
Abstract
Introduction
The health dangers of medicines of unknown identity (MUIs) [loose pharmaceutical units repackaged in individual bags without labelling of their identity] have been suspected in L/MICs. Using visual and analytical tools to identify MUIs, we investigated the frequency of, and factors associated with, adverse drug reaction (ADR)-related hospitalizations in a central hospital in Vientiane Capital, Lao People’s Democratic Republic (PDR).
Methods
All unplanned admissions, except for acute trauma and intentional overdose, were prospectively recorded during a 7-week period in 2013, leading to include 453 adults hospitalized for ≥24 h. The patients or their relatives were interviewed to complete the study questionnaire. MUIs suspected of being involved in ADR(s) were identified through comparison of visual characteristics of tablets/capsules with that of reference medicines (photograph tool), and by proton nuclear magnetic resonance and mass spectrometry analyses. Factors associated with ADRs were identified by multivariate logistic regression.
Results
The frequency of hospitalizations related to an ADR was 5.1% (23/453, 95% confidence interval [CI] 3.1–7.1). Forty-eight (12.8%) patients used MUI(s) in the last 2 weeks preceding hospitalization. They were more likely to be hospitalized because of an ADR (adjusted odds ratio 4.5, 95% CI 1.7–11.5) than patients using medicines of known identity. MUIs were mainly involved in bleeding gastroduodenal ulcers. The photograph tool led to the misidentifications because of look-alike pharmaceutical units in the medicines photograph collection.
Conclusion
According to the results of this study, there is a need to ensure appropriate labelling of medicines at dispensing and to provide well-suited tools to identify MUIs in clinical settings to improve drug safety and patients’ care in developing countries with limited capacities for drug analysis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Our study, conducted at a central hospital of a lower middle income country (Laos) showed that 5.1% of hospitalizations are related to an adverse reaction. |
The study also highlighted that the use of loose pharmaceutical units repackaged in individual bags without labelling of their identity was associated with drug-related morbidity and is detrimental for patient care. |
These findings suggest that evidence-based measures to reduce the mislabelling of medicines by medicine providers and systems (e.g. an international imprint coding of medicines) to identify active pharmaceutical ingredients in medicines are required. |
1 Introduction
Identification of strategies for detecting and preventing adverse reactions due to drugs and medication errors is one of the WHO global priority areas for patient safety research [1]. An adverse drug reaction (ADR) represents “a response to a medicinal product which is noxious and unintended, that arises from the use of the product within or outside the terms of the marketing authorization” (including off-label use, overdose, misuse, abuse and medication errors) or from occupational exposure, as defined by the European Medicines Agency [2, 3]. In low- and middle-income countries (L/MICs), there is relatively little drug safety research, and this is impaired by factors such as the lack of databases on exposure to medicinal products and on medical data during hospitalization.
Unclear labelling of medicines, or even no labelling (i.e. when patients purchase loose tablets or capsules repackaged in individual bags without any labelling as to identity or dose), have been identified in many L/MICs in South-East Asia, Africa, Latin America and the Caribbean [4,5,6,7,8,9,10,11,12,13,14,15,16,17]. In some developed countries, such as the US, medicines are commonly dispensed after repackaging of dosage units from initial bulk packaging. Although variability in the content of instruction and warning on the containers after repackaging has been observed, labels are present [18]. However, prescription medicines packaged loosely without affixed labels have been obtained from international online pharmacies [19, 20]. In South-East Asia, plastic bags containing mixed unidentified tablets are sold by shops without staff with medical or pharmaceutical training. In the late 1990s, Stenson et al. observed that almost half of the medicines sold in community pharmacies of the Lao People’s Democratic Republic (Lao PDR, Laos) bore no label and that in 26% of cases, medicines were mixed in the same package, known as ‘yaa chud’, literally ‘combination medicine’ [21] (Fig. 1).

‘Yaa chud’ sold in Laos, 2013
This practice is also observed in adjacent Thailand and Cambodia [11, 22, 23]. Dispensing unlabelled solid oral dosage forms of medicines is still common practice, as shown in a ‘mystery shopper’ survey conducted in five provinces of Laos in 2012, in which 10.1% of the 158 medicines bought for malaria treatment were sold as loose tablets with no label or written information [24].
These dispensing malpractices are an important public health issue that has been neglected, with few data to inform policy. Potential consequences of such poor dispensing practices are inadequate adherence of patients, if the dosage, time and mode of administration are not written on the plastic bags, and accelerated degradation of the active pharmaceutical ingredients (API) if the medicines are kept for long periods in unsealed plastic bags. An important potential consequence is the risk of ADRs. Analysis of the content of yaa chud tablets/capsules sold in the early 2000s on the Thailand–Myanmar border, to a buyer asking for medicines to treat fever in his pregnant wife. showed that, in addition to not being efficacious to treat malaria, they may be harmful during pregnancy [22].
For serious ADRs leading to hospitalization, lack of knowledge of medicines used by patients impairs patients’ care for both the treatment of the ADR and subsequent prescriptions. In order to characterize the role of medicines of unknown identity (MUIs) in ADR-related hospitalizations, we investigated the frequency of, and factors associated with, hospitalizations due to ADRs in Mahosot Hospital, Vientiane Capital. We achieved this aim by determining the provisional identity of active pharmaceutical ingredients in unknown tablets/capsules suspected to be involved in ADR-related hospitalizations, first from their visual characteristics, in comparison with that of medicines sold in Laos, and then by formal physicochemical analysis.
2 Methods
2.1 Study Settings and Population
This cross-sectional study with prospective inclusion of patients was conducted at Mahosot Hospital, Vientiane, Lao PDR, a 450-bed adult and child primary tertiary care teaching hospital. A sample size of 456 patients was initially estimated as necessary to detect a frequency of medication-related hospital admissions of 5%, with a 95% confidence interval (CI) of 3.0–7.0%, based on international systematic reviews [25, 26]. The study was conducted over a 7-week period in February–June 2013.
All consecutive adults (≥16 years of age) who presented to the adult medical emergency department during weekdays, and who were admitted for 1 day or more (unplanned admissions) to a hospital ward (medical, surgical and intensive care wards), were eligible for enrollment if they gave oral, informed consent. Patients hospitalized for trauma and intentional overdoses of medicines were not included.
2.2 Data Collection
Each patient, or their relatives, was interviewed within 48 h of admission by a Lao medical doctor, trained to complete the study questionnaire developed for the purpose of this study, with a pharmacovigilance pharmacist. The questionnaire was developed in French and the questions were asked in the Lao language by the Lao medical doctor, who is fluent in French. The 40-questions questionnaire included sociodemographic, medical history and medication exposure data (see electronic supplementary material 1). It was tested with 39 patients enrolled in a feasibility study, to assess understanding and ease of completion. The respondents to the feasibility study were asked to tell if all the words were understood. A few minor corrections were made to the original questionnaire.
A detailed prehospital medication exposure history for the 2 weeks preceding admission was taken through open-ended questions to record the name, dosage, place of procurement, if the medicine was obtained through self-medication, and the start and end dates of taking the medication. The respondents were asked to show any medicines, prescriptions, health record booklets and/or referral letters. To minimize information bias, a questionnaire adapted from Roulet et al. [27] was used to record self-medication history. Yaa chud use was also recorded. Medication was considered as chronic use if taken for ≥3 months. Medicines were classified on the basis of the Anatomical Therapeutic Chemical classification index [28].
Patients were followed during the hospitalization and charts were reviewed again following discharge. Patients were subsequently contacted through telephone to ensure data completeness.
2.3 Outcome Measures
A list of trigger events, adapted from Rozich et al. [29] and Mehta et al. [30], was used during the initial screening of ADRs (see electronic supplementary material 2). The investigators did not know when an ADR was involved in the hospitalization. Whether the patients were admitted because of an ADR was first assessed by the Lao medical doctor and the pharmacovigilance specialist during the collection of the data on medication use, medical history, and history of the current condition.
Some unknown medicines used prior to hospitalization were suspected to be involved in ADR-related hospitalizations, based on chronology, reason of use and hospital diagnosis. After identification of API(s) for these unknown medicines, each initially suspected ADR was reviewed and causality assessment was performed, using the WHO criteria, by three pharmacovigilance specialists until consensus was reached [31]. Unassessable cases were excluded from the study. Only ADRs assessed as possible, probable and certain were included in the analysis.
The classification of symptoms and signs of ADRs was based on WHO Adverse Reaction Terminology (WHO ART) [31].
2.4 Identification of Unknown Medicines
We defined an MUI as one for which the name of the brand or active pharmaceutical ingredient(s) was not written on the primary package, and that could not be identified by any other means at the time of the interview (prescription, record booklet, patients statements …).
MUIs suspected of being involved in an ADR-related hospitalization were provisionally identified using a visual identification tool (a photograph tool). This tool relied on the visual comparison of the features of the tablet/capsule with those of 494 known unambiguously labelled medicines collected from private community pharmacies in Vientiane Capital. One sample of all solid oral dosage forms (tablets and capsules) of medicines belonging to the following classes, chosen as most commonly involved in ADRs [25, 26, 32], was bought to create the collection: antidiabetic, anti-infective, cardiovascular, antithrombotic, analgesic, anti-inflammatory medicines and medicines for central nervous system disorders. Identifications were performed using photographs of the reference pharmaceutical units by three health workers—two pharmacists (NS and NM) and one medical doctor (CS)—without conferring. Whenever possible, samples of the MUIs were collected by the research team and proton magnetic nuclear resonance (1H NMR)-mass spectrometry (MS), when needed, was conducted.
2.5 Statistical Analysis
Data were entered into an MS Access Database 2010 (Microsoft Corporation, Redmond, WA, USA) created specifically for the study. Qualitative variables were expressed in numbers and percentages [n (%)] and compared between patients with or without ADR-related hospitalization using Chi-square tests or Fisher’s exact tests, as appropriate. Quantitative variables were expressed as mean ± 95% CI, or median and first and third quartiles (Q1–Q3), and were compared between the two groups using t tests or Wilcoxon–Mann–Whitney tests, as appropriate.
A backward logistic regression model was performed to assess factors associated with ADR-related hospitalizations. All variables associated with ADRs with a p value <0.20 on univariate analysis were entered into a multivariate logistic regression model, in addition to age and sex, factors commonly associated with ADR-related hospitalizations [26]. The goodness-of-fit of the final model was assessed using the Hosmer and Lemeshow test. The results are presented as odds ratio (OR) and adjusted ORs (aOR) and their 95% CIs. Only ADRs assessed as possible, probable and certain were included in the analysis.
Data analysis was carried out using SAS 9.3 software (SAS Institute, Cary, NC, USA). The level of significance was set at 0.05 (two-sided).
3 Results
3.1 Prevalence of Adverse Drug Reaction (ADR)-Related Hospitalizations in the Study Population
During the study period, 2426 adult patients of the 3529 patients visiting the emergency ward presented to the acute medical care department; 483 who were admitted for >24 h provided consent and were included. Thirty cases were excluded from the study, 13 of which were unassessable cases of suspected ADRs, with a lack of information on the medication exposure (n = 10) or the medical history (n = 3). The remaining 17 cases were not suspected as ADRs but were excluded because of a lack of information on the medication exposure (n = 14) or medical history (n = 3). Sufficient information regarding medication and/or medical history was obtained for 453 patients (94%) (Fig. 2).

Participant flowchart. *Patients who left the emergency department hospitalization ward (did not want to be hospitalized or decided to go to another health facility). **Information regarding medication and/or medical history was insufficient or contradictory and could not be supplemented or verified
The 453 patients were mainly hospitalized in the departments of infectious diseases (29.8%), gastroenterology (29.4%) and cardiology (13.5%). The remaining patients were hospitalized in the pneumology (11.3%), intensive care unit (6.8%), psychiatry (4.4%), international clinic (2.0%), surgery (1.5%) and gynaecology/obstetrics (1.3%) departments. The most frequent diagnoses at discharge were dengue fever (n = 55, 12.1%), acute respiratory diseases (n = 34, 7.5%), cancers (n = 32, 7.1%), hypertension (n = 28, 6.2%) and gastric disorders (n = 26, 5.7%). Of the 453 hospitalizations, 23 were initially suspected as ADR-related, giving a frequency of 5.1% (95% CI 3.1–7.1) during the study period.
3.2 Identification of Medicines of Unknown Identity (MUIs) as Factors Associated with ADR-Related Hospitalizations
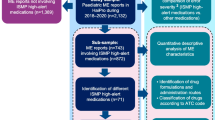
Factors associated with ADR-related hospitalizations were investigated in the 376 (83.0%) patients who used at least one medicine during the 2 weeks preceding hospitalization; 17 admissions were judged as being related to an ADR with known medicines, and six additional ADR-related hospitalizations from MUIs were identified using the visual tool and/or 1H NMR (Fig. 3; Table 1).

Description of the included patients according to ADR-related hospitalizations with MUIs or medicines of known identity. ADR adverse drug reaction, MUIs medicines of unknown identity
The 376 patients used 1488 medicines (median 3.0 medicines per patient, interquartile range [IQR] 2.0–6.0).
Overall, 126 MUIs were used by 48 (12.8%) patients in the 2 weeks preceding hospitalization, 30 (23.8%) of which were suspected, during the initial screening, to be implicated in ADRs in six patients, based on the chronology and symptomatology. Identification of these 30 MUIs was performed by a photograph identification tool specifically developed for this study and checked by 1H NMR/MS for 27 MUIs that were obtained from the patients. The three MUIs identified by the photograph tool only, without chemical analysis, contained ibuprofen (one MUI used by a patient presenting with duodenal ulcer haemorrhage) or paracetamol (two MUIs used by patients with an ADR related to the use of medicines of known identity).
Active pharmaceutical ingredients identified by 1H NMR and/or the photograph tool were mainly vitamins (n = 6, 20.7%), antibiotics (n = 4, 13.8%; β-lactam n = 2, macrolide n = 1, tetracycline n = 1), nonsteroidal anti-inflammatory drugs [NSAIDs] (n = 4, 13.8 %), paracetamol monotherapies (n = 2, 6.9%) and paracetamol combination medicines (n = 1, 3.4%), proton pump inhibitors (n = 2, 7.7%) and cardiovascular diseases medicines (n = 2, 7.7%; digoxin n = 1 and heptaminol n = 1) [see electronic supplementary material 3 and 4].
The photograph tool led to the misidentification of 3 of 14 medicines (21.4%), with at least one dual match in the collection because of look-alike pharmaceutical units in the medicine photograph collection. Colchicine was falsely identified instead of acetylsalicylic acid (judged as implicated in one hospital admission); tetracycline instead of cloxacillin, and codeine-sulfogaiacol-Grindelia combination instead of a dextromethorphan-chlorpheniramine combination.
Excipients only were detected by 1H NMR in one unit that could not be identified by the photograph tool, and excipients plus an unknown macromolecular ingredient were detected in another.
Eleven identified (37.9%) MUIs were found in six ADR-related hospitalizations. For each of these cases, at least one MUI was judged to be involved in the hospitalization.
Patients hospitalized as a result of an ADR had used more medicines (median 7.0 [IQR 3.0–9.0] medicines per patient vs. 3.0 [IQR 2.0–5.0] medicines per patient; p < 0.001) and at least one MUI (n = 8 [34.8%] vs. n = 40 [11.3%]; p < 0.01) than patients hospitalized for other reasons (Table 1). Two patients hospitalized because of an ADR and five patients hospitalized for other reasons had taken yaa chud (8.7 vs. 1.4%, p = 0.06).
Table 2 presents the results of the univariate and multivariate logistic regressions. The number of medicines used in the 2 weeks preceding the hospitalization was not included in the multivariate model because of the strong collinearity of this variable with the use of MUI. Indeed, patients who used MUI(s) used significantly more medicines than those who took medicines of known identity (median 6.0 [IQR 3.0–8.0] medicines per patient versus 3.0 [IQR 1.0–5.0] medicines per patient; p < 0.001). The results of the multivariate model suggest that the use of an MUI was independently associated with ADR-related hospitalizations [aOR 4.5, 95% CI 1.7–11.5).
Patients exposed to MUI(s) were older than those who used medicines of known identity only (mean 55.5 [95% CI 48.8–61.3] years of age vs. 48.8 [95% CI 46.5–51.0] years of age; p = 0.03) (Table 3) and MUIs were more frequently purchased in private clinics and less frequently in public hospitals than medicines of known identity (48.4% vs. 9.0% [p < 0.001] and 34.1% vs. 73.9% [p < 0.001], respectively) (Table 4).
3.3 Characteristics of Cases of ADR-Related Hospitalizations
Electronic supplementary material 5 summarizes the 23 patients with ADR-related hospitalizations. Ten (43.5%) cases of ADRs were classified as probable, and 13 (56.5%) were classified as possible.
Four cases (numbers 1, 2, 3, 4) of drug-induced ulcer were caused by MUIs. Among them, ibuprofen 600 mg was dispensed to patient number 1 in a private clinic after the first symptom of gastrointestinal haemorrhage appeared (melena); one yaa chud containing two different NSAIDs (diclofenac and piroxicam) was taken by a 65-year-old patient (number 2) and one yaa chud containing acetylsalicylic acid (81 mg) and prednisone (5 mg) was taken three times per day by a 68-year-old patient (number 3). Six drug-induced ulcers involved medicine(s) of known identity (NSAIDs, including acetylsalicylic acid). In two of these cases, the culprit medicines were administered after (patient number 7) or continued (patient number 9) after the first symptoms (melena). In one case (patient number 10), the NSAID was obtained through self-medication and taken in the same time as another prescribed NSAID (ibuprofen). Patient number 11 was dispensed two NSAIDs, including a high dose of piroxicam (60 mg/day) for arthralgia in a hospital.
Hypoglycemia induced by oral antidiabetics was responsible for hospitalization in three patients (numbers 13, 14, 15), of which one MUI, identified as glibenclamide, taken in high doses (20 mg/day), induced a hypoglycemic coma. One case of hypokalemia involved three different hypokalemiant medicines, of which one potassium chelative agent was prescribed, whereas the kaliemia of the patient was within normal range (patient number 16). One patient (number 19) developed a severe rash within 1 h following the intake of four MUIs, subsequently identified as clarithromycin, cephalexin and a combination of thiamine-pyridoxine.
One tablet could not be identified by either the photograph tool or NMR/MS. A 17-year-old patient (number 22) developed an acute hepatitis following the intake of four different brand medicines containing paracetamol in a short period of time, of which three were procured by a friend to treat fever and one was dispensed in a hospital after the jaundice occurred.
3.4 Visual Characteristics of Tablets and Capsules in Private Pharmacies
Of the 494 medicines bought in community pharmacies for the implementation of the photograph tool, 215 tablets/capsules (43.5%) did not bear any imprint. Among these unimprinted medicines, 127 (59.1%) had at least one look-alike unit in the collection. Moreover, 7.8% of the 281 imprinted medicines also had look-alike units in the collection (Table 5; Fig. 4). In all cases the imprints represented the name of the manufacturer.

Imprinted look-alike pharmaceutical units containing a phenobarbital and b prednisolone, and c acyclovir and d spiramycin
4 Discussion
We investigated the frequency of, and factors associated with, adult hospitalizations due to ADRs in Mahosot Hospital, Vientiane Capital. We also aimed to characterize the role of MUIs in ADR-related hospitalizations, an aim that was achieved by determining the provisional identity of active pharmaceutical ingredients in unknown tablets/capsules suspected of being involved in ADR-related hospitalizations, first from their visual characteristics (in comparison with that of medicines sold in Laos), and then by formal physicochemical analysis. With a frequency of 5.1% during the survey period, this study demonstrates that ADRs substantially contribute to adult hospitalizations in Mahosot Hospital. Visual identification of MUI(s) at the time of hospitalization, coupled with a physicochemical analysis of active ingredients, allowed us to determine that one-fourth of ADR-related hospitalizations involved the use of MUI(s). Using MUI(s) was identified as a risk factor of ADR-related hospitalization.
As far as we are aware, only two studies have investigated the frequency of ADR-related hospitalizations in adults in L/MICs using similar definitions as in our study; however, these were in upper- to middle-income economies (e.g. Malaysia and South Africa) and reported higher frequencies (8.4 and 9.9%) than in the present work [30, 34].
This study has several limitations. Several reasons could have led to an underestimation of the frequency of ADR-related hospitalization in the present study. First, documenting pharmaceutical and medical histories was mainly based on patient data. Sociocultural issues relating to difficult subjects in Laos (for example HIV and tuberculosis) might have impaired the collection of information. It was difficult to trace pharmaceutical and medical histories as Lao patients often seek care from multiple providers for a single illness [35, 36]. However, patient recall bias was minimized by using an adapted questionnaire to collect medication history [27] and by retrieving information from record booklets whenever possible, although information appeared to be very limited. In addition, the number of ADR-related hospitalizations may have been underestimated as hospitalizations due to trauma were not evaluated, potentially excluding medicine-related falls and resulting fractures commonly observed in older people treated by psychotropic, cardiovascular and hypoglycemic medicines [37]. Our study was conducted in a single tertiary hospital of Laos, and, as such, careful considerations should be taken to generalize our findings to different health structures and to other parts of the country.
As observed in other studies in L/MICs, NSAIDs were the medicines most frequently involved in ADRs [38, 39]. However, cardiovascular medicines, anticancer chemotherapy and antithrombotics were less frequently involved than in other studies, mostly conducted in high-income and upper- to middle-income countries [25, 26, 40]. In Laos, the therapeutic coverage of cardiovascular diseases is not known, but the low rate of ADR to cardiovascular medicines observed here could be related to low use, as observed in other L/MICs [41]. This is likely to be the case for anticancer medicines as cancer treatment within Laos is extremely limited [42]. More than 10% of patients hospitalized in the study period who had taken MUI(s) in the prior 2 weeks preceding the hospitalization developed serious ADRs. Patients who used MUIs also used more medicines than patients using known medicines only, and thus had a higher risk of developing ADRs [26]. In addition, dispensing errors of medicines could have been involved in ADRs, but the design of this study did not allow the investigation of this. Besides increasing the risk of developing ADR-related hospitalizations, using MUI(s) impairs patients’ care, especially in health structures with limited capacities for toxicological or chemical analysis. For example, in our study, a patient developed extensive allergic reaction after taking four different MUIs. Given the risk of severe allergy in case of rechallenge of the culprit medicine or related substances, knowing their identity is essential for subsequent rational prescribing. For another patient, not knowing which antidiabetic medication (and its strength) was involved in the hypoglycemic coma impaired the tailoring of discharge diabetes treatment. More than one-tenth of the MUIs identified by 1H NMR and/or the photograph tool were antibiotics. Not knowing the antibiotic taken prior to admission impairs the choice of appropriate antibiotics by hospital professionals. In addition, inappropriate and subtherapeutic antibiotic use is of particular concern for antimicrobial resistance. This issue has already been raised in a recent study in Laos [24], in which low doses of antibiotics were found in seven of nine yaa chud samples. Measures to ensure medicine labelling at the time of dispensing are required.
A high illiteracy rate and the fact that many medicines are bought by pharmacies in bulk and are not relabelled, were mentioned as reasons for inadequate labelling practices by medicines sellers in private pharmacies in Laos in 2000 [43]. Further investigations are needed to understand the reasons for this risky practice in other health facilities, given that half of the MUIs in our study were provided by health professionals in private clinics, and one-third in public structures.
The Lao regulation stipulates that unlabelled medicines or medicines with unclear labelling should be prohibited. Labels should clearly indicate the name, the dosage, and how to use the medicine. In addition, the mixing of different medicines in the same packaging is prohibited. As the violation of this regulation may be difficult to spot during exposed routine inspections, we suggest that cover inspections by drug inspectors are enhanced.
Identification of solid dosage forms based on their visual characteristics was suggested in the US in the 1960s, encouraged by the American Medical Association [44], and online tools are available in various countries such as Canada, the US, Vietnam and Thailand [45,46,47,48]. Almost half of the medicines bought in community pharmacies for the purpose of this study did not bear any imprint, with half of these unimprinted medicines having look-alike units in the collection. Moreover, a substantial minority of the imprinted medicines also had look-alike units. In our study, the misidentifications of MUIs by the photograph tool because of look-alike medicines, questions the global utility of these tools in routine, especially for the identification of unimprinted units. However, in the presence of unknown imprinted medicine, it could be useful as a rapid screening tool, and active pharmaceutical ingredient-specific identification by physicochemical techniques such as thin-layer chromatography should be performed (e.g. with the Global Pharma Health Fund Minilab) [49]. Other devices, such as handheld devices using Raman or near-infrared instrumentation [50], or MS and low-field NMR technologies [51, 52], although more costly, would be of great utility in clinical settings while medicines continue to be unlabelled. However, in L/MICs, such physicochemical identification techniques cannot be implemented easily in health structures and are usually not affordable.
Trademark imprints on tablets or capsules are clearly insufficient for pill identification, and, rather than investing in complicated and expensive chemistry, it would be more preferable if a global standardized imprint identification coding system for tablets/capsules was introduced, as discussed in the early 2010s [53]. Harmonized, internationally accepted coding systems exist for other small products, such as the colour codes to identify electrical resistors [54], but still nothing is in place for pharmaceuticals. A sustainable comprehensive and easily available database of these codes would allow patients and health professionals to rapidly identify the active pharmaceutical ingredient(s) in medicines and abolish MUI. The WHO leads the International Nonproprietary Names system and we suggest that this should be expanded to an international pharmaceutical identity coding system [55].
5 Conclusion
The results of this cross-sectional study performed in a teaching hospital of Lao PDR highlighted that exposure to medicines not sold in their original packaging and without written identity is a factor associated with a higher risk of ADR-related hospitalizations. The majority of unimprinted tablets/capsules collected during this study had at least one look-alike unit in the collection of medicines collected for identification of the medicines through their visual aspect. Therefore, visual identification of the collected medicines was not sufficient and a physicochemical analysis was required.
The hazardous consequences of practices of use of MUIs must be investigated, particularly in developing countries where capacities for drug analysis are limited. Although any pharmaceutical identity coding system would not substitute the need for improvement in good dispensing practices, it is time for patient protection through research for an international unambiguous pharmaceutical unit imprinting.
References
World Health Organization. WHO Patient Safety Research. 2009. Available at: http://apps.who.int/iris/bitstream/10665/70145/1/WHO_IER_PSP_2009.10_eng.pdf. Accessed 14 Feb 2017.
Food and Drug Administration. Guidance for Industry and Investigators Safety: Reporting Requirements for INDs and BA/BE Studies. 2012. Available at: http://www.fda.gov/downloads/Drugs/…/Guidances/UCM227351.pdf. Accessed 14 Feb 2017.
European Medicines Agency. Guideline on good pharmacovigilance practices (GVP)—Annex 1—Definitions (Rev 3). 2012. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2013/05/WC500143294.pdf. Accessed 14 Feb 2017.
Akerele JO, Ukoh GC. Aspects of microbial contamination of tablets dispensed in hospitals and community pharmacies in Benin City, Nigeria. Trop J Pharm Res. 2002;1(1):23–8.
Gaudiano MC, Di Maggio A, Cocchieri E, et al. Medicines informal market in Congo, Burundi and Angola: counterfeit and sub-standard antimalarials. Malar J. 2007;6:22.
Goodman C, Kachur S, Abdulla S, et al. Regulating Tanzania’s drug shops: why do they break the rules, and does it matter? Health Policy Plan. 2007;22(6):393–403.
Evans L, Coignez V, Barojas A, et al. Quality of anti-malarials collected in the private and informal sectors in Guyana and Suriname. Malar J. 2012;11:203.
Naveed Q, Hashmi S, Iqbal A, et al. Analysis of pathogens in nonsterile pharmaceuticals drugs of public hospital of Daman (U.T). Indian J Pharm Sci. 2014;4:1–3.
Yong YL, Plançon A, Lau YH, et al. Collaborative health and enforcement operations on the quality of antimalarials and antibiotics in southeast Asia. Am J Trop Med Hyg. 2015;92(6 Suppl):105–12.
Goodman C, Brieger W, Unwin A, et al. Medicine sellers and malaria treatment in sub-Saharan Africa: what do they do and how can their practice be improved? Am J Trop Med Hyg. 2007;77:203–18.
Yeung S, Lawford HLS, Tabernero P, et al. Quality of antimalarials at the epicenter of antimalarial drug resistance: results from an overt and mystery client survey in Cambodia. Am J Trop Med Hyg. 2015;92(6 Suppl):39–50.
Kamat VR, Nichter M. Pharmacies, self-medication and pharmaceutical marketing in Bombay, India. Soc Sci Med. 1998;47(6):779–94.
Bate R, Coticelli P, Tren R, et al. Antimalarial drug quality in the most severely malarious parts of Africa: a six country study. PLoS One. 2008;3:e2132.
Bate R, Ayodee T, Tren R, et al.Drug Use in Nigeria-An informal survey of doctors, pharmacists, healthcare workers in Lagos, Ondo, and Ogun, and a pilot quality assessment of essential drugs from Lagos pharmacies. 2009. Available at: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.503.2956&rep=rep1&type=pdf. Accessed 14 Feb 2017.
Hoa NQ, Ohman A, Lundborg CS, et al. Drug use and health-seeking behavior for childhood illness in Vietnam: a qualitative study. Health Policy. 2007;82(3):320–9.
Tipke M, Diallo S, Coulibaly B, et al. Substandard anti-malarial drugs in Burkina Faso. Malar J. 2008;7:95.
Kaur H, Goodman C, Thompson E, et al. A nationwide survey of the quality of antimalarials in retail outlets in Tanzania. PLoS One. 2008;3(10):e3403.
Shrank WH, Agnew-Blais J, Choudhry NK, et al. The variability and quality of medication container labels. Arch Intern Med. 2007;167(16):1760–5.
Westenberger BJ, Ellison CD, Fussner AS, et al. Quality assessment of internet pharmaceutical products using traditional and non-traditional analytical techniques. Int J Pharm. 2005;306(1–2):56–70.
Veronin M. Packaging and labeling of pharmaceutical products obtained from the internet. J Med Internet Res. 2011;13(1):e22.
Stenson B, Syhakhang L, Eriksson B, et al. Real world pharmacy: assessing the quality of private pharmacy practice in the Lao People’s Democratic Republic. Soc Sci Med. 2001;52:393–404.
Newton PN, Hampton CY, Alter-Hall K, et al. Characterization of ‘Yaa Chud’ Medicine on the Thailand-Myanmar border: selecting for drug-resistant malaria and threatening public health. Am J Trop Med Hyg. 2008;79:662–9.
Littrell M, Gatakaa H, Phok S, et al. Case management of malaria fever in Cambodia: results from national anti-malarial outlet and household surveys. Malar J. 2011;10:328.
Tabernero P, Mayxay M, Culzoni MJ, et al. A repeat random survey of the prevalence of falsified and substandard antimalarials in the Lao PDR: a change for the better. Am J Trop Med Hyg. 2015;92(6 Suppl):95–104.
Kongkaew C, Noyce PR, Ashcroft DM. Hospital admissions associated with adverse drug reactions: a systematic review of prospective observational studies. Ann Pharmacother. 2008;42(7):1017–25.
Al Hamid A, Ghaleb M, Aljadhey H, et al. A systematic review of hospitalization resulting from medicine-related problems in adult patients. Br J Clin Pharmacol. 2014;78(2):202–17.
Roulet L, Asseray N, Foucher N, et al. A questionnaire to document self-medication history in adult patients visiting emergency departments. Pharmacoepidemiol Drug Saf. 2013;22(2):151–9.
World Health Organization Collaborating Center for Drug Statistics Methodology. WHOCC - ATC/DDD Index. 2016. Available at: http://www.whocc.no/atc_ddd_index/. Accessed 14 Feb 2017.
Rozich J, Haraden C, Resar R. Adverse drug event trigger tool: a practical methodology for measuring medication related harm. Qual Saf Health Care. 2003;12(3):194–200.
Mehta U, Durrheim DN, Blockman M, et al. Adverse drug reactions in adult medical inpatients in a South African hospital serving a community with a high HIV/AIDS prevalence: prospective observational study. Br J Clin Pharmacol. 2008;65(3):396–406.
World Health Organization-Uppsala Monitoring Centre. The use of the WHO-UMC system for standardised case causality assessment. Available at: http://who-umc.org/Graphics/24734.pdf. Accessed 14 Feb 2017.
Jolivot P-A, Hindlet P, Pichereau C, et al. A systematic review of adult admissions to ICUs related to adverse drug events. Crit Care. 2014;18:643.
Syhakhang L, Freudenthal S, Tomson G, et al. Knowledge and perceptions of drug quality among drug sellers and consumers in Lao PDR. Health Policy Plan. 2004;19(6):391–401.
Karuppanan M, Kang Nee T, Mohd Ali S, et al. The prevalence of adverse drug event-related admissions at a local hospital in Malaysia. Arch Pharm Pract. 2013;4:160.
Alvesson HM, Lindelow M, Khanthaphat B, et al. Coping with uncertainty during healthcare-seeking in Lao PDR. BMC Int Health Hum Rights. 2013;13:28.
Nonaka D, Vongseththa K, Kobayashi J, et al. Public and private sector treatment of malaria in Lao PDR. Acta Trop. 2009;112(3):283–7.
Chen Y, Zhu L-L, Zhou Q. Effects of drug pharmacokinetic/pharmacodynamic properties, characteristics of medication use, and relevant pharmacological interventions on fall risk in elderly patients. Ther Clin Risk Manag. 2014;10:437–48.
Major S, Badr S, Bahlawan L, et al. Drug-related hospitalization at a tertiary teaching center in Lebanon: incidence, associations, and relation to self-medicating behavior. Clin Pharmacol Ther. 1998;64(4):450–61.
Zargarzadeh AH, Emami MH, Hosseini F. Drug-related hospital admissions in a generic pharmaceutical system. Clin Exp Pharmacol Physiol. 2007;34(5–6):494–8.
Chan SL, Ang X, Sani LL, et al. Prevalence and characteristics of adverse drug reactions at admission to hospital: a prospective observational study. Br J Clin Pharmacol. 2016;82(6):1636–46.
Basu S, Millett C. Social epidemiology of hypertension in middle-income countries: determinants of prevalence, diagnosis, treatment, and control in the WHO SAGE study. Hypertension. 2013;62(1):18–26.
Chaleunvong K, Kamsa-Ard S, Suwanrungruang K, et al. Retrospective appraisal of cancer patients from Vientiane Capital City, Lao People’s Democratic Republic (PDR), seeking treatment in Thailand. Asian Pac J Cancer Prev. 2013;14:5435–40.
Stenson B, Syhakhang L, Lundborg CS, et al. Private pharmacy practice and regulation. A randomized trial in Lao P.D.R. Int J Technol Assess Health Care. 2001;17:579–89.
Hefferren JJ. Identification guide for solid dosage forms. J Am Med Assoc. 1959;169:479–84.
RxID. Canadian Pill Identifier - Identify a Tablet. RxID.ca. 2013. Available at: http://canadian-pill-identifier.com/pill-identifier.php?site_language=english. Accessed 14 Feb 2017.
US National Library of Medicines, National Institutes of Health. Identify or Search for a Pill. Pillbox Rapid Identification Reliable Information. 2016. Available at: http://pillbox.nlm.nih.gov/. Accessed 14 Feb 2017.
MIMS. Tìm kiếm hình ảnh nâng cao | MIMS.com Vietnam. MIMS—Mon. Available at: http://www.mims.com/vietnam/image/advancedsearch. Accessed 14 Feb 2017.
Advanced Drug Image Search | MIMS.com Thailand. MIMS—Mon. Available at: http://www.mims.com/thailand/image/advancedsearch. Accessed 14 Feb 2017.
Global Health Pharma Fund. The GPHF-Minilab™—Fact Sheet. GPHF—2016. Available at: http://www.gphf.org/minilab/factsheet.htm. Accessed 14 Feb 2017.
Fernandez FM, Hostetler D, Powell K, et al. Poor quality drugs: grand challenges in high throughput detection, countrywide sampling, and forensics in developing countries. Analyst. 2011;136(15):3073–82.
Pagès G, Gerdova A, Williamson D, et al. Evaluation of a benchtop cryogen-free low-field 1H NMR spectrometer for the analysis of sexual enhancement and weight loss dietary supplements adulterated with pharmaceutical substances. Anal Chem. 2014;86(23):11897–904.
Harris GA, Nyadong L, Fernandez FM. Recent developments in ambient ionization techniques for analytical mass spectrometry. Analyst. 2008;133(10):1297–301.
Schiff GD, Kim S, Seger A, et al. Issues in medication safety. Am J Health Syst Pharm. 2007;64(1):22.
International Electrotechnical Commission. IEC 60062:2016 Marking codes for resistors and capacitors. 2016. Available at: https://webstore.iec.ch/publication/25395. Accessed 14 Feb 2017.
World Health Organization. International Nonproprietary Names. 2016. Available at: http://www.who.int/medicines/services/inn/en/. Accessed 14 Feb 2017.
Acknowledgements
We are very grateful to the Directors of Mahosot Hospital, Dr. Rattanaphone Phetsouvanh, and staff of the Microbiology Laboratory.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
Oral informed consent was obtained from all participants. Ethical clearance for the study was granted by the National Ethics Committee for Health Research, Ministry of Health of the Lao PDR (No. 43/NECHR).
Funding
This work was supported by the Pierre Fabre Foundation, The L’Oreal Foundation-Unesco, the French Ministry of Superior Education and Research, and the French National Agency for the Safety of Medicines and Health Products (ANSM, Project AAP-2012-082). Paul Newton and Mayfong Mayxay are funded by the Wellcome Trust. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Conflict of interest
Céline Caillet, Chanvilay Sichanh, Gaëtan Assemat, Myriam Malet-Martino, Agnès Sommet, Haleh Bagheri, Noudy Sengxeu, Niphonh Mongkhonmath, Mayfong Mayxay, Lamphone Syhakhang, Maryse Lapeyre-Mestre, Paul N. Newton and Anne Roussin declare that they have no competing interests.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Caillet, C., Sichanh, C., Assemat, G. et al. Role of Medicines of Unknown Identity in Adverse Drug Reaction-Related Hospitalizations in Developing Countries: Evidence from a Cross-Sectional Study in a Teaching Hospital in the Lao People’s Democratic Republic. Drug Saf 40, 809–821 (2017). https://doi.org/10.1007/s40264-017-0544-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-017-0544-z