
Abstract
Background and Objective
Ceftaroline fosamil is a β-lactam antibiotic approved as a 600 mg twice daily dose (≤1 h infusion, ‘standard dosing’) or a 600 mg thrice daily dose (2 h infusion) to treat complicated skin and soft tissue infections caused by Staphylococcus aureus (minimum inhibitory concentration [MIC] 2–4 mg/L). We sought to systematically evaluate the relative impact of the three key components of the intensified dosing regimen (i.e. shortened dosing interval, prolonged infusion duration and increased total daily dose [TDD]) on the pharmacokinetic/pharmacodynamic (PK/PD) target attainment given different grades of bacterial susceptibility.
Methods
A population PK model was developed using data from 12 healthy volunteers (EudraCT-2012-005134-11) receiving standard or intensified dosing. PK/PD target attainment (ƒT>MIC = 35% and 100%) after 24 h was compared following systematically varied combinations of the (1) dosing interval (every 12 h [q12h]→ every 8 h [q8h]); (2) infusion duration (1 h→2 h); and (3) individual and total daily dose (400→900 mg, i.e. TDD 1200→1800 mg), as well as for varying susceptibility of S. aureus (MIC 0.032–8 mg/L).
Results
A two-compartment model with linear elimination adequately described ceftaroline concentrations (n = 274). The relevance of the dosing components dosing interval/infusion duration/TDD for ƒT>MIC systematically changed with pathogen susceptibility. For susceptible pathogens with MIC ≤1 mg/L, shortened dosing intervals appeared as the main driver of the improved target attainment associated with the intensified dosing regimen, followed by increased TDD and infusion duration. For less susceptible pathogens, the advantage of q8h dosing and 2 h infusions declined, and increased TDD improved ƒT>MIC the most.
Conclusion
The analysis calls to mind consideration of dose increases when prolonging the infusion duration in the case of low bacterial susceptibility.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Apart from the standard dosing regimen (600 mg, twice daily, 1 h infusion), an intensified dosing regimen (600 mg thrice daily, 2 h infusion) has been approved for the cephalosporin antibiotic ceftaroline fosamil, which involves the intensification of three dosing components simultaneously (i.e., prolonged infusion duration and shorter dosing interval and enhanced total daily dose [TDD]). |
The present population pharmacokinetic analysis systematically evaluated the impact of each of the three key dosing components on a measure of efficacy (ƒT>MIC: time that antibiotic concentrations are above the minimum inhibitory concentration of the pathogen) and demonstrates that the relevance of dosing interval, infusion duration and TDD for ƒT>MIC systematically changes with pathogen susceptibility. |
While for susceptible strains, shortened dosing intervals appeared to be the main driver of high target attainment (ƒT>MIC observed with the approved intensified dosing regimen), increased TDD (rather than every 8 h dosing and 2 h infusions) improved ƒT>MIC the most for less susceptible pathogens, calling to mind not to neglect dose increases when prolonging the infusion duration in the case of low bacterial susceptibility. |
1 Introduction
Bacterial infections remain a serious threat to public health, not least owing to the growing burden of antimicrobial resistance. Given the rather dry pipeline for new antibiotics, prudent dosing of currently available last-resort antibiotics is of paramount importance to preserve their activity. Ceftaroline fosamil (CPT-F), the N-phosphono prodrug of the active metabolite ceftaroline (CPT), is a fifth-generation broad-spectrum cephalosporin with extended Gram-positive coverage, including activity against methicillin-resistant Staphylococcus aureus and penicillin-resistant Streptococcus pneumoniae [1]. CPT-F therefore constitutes a valuable option for the treatment of complicated skin and soft tissue infections (cSSTI) and community-acquired pneumonia (CAP), and is approved for these indications in Europe (and for similar indications in other regions) at a standard dose of 600 mg CPT-F administered twice daily (every 12 h [q12h], as a 5-min to 1 h intravenous infusion) in adults with normal renal function [2, 3].
Like other β-lactams, ceftaroline exhibits ‘time-dependent’ bacterial killing and its antimicrobial activity has been related to the pharmacokinetic/pharmacodynamic (PK/PD) index ƒT>MIC (cumulative percentage of a 24-h time period that unbound plasma concentrations exceed the minimum inhibitory concentration [MIC] of the target organism). Thus, dosing strategies leading to extended T>MIC have been proposed to improve the efficacy of ceftaroline, including shorter dosing intervals (CPT-F 600 mg every 8 h [q8h] vs. q12h) and consequently higher total daily doses (TDD, 1800 mg [i.e. 3*600 mg] vs. 1200 mg [i.e. 2*600 mg]) [4] plus extended infusion durations (2 h vs. 1 h) [5]. This ‘high TDD/prolonged infusion’ dosing regimen showed good clinical efficacy and favourable safety profiles and has been approved for cSSTI confirmed or suspected to be caused by S. aureus with MIC as high as 2 or 4 mg/L [2, 5].
Although significantly higher ƒT>MIC has been shown after the approved intensified dosing regimen (q8h/2 h infusions/TDD 1800 mg) compared with standard dosing (q12h/1 h infusions/TTD 1200 mg) [6], the dosing component primarily responsible for the improved target attainment remained unclear. Population PK modelling and simulations enable the investigation of scenarios not covered by the underlying original study, and thus clarifying the contribution of different dosing strategies to overall antibiotic exposure.
We aimed to systematically evaluate the single effects and relative impact of the three key components of dosing intensification, i.e. shortened dosing interval, prolonged infusion duration, and increased TDD, on ƒT>MIC, and the PK/PD target attainment of ceftaroline in healthy volunteers by population PK modelling. Patterns of importance of the three dosing strategies for effective treatment with the β-lactam were to be investigated for S. aureus with different MIC values, i.e. bacterial susceptibility.
2 Study Population and Methods
2.1 Study Population and Design
A prospective, open-label study including 12 healthy male volunteers constituted the basis for the population PK model [6]. The study was conducted at the Medical University of Vienna (EudraCT number 2012-005134-11) in accordance with International Conference on Harmonisation Good Clinical Practice (ICH-GCP) guidelines and the Declaration of Helsinki after approval by the Institutional Ethics Committee (1930/2012) and Institutional Review Board. Furthermore, signed informed consent was received from all study subjects [6]. In summary (see Table S1 in the electronic supplementary material [ESM]), participants displayed a median age of 27.5 years (range 22–50 years) and a median total body weight (TBW) of 74.5 kg (range 63–106 kg; body mass index [BMI]: median 23.0 [range 19.4–27.6] kg/m2). The study population did not show renal impairment (CLCR_Cockcroft/Gault: median 145 [range 93.2–165] mL/min).
The healthy volunteers were randomly assigned to two different approved dosing groups of equal size (n = 6) receiving either (1) CPT-F 600 mg q8h as a 2 h intravenous infusion (‘intensified dosing regimen’); or (2) CPT-F 600 mg q12h as a 1 h intravenous infusion (‘standard dosing regimen’). Rich sampling of total plasma CPT concentrations (n = 274) was performed on 2 consecutive days (i.e. on two ‘occasions’): (1) after the first dose (n = 12 and n = 10 samples in the standard and intensified dosing groups, respectively); and (2) after three repeated doses (standard q12h dosing group, n = 13 samples) or four doses (intensified q8h dosing group, n = 10–11 samples) of CPT-F. Total concentrations of the active metabolite CPT were investigated during a 12-h (standard q12h dosing group) or 8 h (intensified q8h dosing group) period, and measured by a validated liquid chromatography (LC)-tandem mass spectrometry method [6].
2.2 Population Pharmacokinetic (PK) Modelling
Nonlinear mixed-effects modelling was performed using NONMEM 7.3.0 [7] (ICON Clinical Research LLC, Gaithersburg, MD, USA) and the first-order conditional estimation method (with interaction), assisted by PsN 4.7.0 [8] (Uppsala University, Sweden; https://uupharmacometrics.github.io/PsN). Statistical and graphical analyses were conducted in R3.0.2 (R Core Team, The R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org).
One-, two-, and three-compartment models were explored, all parameterised in terms of volume of distribution and (elimination and intercompartmental) clearance parameters. The difference between the administered and measured entities (CPT-F and CPT) was considered using their ratio of molar masses (CPT-to-CPT-F ratio: 0.883). CPT-F-to-CPT conversion was (1) assumed to be complete and immediate, or (2) modelled using a depot compartment and a first-order transformation rate constant (ktrans). ktrans was estimated or fixed according to prior studies, assuming a conversion half-life of 19 min [9] or a prodrug clearance of 228 L/h (given creatinine clearance [CLCR] = 102 mL/min/1.73 m2) [10]. First-order and nonlinear (Michaelis–Menten) elimination as well as a combination of both models was explored. Owing to previous evidence, CLCR was investigated as a covariate on clearance using linear and power functions as well as a CL-CLCR relationship previously identified for healthy subjects [10,11,12]. Interindividual and interoccasion variability were modelled using an exponential function, assuming a log-normal distribution of the individual PK parameters per occasion. Residual unexplained variability was considered using additive, proportional, and combined additive and proportional models.
Model evaluation and selection was guided by statistical significance (difference in objective function value [∆OFV] = 3.84, α = 0.05, degrees of freedom [df] = 1 for nested models), precision and plausibility of parameter estimates as well as standard goodness-of-fit plots (e.g. observed vs. population/individual predicted concentrations and concentration-time profiles, conditional weighted residuals vs. population predictions and time). The predictive performance of the model was assessed by visual predictive checks stratified by dosing group (n = 1000 simulations).
2.3 Evaluation of ƒT>MIC and PK/PD Target Attainment After Systematically Varied Dosing Regimens
The PK/PD index ƒT>MIC was predicted for each study participant at 24 h of CPT treatment and for an MIC range of 0.032–8 mg/L (wild-type organisms ≤0.5 mg/L, MIC90 = 1 mg/L) representative of S. aureus in Europe [13, 14]. S. aureus was chosen because the intensified dosing regimen of CPT-F has specifically been approved for cSSTI infections caused by S. aureus, and as S. aureus constitutes the most common cause of cSSTI worldwide, highlighting its clinical relevance [15, 16]. To determine ƒT>MIC, unbound concentrations were calculated assuming 20% plasma protein binding in accordance with the summary of product characteristics [2, 3] and the key PK/PD study motivating the expansion of the label by the intensified regimen [17].
PK/PD target attainment was compared following the standard and intensified dosing regimen clinically investigated in the study as well as following simulated dosing regimens for CPT-F with systematically varied combinations of the dosing components: (1) dosing interval (q12h, q8h); (2) infusion duration (1, 2 and 3 h); and (3) dose (400–900 mg, i.e. TDD 1200 and 1800 mg). ƒT>MIC was assessed after changing only one dosing component at a time, while leaving the other two aspects constant. The different dosing regimens were evaluated (1) relative to ƒT>MIC after standard dosing, and (2) with respect to the PK/PD targets ƒT>MIC = 35%, required for a 2-log10 colony-forming unit (CFU) reduction of S. aureus, and ƒT>MIC = 100%, as commonly used for β-lactams in vulnerable patient populations [17]. The selected PK/PD target of 35% was derived based on a solid data basis, i.e. three preclinical models assessing 24 S. aureus isolates (MIC 0.12–4 mg/L), after 24 h of antibiotic exposure [18,19,20]. The 24 h period of our study corresponded to this in vitro timeframe.
3 Results
3.1 Population PK Model
A two-compartment disposition model with linear elimination (CL = 10.9 L/h, Vtotal = 23.1 L) (see Table 1) assuming complete and immediate CPT-F-to-CPT conversion adequately predicted CPT concentrations in healthy volunteers of both dosing groups (see Figs. 1 and 2 for visual predictive checks and individual model predictions; see ESM Fig. S1 for goodness-of-fit plots; see ESM Table S2 for a summary of key models). A three-compartment model provided a comparable fit to the data, with marginally improved predictions for the lowest concentrations (0.2 mg/L) in the q12h dosing group, although less precise (relative standard error [RSE] <29%) and less plausible parameter estimates. Models describing CPT-F-to-CPT-conversion using a depot compartment did not add any advantage to the model fit and resulted in an increase in OFV. A sensitivity analysis revealed best model performance for ktrans >1000/h, indicating virtually immediate conversion. Nonlinear elimination models did not improve the model fit (insignificant decrease in OFV, RSE >80%). Inclusion of a CLCR-CL covariate-parameter relationship was not statistically significant (ΔOFV <1), irrespective of its functional form. A combined additive and proportional residual variability model was the most appropriate to describe CPT concentrations. Neither correlations between interindividual random effects nor interoccasion variability for the different days of sampling (occasion 1: sampling after the first dose; occasion 2: sampling on day 2) were supported by the data (ΔOFV ≤5.23 for interoccasion variability on CL of 3%).

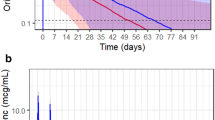
Visual predictive check (n = 1000) for the observed CPT plasma concentrations (open circles, median = dashed blue line) after standard dosing (left) and intensified dosing (right). Shaded areas indicate the 95% confidence intervals for the 50th (solid grey line), 10th and 90th percentile (dashed grey lines) of the simulated data. CPT ceftaroline

Individual observed (open circles) and model-predicted (solid lines) plasma concentration-time profiles of patients receiving intensified dosing (IDs 1–6) and standard dosing (IDs 7–12) of CPT. Blue vertical lines indicate administered doses. CPT ceftaroline
3.2 Comparison of ƒT>MIC between Systematically Varied Dosing Regimens
The intensified dosing regimen led to the highest median ƒT>MIC of all eight studied dosing schemes for MIC = 0.25–4 mg/L (and to higher or comparable ƒT>MIC for MIC = 8 mg/L) [see Fig. 3]. In contrast, the standard dosing regimen resulted in lowest median ƒT>MIC up to MIC = 4 mg/L (ƒT>MIC = 25.5%; attainment of target ƒT>MIC = 35% up to MIC = 2 mg/L). For MIC = 8 mg/L, representing pathogens resistant to ceftaroline, 1200 mg of CPT-F administered in three doses (400 mg/q8h) instead of two doses (600 mg/q12h) resulted in lowest ƒT>MIC overall (median: <10.8%), i.e. in even lower ƒT>MIC than standard dosing.

Target attainment (%ƒT>MIC, given in percentages of the first 24 h of treatment) in the 12 study participants following different systematically varied dosing regimens. The grey dashed lines represent the pharmacokinetic/pharmacodynamic target ƒT>MIC = 35%, indicating a 2-log10 kill of Staphylococcus aureus [17], and the maximum achievable value of 100%. Box-and-whisker plots indicate median and IQR (boxes: 25th–75th percentile) of the data; whiskers extend to a maximum of 1.5 interquartile range of the hinge. Dosing regimens marked with black boxes were clinically investigated in the study [6]. * Standard dosing regimen: 600 mg/q12h/1 h. + Intensified dosing regimen: 600 mg/q8h/2 h. MIC minimum inhibitory concentration (grey shaded area indicates that pathogens with MIC = 8 mg/L are classified as resistant), TDD total daily dose, SD single dose, q12h/q8h dosing every 12 h/8 h, 1 h/2 h infusion duration
3.2.1 Impact of Key Dosing Strategies on ƒT>MIC for Pathogens with Minimum Inhibitory Concentration (MIC) ≤1 mg/L
For MIC values of S. aureus equal or below the susceptibility breakpoint of MIC ≤1 mg/L (‘susceptible pathogens’ according to the European Committee on Antimicrobial Susceptibility Testing [EUCAST] [14]), the eight investigated dosing regimens provoked a similarpattern of changes in ƒT>MIC (see Fig. 3). Table 2 shows trends in ƒT>MIC for MIC = 1 mg/L given standard dosing and alternative regimens involving (1) shortening the dosing interval from 12 h to 8 h (i.e. from twice- to thrice-daily dosing, while keeping the infusion duration and TDD constant); (2) enhancing the TDD from 1200 mg to 1800 mg (while keeping the infusion duration and dosing interval constant); and (3) prolonging the infusion duration from 1 h to 2 h (while keeping the TDD and dosing interval constant). In summary, for susceptible S. aureus strains with MIC ≤1 mg/L, shortening of the dosing interval appeared as the main driver of the improved ƒT>MIC after administration of the approved intensified dosing regimen, followed by an increase in TDD and a prolonged infusion duration.
3.2.2 Impact of Key Dosing Strategies on ƒT >MIC for Pathogens with MIC ≥2 mg/L
For less susceptible and resistant pathogens with MIC ≥2 mg/L [14], the pattern of changes in ƒT>MIC for the investigated dosing regimens deviated from that associated with MIC ≤1 mg/L (Fig. 3 and Table 3). In summary, for MIC values ≥2 mg/mL, increasing the TDD rather than shortening the dosing interval improved ƒT>MIC the most. For example, 900 mg/q12h resulted in comparable (MIC = 2 mg/L) or even superior (MIC ≥4 mg/L) ƒT>MIC than 400 mg/q8h, which stands in contrast to the results obtained for MIC ≤1 mg/L. Hence, the advantage of q8h dosing and 2 h infusions declined with higher MIC values.
For β-lactams, prolonged infusions beyond 2 h have been proposed in an attempt to enhance target attainment and clinical outcome. Dosing regimens with 3 h infusion duration have therefore additionally been investigated (ESM Fig. S2 and ESM Table S3). In summary, similar patterns of fT>MIC across the MIC spectrum could be observed for the different investigated dosing regimens.
3.3 Evaluation of PK/PD Target Attainment with Respect to Reduction of S. aureus
For MIC = 1 mg/L, representing the most abundant S. aureus strains (MIC90) in Europe, all eight investigated dosing regimens, including standard dosing, reached the target ƒT>MIC = 35% (associated with a 2-log10 CFU reduction of S. aureus) in all study participants [17]. For MIC = 2 mg/L, indicating the ceftaroline MIC90 against all S. aureus isolates in the Asia Pacific region, all regimens except standard dosing (75%) attained ƒT>MIC = 35% in >90% of patients [17]. If the infusion duration was prolonged to 3 h, all regimens (TDD 1200/1800 mg q8h/q12h) would reach the target ƒT>MIC=2mg/L = 35% (ESM Fig. S2 and ESM Table S3). For MIC = 4 mg/L, the standard dosing regimen failed to achieve ƒT>MIC = 35% in all subjects. Even for a less conservative treatment target of ƒT>MIC = 27%, indicating bacteriostasis [17], target attainment was <90% after standard dosing. In contrast, the intensified dosing regimen led to attainment of ƒT>MIC = 35% in >90% of study participants up to MIC = 4 mg/L. Given MIC = 8 mg/L, PK/PD target attainment was unsatisfactory for S. aureus for all investigated dosing regimens.
The stricter target of ƒT>MIC >99%, as frequently applied for β-lactams in vulnerable populations such as critically ill patients, was attained in 90% of patients only with the approved intensified dosing regimen for MIC = 0.5 mg/L, and with the four q8h regimens (600 mg/1 h, 2 h; 400 mg/1 h, 2 h) for MIC 0.25 mg/L.
4 Discussion
In the light of increasing antimicrobial resistance, rational dosing of the currently available antibiotics is essential to preserve their activity. For antibiotics with time-dependent bactericidal killing patterns and absent or short persistent effects like many β-lactams, prolonged infusion strategies rather than dose increases have been recommended to better meet ƒT>MIC targets and to ultimately improve outcome, particularly for agents with a short half-life [21, 22].
The current analysis systematically compared the single impact of all three basic principles of dosing, i.e. infusion duration, dosing interval and TDD, on ƒT>MIC and PK/PD target attainment using the example of the β-lactam antibiotic ceftaroline. The analysis was motivated by the separate approval of a ‘high-dose’ regimen for CPT-F, which involves the intensification of all three dosing variables simultaneously, i.e. a combination of prolonged infusion duration, shorter dosing interval and enhanced TDD compared with standard dosing. The study demonstrated that the importance of each dosing component, i.e. its contribution to overall ƒT>MIC after intensified dosing, changes with decreasing susceptibility (i.e. higher MIC).
For susceptible S. aureus strains with MIC ≤1 mg/L, shortened dosing intervals (q12h→q8h) appeared primarily responsible for the high ƒT>MIC following the approved intensified dosing regimen. Prolonged infusion durations (1 h→2 h) increased ƒT>MIC even for resistant strains with MIC = 8 mg/L, but only in the case of sufficiently high doses (≥600 mg). This result is not surprising given that longer infusion durations cause lower maximum (‘peak’) concentrations, which become more relevant for ƒT>MIC at high MIC values.
Importantly, the higher the MIC (>1 mg/L), the more crucial the administered dose amount becomes. For highly susceptible strains, shorter dosing intervals and prolonged infusion durations might even suggest lower than traditional TDDs to reach a specific PK/PD target (although caution has to be exercised in clinical practice before lowering doses, particularly in patients with severe infections). However, for less susceptible strains, shorter dosing intervals and prolonged infusion durations might require higher TDDs to reach the same target. These findings are particularly relevant in the light of the increasing application of prolonged infusions up to continuous infusion of antibiotics, which entails maximum infusion duration and minimum dosing interval. Particularly when switching to a prolonged infusion and/or shorter dosing interval, a simultaneous dose increase should be borne in mind to improve target attainment given known or suspected low bacterial susceptibility. The results also call to mind the importance of considering the susceptibility of the infecting pathogen (and potential variability in MIC) for dosing, which in clinical practice however is commonly not available for healthcare providers.
Our study investigated clinically relevant MIC values up to 8 mg/L. S. aureus with MIC ≤1 mg/L represent the most common strains in Europe (MIC90 = 1 mg/L) and are classified as susceptible to CPT irrespective of its indication (S ≤1 mg/L) [14]. Tallying with this, target attainment rates were high (100%) for MIC = 1 mg/L in the study population. MIC values of 2–4 mg/L are classified resistant according to EUCAST (pneumonia: R >1 mg/L, indications other than pneumonia: R >2 mg/L) [14]. While these are rather rare in Europe, they are more prominent in Latin America and the Asia-Pacific region [23,24,25]. The intensified dosing regimen that has been approved specifically for cSSTI infections caused by S. aureus of MIC 2–4 mg/L was the only dosing strategy leading to sufficient target attainment for MIC = 4 mg/L in the investigated healthy population, highlighting its usefulness. For MIC = 2 mg/L, the PK/PD target was also met by 90% of the population after standard dosing. In cases where severely ill patients display lower antibiotic exposure than healthy volunteers (e.g. as frequently observed in sepsis), the intensified dosing regimen seems more beneficial than standard dosing for MIC = 2 mg/L.
S. aureus with MIC = 8 mg/L is classified as resistant and has rarely been identified in Europe [13, 14]. Nevertheless, MIC = 8 mg/L was included in the analysis as a worst-case scenario and to show target attainment for the full distribution of observed MIC values in Europe [14]. Our analysis suggests that a TDD of 1800 mg would not suffice to achieve a 2-log reduction of such isolates, and even higher doses might be required. However, CPT-F is not approved for the treatment of infections caused by S. aureus with MIC = 8 mg/L, and caution has to be exercised when interpreting target attainment for MIC = 8 mg/L as the target ƒT>MIC = 35% had been determined based on an upper MIC = 4 mg/L [17].
The target ƒT>MIC = 35%, indicating a 2-log10 CFU reduction of S. aureus, was exemplarily chosen in our analysis. We aimed for the most conservative available PK/PD target for ceftaroline against S. aureus, reflecting a 2-log10 CFU reduction, rather than a target reflecting bacteriostasis (ƒT>MIC = 26.8% [17] or ƒT>MIC = 20.3% [13]) even in the healthy study population. In clinical practice, the PK/PD target underlying dosing decisions might differ, e.g. depending on the patient’s clinical condition. For example, stricter PK/PD targets such as ƒT>MIC = 100% have been suggested for β-lactams, especially for intensive care unit (ICU) patients with severe infections [26]. PK/PD targets might also vary for different types of infection and antibiotic agents (even within a β-lactam class). However, the general trends in target attainment across systematically varied dosing regimens and MIC values are likely similar to those illustrated for other antibiotics with PK/PD characteristics and half-life comparable to CPT.
The developed two-compartment population model with linear elimination displayed the same structure as identified in previous population analyses of CPT, including an extensive study covering 21 phase I–III trials [10, 17, 27,28,29]. A different model describing CPT PK solely in healthy volunteers comprised three compartments, potentially supported by q12h dosing and longer periods of rich sampling (12 h) for all subjects [11]. Complete and fast in vivo CPT-F-to-CPT conversion has also been identified by studies with available measurements of both entities [10, 11, 17]. Linear elimination of CPT corresponded to another study in healthy volunteers assessing CPT PK after single-dose CPT-F (600 mg) [11]. Van Wart et al. identified parallel linear and Michaelis–Menten clearance of CPT, although they investigated a broad dose range of 50–2000 mg over a longer observation period (14 days). The study found adequate performance of a linear elimination model for CPT-F doses up to 1000 mg, which is in concordance with our study [10]. The PK parameter estimates were in the range of previous population PK analyses involving healthy volunteers (CL 10.9 L/h vs. 10.7 L/h for CLCR_median = 120 mL/min/1.73 m2 and agemedian = 28 years [17], 11.9 L/h for CLCR_median = 145 mL/min [11]; Vtotal 23.1 L vs. 19.0 L [17], 24.9 L for TBWmedian = 74.5 kg [11]). The interindividual variability associated with clearance was 15.6% and was in line with other studies including healthy volunteers (16.4% [11], 18.4% [30]). Potential sources of variability include renal excretion, factors influencing saturable elimination, or other covariates. In contrast to previous scientific evidence, yet not surprisingly, no significant impact of CLCR on CL was identified in the homogeneous, small population of healthy individuals, who displayed a limited range of unimpaired renal function (CLCR_C/G = 93.2–165 mL/min) [11, 12, 17].
Some limitations should be acknowledged with regard to the present investigation. First, our analysis exclusively considered healthy volunteers without altered pathophysiologic conditions and its results might not necessarily be transferable to infected patients with comorbidities, as suggested by a previous population PK analysis on CPT in patients with CAP, cSSTI and/or renal impairment versus healthy volunteers [17]. Highly variable exposure and faster drug elimination have been shown in infected patients, particularly in severely ill patients and those with augmented renal clearance, implying likely lower target attainment rates than in healthy volunteers [10, 31]. Thus, the dosing regimens required to attain specific PK/PD targets might differ between healthy volunteers and severely ill patients. Next, the small size and homogeneity of the healthy population with rather narrow ranges of clinical characteristics prevented a systematic covariate analysis, i.e. an investigation of the impact of patient factors such as renal function on ceftaroline PK and exposure. However, previous evidence implied only a minimal impact of body size and renal function on CPT target attainment in healthy volunteers [11]. Furthermore, the main purpose of our study was to identify trends in ƒT>MIC and target attainment with respect to different strategies of dosing intensification and bacterial susceptibility rather than causes of PK variability. Our investigation focused on three dosing components combined in the approved intensified dosing regimen [2]. Future exploration of continuous infusion seems relevant given its increasingly widespread use for β-lactams. To optimally and individually balance the interplay between infusion duration, dosing interval and daily dose in future studies, software tools enabling model-informed precision dosing represent a highly promising approach [32]. These tools consider a patient’s demographic and clinical characteristics, dosing history and, if available, measurement of the antibiotic concentration in blood (i.e. therapeutic drug monitoring sample) and allow the selection of an individualised dosing regimen aimed to meet a specific target.
The selection of a dosing regimen in clinical practice also depends on practicability. One vial of Zinforo® 600 mg powder for concentrate for solution for infusion contains 600 mg CPT-F [2]. Hence, two or three vials are required for the approved standard and intensified dosing regimen (and their equivalent with 1 and 2 h infusions), respectively. If 900 mg was used twice daily, four vials would be required to comply with ceftaroline stability (12 h at 2–8°C and 6 h at 25°C [2]); thus, the dosing regimen of 900 mg q12h appears to be the least cost-effective treatment option.
5 Conclusion
Dosing simulations with a successfully developed population PK model for ceftaroline revealed that the relevance of the dosing components dosing interval/infusion duration/TDD changes with decreasing pathogen susceptibility. For susceptible S. aureus strains only, shortening of the dosing interval (from 12 h to 8 h) was the main driver of the high target attainment associated with the approved intensified dosing regimen of CPT-F, followed by increasing the TDD (from 1200 mg to 1800 mg) and extending the infusion duration (from 1 h to 2 h). For higher MIC values ≥2 mg/mL, the advantage of q8h dosing and 2 h infusions declined and an increased TDD rather than shortened dosing interval improved ƒT>MIC the most. Thus, even for antibiotics with time-dependent bactericidal killing patterns, dose increases should not be neglected in the case of low bacterial susceptibility when prolonging the infusion duration. Investigations on the clinical benefit of the studied dosing regimens, including continuous infusion, in target patient populations are warranted.
References
Laudano JB. Ceftaroline fosamil: a new broad-spectrum cephalosporin. J Antimicrob Chemother. 2011;66:iii11–8. https://doi.org/10.1093/jac/dkr095.
AstraZeneca. 2019. Zinforo (powder for concentrate for solution for infusion): summary of product characteristics. https://www.ema.europa.eu/en/documents/product-information/zinforo-epar-product-information_en.pdf. Accessed 8 Oct 2023.
Allergan Inc. 2019. Teflaro® (ceftaroline fosamil) for injection, for intravenous use: prescribing information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/200327s022lbl.pdf. Accessed 8 Oct 2023.
Casapao AM, Davis SL, Barr VO, et al. Large retrospective evaluation of the effectiveness and safety of ceftaroline fosamil therapy. Antimicrob Agents Chemother. 2014;58:2541–6. https://doi.org/10.1128/AAC.02371-13.
Dryden M, Zhang Y, Wilson D, et al. A Phase III, randomized, controlled, non-inferiority trial of ceftaroline fosamil 600 mg every 8 h versus vancomycin plus aztreonam in patients with complicated skin and soft tissue infection with systemic inflammatory response or underlying comorbidities. J Antimicrob Chemother. 2016;71:3575–84. https://doi.org/10.1093/jac/dkw333.
Matzneller P, Lackner E, Lagler H, et al. Single- and repeated-dose pharmacokinetics of ceftaroline in plasma and soft tissues of healthy volunteers for two different dosing regimens of ceftaroline fosamil. Antimicrob Agents Chemother. 2016;60:3617–25. https://doi.org/10.1128/AAC.00097-16.
Beal SL, Sheiner LB, Boeckmann AJ, Bauer RJ (eds). 1989-2018. NONMEM 7.4 user guides.
Keizer RJ, Karlsson MO, Hooker A. Modeling and simulation workbench for NONMEM: Tutorial on Pirana, PsN, and Xpose. CPT Pharmacometrics Syst Pharmacol. 2013;2: e50. https://doi.org/10.1038/psp.2013.24.
U.S. Food and drug administration, Center for drug evaluation and research. 2010. Ceftaroline fosamil for injection: clinical pharmacology and biopharmaceutics review(s). 1–225. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2010/200327Orig1s000ClinPharmR.pdf. Accessed 8 Oct 2023.
Van Wart SA, Forrest A, Khariton T, et al. Population pharmacokinetics of ceftaroline in patients with acute bacterial skin and skin structure infections or community-acquired bacterial pneumonia. J Clin Pharmacol. 2013;53:1155–67. https://doi.org/10.1128/AAC.01680-13.
Justo JA, Mayer SM, Pai MP, et al. Pharmacokinetics of ceftaroline in normal body weight and obese (classes I, II, and III) healthy adult subjects. Antimicrob Agents Chemother. 2015;59:3956–65. https://doi.org/10.1128/AAC.00498-15.
Kiang TKL, Wilby KJ, Ensom MHH. A critical review on the clinical pharmacokinetics, pharmacodynamics, and clinical trials of ceftaroline. Clin Pharmacokinet. 2015;54:915–31. https://doi.org/10.1007/s40262-015-0281-3.
European Committee on Antimicrobial Susceptibility Testing. 2014. Ceftaroline: Rationale for the clinical breakpoints, version 1.0. http://www.eucast.org. Accessed 8 Oct 2023.
The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 13.0, 2023. http://www.eucast.org. Accessed 8 Oct 2023.
Moet GJ, Jones RN, Biedenbach DJ, et al. Contemporary causes of skin and soft tissue infections in North America, Latin America, and Europe: Report from the SENTRY Antimicrobial Surveillance Program (1998–2004). Diagn Microbiol Infect Dis. 2007;57:7–13. https://doi.org/10.1016/j.diagmicrobio.2006.05.009.
Dryden MS. Complicated skin and soft tissue infection. J Antimicrob Chemother. 2010;65:35–44. https://doi.org/10.1093/jac/dkq302.
Das S, Li J, Iaconis J, et al. Ceftaroline fosamil doses and breakpoints for Staphylococcus aureus in complicated skin and soft tissue infections. J Antimicrob Chemother. 2019;74:425–31. https://doi.org/10.1093/jac/dky439.
Singh R, Almutairi M, Alm RA, et al. Ceftaroline efficacy against high-MIC clinical Staphylococcus aureus isolates in an in vitro hollow-fibre infection model. J Antimicrob Chemother. 2017;72:2796–803. https://doi.org/10.1093/jac/dkx214.
MacGowan AP, Noel AR, Tomaselli S, Bowker KE. Pharmacodynamics of Ceftaroline against Staphylococcus aureus Studied in an In Vitro Pharmacokinetic Model of Infection. Antimicrob Agents Chemother. 2013;57:2451–6. https://doi.org/10.1128/AAC.01386-12.
Andes D, Craig WA. Pharmacodynamics of a New Cephalosporin, PPI-0903 (TAK-599), Active against Methicillin-Resistant Staphylococcus aureus in Murine Thigh and Lung Infection Models: Identification of an In Vivo Pharmacokinetic-Pharmacodynamic Target. Antimicrob Agents Chemother. 2006;50:1376–83. https://doi.org/10.1128/AAC.50.4.1376-1383.2006.
Grupper M, Kuti JL, Nicolau DP. Continuous and prolonged intravenous β-lactam dosing: Implications for the clinical laboratory. Clin Microbiol Rev. 2016;29:750–72. https://doi.org/10.1128/CMR.00022-16.
Ehmann L, Zoller M, Minichmayr IK, et al. Development of a dosing algorithm for meropenem in critically ill patients based on a population pharmacokinetic/pharmacodynamic analysis. Int J Antimicrob Agents. 2019;54:309–17. https://doi.org/10.1016/j.ijantimicag.2019.06.016.
Flamm RK, Sader HS, Jones RN. Ceftaroline activity tested against contemporary Latin American bacterial pathogens (2011). Braz J Infect Dis. 2014;18:187–95. https://doi.org/10.1016/j.bjid.2013.11.005.
Biedenbach DJ, Alm RA, Lahiri SD, et al. In vitro activity of ceftaroline against Staphylococcus aureus isolated in 2012 from Asia-Pacific countries as part of the AWARE surveillance program. Antimicrob Agents Chemother. 2016;60:343–7. https://doi.org/10.1093/JAC/DKW315.
Urbán E, Stone GG. Impact of EUCAST ceftaroline breakpoint change on the susceptibility of methicillin-resistant Staphylococcus aureus isolates collected from patients with complicated skin and soft-tissue infections. Clin Microbiol Infect. 2019;25:1429.e1-1429.e4. https://doi.org/10.1016/j.cmi.2019.03.023.
Abdul-Aziz MH, Alffenaar JWC, Bassetti M, et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: a position paper. Int Care Med. 2020;46:1127–53. https://doi.org/10.1007/s00134-020-06050-1.
Barsky EE, Pereira LM, Sullivan KJ, et al. Ceftaroline pharmacokinetics and pharmacodynamics in patients with cystic fibrosis. J Cyst Fibros. 2018;17:e25–31. https://doi.org/10.1016/j.jcf.2017.10.010.
Riccobene TA, Khariton T, Knebel W, et al. Population PK modeling and target attainment simulations to support dosing of ceftaroline fosamil in pediatric patients with acute bacterial skin and skin structure infections and community-acquired bacterial pneumonia. J Clin Pharmacol. 2017;57:345–55. https://doi.org/10.1002/jcph.809.
Li J, Das S, Zhou D, et al. Population pharmacokinetic modeling and probability of target attainment analyses in Asian patients with community-acquired pneumonia treated with ceftaroline fosamil. Clin Pharmacol Drug Dev. 2019;8:682–94. https://doi.org/10.1002/cpdd.673.
Helfer VE, Zavascki AP, Zeitlinger M, et al. Population Pharmacokinetic Modeling and Probability of Target Attainment of Ceftaroline in Brain and Soft Tissues. Antimicrob Agents Chemother. 2022;20(66): e0074122. https://doi.org/10.1128/aac.00741-22.
Roberts JA, Abdul-Aziz MH, Lipman J, et al. Individualised antibiotic dosing for patients who are critically ill: challenges and potential solutions. Lancet Infect Dis. 2014;14:498–509. https://doi.org/10.1016/S1473-3099(14)70036-2.
Wicha SG, Märtson AG, Nielsen EI, et al. From therapeutic drug monitoring to model-informed precision dosing for antibiotics. Clin Pharmacol Ther. 2021;109:928–41. https://doi.org/10.1002/cpt.2202.
Broeker A, Wicha SG. Assessing parameter uncertainty in small-n pharmacometric analyses: value of the log-likelihood profiling-based sampling importance resampling (LLP-SIR) technique. J Pharmacokinet Pharmacodyn. 2020;47:219–28. https://doi.org/10.1007/s10928-020-09682-4.
Acknowledgements
Parts of the present work have previously been presented at the 27th European Congress of Clinical Microbiology and Infectious Diseases (13–16 April 2019, Amsterdam, NL; abstract no. O0829). The underlying study has been registered in the EU Clinical Trials Register (EudraCT number 2012-005134-11).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Open access funding provided by Medical University of Vienna.
Conflicts of interest/Competing interest
Charlotte Kloft reports grants from an industry consortium (AbbVie Deutschland GmbH & Co. KG, Astra-Zeneca, Boehringer Ingelheim Pharma GmbH & Co. KG, Grünenthal GmbH, F. Hoffmann-La Roche Ltd, Merck KGaA and SANOFI), the Innovative Medicines Initiative-Joint Undertaking (‘DDMoRe’), Diurnal Ltd, the Federal Ministry of Education and Research within the Joint Programming Initiative on Antimicrobial Resistance Initiative (JPIAMR), and the European Commission within the Horizon 2020 framework programme (‘FAIR’). Markus Zeitlinger’s institution received various grants from Pfizer for different research purposes but none were associated with the present work. Iris K. Minichmayr, Sebastian G. Wicha, and Peter Matzneller have no conflicts of interest to declare.
Availability of data and material
Data are presented in the manuscript. The datasets generated and/or analysed during the current study are available from the study centre on reasonable request.
Ethics approval
This study was conducted at the Medical University of Vienna in accordance with ICH-GCP guidelines and the Declaration of Helsinki after approval by the Institutional Ethics Committee (1930/2012) and Institutional Review Board (see also the Methods section).
Consent to participate
This study was conducted after signed informed consent was received from all study subjects (see also the Methods section).
Consent for publication
Not applicable.
Code availability
The control stream used for the current analysis is available from the corresponding author on reasonable request.
Author contributions
IKM: conceptualisation of the analysis, data analyses, interpretation of the results, drafting of the manuscript. SGW: methodology, interpretation of the results, critical revision of the manuscript. PM: data acquisition, critical revision of the manuscript. CK: interpretation of the results, supervision, critical revision of the manuscript. MZ: data acquisition, supervision, critical revision of the manuscript. All authors approved the final version of the manuscript.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Minichmayr, I.K., Wicha, S.G., Matzneller, P. et al. Impact of Key Components of Intensified Ceftaroline Dosing on Pharmacokinetic/Pharmacodynamic Target Attainment. Clin Pharmacokinet 63, 121–131 (2024). https://doi.org/10.1007/s40262-023-01325-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-023-01325-4