guidelines would improve both the consistency of medical professionals and the effectiveness of regulatory authorities. Therefore, AI interventions still face potential challenges before being introduced in clinical practice.
Multimodal inputs as structural images and functional data will be the future trend of AI developments [123]. Multiple input types of clinical tests are closer to the real world. However, more inputs also require more training samples to avoid overfitting. Moreover, the weight of each input should be considered when performing the integration.
Up to now, most AI algorithms have been trained with samples far away from clinical reality. AI algorithms are not comparable due to the applications of different databases. An accessible public dataset of multi-ethnicity patient cohorts is the key to enhance the generalizability of AI algorithms [122, 124]. Unified data may thus be beneficial for optimization and comparison among different AI models.
Conclusions
The application of AI in anterior segment diseases is promising (Table 2). With the advanced developments in AI algorithms, early diagnosis of debilitating anterior segment disorders and prediction of relative treatments, in the fields of cornea, refractive surgery, cataract, anterior chamber angle detection, and refractive error prediction, will make great strides. Although AI interventions face potential challenges before their full application into clinical practice, AI technologies swill make a significant impact on intelligent healthcare in the future.
References
Mintz Y, Brodie R. Introduction to artificial intelligence in medicine. Minim Invasive Ther Allied Technol. 2019;28:73–81.
Rampat R, Deshmukh R, Chen X, et al. Artificial intelligence in cornea, refractive surgery, and cataract: basic principles, clinical applications, and future directions. Asia Pac J Ophthalmol (Phila). 2021;10:268–81.
Siddiqui AA, Ladas JG, Lee JK. Artificial intelligence in cornea, refractive, and cataract surgery. Curr Opin Ophthalmol. 2020;31:253–60.
Ting DSJ, Foo VH, Yang LWY, et al. Artificial intelligence for anterior segment diseases: emerging applications in ophthalmology. Br J Ophthalmol. 2021;105:158–68.
Ting DSW, Pasquale LR, Peng L, et al. Artificial intelligence and deep learning in ophthalmology. Br J Ophthalmol. 2019;103:167–75.
Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5:e1221–34.
Ting DSJ, Ho CS, Deshmukh R, Said DG, Dua HS. Infectious keratitis: an update on epidemiology, causative microorganisms, risk factors, and antimicrobial resistance. Eye (Lond). 2021;35:1084–101.
McCarthy J, Minsky M, Rochester N, Shannon CE. A proposal for the dartmouth summer research project on artificial intelligence, August 31, 1955. AI Mag. 2006;27:12–4.
Yu KH, Beam AL, Kohane IS. Artificial intelligence in healthcare. Nat Biomed Eng. 2018;2:719–31.
Deo RC. Machine learning in medicine. Circulation. 2015;132:1920–30.
Hinton G. Deep learning-a technology with the potential to transform health care. JAMA. 2018;320:1101–2.
Austin A, Lietman T, Rose-Nussbaumer J. Update on the management of infectious keratitis. Ophthalmology. 2017;124:1678–89.
Lin A, Rhee MK, Akpek EK, et al. Bacterial keratitis preferred practice pattern®. Ophthalmology. 2019;126:P1-p55.
Ung L, Bispo PJM, Shanbhag SS, Gilmore MS, Chodosh J. The persistent dilemma of microbial keratitis: global burden, diagnosis, and antimicrobial resistance. Surv Ophthalmol. 2019;64:255–71.
Saini JS, Jain AK, Kumar S, Vikal S, Pankaj S, Singh S. Neural network approach to classify infective keratitis. Curr Eye Res. 2003;27:111–6.
Lv J, Zhang K, Chen Q, et al. Deep learning-based automated diagnosis of fungal keratitis with in vivo confocal microscopy images. Ann Transl Med. 2020;8:706.
Liu Z, Cao Y, Li Y, et al. Automatic diagnosis of fungal keratitis using data augmentation and image fusion with deep convolutional neural network. Comput Methods Progr Biomed. 2020;187: 105019.
Kuo MT, Hsu BW, Yin YK, et al. A deep learning approach in diagnosing fungal keratitis based on corneal photographs. Sci Rep. 2020;10:14424.
Hung N, Shih AK, Lin C, et al. Using slit-lamp images for deep learning-based identification of bacterial and fungal keratitis: model development and validation with different convolutional neural networks. Diagnostics (Basel). 2021;11:1246.
Ghosh AK, Thammasudjarit R, Jongkhajornpong P, Attia J, Thakkinstian A. Deep learning for discrimination between fungal keratitis and bacterial keratitis: deepkeratitis. Cornea. 2022;41:616–22.
Li Z, Jiang J, Chen K, et al. Preventing corneal blindness caused by keratitis using artificial intelligence. Nat Commun. 2021;12:3738.
Li W, Yang Y, Zhang K, et al. Dense anatomical annotation of slit-lamp images improves the performance of deep learning for the diagnosis of ophthalmic disorders. Nat Biomed Eng. 2020;4:767–77.
Gu H, Guo Y, Gu L, et al. Deep learning for identifying corneal diseases from ocular surface slit-lamp photographs. Sci Rep. 2020;10:17851.
Loo J, Kriegel MF, Tuohy MM, et al. Open-source automatic segmentation of ocular structures and biomarkers of microbial keratitis on slit-lamp photography images using deep learning. IEEE J Biomed Health Inform. 2021;25:88–99.
Gain P, Jullienne R, He Z, et al. Global survey of corneal transplantation and eye banking. JAMA Ophthalmol. 2016;134:167–73.
Yousefi S, Takahashi H, Hayashi T, et al. Predicting the likelihood of need for future keratoplasty intervention using artificial intelligence. Ocul Surf. 2020;18:320–5.
Hayashi T, Masumoto H, Tabuchi H, et al. A deep learning approach for successful big-bubble formation prediction in deep anterior lamellar keratoplasty. Sci Rep. 2021;11:18559.
Treder M, Lauermann JL, Alnawaiseh M, Eter N. Using deep learning in automated detection of graft detachment in descemet membrane endothelial keratoplasty: a pilot study. Cornea. 2019;38:157–61.
Heslinga FG, Alberti M, Pluim JPW, Cabrerizo J, Veta M. Quantifying graft detachment after descemet’s membrane endothelial keratoplasty with deep convolutional neural networks. Transl Vis Sci Technol. 2020;9:48.
Pan J, Liu W, Ge P, et al. Real-time segmentation and tracking of excised corneal contour by deep neural networks for DALK surgical navigation. Comput Methods Progr Biomed. 2020;197: 105679.
Vigueras-Guillén JP, van Rooij J, Engel A, Lemij HG, van Vliet LJ, Vermeer KA. Deep learning for assessing the corneal endothelium from specular microscopy images up to 1 year after ultrathin-dsaek surgery. Transl Vis Sci Technol. 2020;9:49.
Burgess J, Frank B, Marshall A, et al. Early detection of diabetic peripheral neuropathy: a focus on small nerve fibres. Diagnostics (Basel). 2021;11:165.
Scarpa F, Colonna A, Ruggeri A. Multiple-image deep learning analysis for neuropathy detection in corneal nerve images. Cornea. 2020;39:342–7.
Williams BM, Borroni D, Liu R, et al. An artificial intelligence-based deep learning algorithm for the diagnosis of diabetic neuropathy using corneal confocal microscopy: a development and validation study. Diabetologia. 2020;63:419–30.
Preston FG, Meng Y, Burgess J, et al. Artificial intelligence utilising corneal confocal microscopy for the diagnosis of peripheral neuropathy in diabetes mellitus and prediabetes. Diabetologia. 2022;65:457–66.
Wirostko B, Rafii M, Sullivan DA, Morelli J, Ding J. Novel therapy to treat corneal epithelial defects: a hypothesis with growth hormone. Ocul Surf. 2015;13:204-212.e201.
Noor SSM, Michael K, Marshall S, Ren J. Hyperspectral image enhancement and mixture deep-learning classification of corneal epithelium injuries. Sensors (Basel). 2017;17:2644.
Elhalis H, Azizi B, Jurkunas UV. Fuchs endothelial corneal dystrophy. Ocul Surf. 2010;8:173–84.
Vigueras-Guillén JP, van Rooij J, van Dooren BTH, et al. DenseUNets with feedback non-local attention for the segmentation of specular microscopy images of the corneal endothelium with guttae. Sci Rep. 2022;12:14035.
Burns DM, Johnston FM, Frazer DG, Patterson C, Jackson AJ. Keratoconus: an analysis of corneal asymmetry. Br J Ophthalmol. 2004;88:1252–5.
Santodomingo-Rubido J, Carracedo G, Suzaki A, Villa-Collar C, Vincent SJ, Wolffsohn JS. Keratoconus: an updated review. Cont Lens Anterior Eye. 2022;45: 101559.
Klyce SD. Chasing the suspect: keratoconus. Br J Ophthalmol. 2009;93:845–7.
Chan C, Saad A, Randleman JB, et al. Analysis of cases and accuracy of 3 risk scoring systems in predicting ectasia after laser in situ keratomileusis. J Cataract Refract Surg. 2018;44:979–92.
Klein SR, Epstein RJ, Randleman JB, Stulting RD. Corneal ectasia after laser in situ keratomileusis in patients without apparent preoperative risk factors. Cornea. 2006;25:388–403.
Smolek MK, Klyce SD. Current keratoconus detection methods compared with a neural network approach. Invest Ophthalmol Vis Sci. 1997;38:2290–9.
Accardo PA, Pensiero S. Neural network-based system for early keratoconus detection from corneal topography. J Biomed Inform. 2002;35:151–9.
Saad A, Gatinel D. Evaluation of total and corneal wavefront high order aberrations for the detection of forme fruste keratoconus. Invest Ophthalmol Vis Sci. 2012;53:2978–92.
Kovács I, Miháltz K, Kránitz K, et al. Accuracy of machine learning classifiers using bilateral data from a Scheimpflug camera for identifying eyes with preclinical signs of keratoconus. J Cataract Refract Surg. 2016;42:275–83.
Ruiz Hidalgo I, Rodriguez P, Rozema JJ, et al. Evaluation of a machine-learning classifier for keratoconus detection based on scheimpflug tomography. Cornea. 2016;35:827–32.
Lopes BT, Ramos IC, Salomão MQ, et al. Enhanced tomographic assessment to detect corneal ectasia based on artificial intelligence. Am J Ophthalmol. 2018;195:223–32.
Smadja D, Touboul D, Cohen A, et al. Detection of subclinical keratoconus using an automated decision tree classification. Am J Ophthalmol. 2013;156:237-246.e231.
Xie Y, Zhao L, Yang X, et al. Screening candidates for refractive surgery with corneal tomographic-based deep learning. JAMA Ophthalmol. 2020;138:519–26.
Xu Z, Feng R, Jin X, et al. Evaluation of artificial intelligence models for the detection of asymmetric keratoconus eyes using Scheimpflug tomography. Clin Exp Ophthalmol. 2022;50:714–23.
Chen X, Zhao J, Iselin KC, et al. Keratoconus detection of changes using deep learning of colour-coded maps. BMJ Open Ophthalmol. 2021;6: e000824.
Hwang ES, Perez-Straziota CE, Kim SW, Santhiago MR, Randleman JB. Distinguishing highly asymmetric keratoconus eyes using combined scheimpflug and spectral-domain oct analysis. Ophthalmology. 2018;125:1862–71.
Shi C, Wang M, Zhu T, et al. Machine learning helps improve diagnostic ability of subclinical keratoconus using Scheimpflug and OCT imaging modalities. Eye Vis (Lond). 2020;7:48.
Pérez-Rueda A, Jiménez-Rodríguez D, Castro-Luna G. Diagnosis of subclinical keratoconus with a combined model of biomechanical and topographic parameters. J Clin Med. 2021;10:2746.
Achiron A, Gur Z, Aviv U, et al. Predicting refractive surgery outcome: machine learning approach with big data. J Refract Surg. 2017;33:592–7.
Cui T, Wang Y, Ji S, et al. Applying machine learning techniques in nomogram prediction and analysis for smile treatment. Am J Ophthalmol. 2020;210:71–7.
Park S, Kim H, Kim L, et al. Artificial intelligence-based nomogram for small-incision lenticule extraction. Biomed Eng Online. 2021;20:38.
Wang W, Yan W, Fotis K, et al. Cataract surgical rate and socioeconomics: a global study. Invest Ophthalmol Vis Sci. 2016;57:5872–81.
Chylack LT Jr, Wolfe JK, Singer DM, et al. The Lens Opacities Classification System III. The longitudinal study of cataract study group. Arch Ophthalmol. 1993;111:831–6.
Panchapakesan J, Cumming RG, Mitchell P. Reproducibility of the Wisconsin cataract grading system in the Blue Mountains Eye Study. Ophthalmic Epidemiol. 1997;4:119–26.
Wu X, Huang Y, Liu Z, et al. Universal artificial intelligence platform for collaborative management of cataracts. Br J Ophthalmol. 2019;103:1553–60.
Gao X, Lin S, Wong TY. Automatic feature learning to grade nuclear cataracts based on deep learning. IEEE Trans Biomed Eng. 2015;62:2693–701.
Xu Y, Gao X, Lin S, et al. Automatic grading of nuclear cataracts from slit-lamp lens images using group sparsity regression. Med Image Comput Comput Assist Interv. 2013;16:468–75.
Cheung CY, Li H, Lamoureux EL, et al. Validity of a new computer-aided diagnosis imaging program to quantify nuclear cataract from slit-lamp photographs. Invest Ophthalmol Vis Sci. 2011;52:1314–9.
Keenan TDL, Chen Q, Agrón E, et al. DeepLensNet: deep learning automated diagnosis and quantitative classification of cataract type and severity. Ophthalmology. 2022;129:571–84.
Xu X, Zhang L, Li J, Guan Y, Zhang L. A Hybrid global-local representation CNN model for automatic cataract grading. IEEE J Biomed Health Inform. 2020;24:556–67.
Zhang H, Niu K, Xiong Y, Yang W, He Z, Song H. Automatic cataract grading methods based on deep learning. Comput Methods Progr Biomed. 2019;182: 104978.
Xiong L, Li H, Xu L. An approach to evaluate blurriness in retinal images with vitreous opacity for cataract diagnosis. J Healthc Eng. 2017;2017:5645498.
Yang JJ, Li J, Shen R, et al. Exploiting ensemble learning for automatic cataract detection and grading. Comput Methods Progr Biomed. 2016;124:45–57.
Grewal DS, Brar GS, Grewal SP. Correlation of nuclear cataract lens density using Scheimpflug images with Lens Opacities Classification System III and visual function. Ophthalmology. 2009;116:1436–43.
Lim SA, Hwang J, Hwang KY, Chung SH. Objective assessment of nuclear cataract: comparison of double-pass and Scheimpflug systems. J Cataract Refract Surg. 2014;40:716–21.
Zéboulon P, Panthier C, Rouger H, Bijon J, Ghazal W, Gatinel D. Development and validation of a pixel wise deep learning model to detect cataract on swept-source optical coherence tomography images. J Optom. 2022;15:43–39.
Hill W. Hill-RBF Calculator version 2.0—IOL power calculations for cataract surgery. Available at: https://rbfcalculator.com/. Accessed Feb. 22, 2020.
Kane JX, Van Heerden A, Atik A, Petsoglou C. Accuracy of 3 new methods for intraocular lens power selection. J Cataract Refract Surg. 2017;43:333–9.
Tsessler M, Cohen S, Wang L, Koch DD, Zadok D, Abulafia A. Evaluating the prediction accuracy of the Hill-RBF 30 formula using a heteroscedastic statistical method. J Cataract Refract Surg. 2022;48:37–43.
Connell BJ, Kane JX. Comparison of the Kane formula with existing formulas for intraocular lens power selection. BMJ Open Ophthalmol. 2019;4: e000251.
Ladas JG, Siddiqui AA, Devgan U, Jun AS. A 3-D “Super Surface” combining modern intraocular lens formulas to generate a “super formula” and maximize accuracy. JAMA Ophthalmol. 2015;133:1431–6.
Debellemanière G, Dubois M, Gauvin M, et al. The PEARL-DGS formula: the development of an open-source machine learning-based thick IOL calculation formula. Am J Ophthalmol. 2021;232:58–69.
Clarke GP, Kapelner A. The Bayesian additive regression trees formula for safe machine learning-based intraocular lens predictions. Front Big Data. 2020;3: 572134.
Hipólito-Fernandes D, Elisa Luís M, Gil P, et al. VRF-G, a new intraocular lens power calculation formula: a 13-formulas comparison study. Clin Ophthalmol. 2020;14:4395–402.
Kurochkin P, Weiss R, Chuck RS, Fay J, Yong C, Lee JK. A novel method of intraocular lens power selection in cataract surgery using a Markov Chain Monte Carlo Simulator. Investig Ophthalmol Vis Sci. 2015;56:2977–2977.
Carmona González D, Palomino BC. Accuracy of a new intraocular lens power calculation method based on artificial intelligence. Eye (Lond). 2021;35:517–22.
Li T, Stein J, Nallasamy N. Evaluation of the Nallasamy formula: a stacking ensemble machine learning method for refraction prediction in cataract surgery. Br J Ophthalmol. 2022; bjophthalmol-2021-320599. Epub ahead of print.
Li T, Reddy A, Stein JD, Nallasamy N. Ray tracing intraocular lens calculation performance improved by AI-powered postoperative lens position prediction. Br J Ophthalmol. 2021; bjophthalmol-2021-320283. Epub ahead of print.
Sramka M, Slovak M, Tuckova J, Stodulka P. Improving clinical refractive results of cataract surgery by machine learning. PeerJ. 2019;7: e7202.
Li T, Stein J, Nallasamy N. AI-powered effective lens position prediction improves the accuracy of existing lens formulas. Br J Ophthalmol. 2022;106:1222–6.
Brant AR, Hinkle J, Shi S, et al. Artificial intelligence in global ophthalmology: using machine learning to improve cataract surgery outcomes at Ethiopian outreaches. J Cataract Refract Surg. 2021;47:6–10.
Sheeladevi S, Lawrenson JG, Fielder AR, Suttle CM. Global prevalence of childhood cataract: a systematic review. Eye (Lond). 2016;30:1160–9.
Gilbert C, Foster A. Childhood blindness in the context of VISION 2020—the right to sight. Bull World Health Organ. 2001;79:227–32.
Reid JE, Eaton E. Artificial intelligence for pediatric ophthalmology. Curr Opin Ophthalmol. 2019;30:337–46.
Liu X, Jiang J, Zhang K, et al. Localization and diagnosis framework for pediatric cataracts based on slit-lamp images using deep features of a convolutional neural network. PLoS ONE. 2017;12: e0168606.
Lin H, Li R, Liu Z, et al. Diagnostic efficacy and therapeutic decision-making capacity of an artificial intelligence platform for childhood cataracts in eye clinics: a multicentre randomized controlled trial. EClinicalMedicine. 2019;9:52–9.
Long E, Chen J, Wu X, et al. Artificial intelligence manages congenital cataract with individualized prediction and telehealth computing. NPJ Digit Med. 2020;3:112.
Zhang K, Liu X, Jiang J, et al. Prediction of postoperative complications of pediatric cataract patients using data mining. J Transl Med. 2019;17:2.
Al Hajj H, Lamard M, Conze PH, et al. CATARACTS: Challenge on automatic tool annotation for cataRACT surgery. Med Image Anal. 2019;52:24–41.
Yu F, Silva Croso G, Kim TS, et al. Assessment of automated identification of phases in videos of cataract surgery using machine learning and deep learning techniques. JAMA Netw Open. 2019;2: e191860.
Yeh HH, Jain AM, Fox O, Wang SY. PhacoTrainer: A multicenter study of deep learning for activity recognition in cataract surgical videos. Transl Vis Sci Technol. 2021;10:23.
Yoo TK, Oh E, Kim HK, et al. Deep learning-based smart speaker to confirm surgical sites for cataract surgeries: a pilot study. PLoS ONE. 2020;15: e0231322.
Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90:262–7.
Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121:2081–90.
Qian Z, Xie X, Yang J, et al. Detection of shallow anterior chamber depth from two-dimensional anterior segment photographs using deep learning. BMC Ophthalmol. 2021;21:341.
Yoo TK, Ryu IH, Kim JK, Lee IS, Kim HK. A deep learning approach for detection of shallow anterior chamber depth based on the hidden features of fundus photographs. Comput Methods Progr Biomed. 2022;219: 106735.
Li W, Chen Q, Jiang Z, et al. Automatic anterior chamber angle measurement for ultrasound biomicroscopy using deep learning. J Glaucoma. 2020;29:81–5.
Wang W, Wang L, Wang X, Zhou S, Lin S, Yang J. A deep learning system for automatic assessment of anterior chamber angle in ultrasound biomicroscopy images. Transl Vis Sci Technol. 2021;10:21.
Shi G, Jiang Z, Deng G, et al. Automatic classification of anterior chamber angle using ultrasound biomicroscopy and deep learning. Transl Vis Sci Technol. 2019;8:25.
Porporato N, Baskaran M, Husain R, Aung T. Recent advances in anterior chamber angle imaging. Eye (Lond). 2020;34:51–9.
Pham TH, Devalla SK, Ang A, et al. Deep learning algorithms to isolate and quantify the structures of the anterior segment in optical coherence tomography images. Br J Ophthalmol. 2021;105:1231–7.
Liu P, Higashita R, Guo PY, et al. Reproducibility of deep learning based scleral spur localisation and anterior chamber angle measurements from anterior segment optical coherence tomography images. Br J Ophthalmol. 2022;2021:319798 (Epub ahead of print).
Randhawa J, Chiang M, Porporato N, et al. Generalisability and performance of an OCT-based deep learning classifier for community-based and hospital-based detection of gonioscopic angle closure. Br J Ophthalmol. 2021;2021:319470 (Epub ahead of print).
Porporato N, Tun TA, Baskaran M, et al. Towards ‘automated gonioscopy': a deep learning algorithm for 360° angle assessment by swept-source optical coherence tomography. Br J Ophthalmol. 2022;106:1387–1392.
Li W, Chen Q, Jiang C, Shi G, Deng G, Sun X. Automatic anterior chamber angle classification using deep learning system and anterior segment optical coherence tomography images. Transl Vis Sci Technol. 2021;10:19.
Xu BY, Chiang M, Chaudhary S, Kulkarni S, Pardeshi AA, Varma R. Deep learning classifiers for automated detection of gonioscopic angle closure based on anterior segment OCT images. Am J Ophthalmol. 2019;208:273–80.
Shen L, Melles RB, Metlapally R, et al. The association of refractive error with glaucoma in a multiethnic population. Ophthalmology. 2016;123:92–101.
Lavanya R, Kawasaki R, Tay WT, et al. Hyperopic refractive error and shorter axial length are associated with age-related macular degeneration: the Singapore Malay Eye Study. Invest Ophthalmol Vis Sci. 2010;51:6247–52.
Varadarajan AV, Poplin R, Blumer K, et al. Deep learning for predicting refractive error from retinal fundus images. Invest Ophthalmol Vis Sci. 2018;59:2861–8.
Yoo TK, Ryu IH, Kim JK, Lee IS. Deep learning for predicting uncorrected refractive error using posterior segment optical coherence tomography images. Eye (Lond). 2022;36:1959–65.
Chun J, Kim Y, Shin KY, et al. Deep learning-based prediction of refractive error using photorefraction images captured by a smartphone: Model development and validation study. JMIR Med Inform. 2020;8: e16225.
Yang D, Li M, Li W, et al. Prediction of refractive error based on ultrawide field images with deep learning models in myopia patients. Front Med (Lausanne). 2022;9: 834281.
Group C-AaS-AS. Reporting guidelines for clinical trials evaluating artificial intelligence interventions are needed. Nat Med. 2019;25:1467–8.
Rahimy E. Deep learning applications in ophthalmology. Curr Opin Ophthalmol. 2018;29:254–60.
Topol EJ. Welcoming new guidelines for AI clinical research. Nat Med. 2020;26:1318–20.
Acknowledgements
Funding
No funding or sponsorship was received for this study or publication of this article.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work, and have given their approval for this version to be published.
Author Contributions
Concept and design: Ke YAO and Andrzej Grzybowski; Literature search: Zhe XU, Jia XU, Ce SHI, Wen XU, Xiuming JIN, Wei HAN, and Kai JIN; Manuscript preparation: Zhe XU, Ce SHI, Andrzej Grzybowski, and Ke YAO.
Disclosures
All named authors confirm that they have no conflicts of interest to disclose.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Xu, Z., Xu, J., Shi, C. et al. Artificial Intelligence for Anterior Segment Diseases: A Review of Potential Developments and Clinical Applications. Ophthalmol Ther 12, 1439–1455 (2023). https://doi.org/10.1007/s40123-023-00690-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-023-00690-4