
Abstract
Background and Objective
Finerenone reduces the risk of kidney failure in patients with chronic kidney disease and type 2 diabetes. Changes in the urine albumin-to-creatinine ratio (UACR) and estimated glomerular filtration rate (eGFR) are surrogates for kidney failure. We performed dose–exposure–response analyses to determine the effects of finerenone on these surrogates in the presence and absence of sodium glucose co-transporter-2 inhibitors (SGLT2is) using individual patient data from the FIDELIO-DKD study.
Methods
Non-linear mixed-effects population pharmacokinetic/pharmacodynamic models were used to quantify disease progression in terms of UACR and eGFR during standard of care and pharmacodynamic effects of finerenone in the presence and absence of SGLT2i use.
Results
The population pharmacokinetic/pharmacodynamic models adequately described effects of finerenone exposure in reducing UACR and slowing eGFR decline over time. The reduction in UACR achieved with finerenone during the first year predicted its subsequent effect in slowing progressive eGFR decline. SGLT2i use did not modify the effects of finerenone. The population pharmacokinetic/pharmacodynamic model demonstrated with 97.5% confidence that finerenone was at least 94.1% as efficacious in reducing UACR in patients using an SGLT2i compared with patients not using an SGLT2i based on the 95% confidence interval of the SGLT2i-finerenone interaction from 94.1 to 122%. The 95% confidence interval of the SGLT2i-finerenone interaction for the UACR-mediated effect on chronic eGFR decline was 9.5–144%.
Conclusions
We developed a model that accurately describes the finerenone dose–exposure–response relationship for UACR and eGFR. The model demonstrated that the early UACR effect of finerenone predicted its long-term effect on eGFR decline. These effects were independent of concomitant SGLT2i use.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Finerenone is a novel, selective, nonsteroidal mineralocorticoid receptor antagonist that recently demonstrated efficacy in delaying chronic kidney disease (CKD) progression and reducing cardiovascular events in patients with CKD and type 2 diabetes in the pivotal FIDELIO-DKD study. |
In this secondary model-based analysis, we accurately quantified the dose–exposure–response relationship for the urine albumin-to-creatinine ratio (UACR) and estimated glomerular filtration rate (eGFR). |
The early treatment effect of finerenone on UACR predicted its long-term effect on eGFR supporting UACR as a surrogate. |
The relationship between finerenone exposure and UACR and eGFR effects was not modified by sodium glucose co-transporter 2 inhibitor use and demonstrated independent and additive effects. |
1 Introduction
Blood pressure-lowering treatment with angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) have been the mainstay of therapy for the treatment of chronic kidney disease (CKD) in the last two decades. However, despite use of these agents, the risk of kidney failure remains high. New therapeutic options to improve the management of CKD in patients with and without diabetes have emerged.
Sodium-glucose co-transporter 2 inhibitors (SGLT2is) reduce the risk of kidney failure and slow the progression of estimated glomerular filtration rate (eGFR) decline. These benefits were initially demonstrated in the CREDENCE trial, which recruited patients with type 2 diabetes and CKD [1]. The DAPA-CKD trial confirmed and extended these findings by demonstrating that the reduction in the risk of a composite kidney outcome was similar in patients with CKD with or without type 2 diabetes [2]. In addition, mineralocorticoid receptor antagonists (MRAs) reduce albuminuria in patients with CKD, but clinical trials to establish their effects on major kidney outcomes were lacking until recently. The FIDELIO-DKD trial (ClinicalTrials.gov number, NCT02540993) demonstrated that the nonsteroidal MRA finerenone reduces the risk of a composite kidney outcome in patients with CKD and type 2 diabetes [3]. In the FIDELIO trial, 5734 patients were randomised 1:1 to receive finerenone (10 or 20 mg once daily [OD]) or placebo. Treatment was in addition to standard of care including optimised ACE inhibitors or ARBs.
Based on the different modes of action, complementing benefits of a treatment combining finerenone and SGLT2i are possible, however, not established. In the presented analysis, based on FIDELIO-DKD data, we investigated the relationship of finerenone exposure and the urine albumin-to-creatinine ratio (UACR) and eGFR response, i.e. two well-established biomarkers for CKD progression discussed as surrogate endpoints [4,5,6]. We also determined whether reduced UACR levels during finerenone treatment were associated with changes in the rate of eGFR decline. Finally, we assessed whether concomitant SGLT2i use modified the exposure–response relationship of finerenone on UACR and eGFR.
2 Methods
2.1 Clinical Study
Details on the FIDELIO-DKD study design, patient characteristics and the main results have been published previously [3, 7, 8]. Information on informed consent, ethics and analytical methods are also summarised in the Electronic Supplementary Material (ESM).
In brief, FIDELIO-DKD was a randomised, double-blind, placebo-controlled phase III study investigating the efficacy and safety of finerenone, in addition to standard of care with maximally tolerated labeled doses of a renin–angiotensin system inhibitor, on the progression of kidney disease in patients with type 2 diabetes with CKD. The starting dose of the study drug was selected based on eGFR measured at the screening visit: patients started on finerenone 10 mg/day or matching placebo if their eGFR was between 25 and < 60 mL/min/1.73 m2; if their eGFR was ≥ 60 mL/min/1.73 m2, the starting dose was 20 mg/day. Patients could be up-titrated and down-titrated according to changes in eGFR and serum potassium and at the discretion of the investigator. The primary endpoint of FIDELIO-DKD was a composite of (1) time to the first occurrence of kidney failure, (2) a sustained decrease in eGFR ≥ 40% from baseline over at least 4 weeks or (3) death from renal causes. The key secondary outcome was a cardiovascular composite of cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, and hospitalisation for heart failure and additional secondary and exploratory variables included changes in UACR and eGFR from baseline [3, 7, 8].
Plasma concentrations of finerenone were determined using a sparse sampling approach in all participating patients. Population pharmacokinetic (PK) analyses have been published along with exposure–response analyses of the renal outcome and serum potassium and provided individual post-hoc PK parameters for the current exposure–response analyses [9, 10].
2.2 Model Development
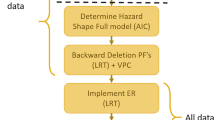
Individual finerenone exposures were simulated using the post-hoc estimates of a population PK model [10] along with individual dosing information. The PK/pharmacodyamic (PD) model development for UACR and eGFR is illustrated in Fig. 1 and described in the following sections.

Flow chart describing the pharmacokinetic/pharmacodynamic model development strategy of the estimated glomerular filtration rate (eGFR) and urine albumin-to-creatinine ratio (UACR) models. SGLT2i sodium-glucose co-transporter-2 inhibitor
2.2.1 UACR and eGFR Model Development
We first developed UACR and eGFR disease progression models using data from the placebo arm only. We subsequently explored additive, proportional, and (for eGFR only) exponential progression over time and subsequently added covariates via stepwise forward inclusion to explain inter-individual variability (significance threshold α = 0.01). Table 1 summarises the continuous and categorical covariates tested. Potential modifications of the structural and statistical model components were investigated to improve the fit of the data.
Next, we fixed UACR and eGFR disease progression parameters and included data from the active treatment arm and developed the PD model representing the relationship between daily exposure considering longitudinal dosing information (AUCτ,md) and its effect on UACR and eGFR. For eGFR, we explored two potential types of effects of finerenone: an ‘acute’ eGFR declining effect as well as a modification of ‘chronic’ eGFR decline [11, 12]. Direct and indirect effects were tested with linear, log-linear, power, and Emax characteristics including a Hill coefficient, again followed by forward inclusion of covariates. Then, all disease progression parameters were re-estimated and a backwards deletion of all covariates in the models was performed (α = 0.001).
2.2.2 Model Integration
To evaluate how far the long-term effect of finerenone on the rate of eGFR decline can be predicted by its effect on UACR, we explored whether the individual post-hoc predictions of UACR over time from the UACR model could replace baseline UACR in the eGFR model as a superior predictor of eGFR decline (Fig. 1). First, the UACR post-hoc predictions were used instead of baseline UACR as a predictor of eGFR decline and we fitted this model to the data of subjects in the placebo arm followed by a re-analysis of the stepwise forward inclusion of covariates (α = 0.01). Covariates that were identified to be significant predictors of eGFR decline during the forward inclusion step were also tested as covariates for the interaction between UACR post-hoc predictions and eGFR decline.
Subsequently, we fixed the eGFR disease progression parameters and fitted the model to the full dataset (both active treatment and placebo). To evaluate whether the effect of finerenone on the chronic eGFR decline is fully characterised via its effect on UACR, we tested whether the model would improve by estimating additional non-UACR-mediated effects of finerenone on eGFR decline. Thereafter, a forward inclusion of covariates on the UACR effect of finerenone on eGFR was performed (α = 0.01). Finally, all disease progression parameters were re-estimated, and a stepwise backwards deletion of all covariates in the eGFR model was performed (α = 0.001).
2.2.3 Integration of SGLT2is
SGLT2i use was recorded as a time-varying binary variable over time (use/no use in last 5 days), without a consideration of the specific SGLT2i drug or its dosing schedule and integrated last into the model. For both UACR and eGFR models, we explored a direct effect of SGLT2i use as well as an effect on the rate of change of these biomarkers. For the direct SGLT2i effects, tested models included an instantaneous onset/offset of the SGLT2i effect, as well as models in which the time to steady-state SGLT2i effect was estimated. Finally, we tested whether the time-varying use of SGLT2is modified the effect of finerenone.
2.3 Model Evaluation
We evaluated the performance of the model by performing simulations of UACR and eGFR profiles and comparing these with observations, from here on referred to as a visual predictive check (VPC). The VPC simulations include residual error and inter-individual variability, but not parameter uncertainty [13].
To illustrate certain aspects of the UACR and eGFR models, we simulated the progression of UACR and eGFR over time with placebo, finerenone and/or SGLT2i treatment using the final population PK/PD models for a typical subject (i.e. without inter-individual or residual variability). For typical simulations of eGFR, the chronic slope was also calculated as the rate of eGFR decline between 1 and 4 years after treatment initiation.
2.4 Computation
The analysis was performed by means of non-linear mixed-effects modelling as implemented in the NONMEM software package (version 7.4.3). NONMEM’s first-order conditional estimation method was used for the estimation of the parameters during this analysis, with the exception of the final eGFR model, which was re-run with the stochastic approximation expectation-maximisation method for parameter estimation, followed by an expectation-only step of the importance sampling method to improve the stability of the model by avoiding rounding errors that occurred with the first-order conditional estimation method.
3 Results
3.1 Clinical Data
The analysis included 5674 patients (full analysis set in FIDELIO-DKD) with 37,296 UACR and 78,132 eGFR observations, respectively. Selected patient characteristics are provided in Table 1. In total, 528 patients were using SGLT2is at any time during the treatment period.
The UACR changes from baseline data at the scheduled study visits are visualised in Fig. S1 of the ESM. In the placebo arm, the median change from baseline UACR increases over time (from − 1.4% at month 4 to + 17.1% at year 3). In the active treatment arm, we observed a direct effect of finerenone on UACR, which was sustained throughout the follow-up. The maximum reduction in UACR was achieved after 1 year (− 35.1% change from baseline), followed by slight increases over time to − 20.4% at 3 years.
The eGFR data at selected scheduled visits (baseline, month 4 and yearly visits) are visualised in Fig. S2 of the ESM. In the finerenone treatment group, we observed an initial median 3.3 mL/min/1.73 m2 decline in eGFR after 4 months, compared with a median 0.8 mL/min/1.73 m2 decline in the placebo group. By year 2, the median eGFR of the placebo group is slightly below the median of the finerenone group, indicating that the ‘curves’ cross again within 2 years.
3.2 UACR Model
The UACR PK/PD model was developed according to Fig. 1 and described the absolute UACR over time. The final NONMEM model code is provided in the ESM.
In the model, the rate of UACR change over time was largely proportional to the current UACR. However, a pure proportional progression model over-estimated the occurrence of very high and very low values of UACR (95th percentile of UACR was over-predicted, 5th percentile under-predicted). Therefore, in the model, the progression rate was adjusted based on model-predicted UACR as well as UACR over baseline. The effect of finerenone on UACR was characterised by a power function and an effect compartment that equilibrates with finerenone exposure. Tested covariates are listed in Table 1, and covariates included in the final model were baseline UACR and eGFR, hepatic impairment, age and ethnicity.
Overall, at the population level, the UACR model describes the longitudinal data well as illustrated by the VPC in Fig. 2. Additional VPCs, goodness-of-fit plots and parameter estimates of the final UACR model are provided in the ESM.

Visual predictive check of absolute urine albumin-to-creatinine ratio (UACR) over time, stratified by baseline UACR quartiles and treatment arm. Solid lines depict the observed median UACR, dashed lines the observed 5th and 95th percentiles and the grey areas show the intervals of these statistics in the simulations, which include variability (inter-individual and residual error) but not parameter uncertainty. ACT active treatment arm, PLAC placebo arm
To illustrate typical treatment effects in FIDELIO-DKD, the model was simulated for a typical patient with constant treatment, i.e. without considering variability or dose titration. These dose–response simulations are shown in Fig. 3A. Although there is a more pronounced UACR reduction with finerenone 20 mg OD compared with 10 mg, the additional reduction is subproportional indicating that the effect starts to saturate towards the higher dose.

Simulated time courses of urine albumin-to-creatinine ratio (UACR) over baseline (A) and estimated glomerular filtration rate (eGFR) (B) comparing different once-daily finerenone doses, and effects of finerenone discontinuation after 3 years on eGFR (C) in a typical patient that is not using sodium-glucose co-transporter-2 inhibitors (SGLT2is) concomitantly. Lines depict the simulated UACR ratio over baseline or eGFR during a 4-year period in a typical patient
3.3 eGFR Model
In addition, the eGFR PK/PD model was developed according to Fig. 1 and described the absolute eGFR over time. Again, the final model equations are provided as part of the NONMEM analysis code in the ESM.
The rate of eGFR decline over time was characterised by an absolute change over time, i.e. the rate of decline is independent of the current eGFR and characterised by a constant chronic slope. Because a purely additive progression model over-estimated the occurrence of very low values of eGFR and would result in negative predicted eGFR values, the disease progression model also contains an exponential function, which reduces the rate of eGFR decline to 0 when eGFR levels approach a stabilisation point (estimated at 16.2 mL/min/1.73 m2).
Two finerenone treatment effects were identified: (i) an acute eGFR decreasing effect and (ii) a superimposed flattening of the chronic slope. The acute eGFR decline was characterised by a power function and an effect compartment that equilibrates with finerenone exposure. In line with a previous analysis based on the phase IIb study ARTS-DN [14], a model assuming full reversibility of the acute eGFR decline described the data well, including those after finerenone discontinuation, supporting the assumption. Additional data analyses (model-free) correcting for eGFR decline also under standard of care were conducted demonstrating a ‘rebound’ (eGFR increase of 6.9%, [95% confidence interval (CI): + 3.9% to + 10.0%], compared with a simulated model-based acute decline for finerenone 20 mg OD of 5.4%) for subjects discontinuing treatment in FIDELIO-DKD with a median time window between treatment start and discontinuation of 1.8 years (5th–95th percentiles: 0.4 to 3.6 years) and an eGFR follow-up assessment within 90 days after discontinuation, as detailed in the ESM.
3.4 UACR as a Predictor of eGFR
As UACR at baseline was a strong predictor of eGFR decline, we further explored how well (model-predicted) longitudinal UACR characterised eGFR decline. The model-predicted individual UACR over time was directly linked to the chronic eGFR slope, which strongly improved (p < 1e−16) the fit compared with models where the observed baseline UACR was used. Longitudinal UACR characterised the eGFR decline both on placebo and finerenone treatment, i.e. with the effect of model-predicted UACR linked to the chronic eGFR slope, the drug effects of finerenone on UACR propagate to eGFR. For finerenone treatment, no additional UACR-independent effect on the chronic eGFR slope could be identified, suggesting that the sustainable benefit on long-term eGFR decline can be completely characterised by its immediate effect on UACR.
This is further supported by data-based visualisations shown in Fig. 4, where the observed eGFR change between year 1 and 3, as a data-based approximation of the chronic slope, is shown in dependence of either baseline UACR (Fig. 4A) or UACR at year 1 (Fig. 4B). Although the chronic eGFR decline is attenuated on finerenone compared with placebo for a given baseline UACR, this difference seems to vanish once the effect of finerenone on UACR has been established. By year 1, when the effect of finerenone on UACR reaches its maximum, the chronic eGFR decline does not differ between finerenone and placebo for a given UACR at year 1. However, UACR is lower for finerenone-treated subjects. Thus, the beneficial effect of finerenone can be explained via its UACR effect at year 1, i.e. the attenuated chronic eGFR decline between year 1 and 3 on finerenone compared with placebo is mediated via its UACR reduction during year 1.

Observed estimated glomerular filtration rate (eGFR) change between ‘year 1’ and ‘year 3’ visit vs baseline urine albumin-to-creatinine ratio (UACR) (A) and vs observed UACR at ‘year 1’ visit (B). (A) In the linear model with baseline UACR as the only other predictor, active treatment has a significantly higher value of eGFR change (i.e. reduced eGFR decline) compared with placebo (p = 3.88e−05). (B) In the linear model with UACR at ‘year 1’ visit as the only other predictor, study treatment (‘active treatment’ vs ‘placebo’) is not a significant predictor of the eGFR change between ‘year 1’ and year 3’ (p = 0.075). Solid lines indicate the trend line (linear model) estimated separately for active treatment and placebo. Open circles indicate individual data points, whereas the larger solid circles indicate the median observed eGFR change between ‘year 1’ and ‘year 3’ visit vs median baseline UACR (A) or median observed UACR at ‘year 1’ visit (B)
Significant covariates included in the final eGFR model were baseline eGFR and serum potassium, hepatic impairment, and ethnicity in addition to the covariates influencing UACR and propagating to eGFR. Overall, at the population level, the eGFR model represents the longitudinal data well, as illustrated by the VPC in Fig. 5. Additional VPCs, goodness-of-fit plots and the parameter estimates of the final eGFR model are provided in the ESM.

Visual predictive check of absolute estimated glomerular filtration rate (eGFR) over time, stratified by baseline urine albumin-to-creatinine ratio (UACR) quartiles and treatment. Solid lines depict the observed median eGFR, dashed lines indicate the observed 5th and 95th percentiles and the grey areas show the intervals of these statistics in the simulations, which include variability (inter-individual and residual error) but not parameter uncertainty. ACT active treatment arm, PLAC placebo arm, SGLT2i sodium-glucose co-transporter-2 inhibitor
The covariate effect sizes for both eGFR and UACR models are illustrated in Table 2. For the subset of these covariates that impact the dose–response relationship of finerenone on chronic eGFR decline, their impact is illustrated in Table 3.
To illustrate typical treatment effects in FIDELIO-DKD, the model was simulated for a typical patient with constant treatment, i.e. without considering variability or dose titration, and dose–response simulations are shown in Fig. 3B. Although there is a more pronounced acute eGFR decline as well as a more pronounced attenuation of chronic eGFR decline with finerenone 20 mg OD compared with 10 mg, the effect saturates towards the higher dose. Figure 3C illustrates the reversibility of the acute decline leading to a ‘rebound’ when finerenone is discontinued.
3.5 Impact of Concomitant SGLT2i Use
We identified SGLT2i effects using data from both the placebo as well as the finerenone treatment arms, first assessing an SGLT2i treatment effect per se (independent of finerenone), and subsequently testing if SGLT2i use modified the treatment effect of finerenone.
3.5.1 UACR
The effect of SGLT2i use was modelled as a direct proportional effect on UACR, as a model with an estimated time to steady-state did not describe the data better (p > 0.001). There was no significant effect of SGLT2is on the effect of finerenone, suggesting independent effects of finerenone and SGLT2is on UACR. We estimated the (non-significant) effect of SGLT2i use on the effect of finerenone. The 95% CI of the interaction effect (94.1–122%) suggests with 97.5% confidence that finerenone is at least 94.1% as efficacious in reducing UACR in patients currently using an SGLT2i compared with patients not currently using an SGLT2i. Simulations for typical patients receiving placebo or finerenone in addition to standard of care with or without SGLT2is are shown in Fig. 6A, illustrating the additive nature of SGLT2is and the effects of finerenone.

Simulation of progression of the urine albumin-to-creatinine ratio (UACR) (A) and estimated glomerular filtration rate (eGFR) (B), comparing placebo treatment and finerenone 20 mg once-daily treatment, with or without a sodium-glucose co-transporter-2 inhibitor (SGLT2i), in a typical patient. Solid lines depict the simulated UACR and eGFR over a 4-year treatment period at a constant dose level for a typical patient. Dashed lines are used for the first 6 months of simulated progression under SGLT2i treatment to reflect the fact that the dynamics of the onset of the effect of SGLT2is could not be estimated from the current dataset
3.5.2 eGFR
The acute reversible eGFR decline with SGLT2i use was modelled as a direct effect on eGFR, as a model with an estimated time to steady-state did not describe the data better (p > 0.001). With the effect of model-predicted UACR linked to the chronic eGFR slope, also the drug effects of SGLT2is on UACR propagate to eGFR. However, for SGLT2is, an additional UACR-independent treatment effect on the chronic eGFR slope was identified.
There was neither a significant effect of current SGLT2is on the acute eGFR-decreasing effect of finerenone nor on its UACR-mediated effect on the chronic eGFR slope, suggesting independence of the effects of finerenone and SGLT2is on eGFR. We estimated the (non-significant) effect of SGLT2i use on the acute eGFR decline and the UACR-mediated effect of finerenone on the chronic eGFR slope and the 95% CIs of the interaction effect are 73.2–120% and 9.5–144%, respectively.
Simulations for typical patients receiving placebo or finerenone in addition to standard of care with or without SGLT2i are shown in Fig. 6B, illustrating the additive nature of SGLT2i and the drug effects of finerenone. The effect sizes of different doses of finerenone on UACR and eGFR as well as of an SGLT2i alone or in combination with finerenone are also summarised in Table 4.
4 Discussion
The presented finerenone dose–exposure UACR and eGFR response models considering time-varying SGLT2i use provide an accurate representation of the clinical data from FIDELIO-DKD. These integrated analyses enabled a detailed investigation of the interaction of the biomarkers UACR and eGFR as well as the drugs finerenone and SGLT2is.
4.1 Acute Reversible Decline and Sustainable Chronic Improvement of eGFR
Renal function decline, slow in ageing healthy individuals or accelerated in CKD, is characterised by a largely constant eGFR decline rate over time that can be approximated by a linear model with a characteristic (chronic) eGFR slope modifiable with treatment [11, 15, 16]. Placebo data from FIDELIO-DKD show the same characteristics and could be used to derive an accurate disease progression model for the phase III trial population.
Estimated glomerular filtration rate decline in finerenone-treated patients shows a biphasic pattern as confirmed during model development. Although the finerenone treatment introduced an acute decline as a one-time offset to the chronic decline within the first weeks, the sustained attenuation of the chronic decline slope introduces benefits that are increasing over time and eventually outweigh acute effects. Further, the acute decline was reversible and is generally considered to represent hemodynamic effects, where even an eGFR decline is rather considered beneficial for the kidney than representing disease progression [17,18,19].
4.2 Short-Term Effects of Finerenone on UACR as a Predictor of Chronic eGFR Benefits
Prior studies have shown that UACR is an established renal and cardiovascular risk factor in patients with CKD and type 2 diabetes. Additionally, in the FIDELIO-DKD study, UACR levels at baseline predicted the rate of eGFR decline in both the finerenone and placebo arms. The strong epidemiological association between UACR and kidney failure supported further analyses to investigate whether UACR qualifies as a valid surrogate outcome for trials of CKD progression. A meta-analysis of randomised controlled trials demonstrated that early treatment effects on UACR are associated with treatment effects on established endpoints, suggesting a role for UACR as a surrogate outcome for kidney failure [20, 21]. Other studies more specifically investigated ACE inhibitors and ARBs [22, 23], SGLT2is [24, 25] and glucagon-like peptide-1 receptor agonists [26]; however, whether the validity of UACR as a surrogate outcome extends to novel therapies including (nonsteroidal) MRAs is unknown. In the developed eGFR model, a single mathematical function characterised the relationship between UACR and chronic eGFR decline, regardless whether patients were receiving placebo or finerenone treatment. Adding a UACR-independent drug effect did not improve the eGFR model, suggesting that the effect of finerenone on eGFR can be attributed, at least to a large extent, to its effect on UACR. We note, however, that these analyses do not prove a causal association between early treatment effects on UACR and treatment effects on eGFR slope with finerenone, i.e. while UACR is driving eGFR decline in the model, this may not represent the true pathophysiological relationship where UACR could also simply represent the more sensitive parameter. Yet, these analyses do support the validity of UACR as a surrogate and early response biomarker for the long-term effect of finerenone in slowing the decline of eGFR. Simulations with the finerenone dose–exposure–response model illustrate the fast onset of UACR effects, whereas benefits on eGFR only become visible when the reduction in chronic eGFR decline outweighs the initial decline upon treatment initiation (Fig. 3).
4.3 Impact of Patient Characteristics on Finerenone Pharmacodynamics
Several covariates were identified that affected UACR/eGFR or the effect of finerenone on these biomarkers. For covariates affecting the effect of finerenone on chronic eGFR decline (Table 3), the simulated effect of finerenone 20 mg OD on the chronic eGFR slope ranged from reducing the slope relative to placebo treatment by − 22.1% (in patients with high baseline UACR of 3366 mg/g) to − 41.3% (in patients with low baseline eGFR of 26.7 mL/min/1.73 m2). Interestingly, the proportional effect of finerenone on eGFR decline is lower for both the low UACR and high UACR scenario, compared with the reference subject with median UACR. In subjects with low UACR, the impact of UACR on chronic eGFR decline is more modest and correspondingly, the impact of finerenone on the reduction of UACR has a smaller proportional effect on eGFR decline. For subjects with high UACR, the reduced proportional effect on chronic eGFR decline is explained by a smaller proportional reduction of UACR by finerenone, caused by the covariate effect of baseline UACR on the UACR drug effect of finerenone. However, despite the fact that patients with high baseline UACR have the lowest proportional finerenone effect on chronic eGFR decline, because of their high baseline rate of eGFR decline, it takes less time before the beneficial finerenone effect on eGFR decline outweighs the acute eGFR-decreasing effect of finerenone. The opposite is true for patients with a low UACR, as they typically have a low rate of decline.
4.4 Additive Treatment Effects of Finerenone and SGLT2is
While FIDELIO-DKD was not designed to demonstrate SGLT2i effects, finerenone but also SGLT2is showed strong and highly significant treatment effects on UACR and eGFR in FIDELIO-DKD. Based on the limited number of subjects and, more importantly, based on the trial not being randomised for SGLT2i use, the quantitative effect sizes estimated for SGLT2i should be interpreted with caution as these may be confounded by selection bias. In addition, the data did not support estimating the dynamics of SGLTI2i treatment onset. However, the data do allow reliable conclusions on the interaction of SGLT2i and finerenone. Concomitant SGLT2i use did not statistically significantly modify the treatment effect of finerenone in the presented analyses. This indicates independent and additive effects of SGLT2i in addition to finerenone. Confidence intervals are narrow for UACR where the analysis provides 97.5% confidence that finerenone is at least 94.1% as efficacious in reducing UACR in patients currently using SGLT2is compared with patients not currently using SGLT2is. Furthermore, a dose–exposure–time-to-event analysis of FIDELIO-DKD recently indicated additive effects on the renal outcome, though with lower confidence based on the limited number of subjects with events [10], where also potential advantages of exposure–response analyses compared with subgroup analyses have been discussed.
Based on the two independent modes of action, complementing benefits on slowing renal disease progression may be expected; however, empirical data were lacking. The presented clinical evidence is further supported by recent data from a preclinical model of hypertension-induced end-organ damage, where cardiorenal protection of finerenone and empagliflozin monotherapy and combination therapy was investigated. Monotherapies dose-dependently reduced proteinuria, whereas a low-dose combination revealed an early, sustained and even over-additive reduction in proteinuria, as well as effects on additional functional parameters and mortality [27].
Simulating combined treatment effects illustrate (Fig. 6), in comparison to either single treatment effect, larger UACR reductions, a more pronounced acute eGFR decline and a further attenuated chronic eGFR slope. Because of the acute eGFR decreasing effect of both SGLT2is and finerenone, it takes time for the additive benefits to manifest in terms of eGFR; however, the attenuated chronic slope can provide sustainable long-term benefits for patients [28].
5 Conclusions
In summary, the finerenone dose–exposure–response analyses for UACR and eGFR based on FIDELIO-DKD data provide detailed insights into its effects on relevant biomarkers of surrogate quality supporting the benefits of finerenone for patients with CKD with type 2 diabetes. The analyses further reveal that treatment effects on UACR are predictive for finerenone treatment effects on chronic eGFR decline. Finally, the analyses demonstrate additive benefits of SGLT2i use in addition to finerenone for UACR and eGFR.
References
Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–306.
Heerspink HJL, Stefansson BV, Correa-Rotter R, Chertow GM, Greene T, Hou FF, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383(15):1436–46.
Bakris GL, Agarwal R, Anker SD, Pitt B, Ruilope LM, Rossing P, et al. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med. 2020;383(23):2219–29.
Thompson A, Smith K, Lawrence J. Change in estimated GFR and albuminuria as end points in clinical trials: a viewpoint from the FDA. Am J Kidney Dis. 2020;75(1):4–5.
Holtkamp F, Gudmundsdottir H, Maciulaitis R, Benda N, Thomson A, Vetter T. Change in albuminuria and estimated GFR as end points for clinical trials in early stages of CKD: a perspective from European regulators. Am J Kidney Dis. 2020;75(1):6–8.
Levey AS, Gansevoort RT, Coresh J, Inker LA, Heerspink HL, Grams ME, et al. Change in albuminuria and GFR as end points for clinical trials in early stages of CKD: a scientific workshop sponsored by the National Kidney Foundation in collaboration with the US Food and Drug Administration and European Medicines Agency. Am J Kidney Dis. 2020;75(1):84–104.
Bakris GL, Agarwal R, Anker SD, Pitt B, Ruilope LM, Nowack C, et al. Design and baseline characteristics of the finerenone in reducing kidney failure and disease progression in diabetic kidney disease trial. Am J Nephrol. 2019;50(5):333–44.
Filippatos G, Anker SD, Agarwal R, Pitt B, Ruilope LM, Rossing P, et al. Finerenone and cardiovascular outcomes in patients with chronic kidney disease and type 2 diabetes. Circulation. 2020.
Goulooze B, Snelder N, Seelmann A, Horvat-Broecker A, Brinker M, Joseph A, Garmann D, Lippert J, Eissing T. Finerenone dose-exposure-serum potassium response analysis of FIDELIO-DKD phase 3: the role of dosing, titration, and inclusion criteria. Clin Pharmacokinet. 2022. https://doi.org/10.1007/s40262-021-01083-1.
van den Berg P, Ruppert M, Mesic E, Snelder N, Seelmann A, Heinig R, Joseph A, Garmann D, Lippert J, Eissing T. Finerenone dose-exposure-primary efficacy response in FIDELIO-DKD phase 3—population pharmacokinetic and time-to-event analysis. Clin Pharmacokinet. 2022. https://doi.org/10.1007/s40262-021-01082-2.
Vonesh E, Tighiouart H, Ying J, Heerspink HL, Lewis J, Staplin N, Inker L, Greene T. Mixed-effects models for slope-based endpoints in clinical trials of chronic kidney disease. Stat Med. 2019;38(22):4218–39.
Levey AS, Inker LA, Matsushita K, Greene T, Willis K, Lewis E, de Zeeuw D, Cheung AK, Coresh J. GFR decline as an end point for clinical trials in CKD: a scientific workshop sponsored by the National Kidney Foundation and the US Food and Drug Administration. Am J Kidney Dis. 2014;64(6):821–35.
Karlsson MO, Holford N. A tutorial on visual predictive checks. 2008;abstract 1434: p. 17. www.page-meeting.org/?abstract=1434. Accessed 8 Apr 2022.
Snelder N, Heinig R, Drenth HJ, Joseph A, Kolkhof P, Lippert J, et al. Population pharmacokinetic and exposure-response analysis of finerenone: insights based on phase IIb data and simulations to support dose selection for pivotal trials in type 2 diabetes with chronic kidney disease. Clin Pharmacokinet. 2020;59(3):359–70.
Inker LA, Heerspink HJL, Tighiouart H, Levey AS, Coresh J, Gansevoort RT, et al. GFR slope as a surrogate end point for kidney disease progression in clinical trials: a meta-analysis of treatment effects of randomized controlled trials. J Am Soc Nephrol. 2019;30(9):1735–45.
Weldegiorgis M, de Zeeuw D, Heerspink HJ. Renal end points in clinical trials of kidney disease. Curr Opin Nephrol Hypertens. 2015;24(3):284–9.
Brenner BM, Meyer TW, Hostetter TH. Dietary protein intake and the progressive nature of kidney disease: the role of hemodynamically mediated glomerular injury in the pathogenesis of progressive glomerular sclerosis in aging, renal ablation, and intrinsic renal disease. N Engl J Med. 1982;307(11):652–9.
Holtkamp FA, de Zeeuw D, Thomas MC, Cooper ME, de Graeff PA, Hillege HJ, Parving HH, et al. An acute fall in estimated glomerular filtration rate during treatment with losartan predicts a slower decrease in long-term renal function. Kidney Int. 2011;80(3):282–7.
Weir MR. Acute fall in glomerular filtration rate with renin-angiotensin system inhibition: a biomeasure of therapeutic success? Kidney Int. 2011;80(3):235–7.
Waijer SW, Gansevoort RT, Heerspink HJL. Change in albuminuria as a surrogate endpoint. Curr Opin Nephrol Hypertens. 2019;28(6):519–26.
Heerspink HJL, Greene T, Tighiouart H, Gansevoort RT, Coresh J, Simon AL, et al. Change in albuminuria as a surrogate endpoint for progression of kidney disease: a meta-analysis of treatment effects in randomised clinical trials. Lancet Diabetes Endocrinol. 2019;7(2):128–39.
de Zeeuw D, Remuzzi G, Parving HH, Keane WF, Zhang Z, Shahinfar S, et al. Proteinuria, a target for renoprotection in patients with type 2 diabetic nephropathy: lessons from RENAAL. Kidney Int. 2004;65(6):2309–20.
Heerspink HJ, Ninomiya T, Persson F, Brenner BM, Brunel P, Chaturvedi N, et al. Is a reduction in albuminuria associated with renal and cardiovascular protection? A post hoc analysis of the ALTITUDE trial. Diabetes Obesity Metab. 2016;18(2):169–77.
Oshima M, Neuen BL, Li J, Perkovic V, Charytan DM, de Zeeuw D, et al. Early change in albuminuria with canagliflozin predicts kidney and cardiovascular outcomes: a post hoc analysis from the CREDENCE trial. J Am Soc Nephrol. 2020;31(12):2925–36.
Jongs N, Greene T, Chertow GM, McMurray JJV, Langkilde AM, Correa-Rotter R, et al. Effect of dapagliflozin on urinary albumin excretion in patients with chronic kidney disease with and without type 2 diabetes: a prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021;9(11):755–66.
Persson F, Bain SC, Mosenzon O, Heerspink HJL, Mann JFE, Pratley R, et al. Changes in albuminuria predict cardiovascular and renal outcomes in type 2 diabetes: a post hoc analysis of the LEADER Trial. Diabetes Care. 2021;44(4):1020–6.
Kolkhof P, Hartmann E, Freyberger A, Pavkovic M, Mathar I, Sandner P, et al. Effects of finerenone combined with empagliflozin in a model of hypertension-induced end-organ damage. Am J Nephrol. 2021;52(8):642–52.
Meraz-Muñoz AY, Weinstein J, Wald R. eGFR decline after SGLT2 inhibitor initiation: the tortoise and the hare reimagined. Kidney. 2021;360:1042–7.
Acknowledgements
The authors thank the FIDELIO-DKD Committees, investigators and patients; Andreas Seelmann (Bayer) for pharmacometric analysis dataset creation; Dirk Garmann (Bayer) for discussion; and Sissy Stauffenberg (ClinStat), Martin Gebel, Cosima Klein, Aziz Tuermer, Jacobus Buytendach and Patrick Schloemer (Bayer) for derived variables and information about data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
LAP&P conducted the analysis as contract research for Bayer. However, LAP&P (SCG, MvN, NS) and HJLH were not paid to contribute to manuscript preparation.
Conflict of Interest
SCG, MvN and NS are employed by LAP&P, a CRO working for Bayer. HJLH is co-chairing the executive committee of the ongoing finerenone FIND-CKD trial and advising Bayer including payments. He also had and has various roles in several SGLT2i trials. MB, JL and TE are Bayer employees and potential shareholders of Bayer AG.
Ethics approval
The study protocol was approved by international review boards, independent ethics committees, and competent authorities according to national and international regulations. FIDELIO-DKD was conducted in accordance with the ICH Harmonized Tripartite Guideline for Good Clinical Practice.
Consent to participate
All study participants provided written informed consent before entering the study.
Consent for publication
All study participants provided written informed consent before entering the study.
Availability of data and material
Data will be made available in an electronic repository in the future, at a date to be specified by Bayer.
Code availability
NONMEM analyses codes are provided as Electronic Supplementary Material.
Author contributions
SCG: wrote the manuscript, designed the research, performed the population PK/PD analysis and analysed the data; HJLH: wrote the manuscript and designed the research; MvN: performed the population PK/PD analysis and analysed the data; NS: designed the research, supported the population PK/PD analysis and analysed the data; MB: designed the research; JL: designed the research and wrote the manuscript; TE: wrote the manuscript and designed and steered analysis and research.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Goulooze, S.C., Heerspink, H.J.L., van Noort, M. et al. Dose–Exposure–Response Analysis of the Nonsteroidal Mineralocorticoid Receptor Antagonist Finerenone on UACR and eGFR: An Analysis from FIDELIO-DKD. Clin Pharmacokinet 61, 1013–1025 (2022). https://doi.org/10.1007/s40262-022-01124-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-022-01124-3