
Abstract
Introduction
Obesity has been associated with increased arterial stiffness. Sex-differences in arterial stiffness in obesity have been less explored.
Aim
To explore sex-differences in arterial stiffness by applanation tonometry in 323 women and 225 with overweight and obesity, free of cardiovascular disease.
Methods
Covariables of arterial stiffness were identified in multivariable linear regression analyses in the total cohort and separately in women and men.
Results
In the total study cohort, women had higher augmentation pressure (AP) and augmentation index (AIx), and lower carotid-femoral pulse wave velocity (cf-PWV) than men, independent of confounders (all p < 0.001). In sex-specific analyses, higher AP was associated with higher age and 24-hours systolic blood pressure (BP), and with lower heart rate in women (all p < 0.001), and with higher age and BP in men (all p < 0.001). Similarly, higher AIx was associated with higher age and BP, and lower body mass index (BMI) and heart rate in women (all p < 0.05), and with higher age in men (all p < 0.001). Higher cf-PWV correlated with higher age and BP in women (all p < 0.005), and additionally with higher heart rate and non-smoking in men (all p < 0.05). When replacing BMI with waist-hip ratio, higher waist-hip ratio was associated with higher cf-PWV in men only (p < 0.05).
Conclusions
Among subjects with overweight and obesity, AP and AIx were higher in women, and cf-PWV was higher in men. Age and 24-hours systolic BP were the main factors associated with arterial stiffness in both sexes, while measures of adiposity had little impact on arterial stiffness.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Arterial stiffness increases in parallel with presence of known cardiovascular (CV) risk factors, in particular age and systolic blood pressure (BP), in both women and men [1,2,3]. There are several methods to assess arterial stiffness, and well-known sex differences between these measures. While the gold standard measure of arterial stiffness, carotid-femoral pulse wave velocity (cf-PWV), is higher in men, other measures like augmentation pressure (AP) and augmentation index (AIx) are higher in women [1, 4]. Among participants with normal BP and body mass index (BMI) in the Framingham Heart Study, women had a lower cf-PWV compared to men up to 70 years of age [2]. Furthermore, in a subset of 4001 healthy participants aged 18–90 years in the Anglo-Cardiff Collaborative Trial, AP and AIx were higher in women compared to men regardless of age, while no sex difference in cf-PWV was found [1].
Obesity leads to chronic CV inflammation and has been associated with increased arterial stiffness [5]. Both prevalence of obesity and adipose tissue distribution differ between women and men [6,7,8,9]. Previous studies of sex differences in arterial stiffness in overweight or obese individuals have found diverging results. In a Dutch population based study, higher BMI was associated with higher cf-PWV only in women, while higher waist circumference and waist-height ratio were associated with higher cf-PWV only in men [10]. In subjects with hypertension and overweight, abdominal adiposity measured by waist–hip ratio and waist-height ratio were associated with higher cf-PWV in both sexes [11]. However, while these previous studies on arterial stiffness in obesity mostly focused on cf-PWV [10, 12], there is less knowledge about how obesity influences other measures of arterial stiffness like AP and AIx. The aim of the current study was to explore covariates of different measures of arterial stiffness among women and men with increased BMI in the FAT associated CardiOvasculaR dysfunction (FATCOR) study.
2 Methods
2.1 Study Population
The FATCOR study was performed from 2009 to 2017 in Bergen, Norway as a collaboration between a general practitioner center specialized in the management of obese patients and the Department of Heart Disease, Haukeland University Hospital. Women and men aged 30–65 years with a BMI >27.0 kg/m2 were recruited after advertisement in a local newspaper and screened by a general practitioner [13]. Exclusion criteria were history of myocardial infarction, gastrointestinal disorders, severe psychiatric illness, or the inability to communicate in Norwegian language. A total number of 620 participants were recruited. For the present analysis, participants who withdrew consent (n = 2), or with incomplete recording of cf-PWV (n = 24), pulse wave analysis (n = 26), and 24-hours (24-h) systolic BP (n = 55) were excluded, leaving 323 women and 225 men eligible for analysis.
2.2 Compliance with Ethical Standards
The FATCOR study was approved by the Regional Ethics Committee (approval number 17173) and complied with the Declaration of Helsinki. All participants signed written informed consent.
2.3 Cardiovascular Risk Factors
Self-reported information about general health, including use of medication, was collected in a standardized questionnaire. The information was quality assured against medical hospital records by a study nurse. BMI was calculated as body weight in kilograms/body height in meters squared (kg/m2). Obesity was defined as BMI ≥30 kg/m2. Waist and hip circumferences were measured as recommended by the WHO using a nonflexible measuring tape [14]. Waist–hip ratio was calculated as waist circumference/hip circumference, and waist-height ratio as waist circumference/body height, all measured in centimeters. Tetrapolar bioelectrical impedance analysis (Tanita-TBF-300A, Tanita Corporation of America, Arlington Heights, USA) was used to analyze body composition. Blood glucose and lipids were measured in fasting, venous blood samples. Diabetes mellitus was considered present if history of diabetes mellitus, fasting blood glucose ≥7 mmol, 2-hours plasma glucose ≥11.1 mmol/l during oral glucose tolerance test (OGTT), or glycated hemoglobin A1C (HbA1c) ≥6.5% [15]. Estimated glomerular filtration rate (eGFR) was calculated using the equation from the Chronic Kidney Disease Epidemiology Collaboration [16]. Smoking was defined as current smoking. High-sensitive C-reactive protein (hs-CRP) was measured in serum by Matrix-Assisted Laser Desorption/Ionization Time-Of-Flight mass spectrometry.
2.4 Blood Pressure Measurement
BP was measured by a study nurse at the general practitioner’s office. Attended BP and heart rate were measured three times with 1 min intervals after 5 min initial rest in the sitting position, using a regularly calibrated digital automatic Omron M4 sphygmomanometer (Omron Healthcare Co. Ltd., Hoofdorp, The Netherlands) and an appropriate cuff size on the non-dominant arm [17]. Clinical BP and heart rate were calculated as the average of the last 2 measurements. 24-h ambulatory BP was recorded using a Diasys Integra II apparatus (Novacor, Cedex, France). BP was recorded every 20 minutes during daytime and every 30 minutes during nighttime with an appropriately sized cuff on the non-dominant arm. Participants were instructed to avoid hard exercise and to relax their arm while the apparatus was measuring, but otherwise engage in normal activities [17]. The 24-h BP recording was repeated if <70% of measurements were valid. Hypertension was considered present if the participant reported use of antihypertensive drugs or had elevated 24-h BP (average 24-h systolic BP ≥130 mmHg or average 24-h diastolic BP ≥80 mmHg) [18].
2.5 Arterial Stiffness
Arterial stiffness was assessed by AP, AIx, and cf-PWV by using applanation tonometry (SphygmoCor, AtCor Medical, Sydney, West Ryde, Australia) under standardized laboratory conditions in accordance with guidelines [4]. Carotid pulse wave analysis was used to estimate AP and AIx. Pulse pressure waveforms were acquired transcutaneously from the right common carotid and femoral arteries with simultaneous recordings of the electrocardiograms to synchronize times for carotid and femoral pulse waves. Cf-PWV was calculated as the distance in meters between the two recording sites divided by the transit time between the recording sites in seconds [4].
2.6 Statistics
Statistical analyses were performed using the IBM SPSS version 28 (IBM, Armonk, New York, USA). Continuous variables are presented as means ± standard deviations, and categorical variables are presented as numbers and percentages. hs-CRP was not normally distributed in the cohort, and therefore presented as median and interquartile range in the total cohort and in groups of women and men, and log transformed before included in statistical analyses. In group comparison, the Student’s t-test was used for continuous variables and the Chi-square test was used for categorical variables. Factors associated with AP, AIx, and cf-PWV were identified in univariable linear regression in the total study cohort and in sex-specific analyses, and significant covariates were included in multivariable models. The multivariable models on AP and AIx were adjusted for sex, age, BMI, 24-h systolic BP, heart rate, and smoking. Multivariable models on cf-PWV were additionally adjusted for diabetes mellitus. In secondary models, BMI was replaced by waist–hip ratio, fat mass percentage, waist circumference, waist-height ratio, and obesity as a categorical variable. Results were reported as standardized β-coefficients and p-values. In all analyses, a p-value<0.05 was considered statistically significant.
3 Results
3.1 Characteristics of the Total Study Population and Groups of Women and Men
Clinical characteristics and data on arterial stiffness are presented in Table 1. In this middle-aged population, women had higher mean AP and AIx compared to men, while men had higher mean cf-PWV than women (all p < 0.001) (Table 1) (Fig. 1). Women also had higher BMI, fat mass percentage, hip circumference, waist-height ratio, and heart rate than men (all p < 0.05). Men had higher waist circumference, waist-hip ratio, 24-h systolic BP and 24-h diastolic BP values, and higher prevalence of hypertension (all p < 0.001). Prevalence of obesity, diabetes mellitus, smoking, and mean eGFR did not differ by sex (all p>0.05).

Measures of arterial stiffness in women and men. Violin plot. The white dot marks the median and the blue bar in the center of the violin marks the interquartile range. The light red and light blue colored areas demonstrate distribution of data in women and men, respectively
3.2 Factors Associated with Arterial Stiffness in the Total Study Population
Results from univariable analyses are presented in Table 2. In multivariable analyses, women had higher AP (β = 0.41) and AIx (β = 0.48) compared to men, independent of age, BMI, 24-h systolic BP, heart rate, and smoking (all p < 0.05) (Table 2). Men had higher cf-PWV (β = 0.16) compared to women, independent of age, BMI, 24-h systolic BP, heart rate, diabetes mellitus, and smoking (all p < 0.001).
3.3 Factors Associated with Arterial Stiffness in Women
Results from univariable analysis are presented in Table 3. In multivariable analysis in women, higher AP was associated with higher age and 24-h systolic BP, and lower heart rate (all p < 0.001) (Table 3). Higher AIx was associated with higher age and 24-h systolic BP, and lower BMI and heart rate (all p < 0.05). In the same model, when BMI was replaced by obesity as a dichotomous variable, obesity was not significantly associated with AIx in women (data not shown). Higher cf-PWV was associated with higher age and 24-h systolic BP (all p < 0.001). Measures of adiposity, including BMI, obesity, waist-hip ratio, fat mass percentage, waist circumference, and waist-height ratio were not significantly associated with cf-PWV in women (all p > 0.05) (Table 4).
3.4 Factors Associated with Arterial Stiffness in Men
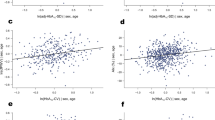
In multivariable analysis in men, higher AP was associated with higher age and 24-h systolic BP (both p < 0.001), while higher AIx was associated with higher age only (p < 0.001) (Table 3). Higher cf-PWV was associated with higher age, 24-h systolic BP, heart rate, and with non-smoking habit (all p < 0.05). Among measures of adiposity, higher cf-PWV was associated with higher waist–hip ratio in men (p < 0.05) (Table 4) (Fig. 2), while no significant associations with BMI, obesity, fat mass percentage, waist circumference, or waist height-ratio were found (Table 4).

Sex specific associations between waist-hip ratio and carotid-femoral pulse wave velocity (cf-PWV) in linear regression analyses. Slope women: 3.4 m/s (p = 0.006). Slope men: 7.7 m/s (p < 0.001)
4 Discussion
This study adds important new knowledge on sex differences in arterial stiffness in overweight and obesity. Among subjects with overweight and obesity in the FATCOR study, women had higher AP and AIx, while cf-PWV was higher in men, independent of confounders. Increasing age and higher 24-h systolic BP were the main factors associated with higher arterial stiffness in both women and men, reflecting previous findings in healthy normal-weight cohorts [1, 2], while measures of adiposity seemed to have little impact on arterial stiffness in the present cohort.
4.1 Sex-Differences in Arterial Stiffness
Our finding that AP and AIx were higher in women, and cf-PWV was higher in men, are in line with previous large population-based studies in healthy, normotensive, non-obese subjects [2, 3, 19]. Prior to the current study, sex-specific information regarding arterial stiffness in obesity was scarce. In a small study of 133 morbidly obese patients, cf-PWV was higher in men than women, and increased in parallel with obesity severity in women, but not in men [20]. However, this study included a high number of patients with diabetes mellitus and coronary artery disease. Current European guidelines for assessment of arterial stiffness recommend use of cf-PWV and consider cf-PWV >10 m/s as a common threshold indicating increased arterial stiffness in both sexes [17]. Taken together, these results suggest that sex-specific thresholds for diagnosis of increased arterial stiffness may be considered when BMI is increased. This should be further tested in prospective outcome studies.
While cf-PWV is dependent on aortic wall stiffness and lumen diameter, AP and AIx are both measures of the peripheral wave reflection and express central pressure wave characteristics in the aorta [21, 22]. In specific, AIx is the proportion of central pulse pressure that is attributable to late systolic increase in pressure caused by overlap between the forward and reflected pressure wave [22]. It has been suggested that AIx is a better measure for arterial stiffness than cf-PWV in individuals under 50 years of age [1]. Still, few previous studies on arterial stiffness in obesity have included assessment of arterial stiffness by measures of peripheral wave reflection like AP and AIx. The Copenhagen City Heart Study found that age-group specific high AIx was significantly related to all-cause mortality in men but not in women, even after adjusting for CV risk factors such as BP [23]. In the present study, higher age and 24-h systolic BP were the most important factors associated with higher AP in both sexes. Higher levels of 24-h systolic BP were strongly associated with AIx only in women, suggesting important sex-differences in BP related pulsative vascular load. This is in line with previous findings that young women are more prone to develop hypertension and associated complications in obesity compared to their male counterparts [24]. Furthermore, sex differences in pulsative vascular load may partly explain why hypertension is a stronger risk factor for heart disease in women compared to men [25].
Interestingly, lower BMI was associated with higher AIx in women in the current study. However, when adjusting for BMI as a dichotomous variable, obesity was not associated with AIx in women, nor in men. In contrast, a study in normotensive non-obese healthy men and women found that BMI, waist circumference, and waist-hip ratio were inversely associated with aortic AIx in women [26], after adjusting for confounders.
4.2 Association of Different Measures of Adiposity with Arterial Stiffness
Body fat distribution differ by sex [9]. Visceral adipose tissue is on both relative and absolute terms higher in men than in women, while the amount of subcutaneous adipose tissue is relatively higher in women [9]. Measures of obesity have been associated with arterial stiffness in both women and men in population-based studies [27, 28]. In a large Italian population-based study, an association between adiposity and cf-PWV was found in both sexes [27]. A Czech population-based study found that measures of abdominal adiposity such as waist circumference, waist-hip ratio, and waist-height ratio correlated better with cf-PWV than general adiposity measures such as BMI, even after adjusting for age, sex, mean arterial pressure, hypertension, diabetes mellitus, and dyslipidemia [29]. In a small Brazilian study in obese adults without diabetes mellitus, lower American Heart Association CV health life’s essential 8 score (based on health behaviours and metabolic risk factors) was associated with higher AP, but not with cf-PWV [30]. However, lower score was associated with high-for-age cf-PWV, reflecting early vascular aging. Among overweight and obese participants in the current study, waist-hip ratio was the only measure of adiposity that was significantly associated with cf-PWV, but only in men. Taken together, these results may suggest that in a population with increased BMI, the level of obesity has less impact on arterial stiffness.
4.3 Other Confounders of Arterial Stiffness
Traditionally, office BP measurement has been used to identify hypertension, and most studies on arterial stiffness have reported office BP [1, 20]. The use of 24-h BP is advantageous in obesity because the prevalence of masked hypertension is greater than in the general population [31]. Furthermore, 24-h BP has a stronger association with CV organ damage compared to office BP [32]. Therefore, 24-h systolic BP was measured in the present study. As demonstrated, higher age and 24-h systolic BP were the main covariables of higher AP and cf-PWV both in women and men.
Higher heart rate was associated with higher cf-PWV in men. In contrast, among women, higher heart rate was associated with both lower AP and AIx. Earlier studies have demonstrated the same negative association between heart rate and AIx [33]. The lower AIx found with increasing heart rate may be explained by a reduction in ejection duration, causing a shift of the reflected pulse wave into diastole [33].
5 Study Limitations
Health information in the current study was self-reported, and even though the information was quality assured by a study nurse, health problems may have been underreported.
Volunteer bias is also possible as participants were recruited via advertisement in a local newspaper. The design of this study was cross-sectional, hence cause–effect relationship could not be confirmed, and future prospective longitudinal studies might therefore be necessary. The low prevalence of diabetes mellitus in the FATCOR study cohort precluded more detailed assessment of this important risk factor. The association of obesity-associated chronic CV inflammation with arterial stiffness could not be widely explored, since only data on hs-CRP was available for the present analysis. Performing bioelectrical analysis using foot-foot system may result in underestimation of the actual fat-free mass in subjects with increased BMI, and also result in underestimation and overestimation of body fat in men and women, respectively [34].
6 Conclusion
In the FATCOR study, including overweight and obese subjects without known CV disease, AP and AIx were higher in women, while cf-PWV was higher in men. The main factors associated with increased arterial stiffness in both sexes were higher age and 24-h systolic BP. Measures of adiposity had little impact on arterial stiffness among overweight and obese subjects in the present study.
References
McEniery CM, Yasmin Hall IR, Qasem A, Wilkinson IB, Cockcroft JR. Normal vascular aging: differential effects on wave reflection and aortic pulse wave velocity: the Anglo-Cardiff Collaborative Trial (ACCT). J Am Coll Cardiol. 2005;46(9):1753–60.
Mitchell GF, Parise H, Benjamin EJ, Larson MG, Keyes MJ, Vita JA, Vasan RS, Levy D. Changes in arterial stiffness and wave reflection with advancing age in healthy men and women: the Framingham Heart Study. Hypertension. 2004;43(6):1239–45.
Sutton-Tyrrell K, Newman A, Simonsick EM, Havlik R, Pahor M, Lakatta E, Spurgeon H, Vaitkevicius P. Aortic stiffness is associated with visceral adiposity in older adults enrolled in the study of health, aging, and body composition. Hypertension. 2001;38(3):429–33.
Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier H. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27(21):2588–605.
Jain S, Khera R, Corrales-Medina VF, Townsend RR, Chirinos JA. Inflammation and arterial stiffness in humans. Atherosclerosis. 2014;237(2):381–90.
Flegal KM, Kruszon-Moran D, Carroll MD, Fryar CD, Ogden CL. Trends in obesity among adults in the United States, 2005 to 2014. JAMA. 2016;315(21):2284–91.
Ogden CL, Carroll MD, Fryar CD, Flegal KM. Prevalence of obesity among adults and youth: United States, 2011–2014. NCHS Data Brief. 2015;219:1–8.
Taylor H, Liu J, Wilson G, Golden SH, Crook E, Brunson CD, Steffes M, Johnson WD, Sung JH. Distinct component profiles and high risk among African Americans with metabolic syndrome: the Jackson Heart Study. Diabetes Care. 2008;31(6):1248–53.
Geer EB, Shen W. Gender differences in insulin resistance, body composition, and energy balance. Gend Med. 2009;6(Suppl 1):60–75.
van den Munckhof ICL, Holewijn S, de Graaf J, Rutten JHW. Sex differences in fat distribution influence the association between BMI and arterial stiffness. J Hypertens. 2017;35(6):1219–25.
Vallée A, Olié V, Lelong HÉL, Kretz S, Safar ME, Blacher J. Relationship between BMI and aortic stiffness: influence of anthropometric indices in hypertensive men and women. J Hypertens. 2020;38(2):249–56.
Zuo J, Chao H, Tang B, Avolio AP, Schlaich MP, Nolde JM, Adji A, Carnagarin R. Female gender is associated with higher susceptibility of weight induced arterial stiffening and rise in blood pressure. J Clin Med. 2021;10(16):3479.
Halland H, Matre K, Einarsen E, Midtbø H, Saeed S, Pristaj N, Lønnebakken MT, Gerdts E. Effect of fitness on cardiac structure and function in overweight and obesity (the FATCOR study). Nutr Metab Cardiovasc Dis. 2019;29(7):710–7.
Nishida C, Ko GT, Kumanyika S. Body fat distribution and noncommunicable diseases in populations: overview of the 2008 WHO Expert Consultation on Waist Circumference and Waist-Hip Ratio. Eur J Clin Nutr. 2010;64(1):2–5.
American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81-90.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, Coresh J. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–12.
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, Kahan T, Mahfoud F, Redon J, Ruilope L, Zanchetti A, Kerins M, Kjeldsen SE, Kreutz R, Laurent S, Lip GYH, McManus R, Narkiewicz K, Ruschitzka F, Schmieder RE, Shlyakhto E, Tsioufis C, Aboyans V, Desormais I. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021–104.
Halland H, Lønnebakken MT, Saeed S, Midtbø H, Cramariuc D, Gerdts E. Does fitness improve the cardiovascular risk profile in obese subjects? Nutr Metab Cardiovasc Dis. 2017;27(6):518–24.
Kalenga CZ, Ramesh S, Dumanski SM, MacRae JM, Nerenberg K, Metcalfe A, Sola DY, Ahmed SB. Sex influences the effect of adiposity on arterial stiffness and renin-angiotensin aldosterone system activity in young adults. Endocrinol Diabetes Metab. 2022;5(2): e00317.
Nordstrand N, Gjevestad E, Dinh KN, Hofsø D, Røislien J, Saltvedt E, Os I, Hjelmesæth J. The relationship between various measures of obesity and arterial stiffness in morbidly obese patients. BMC Cardiovasc Disord. 2011;11:7.
Gurovich AN, Braith RW. Pulse wave analysis and pulse wave velocity techniques: are they ready for the clinic? Hypertens Res. 2011;34(2):166–9.
Kaess BM, Rong J, Larson MG, Hamburg NM, Vita JA, Levy D, Benjamin EJ, Vasan RS, Mitchell GF. Aortic stiffness, blood pressure progression, and incident hypertension. JAMA. 2012;308(9):875–81.
Janner JH, Godtfredsen NS, Ladelund S, Vestbo J, Prescott E. High aortic augmentation index predicts mortality and cardiovascular events in men from a general population, but not in women. Eur J Prev Cardiol. 2013;20(6):1005–12.
Sharabi Y, Grotto I, Huerta M, Grossman E. Susceptibility of the influence of weight on blood pressure in men versus women: lessons from a large-scale study of young adults. Am J Hypertens. 2004;17(5 Pt 1):404–8.
Kringeland E, Tell GS, Midtbø H, Igland J, Haugsgjerd TR, Gerdts E. Stage 1 hypertension, sex, and acute coronary syndromes during midlife: the Hordaland Health Study. Eur J Prev Cardiol. 2021;29(1):147–54.
Budimir D, Jeroncic A, Gunjaca G, Rudan I, Polasek O, Boban M. Sex-specific association of anthropometric measures of body composition with arterial stiffness in a healthy population. Med Sci Monit. 2012;18(2):Cr65-71.
Scuteri A, Orru M, Morrell CH, Tarasov K, Schlessinger D, Uda M, Lakatta EG. Associations of large artery structure and function with adiposity: effects of age, gender, and hypertension. The SardiNIA Study. Atherosclerosis. 2012;221(1):189–97.
Lee CM, Huxley RR, Wildman RP, Woodward M. Indices of abdominal obesity are better discriminators of cardiovascular risk factors than BMI: a meta-analysis. J Clin Epidemiol. 2008;61(7):646–53.
Wohlfahrt P, Somers VK, Cifkova R, Filipovsky J, Seidlerova J, Krajcoviechova A, Sochor O, Kullo IJ, Lopez-Jimenez F. Relationship between measures of central and general adiposity with aortic stiffness in the general population. Atherosclerosis. 2014;235(2):625–31.
Cunha MR, Mattos S, Klein M, Neves MF. Early vascular aging in obese individuals with low cardiovascular health. High Blood Press Cardiovasc Prev. 2023;30(1):45–54.
Kenny IE, Saeed S, Gerdts E, Midtbø H, Halland H, Lønnebakken MT. Masked hypertension in obesity: potential predictors and arterial damage. Blood Press Monit. 2017;22(1):12–7.
Bliziotis IA, Destounis A, Stergiou GS. Home versus ambulatory and office blood pressure in predicting target organ damage in hypertension: a systematic review and meta-analysis. J Hypertens. 2012;30(7):1289–99.
Wilkinson IB, MacCallum H, Flint L, Cockcroft JR, Newby DE, Webb DJ. The influence of heart rate on augmentation index and central arterial pressure in humans. J Physiol. 2000;525(Pt 1):263–70.
Dittmar M. Comparison of bipolar and tetrapolar impedance techniques for assessing fat mass. Am J Hum Biol. 2004;16(5):593–7.
Acknowledgements
We thank Hilde Jacobsen (staff engineer), Marina V. Kokorina (MD), Synnøve Ygre Hauge (RN) and Liv Himle (RN) for technical assistance with participant management, registration, and data collection.
Funding
Open access funding provided by University of Bergen (incl. Haukeland University Hospital). Western Norwegian Health Authorities Grant number 911402.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest.
Funding
The current study was funded by a donation from the Western Norwegian Health Authorities and from the Grieg Foundation, Bergen, Norway. The funding sources did not participate in study design, data collection, overall design and data interpretation, nor in writing the manuscript and further submitting the manuscript for publication.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Eikås, J.G., Gerdts, E., Halland, H. et al. Arterial Stiffness in Overweight and Obesity: Association with Sex, Age, and Blood Pressure. High Blood Press Cardiovasc Prev 30, 435–443 (2023). https://doi.org/10.1007/s40292-023-00593-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40292-023-00593-2