
Abstract
Background and Objectives
Acoziborole is a novel boron-containing candidate developed as an oral drug for the treatment of human African trypanosomiasis (HAT). Results from preclinical studies allowed progression to Phase 1 trials. We aimed to determine the best dose regimen for all stages of HAT.
Methods
Acoziborole was assessed in 128 healthy adult males of sub-Saharan African origin living in France. The study included a single oral administration of a 20- to 1200-mg dose in a randomised double-blind study in cohorts of 8 (6 active, 2 placebo) to assess safety, tolerability, and pharmacokinetics. In three additional open cohorts of 6 participants, the effect of activated charcoal was evaluated, bioequivalence of capsules versus tablets was assessed, and safety in the 960-mg tablet cohorts was monitored.
Results
Acoziborole was well tolerated at all doses tested; no dose-related adverse events were observed. The drug appeared rapidly in plasma (at 1 h), reached tmax between 24 and 72 h, and remained stable for up to 96 h, after which a slow decrease was quantifiable until 14 weeks after dosing. Charcoal had little impact on the enterohepatic recirculation effect, except for the 20-mg dose. Bioequivalence between capsule and tablet formulations was demonstrated. The therapeutic single dose for administration under fasted conditions was fixed to 960 mg. The maximum administered dose was 1200 mg.
Conclusions
This study showed that acoziborole could be safely assessed in patients as a potential single-dose oral cure for both stages of gambiense HAT.
Trial Registration
The study was registered with ClinicalTrials.gov: NCT01533961.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Acoziborole is a novel boron-containing candidate developed as an oral drug for the treatment of human African trypanosomiasis (HAT). This Phase I study in three parts assessed acoziborole for safety, tolerability, pharmacokinetics, and the bioequivalence of capsules versus tablets and aimed to determine the therapeutic dose. This study showed that acoziborole could be safely assessed in patients as a potential single-dose oral cure for both stages of gambiense HAT. |
1 Introduction
Human African trypanosomiasis (HAT), or sleeping sickness, is a life-threatening vector-borne parasitic disease transmitted through the bite of the tsetse fly [1, 2]. Over 95% of HAT cases are caused by the Trypanosoma brucei gambiense parasite (g-HAT), with the remainder following infection with T. b. rhodesiense (r-HAT). Both forms of the disease occur in two clinical stages: a first haemolymphatic stage, when parasites reside in the blood and lymphatic system, and a second meningoencephalitic stage, which occurs once the parasite has crossed the blood–brain barrier (BBB), resulting in severe neurological symptoms that, without treatment, progress to coma and eventually death [1, 2]. In 2010–2014, 10.85 million people were living at medium to high risk of infection with T. b. gambiense according WHO [3]. In 2012, at the start of this study, a total of 7092 new cases of g-HAT were reported by WHO; this number had reduced to 565 in 2020 [4, 5].
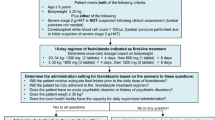
In 2012, at study start, the first-line treatment for stage 2 g-HAT was nifurtimox eflornithine combination therapy (NECT) [1, 6, 7]. It replaced eflornithine monotherapy in 2009, and although it was highly efficacious, this treatment was not optimal as it required slow intravenous administration of eflornithine (14 infusions over 7 days), a procedure that can only be performed by well-trained staff in a hospital setting [1, 6, 7]. Fexinidazole, a new 10-day oral treatment, was approved in 2018 in the Democratic Republic of the Congo (DRC) after the positive opinion of European Medicines Agency (EMA). It was included in the WHO guidelines in 2019 as a first-line treatment for both stages of g-HAT [8,9,10,11,12], and was approved by the US Food and Drug Administration (FDA) in 2021.
However, a new oral treatment was considered necessary to simplify treatment for both stages with no cumbersome parasitological explorations. Acoziborole (SCYX-7158), a novel boron-containing drug candidate [13,14,15], was included in the Drugs for Neglected Diseases Initiative (DNDi) lead optimisation programme in 2007 in collaboration with Anacor, SCYNEXIS, and the Swiss Tropical and Public Health Institute. Its excellent in vitro activity against Trypanosoma brucei spp, outstanding physicochemical properties (chemically stable, BCS class 2, pKa = 9.61, logD at pH 7.4 = 3.51, non-hydroscopic, no acid- or photodegradation) and reassuring toxicokinetics, which led us to expect a possible long half-life in human, allowed for a first-in-man study in 2012 [13, 14]. This combined single ascending dose/multiple ascending dose (SAD/MAD) study, aimed to investigate the safety, tolerability and pharmacokinetics of SCYX-7158 in humans, whose protocol was designed with flexibility for potential amendment, is described here.
2 Methods
2.1 Participants and Procedures
This study was conducted in accordance with the Declaration of Helsinki, French Huriet law (No. 2004-806), and Good Clinical Practice guidelines [16]. The protocol and amendments were approved by the Committee of Protection of Persons (Paris, France) and by the national competent authority (Agence Nationale de Sécurité du Médicament). Written informed consent was obtained from all participants. Details of study design and analytical methods employed are provided in Online Resource 1. Healthy male volunteers of sub-Saharan origin aged 18–45 years with a body mass index of 18–28 kg/m2 living in France were eligible for inclusion. Exclusion criteria included history of gastrointestinal (GI) disturbances, or a positive drug screening test.
2.2 Study Drugs
The interventional product acoziborole was administered in either 20 mg or 80 mg capsules with matching placebo (Penn Pharma, Tredegar, UK) or in 40 mg or 160 mg tablets (Patheon Pharmaceutical Development, Swindon, UK). Activated charcoal (Toxicarb®) was used in oral suspension (20 g/100 mL). The 20-mg starting dose in the initial SAD study was based on the 15 mg/kg/day no observed adverse effect level determined in 4-week toxicity studies in rat and dog.
2.3 Design of Studies
The study was initially designed in three parts: safety and tolerability of oral single ascending doses of acoziborole (I), food effect (II), and safety and tolerability of oral multiple ascending doses (III). However, after the lowest dose of acoziborole (20 mg), it was found that the half-life in human (t1/2 > 400 h) was longer than predicted from preclinical data. Part I was suspended while additional preclinical pharmacokinetic studies in dogs, including charcoal-block methodology to evaluate the adsorption on charcoal and bile-duct cannulation, were conducted that highlighted mild enterohepatic recirculation of acoziborole. The protocol was amended as presented in Table 1 and a Safety Review Committee (SRC) constituted to oversee ascending-dose studies.
2.4 Study Protocol
Part I was a randomised, double-blind, within-cohort placebo-controlled SAD study of oral doses of acoziborole ranging from 20 to 1200 mg in capsule or tablet form, to determine the safety and tolerability of the drug. All cohorts, except 1 and 9, also received once-daily activated charcoal (60 g) in oral suspension (300 mL) for 7 days starting from Day 5. For Cohort 1, blood samples were taken up to 168 h post-dose; for Cohorts 2–14, blood samples were collected up to 240 h and then at every ambulatory visit. Cerebrospinal fluid (CSF) was collected on Day 5 in cohorts 7 and 8. Participants were monitored for adverse events (AEs), physical signs, vital signs, electrocardiogram (ECG) findings, and changes in clinical laboratory tests (haematology, biochemistry, and urinalysis). Quintuplicate ECGs were averaged from 24-h continuous ECG Holter recordings taken for cohorts 7–14 on up to 3 separate days. Triplicate ECGs were recorded in cohorts 9 and 12–14 on three separate days and five follow-up visits. Safety and plasma pharmacokinetic (PK) data from Day 15 post-dose were reviewed in a blinded fashion by the SRC prior to administration of the next dose. Blood samples for plasma PK analysis were collected over a follow-up period of 6 months after the end-of-study, or until the plasma concentration of acoziborole was below the level of quantification (BLQ).
Parts II (food effect) and III (multiple dose escalation) were cancelled following the first dose in part one due to the long half-life of acoziborole in healthy volunteers.
Part IV was an intermediate open-label pharmacokinetic study to assess the effect of activated charcoal on the plasma concentration of acoziborole, following the results of the bile-duct cannulation in dogs. Two cohorts of three participants received charcoal 24 h after administration of a single oral dose of 20 mg acoziborole in capsule form. Cohort 1 received 60 g activated charcoal 10 minutes before breakfast for seven days. Cohort 2 received 20 g activated charcoal three times daily 10 minutes before each meal for 7 days. Blood samples were collected up to 192 h post-dose for PK analysis. Participants were monitored as in part I. Data were reviewed by the SRC to determine an adapted treatment schedule of acoziborole with charcoal to allow resumption of part I.
Part VI was a complementary open-label study in two cohorts of six participants to evaluate the bioavailability of acoziborole in tablet compared with capsule form (part I). Each cohort received a single dose of either 40 or 160 mg acoziborole in tablet form. To explore the impact of high-dose activated charcoal on acoziborole pharmacokinetics, both cohorts received 50 g activated charcoal starting on Day 5 in the morning, and every 4 h for 3 days, and one single dose of charcoal on follow-up visits. The same monitoring was applied as in part I.
Levels of acoziborole and its metabolite SCYX-3109 were determined in plasma and cerebrospinal fluid (CSF). Details of treatment duration, dosage regimen, criteria for evaluation, and sample (blood, urine, CSF) collection are given on page 4 of online resource 1.
2.5 Pharmacokinetic Analysis
Levels of SCYX-7158 and its metabolite SCYX-3109 were determined in plasma and analysed on a Kinetex C18, 2.6 µm, 50 × 3.0 mm I.D. column using a validated liquid chromatography–tandem mass spectrometry (LCMS/MS) method. In lithium heparinised plasma, the quantification limit of SCYX-7158 and SCYX-3109 was 0.25 ng/mL and 10 ng/mL, respectively.
Pharmacokinetic parameters for acoziborole and its metabolite SCYX-3109 were estimated using non-compartmental methods (Phoenix WinNonlin® software, version 6.3, Pharsight Corporation, Mountain View, CA, USA). The plasma pharmacokinetic parameters studied were: maximum plasma concentration (Cmax); time to reach Cmax (tmax); time to the start of absorption (tlag); elimination rate constant (ke), determined by log-linear regression using at least three time points on the terminal phase including the last time point and excluding Cmax; terminal elimination half-life (t1/2), determined by linear regression using at least three time points; area under the plasma concentration–time curve (AUC) from time zero to 96 h post-dose (AUC0–96) before the administration of activated charcoal, AUC from time zero to the last measurable concentration (AUC0–t), and AUC and from time zero to infinity (AUC0–∞), all determined by a linear trapezoidal method. Free fraction of the drug in plasma was calculated using the ratio of the free plasma concentration to the total plasma concentration, multiplied by 100. The fraction of the drug in CSF was calculated using the ratio of the CSF concentration to the total plasma concentration, multiplied by 100.
2.6 Statistical Analysis
All plasma concentrations were summarised by dose level or treatment. The derived PK parameters were listed by participant and summarised by dose level or treatment and day where appropriate. Similar descriptive statistics were presented for acoziborole plasma free fraction concentrations by dose level. Moreover, ratios of each free fraction concentration to the matching plasma concentration were calculated and similar descriptive concentrations were presented by dose level.
In part I, AUC0–96 and Cmax values were analysed for dose proportionality using analysis of variance techniques, and acoziborole concentrations in CSF were summarised by dose level. Descriptive statistics were performed in part IV. In part VI, the relative bioavailability between the capsule and the tablet formulation was assessed by comparing the participants receiving the new tablet formulation at doses of 40 and 160 mg, to participants receiving the same doses using the capsule formulation in part I. The comparison was performed on Cmax and AUC0–96, which were dose-normalised, log-transformed, and evaluated using a one-way analysis of variance, including a factor for formulation. The difference between formulations (tablet and capsule) was calculated with its 90% CI.
Populations used for the analyses are summarised in Table 2, and include:
Safety Analysis Set all randomised participants, who received a dose of the study drug and have a post-randomisation safety evaluation. Participants were analysed according to the treatment schedule they actually received.
Pharmacokinetic Analysis Set all participants who completed the study and did not have any protocol deviation or events implying a bias for the PK evaluation.
Replicate ECG analysis set (part I) all participants from the safety population with reliable replicate ECG data.
All statistical analyses were performed using SAS® software, version 9.2 (SAS Institute Inc., Cary, NC, USA).
3 Results
3.1 Safety and Tolerability
A total of 102 /128 participants received acoziborole (84 in part I, 6 in part IV and 12 in part VI) and 26 received placebo. One hundred and fourteen participants also received activated charcoal. Two participants withdrew for personal reasons, one after randomisation in part I and one after randomisation in part VI—126 participants completed the study (Table 2).
After administration of study drug and before the first administration of activated charcoal, 15/102 (15%) participants receiving acoziborole reported 20 treatment-emergent AEs (TEAEs), and 3/26 (12%) participants receiving placebo reported 4 TEAEs. The occurrence of the TEAEs per treatment administered are presented in Table 3.
One serious AE (SAE) was reported (thyroid-stimulating hormone reduced below the lower normal limit, and free triiodothyronine (fT3) and thyroxine (fT4) increased above the upper normal limit), 3 months after dosing in the 240-mg dose group in part I. There were no clinical signs associated with these changes, which resolved spontaneously over time; this SAE was considered possibly related to acoziborole. No deaths or severe AEs were reported. The intensity of TEAEs varied from mild (33 in part I; 16 in part VI) to moderate (52 in part I; 24 in part VI). The most frequent acoziborole-related AEs were gastrointestinal disorders (15 events reported by 14/84 participants [16.6%] in part I; 34 events reported by 12/12 participants in part VI), investigational abnormalities (13 events reported by 13/84 participants [15.4%] in part I; 4 events reported by 4 /6 participants in part VI) and nervous system disorders (16 events reported by 14 participants in part I), see Online Resource 2. There were no dose-related TEAEs (Fig. 1).

Percentage of participants with at least one TEAE per cohort. N = 6 for all cohorts. *Without charcoal
Laboratory results showed some isolated clinically significant abnormalities, i.e., increases in creatine phosphokinase (CPK) in 6 participants (1 receiving placebo, 5 receiving acoziborole), which returned to normal levels and were considered unlikely to be related to acoziborole, and in transaminases in 6 participants (2 receiving placebo, 4 receiving acoziborole), which returned to normal levels. All six cases were considered possibly related to acoziborole and/or placebo. Overall, 13 AEs were reported by 13 (11.8%) of the 110 participants (Online Resource 3). No relevant findings were observed on physical examinations, ECG, or vital signs. The 24-h Holter analysis was conducted on seven Cohorts. Categorical analysis showed some abnormalities, mainly PR values above 200 ms observed in 7 participants who received acoziborole, none were above 220 ms. No QTc values above 450 ms were measured during the study with acoziborole and no difference was observed in morphological analysis compared to baseline or between active groups and placebo. Furthermore, the concentration/response relationship on ΔΔQTcF showed variations of limited extent. Within the limitations of the study (i.e., low participant numbers, the absence of a positive control and methodological differences between groups of cohorts), the results do not indicate an effect of acoziborole on QTcF.
3.2 Pharmacokinetics
Acoziborole exhibited rapid oral absorption and very long elimination half-life (~ 400 h), despite administration of activated charcoal. In addition, and in contrast to preclinical PK data, metabolism of acoziborole was very limited. Plasma exposure of acoziborole increased in a less than dose proportional manner across the range of 20–1200 mg. At the doses studied (40 and 160 mg) in part VI, capsule and tablet formulations of acoziborole were shown to be bioequivalent. The unbound concentration of acoziborole in CSF (0.3–4.6%) was similar to that observed in preclinical studies (0.3–3.9% in mouse). Furthermore, the unbound concentration of acoziborole in plasma appears to be a reliable indicator of CSF exposure.
3.2.1 Part I
After administration of SADs, acoziborole was slowly absorbed with a median tmax of 12 to 72 h, followed by sustained high plasma concentrations up to 96 h (Table 4). After 96 h post-dose (i.e., following charcoal administration, except for Cohorts 1 and 9), acoziborole plasma concentrations started to decrease very slowly and generally remained quantifiable up to 9 weeks post-dose for doses up to 320 mg, and up to 14 weeks post-dose for doses beyond 400 mg (Fig. 2). This decrease in plasma exposure was parallel across all cohorts that received activated charcoal; for Cohorts 1 and 9 (20 mg and 960 mg), which did not receive activated charcoal, the decrease in exposure was slower. The terminal half-life of acoziborole was 267–411 h for Cohorts with charcoal (2–8, 10–14), and 399–409 h for Cohorts without charcoal (1, 9) indicating a low charcoal effect (Table 4, Fig. 3). The rate and extent of absorption of acoziborole was less than dose proportional over the studied dose range (40–1200 mg) in Cohorts with charcoal administration (2–8, 10–14). Dose proportionality was generally comparable for AUC0–∞ and AUC0–96 (i.e., before charcoal administration). Inter-individual variability of Cmax and AUC0–∞ values was low around 16–17%.

Mean plasma concentration versus time profiles after single oral administration of increasing doses of acoziborole from 20 to 1200 mg, for Study Part I

Mean plasma concentration versus time profiles after single oral administration of 20 mg of acoziborole on Day 1, either alone in Study Part I, or followed by intensive charcoal administration from Days 2 to 8 in Study Part IV
Mean CSF levels of acoziborole of 112 and 172 ng/mL were measured 96 h post-dose in participants from Cohorts 7 and 8 (240 and 320 mg), respectively. Mean CSF-to-plasma ratios were comparable between cohorts: 2.2% and 2.6%, respectively. The concentration of unbound acoziborole, determined in samples taken across the majority of the dose range and up to 1200 mg, was found to be very low and close to the limit of quantification (LOQ). Consequently, relatively wide inter-individual variability was reported, resulting in a median unbound fraction of 0.4–3.4%. However, these data are consistent with previous in vitro measurement of unbound fraction (2.2%) and suggest acoziborole is highly bound to plasma proteins.
Plasma levels of the metabolite SCYX-3109 were generally very low (BLQ-317 ng/mL) across the dosing range (20–1200 mg) and therefore, no PK calculation was performed. Accordingly, mean CSF levels of SCYX-3109 in Cohorts 7 and 8 were also very low (0.6–0.8 ng/mL).
3.2.2 Part IV
During the first 24 h following administration of 20 mg acoziborole (prior to charcoal administration), several absorption peaks were observed in the acoziborole plasma profiles. Thereafter, despite administration of charcoal three times daily (tid) or once daily (qd), absorption peaks were observed in the plasma profiles up to 72 h. Between 72 and 192 h, plasma acoziborole levels decreased slowly with a terminal half-life of approximately 200 h. After 192 h post-dose, administration of charcoal was stopped. Plasma acoziborole levels subsequently reached concentrations comparable to those observed in Cohort 1 (20 mg dose, without charcoal) of part I, and decreased very slowly with a terminal half-life (262–497 h) comparable to that reported in part I (Fig. 3, Table 5). Plasma levels of the metabolite SCYX-3109 were BLQ.
3.2.3 Part VI
After a single administration of a tablet formulation (40 or 160 mg), acoziborole plasma concentrations appeared rapidly, increased up to 9–12 h and remained steady up to 96 h post-dose (when activated charcoal was administered) (Fig. 4). The median tmax values observed (12–24 h) were similar to those for the capsule formulation (12–30 h) used in part I (Table 6, Fig. 3). After 96 h post-dose, acoziborole plasma concentrations decreased slowly and remained quantifiable in most subjects up 7 weeks post-dose. The drop in acoziborole plasma concentration at 168 h appeared to be slightly more rapid in this part (high charcoal administration every 4 h) than that observed in part I (charcoal once daily) (Fig. 4). However, the effect seems transient, as beyond 240 h, the decrease in mean plasma concentrations was parallel between cohorts of parts I and VI. The mean terminal half-life was 327–373 h, compared to 267–270 h for the same capsule doses in part I (Table 6). AUC0–96 and Cmax values were similar for both formulations, the 90% CIs of the ratio were included within the bioequivalence range of 0.80–125 indicating that the tablet formulation dosed at 40 or 160 mg are bioequivalent to the reference capsules. Plasma levels of SCYX-3109 were BLQ in 10/12 participants. Overall, there was no noticeable difference between administration of the tablet form of acoziborole with charcoal every 4 h and administration of the capsule form of acoziborole with charcoal qd (Part I). Therefore, at 40 and 160 mg doses, the capsule and tablet formulations of acoziborole are considered bioequivalent (Table 7). The concentration of unbound acoziborole in plasma was found to be BLQ in the majority of cases after the 40 mg dose and was quite low after the 160 mg dose. Consequently, variable results were obtained with unbound fraction of ~ 1% but reaching 8% in 2 cases.

Mean plasma concentration versus time profiles after single oral administration of 40 or 160 mg of acoziborole as a capsule (Study Part I) or tablet (Study Part VI): a up to 96 h post-dose; b full follow-up period
4 Discussion
The original design of part I was based on preclinical pharmacokinetic data that showed acoziborole had a long elimination half-life (t1/2 >20 h) [13, 14]. However, following initiation of part I with the lowest dose of acoziborole (20 mg), it became clear that this was a significant underestimation of the actual half-life in human subjects (t1/2 ~ 400 h). The study was suspended to ensure the safety of participants, to allow time to develop a better understanding of the PK characteristics of acoziborole, and to amend the study design. In-depth dog PK studies, including charcoal-block methodology and bile-duct cannulation highlighted that enterohepatic recirculation of acoziborole could be responsible. Information from these studies was used to design the intermediate study, part IV, which confirmed that during administration of both charcoal regimens (20 g tid or 60 g qd, for 7 days) the elimination half-life of acoziborole was halved whilst maintaining therapeutically relevant exposure. In fact, these treatment regimens were very consistent: the mean ratio of acoziborole plasma concentration after seven days post-dose and observed Cmax was always approximately 0.50, regardless of the participant or the activated charcoal regimen. Following expert review of these data by the Ethics Committee and the Sponsor, it was decided that Study part I could be safely resumed with acoziborole and a charcoal regimen (to shorten the follow-up period).
In part I, before administration of charcoal, exposure of acoziborole was not linear with dose. However, meaningful increases in both Cmax and AUC0–96 were achieved for acoziborole across the entire dose range. This conclusion was also supported by AUC0–96, following administration of charcoal at 96 h post-dose for the majority of the dose range. Another important characteristic was the low inter-participant variability (mean values varying from 8% to approximately 28%, independent of the dose). As expected, acoziborole exhibited a very long elimination half-life (267–411 h) across the entire dose range. For Cohorts 1 and 9 that did not receive activated charcoal, the observed half-life (399 and 409 h) was at the upper end of this range, suggesting that charcoal administration was less effective in reducing the half-life of acoziborole in doses over 20 mg. As observed in preclinical species, acoziborole was metabolised by oxidation to a single, inactive metabolite, SCYX-3109 [13], although its plasma levels were very low (< 10–31 ng/mL) across the dose range. Consequently, the very long half-life of acoziborole in human is probably due to very limited metabolism.
Comparison of PK data showed that tablets were bioequivalent to capsules, and that there was no discernible difference between high- and low-dose charcoal, allowing flexibility in choice of tablet or capsule formulations for future studies.
It is widely accepted that only unbound drug can diffuse in tissues and reach the site of action [17]. For HAT, it is important to not only consider free fraction in plasma but also in the brain (or CSF) [14, 17]. In this study, the concentration of unbound acoziborole in plasma samples was very low and difficult to quantify across the dose range, and was estimated to be between 0.4 and 8%, broadly consistent with previous in vitro measurements (2.2%). In the two cohorts studied (240 and 320 mg), mean CSF-to-plasma ratios were found to be comparable (2.2% and 2.6%, respectively), indicating that acoziborole is able to freely cross the BBB and reach the site of action associated with the second stage of the disease, indicating that pharmacologically active exposure should be reached in patients. Furthermore, as the unbound concentration of acoziborole in plasma appeared to be a reliable indicator of CSF exposure, this was a useful parameter for planning subsequent doses of acoziborole. Pharmacokinetic modelling was performed after the 320 mg dose to simulate the dose progression required to reach the pharmacologically active free concentration in CSF (unbound AUC = 5.8 µg.h/mL) [14]. Subsequently, this concentration was observed in over 90% of all participants in the dose groups receiving 960–1200 mg acoziborole. Therefore, 960 mg acoziborole was considered to be the therapeutic dose. Due to the number of capsules to be swallowed (15 for the 1200 mg dose) the study scientific advisory board considered it not ethical to escalate the dose, therefore, 1200 mg was the maximum dose administered.
Escalating doses of acoziborole ranging from 20 to 1200 mg did not generate safety concerns. There were no treatment discontinuations, deaths, or severe AEs and only one SAE of mild intensity that was reported 3 months after dosing (part I). A relatively high number of exclusively mild to moderate AEs were recorded but are probably due to the long follow-up period (6 months), required given the very long half-life of acoziborole. Gastrointestinal disorders were among the most frequently reported AEs; however, as these symptoms occurred in participants receiving both placebo and acoziborole (part I), and extensively so in participants receiving high-dose charcoal (part VI), this can probably be attributed to coadministration of activated charcoal. This may explain the reports of drug-related nausea that always occurred within 36 h of activated charcoal administration and, therefore, more than four days after administration of acoziborole.
The relatively high number of laboratory abnormalities was probably due to the very long follow-up period. Furthermore, they were observed in participants who received placebo and study drugs and were independent from dose or time from administration. Clinically significant changes were observed for plasma levels of CPK, aspartate amino transferase (ASAT), and alanine amino transferase (ALAT), but these generally returned to normal levels without corrective treatment or were considered unrelated to acoziborole. Although there was one report of a SAE related to clinically significant changes in thyroid hormones in one participant (240 mg acoziborole), a meeting of experts concluded that these findings were discreet and transient and had no clinical consequence. However, this was taken as a warning and observation of thyroid hormones was included in subsequent studies in patients.
Mean ECG parameters across time exhibited no differences between placebo and acoziborole, regardless of the dose, and remained within a similar range from screening to EOS. Overall, and within the limitations of this study, it can be concluded that single doses of acoziborole have no impact on cardiac activity. However, given the variations observed in this study, ECG recordings were made in subsequent clinical trials and will continue to be collected in future studies in patients.
5 Conclusions
In this first-in-human study, acoziborole demonstrated an excellent non–dose-related safety profile at up to 1200 mg in healthy male participants of sub-Saharan origin. Administered as a single oral dose in fasted condition, acoziborole achieved high levels of sustained plasma and CSF exposure; according to the results of pre-clinical efficacy studies, this sustained exposure indicates that acoziborole may be fully efficacious in patients with HAT [13]. Acoziborole may represent a single-dose oral treatment for this life-threatening disease.
References
WHO. Control and surveillance of human African trypanosomiasis: report of a WHO expert committee. WHO Tech Rep Ser. 2013;984:i–x (1–237).
Brun R, Blum J, Chappuis F, Burri C. Human African trypanosomiasis. Lancet. 2010;375:148–59.
World Health Organization. WHO outlines criteria to assess elimination of sleeping sickness [Internet]. 2018. https://www.who.int/neglected_diseases/news/criteria-eliminate-sleeping-sickness/en/. Accessed 16 Jul 2020.
Franco JR, Cecchi G, Paone M, Diarra A, Grout L, et al. The elimination of human African trypanosomiasis: Achievements in relation to WHO road map targets for 2020. PLOS Negl Trop Dis. 2022;16(1):e0010047. https://doi.org/10.1371/journal.pntd.0010047.
Franco JR, Cecchi G, Priotto G, et al. Monitoring the elimination of human African trypanosomiasis at continental and country level: Update to 2018. PLoS Negl Trop Dis. 2020;14: e0008261.
Priotto G, Kasparian S, Mutombo W, Ngouama D, Ghorashian S, Arnold U, et al. Nifurtimox-eflornithine combination therapy for second-stage African Trypanosoma brucei gambiense trypanosomiasis: a multicentre, randomised, Phase III, non-inferiority trial. Lancet (London, England). 2009;374:56–64.
Schmid C, Kuemmerle A, Blum J, Ghabri S, Kande V, Mutombo W, et al. In-hospital safety in field conditions of nifurtimox eflornithine combination therapy (NECT) for T. b. gambiense sleeping sickness. PLoS Negl Trop Dis. 2012;6:e1920.
Torreele E, Bourdin Trunz B, Tweats D, Kaiser M, Brun R, Mazué G, et al. Fexinidazole—a new oral nitroimidazole drug candidate entering clinical development for the treatment of sleeping sickness. PLoS Negl Trop Dis. 2010;4: e923.
Kaiser M, Bray MA, Cal M, Bourdin Trunz B, Torreele E, Brun R. Antitrypanosomal activity of fexinidazole, a new oral nitroimidazole drug candidate for treatment of sleeping sickness. Antimicrob Agents Chemother. 2011;55:5602–8.
Tweats D, Bourdin Trunz B, Torreele E. Genotoxicity profile of fexinidazole–a drug candidate in clinical development for human African trypanomiasis (sleeping sickness). Mutagenesis. 2012;27:523–32.
Tarral A, Blesson S, Mordt OV, Torreele E, Sassella D, Bray MA, et al. Determination of an optimal dosing regimen for fexinidazole, a novel oral drug for the treatment of human African trypanosomiasis: first-in-human studies. Clin Pharmacokinet. 2014;53:565–80.
Mesu VKBK, Kalonji WM, Bardonneau C, Mordt OV, Blesson S, Simon F, et al. Oral fexinidazole for late-stage African Trypanosoma brucei gambiense trypanosomiasis: a pivotal multicentre, randomised, non-inferiority trial. Lancet. 2018;391:144–54.
Jacobs RT, Nare B, Wring SA, Orr MD, Chen D, Sligar JM, et al. SCYX-7158, an orally-active benzoxaborole for the treatment of stage 2 human African trypanosomiasis. PLoS Negl Trop Dis. 2011;5: e1151.
Wring S, Gaukel E, Nare B, Jacobs R, Beaudet B, Bowling T, et al. Pharmacokinetics and pharmacodynamics utilizing unbound target tissue exposure as part of a disposition-based rationale for lead optimization of benzoxaboroles in the treatment of Stage 2 Human African Trypanosomiasis. Parasitology. 2014;141:104–18.
Jacobs RT, Plattner JJ, Nare B, Wring SA, Chen D, Freund Y, et al. Benzoxaboroles: a new class of potential drugs for human African trypanosomiasis. Future Med Chem. 2011;3:1259–78.
ICH HARMONISED TRIPARTITE GUIDELINE FOR GOOD CLINICAL PRACTICE E6 (R1). https://www.ema.europa.eu/en/ich-e6-r2-good-clinical-practice#document-history-revision-1-section. Accessed 16 Jul 2020.
Trainor GL. Chapter 31. Plasma protein binding and the free drug principle: recent developments and applications. Annu Rep Med Chem. 2007;42:489–502. https://doi.org/10.1016/S0065-7743(07)42031-0.
Acknowledgements
The clinical studies were performed by the SGS Aster Clinical Unit (Paris, France) and Eurofins Optimed (Gières, France). Pharmacokinetic and statistical analysis, and preparation of the clinical study report was performed by PhinC Development (Evry, France). The manuscript was prepared by Paul Glossop (Sandexis Medicinal Chemistry Ltd, Sandwich, UK) and Eliane Tarral MD (Seven Office, Chambery France). This study was funded by the Norwegian Agency for Development and Cooperation (Norad), Norwegian Ministry of Foreign Affairs, as part of Norway’s in-kind contribution to EDCTP2 (Norway); the Federal Ministry of Education and Research (BMBF) through KfW (Germany); the Dutch Ministry of Foreign Affairs (DGIS, the Netherlands); the Swiss Agency for Development and Cooperation (SDC) (Switzerland); UK aid (UK); the Bill & Melinda Gates Foundation (Grant # INV 002384); and Médecins Sans Frontières (MSF). The findings and conclusions contained herein are those of the authors and do not necessarily reflect positions or policies of the aforementioned funding bodies. The donors had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
See title page.
Conflicts of interest
VG and MF declare employment by PhinC Development, a CRO sub-contracted for this project. PV is CMO and President of Cardiabase, which provided central ECG services during the study. AT, SD, OV, SB, and NSW declare employment by study sponsor Drugs for Neglected Diseases initiative. YD declares employment by Eurofins Optimed. TD declares employment by SGS Aster at the time of the study. No other potential conflicts of interest were declared.
Availability of data and material
The data underlying the results of this study are available upon request because they contain potentially sensitive information. Interested researchers may contact the Drugs for Neglected Diseases initiative (DNDi), commissioner of this study, for data access requests via email at CTdata@dndi.org. Researchers may also request data by completing the form available at https://www.dndi.org/category/clinical-trials/. In this, they confirm that they will share data and results with DNDi and will publish any results open access.
Ethics approval
This study was conducted in accordance with the Declaration of Helsinki, French Huriet law (No. 2004-806), and Good Clinical Practice guidelines. The protocol and amendments were approved by the Committee of Protection of Persons (Paris, France) and by the national competent authority (Agence Nationale de Sécurité du Médicament).
Consent to participate
Written informed consent was obtained from all participants
Consent for publication
Not applicable
Code availability
Not applicable
Author contributions
AT, OV, SD SB, NSW, TD, LH, and VG conceived and designed the experiments; LH, TD, ML, and YD performed the clinical studies; VG, MF and PV analysed the data and performed the statistical and pharmacokinetic analyses.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Tarral, A., Hovsepian, L., Duvauchelle, T. et al. Determination of the Optimal Single Dose Treatment for Acoziborole, a Novel Drug for the Treatment of Human African Trypanosomiasis: First-in-Human Study. Clin Pharmacokinet 62, 481–491 (2023). https://doi.org/10.1007/s40262-023-01216-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-023-01216-8