
Abstract
Aim
Chronic kidney disease is associated with increased risk of cardiovascular diseases (CVD). This meta-analysis aims to evaluate the efficacy and safety of aspirin administered for primary prevention of CVD in patients with chronic kidney disease.
Methods
PubMed, Scopus, Web of Science, CENTRAL and Clinicaltrials.gov were systematically searched from inception to 22 June 2023. Randomized controlled trials (RCTs) and cohort studies evaluating aspirin as primary prevention of CVD in chronic kidney disease were included. Meta-analysis was conducted using random-effects models.
Results
Overall, 11 studies (6 RCTs and 5 cohort studies) with 24,352 patients were included. The meta-analysis of RCTs indicated that aspirin was associated with lower risk of major adverse cardiovascular events [hazard ratio (HR): 0.79; 95% confidence intervals (CI): 0.64–0.97] and higher risk of major bleeding [risk ratio (RR): 1.35; 95% CI 1.15–1.58]. Incorporating observational evidence led to statistically non-significant findings in terms of risk of both cardiovascular events (pooled HR: 0.97; 95% CI 0.75–1.25; low certainty) and major bleeding (pooled RR: 1.21; 95% CI 0.99–1.48; moderate certainty). No statistically significant differences between aspirin and placebo were observed in the outcomes of mortality, coronary heart disease, stroke and renal events.
Conclusions
RCT evidence points to a possible benefit in cardiovascular event reduction from aspirin administration, at the cost of increased major bleeding risk. This finding was not confirmed when the existing observational evidence was incorporated. Further research should determine the most appropriate subpopulation of chronic kidney disease patients that would benefit the most from prophylactic aspirin therapy.
Registration
The study protocol has been prospectively registered and is publicly available from:
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
RCTs indicate cardiovascular event reduction with aspirin in chronic kidney disease. |
Aspirin is linked to an increased bleeding risk in RCTs. |
No significant benefit or harm is confirmed by observational studies. |
The current certainty of evidence is low to moderate. |
1 Introduction
Chronic kidney disease represents a rising global health concern, as it is associated with significant morbidity and financial costs. It is estimated to affect 15–20% of adults and constitutes a leading non-communicable cause of death worldwide [1]. Chronic kidney disease increases the risk of cardiovascular events, such as coronary heart disease, stroke and limb-threatening ischemia [2]. Among patients with impaired kidney function, the risk of cardiovascular death presents a steady rise with decreasing glomerular filtration rate and surpasses the risk of progression to kidney failure [3]. Chronic kidney and cardiovascular disease share common risk factors, especially hypertension, diabetes mellitus, dyslipidaemia and metabolic syndrome. In addition, chronic kidney disease is linked to various non-traditional cardiovascular risk factors, such as volume overload, metabolic acidosis, anaemia and bone mineral disease, while the accumulation of uremic toxins predisposes the patient to a pro-inflammatory state with increased oxidative stress, contributing to vascular calcification, heart valve disease and myocardial fibrosis [4]. However, current evidence for cardiovascular event prevention remains limited in patients with advanced kidney disease since data mainly derive from subgroup analyses or nonrandomized cohorts [5].
Low-dose aspirin is the mainstay of secondary cardiovascular prevention, as its administration is associated with improved survival in patients with pre-existing cardiovascular disease [6]. However, for the majority of individuals without evidence of cardiovascular disease, the modest benefit of aspirin in terms of cardiovascular event reduction does not outweigh the risk of major bleeding [7]. Therefore, identifying specific patient populations with an optimal risk–benefit tradeoff remains a research challenge. Chronic kidney disease is associated with altered haemostasis with increased propensity to both thrombosis and bleeding events due to the interplay of various mediators, such as endothelial dysfunction, platelet-vessel wall interaction, hyperfibrinogenaemia and anaemia [8]. Importantly, chronic kidney disease is characterized by increased platelet activation, presenting an attenuated response to antiplatelet therapy [9].
Evidence regarding aspirin administration for primary prevention in patients with chronic kidney disease currently remains inconclusive [10, 11]. The present systematic review and meta-analysis aims to accumulate the existing literature knowledge in the field and provide an updated evaluation of aspirin efficacy and safety among patients with chronic kidney disease without evidence of prior cardiovascular disease.
2 Materials and Methods
2.1 Study Design
The meta-analysis was reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [12]. The study protocol has been prospectively registered (dx.doi.org/https://doi.org/10.17504/protocols.io.261ged63jv47/v1) and is publicly available. No ethical approval was required, since the study was based on already published data.
2.2 Eligibility Criteria
The population of the meta-analysis consisted of patients with diagnosed chronic kidney disease, without evidence of cardiovascular disease at baseline. The intervention of interest was aspirin administration, prescribed for primary cardiovascular prevention. The intervention was compared with placebo. The primary outcome of interest was the occurrence of major adverse cardiovascular events (MACE). Secondary outcomes included cardiovascular mortality, all-cause mortality, coronary heart disease, stroke, adverse renal outcomes (doubling of serum creatinine or progression to kidney failure) and bleeding (major, minor and gastrointestinal). Both randomized controlled trials (RCTs) and cohort studies were potentially eligible. Case-control, cross-sectional and descriptive studies, as well as those exclusively examining dialysis patients were excluded. Studies evaluating the effects of aspirin given for atrial fibrillation treatment were also not included in the present review.
2.3 Definitions
Chronic kidney disease could be defined on the basis of estimated glomerular filtration rate (eGFR)-based criteria or following the Kidney Disease Improving Global Outcomes (KDIGO) guidelines [13]. Specifically, according to the KDIGO criteria, chronic kidney disease is diagnosed as the presence of structural/functional kidney abnormalities (albuminuria ≥ 30 mg/24 h, urine sediment, imaging or histological abnormalities) or reduced eGFR (< 60 ml/min/1.73 m2) for at least 3 months. The primary outcome of MACE was a composite one, based on combinations of cardiovascular mortality, myocardial infarction, stroke, heart failure and peripheral artery disease. The occurrence of a renal event was defined as the doubling of serum creatinine or progression to kidney failure requiring renal replacement therapy. The calculation of eGFR was performed with the modification of diet in renal disease (MDRD) [14], with Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) [15] or with modified equations [16, 17].
2.4 Literature Search
Literature was systematically searched via the following databases: PubMed, Scopus, Web of Science, CENTRAL and Clinicaltrials.gov. Additionally, Google Scholar along with the reference lists of the included studies (“snowball” method [18]) were screened to identify potentially missing studies. The databases were searched from inception to 22 June 2023. The search algorithm included both Medical Subject Headings (MeSH) terms and keywords. The main algorithm was the following: “(‘Aspirin’ [Mesh] OR ‘aspirin’ OR ‘acetylsalicylic acid’) AND (‘Kidney Failure, Chronic’ [Mesh] OR ‘Renal Insufficiency, Chronic’ [Mesh] OR ‘chronic kidney disease’ OR ‘CKD’ OR ‘chronic kidney failure’ OR ‘chronic renal disease’ OR ‘chronic renal failure”’ OR ‘chronic renal impairment’ OR ‘chronic kidney impairment’ OR ‘impaired renal function’ OR ‘impaired kidney function’)”. No date or language restrictions were applied.
2.5 Study Selection
At first, the titles and abstracts of all electronic records were screened and evaluated for eligibility. Subsequently, all articles that were considered to be potentially eligible were retrieved in full-text form. Then, the studies that did not report the outcomes of interest or that met any of the exclusion criteria were excluded from the meta-analysis. The process of the study selection was independently performed by two researchers, resolving any possible discrepancies through their consensus.
2.6 Data Extraction
Pre-piloted forms were used to facilitate data extraction. Specifically, the following information was collected from all included studies: year of publication, study design, location, eligibility criteria, definition of endpoints, type of population, sample size, chronic kidney disease definition, eGFR formula, aspirin dose, mean age and systolic blood pressure, percentage of females, participants with hypertension, diabetes mellitus and patients on statin therapy. Concerning the outcomes of interest, hazard ratios (HR) and risk ratios (RR) were extracted from multivariable regression or propensity score matching models, where available. Alternatively, the number of events in the total of patients was recorded, and risk ratios were calculated. Data extraction was independently conducted by two researchers; any potential disagreements were resolved after discussion with all authors.
2.7 Quality Assessment
The risk of bias of the included RCTs was evaluated using the RoB-2 tool [19], which takes into account the following domains: randomization, deviations from intended interventions, missing outcome data, measurement of the outcome and selection of the reported results. The risk of bias in cohort studies was assessed with the ROBINS-I tool [20], considering the domains of confounding, selection of participants, classification of interventions, departures from intended interventions, missing data, measurement of outcomes and selection of the reported results. The risk of bias evaluation was performed by two researchers blinded to each other, and any discrepancies were resolved through their consensus.
2.8 Statistical Analysis
The statistical analysis was conducted in R-3.6.5 (package “metafor” [21]). Random-effects models using the maximum likelihood method were fitted to provide pool estimates of HR and RR, along with their 95% confidence intervals (CI). The statistical inter-study heterogeneity was quantified by the inconsistency index (I2) [21], while the 95% predictive intervals were calculated to evaluate the effects to be expected by future studies in the field [22]. Stratified analysis was performed on the basis of study design (RCTs versus cohort studies) and interactions were tested. In addition, the primary outcome was analysed in subgroups based on study location (North America or Asia), chronic kidney disease definition (eGFR-based or KDIGO criteria), chronic kidney disease stage (stage 3a or 3b/4) and presence of comorbidities (hypertension or diabetes mellitus). Publication bias was assessed by the visual inspection of histograms. The trim–fill method was used to adjust for publication bias by imputing potentially missing studies and providing new estimates [23]. The asymmetry of funnel plots was statistically tested using Egger’s regression test (p < 0.10) in the case of at least 10 included studies [18].
2.9 Certainty of Evidence
The certainty of the existing evidence per outcome was assessed following the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach [24]. The following domains were taken into account: study limitations, indirectness, imprecision, inconsistency and publication bias.
3 Results
3.1 Study Selection
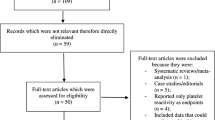
The process of study selection is schematically illustrated in the PRISMA flowchart (Fig. 1). Overall, 2683 electronic records were identified through literature search. After the removal of duplicates, 1549 articles were screened, and 17 of them were retrieved as full texts. Subsequently, six studies [25,26,27,28,29,30] were excluded due to the following reasons: overlapping population (n = 1), secondary prevention (n = 2) and exclusive evaluation of dialysis patients (n = 3; Supplementary Table 1). As a result, 11 studies [31,32,33,34,35,36,37,38,39,40,41] were included in the present meta-analysis, comprising a total of 24,352 participants. Of them, 10,036 were treated with aspirin and 14,316 with placebo.

Search plot diagram
3.2 Included Studies
The methodological and participant characteristics of the included studies are presented in Table 1. The meta-analysis included six RCTs and five cohort studies (three prospective and two retrospective). The KDIGO criteria for chronic kidney disease definition were used in three studies. The dose of aspirin ranged from 75 to 100 mg daily. The exclusion criteria and the definitions of endpoints for each study are described in Supplementary Table 2. In particular, the primary outcome was defined as the 3-point MACE consisting of cardiovascular death, non-fatal myocardial infraction or stroke in three studies; as cardiovascular death or non-fatal myocardial infraction in one study; as myocardial infraction, stroke or peripheral artery disease in three studies; as myocardial infraction, stroke or heart failure in one study; as cardiovascular death, non-fatal myocardial infraction, stroke or peripheral artery disease in one study; and as non-fatal myocardial infraction, stroke, heart failure or peripheral artery disease in one study.
Overall, a low risk of bias was recognized in three studies and a moderate risk of bias in eight studies. Specifically, the ROB-2 tool identified a moderate risk of bias in four RCTs due to concerns regarding the randomization process (n = 3), deviations from intended intervention (n = 3) and selection of the reported result (n = 3; Supplementary Fig. 1). In contrast, according to the ROBINS-I tool, a moderate risk of bias was attributed to four cohort studies owing to concerns of bias in the domains of confounding (n = 3), classification of interventions (n = 2) and deviations from intended interventions (n = 1; Supplementary Table 3).
3.3 Primary Outcome
The primary outcome of MACE was evaluated in 10 studies (5 RCTs and 5 cohort studies; Fig. 2). The meta-analysis of RCTs indicated that aspirin administration versus placebo is associated with a significantly lower risk of MACE (HR: 0.79; 95% CI 0.64–0.97). In contrast, the analysis of cohort studies demonstrated no significant difference between the two groups (HR: 1.35; 95% CI 0.75–1.25). A significant subgroup difference between RCTs and cohort studies was observed (PHeterogeneity: 0.007). The pooling of both RCTs and cohort studies indicated no significant difference in MACE risk (HR: 0.97; 95% CI 0.75–1.25). The statistical heterogeneity was remarkable (I2: 88.3%), while the 95% prediction intervals ranged from 0.41 to 2.29 (Table 2). The funnel plot showed evidence of asymmetry (Egger’s p-value: 0.038), while the trim–fill method identified four potentially missing studies (new HR: 1.18; 95% CI 0.89–1.57; Supplementary Fig. 2). The certainty of evidence was judged to be low, downgrading for inconsistency and publication bias (see Table 3).

Forest plot comparing the risk of cardiovascular events between aspirin and placebo by pooling randomized controlled trials and cohort studies.
3.4 Secondary Outcomes
3.4.1 All-Cause Mortality
No significant difference in all-cause mortality was observed in the meta-analysis of all studies (HR: 0.91; 95% CI 0.78–1.05; 10 studies). The statistical heterogeneity was moderate (I2: 53.5%), and the 95% prediction intervals ranged from 0.63 to 1.29. The trim–fill method identified two potentially missing studies (new HR: 0.95; 95% CI 0.82–1.11; Supplementary Fig. 3). Pooling of cohort studies demonstrated that aspirin administration was associated with significantly better survival rates (HR: 0.84; 95% CI 0.72–0.97); however, no significant subgroup heterogeneity was evident between RCTs and cohort studies (PHeterogeneity: 0.301; Fig. 3). The certainty of evidence was assessed to be moderate due to downgrading for inconsistency.

Subgroup analysis of secondary outcomes based on study design. PHeterogeneity < 0.05 indicates significantly different effects between RCTs and cohort studies.
3.4.2 Cardiovascular Mortality
The endpoint of cardiovascular mortality was evaluated in four studies (two RCTs and two cohort studies). No significant difference was noted between the two groups (HR: 0.93; 95% CI 0.80–1.09; I2: 0.0%). The trim–fill method recognized three potentially missing studies (new HR: 1.01; 95% CI 0.76–1.33; Supplementary Fig. 4). The outcomes of RCTs and cohort studies did not differ significantly (PHeterogeneity: 0.423). The certainty of evidence was judged as moderate due to concerns of publication bias.
3.4.3 Coronary Heart Disease
Pooling four RCTs and two cohort studies demonstrated no significantly different risk of coronary heart disease (HR: 0.91; 95% CI 0.79–1.05). The statistical heterogeneity was low (I2: 9.1%), and the 95% prediction intervals ranged from 0.75 to 1.10. The trim–fill method imputed two potentially missing studies (new HR: 1.01; 95% CI 0.76–1.33; Supplementary Fig. 5). The outcomes of RCTs and cohort studies were similar (PHeterogeneity: 0.121). The certainty of evidence was evaluated as moderate due to downgrading for inconsistency.
3.4.4 Stroke
Aspirin administration was not associated with significantly different stroke risk (HR: 0.88; 95% CI 0.70–1.11; four studies). Statistical heterogeneity was moderate (I2: 26.5%), and the 95% prediction intervals ranged from 0.61 to 1.29. No missing studies were recognized by the trim–fill method (Supplementary Fig. 6). Stratified analysis showed no significant heterogeneity between RCTs and cohort studies (PHeterogeneity: 0.461). The certainty of evidence was assessed to be moderate due to concerns of inconsistency.
3.4.5 Renal Event
Aspirin was not associated with significantly different risk of renal event (HR: 0.76; 95% CI 0.27–2.10; two studies). Statistical heterogeneity was high (I2: 63.5%), and the 95% prediction intervals ranged from 0.15 to 3.73. The funnel plot is depicted in Supplementary Fig. 7. The certainty of evidence was low due to downgrading in the domains of inconsistency and imprecision.
3.4.6 Kidney Failure
The risk of progression to kidney failure was examined in four studies (one RCT and three cohort studies), indicating no significant difference between the two groups (HR: 1.19, 95% CI 0.90–1.57). Remarkable statistical heterogeneity was observed (I2: 65.1%), with 95% prediction intervals ranging from 0.73 to 1.93. One potentially missing study was identified by the trim–fill method (new HR: 1.12; 95% CI 0.86–1.46). Similar outcomes were obtained by RCTs and cohort studies (PHeterogeneity: 0.971). The certainty of evidence was judged to be low, downgrading for inconsistency and imprecision.
3.4.7 Any Bleeding
The risk of any bleeding did not differ significantly between the two groups (RR: 1.42; 95% CI 0.80–2.51; four studies). Moderate statistical heterogeneity was noted (I2: 49.6%). The 95% prediction intervals ranged from 0.54 to 3.74. No heterogeneity was noted between the estimates of RCTs and cohort studies (PHeterogeneity: 0.974). No missing studies were imputed by the trim–fill method. The certainty of evidence was low due to concerns of inconsistency and imprecision.
3.4.8 Major Bleeding
Combining the outcomes of five RCTs and two cohort studies indicated that the major bleeding risk did not differ significantly between the two groups (RR: 1.21; 95% CI 0.99–1.48). However, the meta-analysis of RCTs demonstrated that aspirin administration was associated with a significantly higher risk of major bleeding (RR: 1.35; 95% CI 1.15–1.58). Therefore, a significant subgroup difference was observed between RCTs and cohort studies (PHeterogeneity: 0.016). The overall statistical heterogeneity was low (I2: 28.2%), and the 95% prediction intervals ranged from 0.84 to 1.74. The trim–fill method recognized two potentially missing studies (new RR: 1.15; 95% CI 0.94–1.40). The certainty of evidence was evaluated as moderate due to downgrading in the domain of imprecision.
3.4.9 Minor Bleeding
The endpoint of minor bleeding was reported by two RCTs, demonstrating no significantly different risk between the compared groups (RR: 1.61; 95% CI 0.45–5.45). High statistical heterogeneity was present (I2: 75.3%), with the 95% prediction intervals ranging from 0.23 to 11.16. The funnel plot is illustrated in Supplementary Fig. 8. The certainty of evidence was assessed to be low, downgrading for inconsistency and imprecision.
3.4.10 Gastrointestinal Bleeding
The risk of gastrointestinal bleeding was evaluated in two cohort studies, indicating no significant difference between the two groups (RR: 0.92; 95% CI 0.67–1.26). No statistical heterogeneity was observed (I2: 0.0%). The funnel plot is depicted in Supplementary Fig. 9. The certainty of evidence was low due to concerns about study limitations and imprecision.
4 Discussion
The present meta-analysis combined the outcomes of six RCTs and five cohort studies, evaluating the efficacy and safety of low-dose aspirin administered for the indication of primary prevention among patients with chronic kidney disease. Pooling of RCTs results indicated a potentially beneficial effect of aspirin in terms of cardiovascular event reduction, although at the cost of increased risk of major bleeding. However, this outcome was not confirmed by observational studies, which showed no statistically significant difference in MACE risk. In cohort studies, the risk of major bleeding was also similar between the two groups, while aspirin therapy was associated with a lower risk of all-cause mortality. Stratified analyses showed no significant benefit from aspirin administration in subgroups of different chronic kidney disease stages and the presence of comorbidities (hypertension, diabetes mellitus). The overall certainty of the existing evidence in the field was evaluated to be low to moderate, mainly due to concerns of inter-study heterogeneity leading to inconsistent results between RCTs and cohort studies, as well as to imprecise estimates, especially in the case of a small number of studies.
A previous meta-analysis [10] in the field combined the outcomes of five RCTs, proposing no statistically significant benefit from aspirin given for primary prevention. The present analysis incorporated the results of the recent TIPS-3 trial [41], as well as the outcomes of the available cohort studies. Specifically, the TIPS-3 trial included 983 patients with chronic kidney disease and demonstrated that aspirin may effectively reduce the risk of cardiovascular events, and thus the overall estimate of the present meta-analysis of RCTs indicated a statistically significant effect. In contrast, the pooling of observational cohorts showed a non-significant trend towards increased cardiovascular risk in the aspirin group. The significant heterogeneity of outcomes between RCTs and cohort studies may be partially explained by different inclusion criteria in conjunction with possible effects of selection bias, confounding by indication, protocol-enforced surveillance and compliance. The estimates of cohort studies were derived from multivariate or propensity score matching models, although the risk of residual confounding is not negligible due to the inherent limitations of observational studies. When interpreting the data, one should be aware that findings from RCTs are not always replicated in real-world settings, captured better with prospective cohort studies [42]. Information from clinical trials and observational studies should be considered complementary for decision-making.
Current data regarding the role of aspirin in dialysis populations remain sparse. An analysis of the DOPPS study [26] including 28,320 haemodialysis patients has proposed that aspirin administration is not associated with cardiovascular event reduction but with a potential decrease in stroke risk. In addition, a prospective cohort study using propensity score matching has suggested no clinical benefit from aspirin administration in haemodialysis patients [27]. Similarly, Chen et al. [29]. proposed that aspirin prescribed for primary or secondary prevention does not reduce the risk of cardiovascular disease or mortality in both haemodialysis and peritoneal dialysis patients. Interestingly, in all three studies of dialysis populations, aspirin was not linked to significantly higher rates of major bleeding.
This meta-analysis has several strengths. A comprehensive literature search with strict eligibility criteria was conducted, providing an updated assessment of the current evidence in the field. Both RCTs and cohort studies were included but separately pooled, allowing the identification of the potential impact of study design on the estimated outcomes. The 95% prediction intervals were calculated, accounting for inter-study heterogeneity and providing estimates of the effects to be expected by future studies. The certainty of evidence was also critically evaluated following the GRADE approach to generate a realistic assessment of the quality of the existing evidence. However, the interpretation of outcomes is limited by the presence of heterogeneity across studies, among others, in terms of inclusion criteria and definitions of composite endpoints. Additionally, as was suggested from the examination of funnel plots, publication bias may have potentially complicated the analysis of the outcomes of cardiovascular events and mortality. It should be also noted that limited data existed concerning stage 4 chronic kidney disease, while the potential influence of the degree of albuminuria could not be taken into account in the analyses.
The findings of the existing RCTs point towards a potential benefit of aspirin in terms of cardiovascular event risk reduction, although this effect is not supported by real-world observational evidence. This discrepancy underscores the necessity of individualizing clinical decisions to identify the subset of patients that would benefit the most from aspirin prescription, without increasing significantly the risk of major bleeding events. Cardiovascular risk prediction should incorporate information regarding both eGFR and albuminuria, while further research is needed to evaluate the predictive efficacy of novel biomarkers of cardiac and vascular dysfunction [43]. Clinical studies are also warranted to evaluate a possible platelet-centric approach using methods such as light transmission aggregometry and platelet transcriptomics aiming to identify patients with a hyperreactive platelet phenotype that would benefit the most from prophylactic aspirin therapy [44]. Furthermore, the outcomes of the placebo-controlled ATTACK trial (NCT03796156) are awaited to shed more light in the field and provide further randomized evidence regarding the role of aspirin (75 mg daily) as primary prevention of cardiovascular disease in non-dialysis chronic kidney disease patients.
In conclusion, current RCT data indicate that prophylactic aspirin administration in chronic kidney disease patients may be associated with a reduction in cardiovascular events at the cost of increased risk of major bleeding, although these effects are not confirmed by the existing observational evidence. Based on the above, aspirin cannot yet be routinely suggested as a universal primary prevention measure in chronic kidney disease populations, while further research is warranted to guide its prescription based on an individualized approach aiming for an optimal risk–benefit tradeoff.
References
Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010 [cited 2023 Jul 9];375:2073–81. Available from: https://pubmed.ncbi.nlm.nih.gov/20483451/.
Matsushita K, Ballew SH, Wang AYM, Kalyesubula R, Schaeffner E, Agarwal R. Epidemiology and risk of cardiovascular disease in populations with chronic kidney disease. Nat Rev Nephrol. 2022 [cited 2023 Jul 9];18:696–707. Available from: https://pubmed.ncbi.nlm.nih.gov/36104509/.
Tonelli M, Wiebe N, Culleton B, House A, Rabbat C, Fok M, et al. Chronic kidney disease and mortality risk: a systematic review. J Am Soc Nephrol. 2006 [cited 2023 Jul 9];17:2034–47. Available from: https://pubmed.ncbi.nlm.nih.gov/16738019/.
Jankowski J, Floege J, Fliser D, Böhm M, Marx N. Cardiovascular disease in chronic kidney disease: pathophysiological insights and therapeutic options. Circulation. 2021 [cited 2023 Jul 9];143:1157–72. Available from: https://pubmed.ncbi.nlm.nih.gov/33720773/.
Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJL, Mann JF, et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013 [cited 2023 Jul 9];382:339–52. Available from: https://pubmed.ncbi.nlm.nih.gov/23727170/.
Berger JS, Brown DL, Becker RC. Low-dose aspirin in patients with stable cardiovascular disease: a meta-analysis. Am J Med. 2008 [cited 2023 Jul 9];121:43–9. Available from: https://pubmed.ncbi.nlm.nih.gov/18187072/.
Zheng SL, Roddick AJ. Association of aspirin use for primary prevention with cardiovascular events and bleeding events: a systematic review and meta-analysis. JAMA. 2019 [cited 2023 Jul 9];321:277–87. Available from: https://pubmed.ncbi.nlm.nih.gov/30667501/.
Lutz J, Menke J, Sollinger D, Schinzel H, Thürmel K. Haemostasis in chronic kidney disease. Nephrol Dial Transplant. 2014 [cited 2023 Jul 9];29:29–40. Available from: https://pubmed.ncbi.nlm.nih.gov/24132242/.
Gremmel T, Müller M, Steiner S, Seidinger D, Koppensteiner R, Kopp CW, et al. Chronic kidney disease is associated with increased platelet activation and poor response to antiplatelet therapy. Nephrol Dial Transplant. 2013 [cited 2023 Jul 9];28:2116–22. Available from: https://pubmed.ncbi.nlm.nih.gov/23729489/.
Pallikadavath S, Ashton L, Brunskill NJ, Burton JO, Gray LJ, Major RW. Aspirin for the primary prevention of cardiovascular disease in individuals with chronic kidney disease: a systematic review and meta-analysis. Eur J Prev Cardiol . 2022 [cited 2023 Jul 10];28:1953–60. Available from: https://pubmed.ncbi.nlm.nih.gov/34448849/.
Qu B, He Y, Wu L, Lu H, Wu H, Li M. Is there a cardiovascular protective effect of aspirin in chronic kidney disease patients? A systematic review and meta-analysis. Int Urol Nephrol. 2020 [cited 2023 Sep 12];52:315–24. Available from: https://pubmed.ncbi.nlm.nih.gov/31820360/.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 [cited 2021 Jul 20];372. Available from: https://www.bmj.com/content/372/bmj.n71.
KDIGO. Chapter 2: Definition, identification, and prediction of CKD progression. Kidney Int Suppl. 2013 [cited 2020 Jun 6];3:63–72. Available from: https://www.sciencedirect.com/science/article/pii/S2157171615311023.
Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999 [cited 2023 Jul 9];130:461–70. Available from: https://pubmed.ncbi.nlm.nih.gov/10075613/.
Levey AS, Stevens LA, Schmid CH, Zhang Y, Castro AF, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009 [cited 2022 Nov 5];150:604–12. Available from: https://pubmed.ncbi.nlm.nih.gov/19414839/.
Anderson AH, Yang W, Hsu CY, Joffe MM, Leonard MB, Xie D, et al. Estimating GFR among participants in the Chronic Renal Insufficiency Cohort (CRIC) Study. Am J Kidney Dis. 2012;60:250.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009 [cited 2023 Jul 9];53:982–92. Available from: https://pubmed.ncbi.nlm.nih.gov/19339088/.
Ioannidis JPA, Trikalinos TA. The appropriateness of asymmetry tests for publication bias in meta-analyses: a large survey. CMAJ. 2007;176:1091–6. https://doi.org/10.1503/cmaj.060410.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019 [cited 2020 Jun 6];366:l4898. Available from: http://www.ncbi.nlm.nih.gov/pubmed/31462531.
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016 [cited 2019 Sep 26];355:i4919. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27733354.
Viechtbauer W. Conducting Meta-Analyses in R with the metafor Package. J Stat Softw. 2010 [cited 2018 Aug 21];36:1–48. Available from: http://www.jstatsoft.org/v36/i03/.
IntHout J, Ioannidis JPA, Rovers MM, Goeman JJ. Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open. 2016;6: e010247. https://doi.org/10.1136/bmjopen-2015-010247.
S D, R T. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000 [cited 2019 Nov 21];56. Available from: https://pubmed.ncbi.nlm.nih.gov/10877304-trim-and-fill-a-simple-funnel-plot-based-method-of-testing-and-adjusting-for-publication-bias-in-meta-analysis/.
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011 [cited 2021 Jul 20];64:383–94. Available from: http://www.jclinepi.com/article/S0895435610003306/fulltext.
Hsiao KC, Huang JY, Lee C Te, Hung TW, Liaw YP, Chang HR. Different impact of aspirin on renal progression in patients with predialysis advanced chronic kidney disease with or without previous stroke. Eur J Intern Med. 2017 [cited 2021 May 8];39:63–8. Available from: https://pubmed.ncbi.nlm.nih.gov/27884500/.
Éthier J, Bragg-Gresham JL, Piera L, Akizawa T, Asano Y, Mason N, et al. Aspirin prescription and outcomes in hemodialysis patients: the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis. 2007 [cited 2021 May 8];50:602–11. Available from: https://pubmed.ncbi.nlm.nih.gov/17900460/.
Liu J, Pan Y, Chen L, Qiao QY, Wang J, Pan LH, et al. Low-dose aspirin for prevention of cardiovascular disease in patients on hemodialysis: a 5-y prospective cohort study. Hemodial Int. 2016 [cited 2021 May 8];20:548–57. Available from: https://pubmed.ncbi.nlm.nih.gov/26932276/.
Mahady SE, Polekhina G, Woods RL, Wolfe R, Wetmore JB, Margolis KL, et al. Association between CKD and major hemorrhage in older persons: data from the Aspirin in Reducing Events in the Elderly Randomized Trial. Kidney Int reports. 2023 [cited 2023 Jul 9];8. Available from: https://pubmed.ncbi.nlm.nih.gov/37069989/.
Chen ZW, Wu CK, Yang YH, Huang JW, Wu VC, Lee JK, et al. Efficacy of antiplatelet agent usage for primary and secondary prevention in dialysis patients: a nationwide data survey and propensity analysis. Cardiovasc Drugs Ther. 2019 [cited 2023 Jul 9];33:471–9. Available from: https://pubmed.ncbi.nlm.nih.gov/31069576/.
Tsai MH, Liou HH, Huang YC, Lee TS, Chen M, Fang YW. Hazardous effect of low-dose aspirin in patients with predialysis advanced chronic kidney disease assessed by machine learning method feature selection. Healthcare (Basel). 2021 [cited 2023 Jul 9];9. Available from: https://pubmed.ncbi.nlm.nih.gov/34828530/.
Kim AJ, Lim HJ, Ro H, Ko KP, Han SY, Chang JH, et al. Low-dose aspirin for prevention of cardiovascular disease in patients with chronic kidney disease. PLoS One. 2014 [cited 2021 May 8];9. Available from: https://pubmed.ncbi.nlm.nih.gov/25093403/
Wolfe R, Wetmore JB, Woods RL, McNeil JJ, Gallagher H, Roderick P, et al. Subgroup analysis of the ASPirin in Reducing Events in the Elderly randomized clinical trial suggests aspirin did not improve outcomes in older adults with chronic kidney disease. Kidney Int [Internet]. 2021 [cited 2021 May 8];99:466–74. Available from: https://pubmed.ncbi.nlm.nih.gov/32920022/
Saito Y, Morimoto T, Ogawa H, Nakayama M, Uemura S, Doi N, et al. Low-dose aspirin therapy in patients with type 2 diabetes and reduced glomerular filtration rate: subanalysis from the JPAD trial. Diabetes Care. 2011;34:280–5.
Jardine MJ, Ninomiya T, Perkovic V, Cass A, Turnbull F, Gallagher MP, et al. Aspirin is beneficial in hypertensive patients with chronic kidney disease: a post-hoc subgroup analysis of a randomized controlled trial. J Am Coll Cardiol. 2010 [cited 2021 May 8];56:956–65. https://pubmed.ncbi.nlm.nih.gov/20828648/.
Goicoechea M, de Vinuesa SG, Quiroga B, Verde E, Bernis C, Morales E, et al. Aspirin for primary prevention of cardiovascular disease and renal disease progression in chronic kidney disease patients: a multicenter randomized clinical trial (AASER Study). Cardiovasc Drugs Ther. 2018 [cited 2021 May 8];32:255–63. https://pubmed.ncbi.nlm.nih.gov/29943364/.
Desai N, Wilson B, Bond M, Conant A, Rahman M. Association between aspirin use and cardiovascular outcomes in ALLHAT participants with and without chronic kidney disease: a post hoc analysis. J Clin Hypertens. 2021 [cited 2021 May 8];23:352–62. https://pubmed.ncbi.nlm.nih.gov/33340443/.
Baigent C, Landray M, Leaper C, Altmann P, Armitage J, Baxter A, et al. First United Kingdom Heart and Renal Protection (UK-HARP-I) study: biochemical efficacy and safety of simvastatin and safety of low-dose aspirin in chronic kidney disease. Am J Kidney Dis. 2005 [cited 2021 May 8];45:473–84. https://pubmed.ncbi.nlm.nih.gov/15754269/.
Oh YJ, Kim AJ, Ro H, Chang JH, Lee HH, Chung W, et al. Low-dose aspirin was associated with an increased risk of cardiovascular events in patients with chronic kidney disease patients and low bodyweight: results from KNOW-CKD study. Sci Rep. 2021 [cited 2021 May 8];11. https://pubmed.ncbi.nlm.nih.gov/33758303/.
Haim-Pinhas H, Yoskovitz G, Lishner M, Pereg D, Kitay-Cohen Y, Topaz G, et al. Effect of aspirin on primary prevention of cardiovascular disease and mortality among patients with chronic kidney disease. Sci Rep. 2022 [cited 2023 Jul 9];12. https://pubmed.ncbi.nlm.nih.gov/36273098/.
Taliercio JJ, Nakhoul G, Mehdi A, Yang W, Sha D, Schold JD, et al. Aspirin for primary and secondary prevention of mortality, cardiovascular disease, and kidney failure in the Chronic Renal Insufficiency Cohort (CRIC) Study. Kidney Med. 2022 [cited 2023 Jul 9];4. https://pubmed.ncbi.nlm.nih.gov/36339663/.
Mann JFE, Joseph P, Gao P, Pais P, Tyrwhitt J, Xavier D, et al. Effects of aspirin on cardiovascular outcomes in patients with chronic kidney disease. Kidney Int. 2023 [cited 2023 Jul 9];103:403–10. https://pubmed.ncbi.nlm.nih.gov/36341885/.
Richardson PG, San Miguel JF, Moreau P, Hajek R, Dimopoulos MA, Laubach JP, et al. Interpreting clinical trial data in multiple myeloma: translating findings to the real-world setting. Blood Cancer J. 2018 [cited 2023 Sep 12];8. https://pubmed.ncbi.nlm.nih.gov/30413684/.
Li X, Lindholm B. Cardiovascular risk prediction in chronic kidney disease. Am J Nephrol S. 2022;53:730–9. https://doi.org/10.1159/000528560.
Cofer LB, Barrett TJ, Berger JS. Aspirin for the primary prevention of cardiovascular disease: time for a platelet-guided approach. Arterioscler Thromb Vasc Biol. 2022;42:1207–16. https://doi.org/10.1161/ATVBAHA.122.318020.
Funding
Open access funding provided by HEAL-Link Greece.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No external funding was used in the preparation of this manuscript.
Conflict of Interest
Ioannis Bellos, Smaragdi Marinaki, Pagona Lagiou and Vassiliki Benetou declare that they have no potential conflicts of interest that might be relevant to the contents of this manuscript.
Authors’ Contributions
IB: conceptualization, data curation, analysis, methodology and writing. SM: investigation, supervision, validation, reviewing and editing. PL: supervision, validation, reviewing and editing. VB: methodology, supervision, validation, reviewing and editing.
Data Availability Statement
Data used in the analysis are presented in tables and figures. The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
Not required.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Code Availability
Not applicable.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Bellos, I., Marinaki, S., Lagiou, P. et al. Aspirin for the Primary Prevention of Cardiovascular Diseases in Patients with Chronic Kidney Disease: An Updated Meta-analysis. Am J Cardiovasc Drugs 24, 241–253 (2024). https://doi.org/10.1007/s40256-024-00630-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40256-024-00630-y