
Abstract
Background
Evidence about the relationship between albumin-bilirubin (ALBI) grade and sequential systemic therapy for advanced hepatocellular carcinoma in real-world Japanese clinical practice is limited.
Objective
The objective of this study was to investigate ALBI grades and sequential treatment for advanced hepatocellular carcinoma in Japanese clinical practice.
Methods
We conducted a retrospective cohort study using a Japanese hospital-based administration database to assess treatment sequence in patients with confirmed advanced hepatocellular carcinoma and first prescription (index line) of lenvatinib (July 2014–June 2019; N = 1558) or sorafenib (July 2014–June 2016 [sorafenib-A; N = 1511] or June 2017–June 2019 [sorafenib-B; N = 1276]). Transition to subsequent line was assessed in patients who completed the index line without transarterial chemoembolization. The ALBI grade and sequential treatment relationships were analyzed in patients with baseline and/or end of index line ALBI scores.
Results
Transition to a subsequent line was low (sorafenib-A [n = 1320]: 12.6%; sorafenib-B [n = 1049]: 40.7%; lenvatinib [n = 786]: 27.2%). In patients with baseline ALBI data (combined cohorts; n = 385), overall treatment duration was shorter in those with baseline ALBI grade 2b or 3 vs grade 1 or 2a (median: 7.1, 6.7, 4.5, and 3.0 months for grades 1, 2a, 2b, and 3, respectively). In patients with baseline and end of index line ALBI data (combined cohorts; n = 222), ALBI grade worsened during index line regardless of baseline grade. Of these patients in the sorafenib-B or lenvatinib cohorts who completed the index line without transarterial chemoembolization (n = 120), transition to a subsequent line was higher with the end of index line grade 1/2a (66.7/68.4%) than with grade 2b/3 (34.0/11.1%).
Conclusions
Adequate liver function, indicated by ALBI grade, at the start and end of first-line treatment is associated with successful sequential therapy in Japanese clinical practice.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
In this study of real-world clinical practice in Japan, better liver function (measured with albumin-bilirubin grade using serum albumin and total bilirubin) at the start of anti-cancer treatment was associated with longer overall treatment period in patients with advanced liver cancer. |
Liver function can deteriorate during anti-cancer treatment, and deterioration was associated with worse prognosis for these patients. |
These results imply that starting anti-cancer treatment before liver function deteriorates and preserving liver function as much as possible during treatment are important for improving patient outcomes. |
1 Introduction
Hepatocellular carcinoma (HCC) is the most common form of liver cancer and is a leading cause of death worldwide [1, 2]. Early-stage HCC can often be successfully treated by surgical resection, transplantation, or radiofrequency or microwave ablation. At later stages, treatment includes transarterial chemoembolization (TACE) for intermediate-stage HCC and systemic treatments for advanced HCC. Current Japanese treatment guidelines recommend sorafenib (approved in 2009) and lenvatinib (approved in 2018) as standard first-line treatment, and regorafenib (approved in 2017) as standard second-line treatment, for advanced HCC [3]. The choice of treatment depends not only on the cancer stage, but also on the extent of liver damage [2]. Most patients with HCC also have cirrhosis caused by pre-existing medical conditions, such as hepatitis or alcoholic liver disease. Because some treatments can further deteriorate liver function, the level of residual function should be considered when choosing treatment options and monitored during cancer treatment.
The Child–Pugh grading system has been used extensively to assess liver function [4]. However, the Child–Pugh system includes measures that are primarily subjective (ascites and encephalopathy) or are interrelated (e.g., ascites and serum albumin level), and may not be optimal for assessing liver function in patients with HCC to identify potential candidates eligible for systemic treatment according to current guidelines [5]. Recently, the albumin-bilirubin (ALBI) score has been proposed as an objective and simpler alternative to the Child–Pugh grading system for assessing liver function in patients with HCC [5, 6]. The ALBI scoring system is based only on objective laboratory measurements of serum albumin and total bilirubin, as determined by the equation: ALBI score = (log10 bilirubin [μmol/L] × 0.66) + (albumin [g/L] × − 0.085). This is advantageous when used in retrospective database studies because laboratory measurement results are relatively more accessible compared with other clinical information in secondary data sources in Japan [7,8,9]. Another advantage is that the ALBI score can be evaluated as a continuous measure, and can also be further divided into defined categories based on clinically relevant criteria. Evidence suggests that the ALBI score is a better predictor of prognosis following curative or palliative treatment than the Child–Pugh grade [6, 10,11,12]. Although several studies from academic institutions such as university hospitals have been published recently [11, 13,14,15,16], information about the distribution of ALBI scores/grades and their relationship with successful sequential systemic treatment in real-world clinical practice in Japan is still limited. Given that the current standard-of-care (SoC) systemic therapies were developed primarily in patients with better liver function (Child–Pugh grade A), it is important to assess whether the variation in liver function seen in clinical practice affects sequential treatment.
Administrative claims databases, which routinely collect information on daily medical activities, are considered a suitable and valuable data source for the investigation of real-world clinical practice. In this study, we used a hospital-based administrative database in Japan to investigate the distribution of ALBI scores and grades at baseline and at the end of first-line treatment in patients with HCC who were treated with SoC systemic therapy. We also described patient characteristics, the pattern of SoC treatment, and the relationship between ALBI score/grade and sequential SoC treatment, including duration of treatment.
2 Materials and Methods
2.1 Study Design
This was a retrospective observational cohort study using data from the Medical Data Vision Co., Ltd (MDV) database (Tokyo, Japan) [7]. The MDV database includes de-identified administrative claims and Diagnosis Procedure Combination (DPC; a per diem payment system for acute inpatient care using a diagnosis classification) data from hospitalizations and outpatient visits to hospitals participating in the DPC system in Japan. The DPC system encompasses hospitals that provide acute-phase medical care and may also provide other levels of care [17, 18]. As of September 2019, the MDV database included approximately 28.4 million patients from 385 DPC hospitals (approximately 22% of DPC hospitals in Japan) and is one of the largest claims databases available in Japan with access to some laboratory test results [8]. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and Good Pharmacoepidemiology Practices. Because the study used retrospective de-identified data, ethical review and informed consent were not required, in line with the Japanese Ethical Guidelines for Medical and Health Research Involving Human Subjects.
2.2 Study Population
Patients for this study were derived from the population with at least one confirmed neoplasm diagnosis (International Statistical Classification of Diseases and Related Health Problems, 10th Revision [ICD-10] codes C00–D48) in the MDV database between April 2008 and June 2019 (data cut-off by MDV on 23 August, 2019). From this starting population, patient eligibility was determined using database records for the selection period 1 July, 2014 to 30 June, 2019; the selection period dates were chosen to include similar observation durations before and after the approval of regorafenib in June 2017. Patients were included in the overall cohort if they were ≥ 20 years of age at the index date (defined as the date of the first prescription of sorafenib or lenvatinib during the selection period, which was considered the index line treatment) and had at least one confirmed diagnosis of HCC (Table 1 of the Electronic Supplementary Material [ESM]) during the selection period. Our analysis was limited to patients who newly initiated sorafenib or lenvatinib during the selection period with no SoC prescription within 3 years before the index date, and to patients with more than 5 days between the index date and the last prescription of index line treatment, to exclude early discontinuations possibly owing to acute adverse events. Patients were excluded if they had hospitalization as part of a clinical trial between each patient’s index date and the end of the selection period (outpatient visits that were part of a clinical trial could not be identified in the database).
Patients were assigned to three cohorts based on their index line treatment (earliest prescription of sorafenib or lenvatinib during the selection period), which was assumed to be first-line treatment (Fig. 1). As sorafenib was approved before regorafenib was available as second-line treatment for HCC in June 2017, patients with sorafenib as index line treatment were divided into two cohorts based on the index date to account for potential changes in clinical practice. Patients whose index line treatment was sorafenib with an index date between July 2014 and June 2016 or between June 2017 and June 2019 were assigned to the sorafenib A cohort or the sorafenib B cohort, respectively. Most patients in the sorafenib A cohort were presumed not to have been able to receive regorafenib as second-line treatment. Patients prescribed sorafenib with an index date between July 2016 and May 2017 were not included in the analysis because the availability of second-line treatments could vary after the approval of regorafenib in June 2017, which would complicate the interpretation of treatment sequence results. The lenvatinib cohort included all patients with lenvatinib as the index line treatment.

Study design. 1L index line treatment (assumed first line), 2L subsequent line treatment (assumed second line), ALBI albumin-bilirubin, HCC hepatocellular carcinoma, SoC standard of care
2.3 Baseline Demographics and Clinical Characteristics
Demographic and clinical characteristics during the baseline period (defined as 60 days before and including the index date) included age at index date, sex, body mass index, tumor-node-metastasis (TNM) cancer stage (where available), presence of hospital admission within 60 days before the index date (but excluding index date), and comorbidities (including diabetes mellitus, hepatitis B or C, alcoholic liver disease, or any liver diseases [ICD-10 codes K70–K77; includes alcoholic liver disease], as defined in Table 1 of the ESM). Baseline laboratory test results were summarized (where available), including albumin, total bilirubin, prothrombin time and international normalized ratio, creatinine, and alpha-fetoprotein. The Fibrosis-4 Index (a non-invasive scoring system used to estimate the level of liver scarring [19, 20]) was calculated based on platelet count, aspartate transaminase, and alanine transaminase data. A model for end-stage liver disease score was calculated based on creatinine, bilirubin, and prothrombin time and international normalized ratio [21]. Other collected information included whether the treating facility was a designated cancer hospital and whether the patient had undergone TACE within 3 years before the index date (to account for any potential impact of TACE on the ALBI score during index line treatment).
2.4 Treatment Sequence
The sequence of treatment with SoC therapy was assessed in each cohort. Index line treatment started on the index date, and the subsequent line of therapy was considered to have started when the patient started another SoC or restarted the same SoC after a gap (last prescription plus days of supply) of 60 days or longer, whichever occurred first. In the absence of subsequent treatment lines, the index line was considered ended when the number of days after the last dose date that elapsed was twice the average number of days supplied per SoC prescription in an outpatient setting, calculated individually for that patient. For patients without outpatient prescriptions during the index line, this duration was imputed using the median value for the rest of the cohort. The end date of the index line was defined as the last presumed dose date of the SoC in the index line (the date of the last SoC prescription in the index line plus the number of days supplied minus 1 day). As the MDV database does not define lines of therapy, the index line was assumed to be first line in this study. For those with subsequent treatment lines, second-line and third-line were defined in the same manner.
2.5 Overall Treatment Duration and Transition Rate
Overall treatment duration was defined as the time from the index date to the estimated end of therapy, defined as the date of last SoC prescription plus the number of days supplied minus 1 day. In the time-to-event analysis of overall treatment duration, patients with < 60 days between the estimated end of therapy and the end of available data were censored at the estimated dosing date of the last observed SoC, without defining the event. The rate of transition from the index line to subsequent line treatment was assessed in patients who completed index line treatment without TACE during index line treatment. Patients with TACE during index line treatment were not included in the analysis because of the possible effect of TACE on the ALBI score.
2.6 ALBI Score and Grade
The ALBI scores were determined from laboratory test results for albumin and total bilirubin, where available, using the equation ALBI score = (log10 bilirubin [μmol/L] × 0.66) + (albumin [g/L] × − 0.085) [5, 22]. Modified ALBI grades were assigned according to the ALBI scores, wherein an ALBI score ≤ − 2.60 was grade 1, − 2.60 < ALBI score ≤ − 2.27 was grade 2a, − 2.27 < ALBI score ≤− 1.39 was grade 2b, and ALBI score >− 1.39 was grade 3 [22]. Using this system, a higher ALBI score/grade indicates worse liver function. The ALBI score and grade were determined during the baseline period, using the last value before index line treatment started, and around the end of the index line treatment, using the first value available between −5 and +15 days of the end of the index line treatment and before subsequent line treatment started (Fig. 1). The ALBI score and grade at the end of index line treatment were only analyzed in patients who had completed the index line without TACE during index line treatment (as defined above), and with a baseline ALBI score. The ALBI grade was considered to have worsened if it changed from grade 1 or 2a at baseline to grade 2b or 3 at the end of index line treatment.
2.7 Statistical Analysis
The descriptive statistics of collected data are presented as n (%), mean with standard deviation, and/or median with interquartile range, as applicable, for patients in each overall cohort and for those patients in each cohort with baseline ALBI data available. The ALBI scores at baseline and at the end of index line treatment were compared using a paired t test in patients who completed index line treatment without TACE and who had ALBI data available at both timepoints (all cohorts combined). Overall treatment duration by baseline ALBI grade was analyzed by the Kaplan–Meier method in patients with baseline ALBI available and with all cohorts combined. The median overall treatment duration and 95% confidence intervals (CIs) were calculated and compared among patients with different baseline ALBI grades using a log-rank test. Multiple logistic regression was used to determine available factors associated with ALBI grade worsening from baseline to the end of the index line treatment. A Cox regression model was used to explore factors associated with the overall duration of systemic treatment. Sample selection and creation of analytic variables were performed using the Instant Health Data platform (Panalgo, Boston, MA, USA). Statistical analyses were undertaken with R, Version 3.2.1 (R Foundation for Statistical Computing, Vienna, Austria) and SAS, Version 9.4 (SAS Institute, Cary, NC, USA), and a two-sided p < 0.05 was considered statistically significant.
3 Results
3.1 Patient Selection
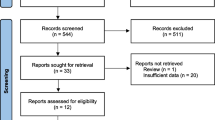
A total of 80,698 patients had at least one confirmed diagnosis of HCC during the selection period (1 July, 2014 to 30 June, 2019) (Fig. 2a). Of these, 1511 patients who received sorafenib as the index line treatment in or before June 2016 comprised the sorafenib A cohort, and 1276 patients who received sorafenib as the index line treatment in or after June 2017 comprised the sorafenib B cohort. Similarly, 1558 patients who received lenvatinib as the index line treatment and met other eligibility criteria comprised the lenvatinib cohort. Treatment sequence was summarized for these three cohorts. Within each cohort, 1320 (87.4%), 1049 (82.2%), and 786 (50.4%) patients, respectively, were considered to have completed index line treatment without concurrent TACE and were evaluated for transition to subsequent line treatment (Fig. 2a). Demographic and baseline clinical characteristics for the full cohorts are shown in Table 1.

Patient flow diagram. a Overall lenvatinib, sorafenib A, and sorafenib B cohorts evaluated for treatment sequence, and subgroups of these patients who completed index line treatment without transarterial chemoembolization (TACE) during index line treatment evaluated for transition to subsequent line treatment. b Patients in each cohort with baseline albumin-bilirubin (ALBI) data available evaluated for overall duration of treatment by baseline ALBI grade, and subgroups of these patients who completed index line treatment without TACE during index line treatment evaluated for ALBI score/grade at the end of index line treatment. 1L index line treatment (assumed first line), 2L subsequent line treatment (assumed second line), HCC hepatocellular carcinoma, MDV Medical Data Vision, SoC standard of care. aExclusion criteria: age < 20 years at index date, any SoCs in 3 years before the index date, ≤ 5 days from the index date to last 1L prescription, clinical trial inpatient visits between index date and 30 June, 2019
Baseline ALBI results were available for 140 (9.3%), 103 (8.1%), and 142 (9.1%) patients in the sorafenib A, sorafenib B, and lenvatinib cohorts, respectively, consistent with the general availability of laboratory test results in the MDV database. The baseline ALBI cohorts were pooled for evaluation of the overall treatment duration by baseline ALBI grade (N = 385; Fig. 2b). Of these, 102 (72.9%), 68 (66.0%), and 52 (36.6%) patients, respectively, completed index line treatment without concurrent TACE and were pooled for evaluation of ALBI score/grade at the end of index line treatment (N = 222; Fig. 2b).
3.2 Treatment Sequence
Treatment sequence was evaluated in each of the three cohorts (Fig. 1 of the ESM). In the sorafenib A cohort, the most common therapy after the sorafenib index line treatment line was re-administration of sorafenib after a treatment gap of at least 60 days, which was classified as a subsequent treatment line in this study (148 patients; 9.8%). As expected, in the sorafenib B cohort, which included patients who started sorafenib in or after June 2017 when regorafenib became available for HCC, the most common subsequent lines of therapy were lenvatinib (231 patients; 18.1%) and regorafenib (204 patients; 16.0%). In the lenvatinib cohort, the most common subsequent line of therapy was sorafenib (157 patients; 10.1%). Among patients who completed index line treatment without concurrent TACE, the rate of transition to subsequent line treatment was 12.6% in the sorafenib A cohort, 40.7% in the sorafenib B cohort, and 27.2% in the lenvatinib cohort (Table 2).
3.3 Demographic and Baseline Clinical Characteristics in the Baseline ALBI Cohorts
Among patients with baseline ALBI scores available, baseline demographic and clinical characteristics were generally similar across the three cohorts (Table 3) and were similar to the full cohorts (Table 1). Approximately 80% of patients were male, with a mean age of around 70 years. More than half (63.1%) of patients had been admitted to hospital during the 60-day baseline period; of those with tumor stage information, most had Stage III or IV cancer. Comorbidities of interest were commonly observed in the study population, with approximately half of patients having any liver disease (ICD-10 codes K70–K77) or diabetes mellitus, and about 40% having hepatitis C. The utilization rate of TACE within 3 years before the index date was 60.0%, 64.1%, and 67.8% in the sorafenib A, sorafenib B, and lenvatinib cohorts, respectively.
3.4 Change in ALBI Score/Grade from Baseline to End of Index Line Treatment
Among patients who completed index line treatment without concurrent TACE and who had ALBI data available at both baseline and at the end of index line treatment (combined N = 222), average ALBI scores significantly increased (i.e., worsened) from − 2.26 at baseline to −1.75 at the end of index line treatment (p < 0.0001; Fig. 3a). The extent of ALBI score worsening was similar regardless of baseline ALBI grade (grade 1/2a or grade 2b/3). The distribution of ALBI grades at the end of index line treatment compared with baseline also indicated worsening during treatment (Fig. 3b). At baseline, approximately 54% of patients had ALBI grade 1 or 2a, and only 6.3% had ALBI grade 3. By the end of index line treatment, only about 25% had ALBI grade 1 or 2a, and about 30% had ALBI grade 3. The ALBI scores/grades for each cohort at baseline and at the end of index line treatment are shown in Fig. 2 of the ESM.

a Mean (± SD) albumin-bilirubin (ALBI) score at baseline (BL) and at the end of index line treatment. Patients from all cohorts who completed index line treatment without transarterial chemoembolization (TACE) and had ALBI scores available at BL and at the end of index line treatment were included (N = 222; BL ALBI grade 1/2a, n = 120; BL ALBI grade 2b/3, n = 102). b Distribution of ALBI grade at BL and at the end of index line treatment in patients who completed index line treatment without TACE and who had ALBI scores available at both timepoints (N = 222). 1L index line treatment (assumed first line), SD standard deviation
3.5 Factors Associated with Worsening ALBI Grade
In a multiple logistic regression analysis, ALBI grade was less likely to worsen from baseline to the end of index line treatment in patients who were treated at a designated cancer hospital than in patients who were treated at other hospitals (odds ratio [95% CI]: 0.14 [0.03–0.71], p = 0.0175; Table 4). As expected, a baseline ALBI grade of 2a was significantly associated with an increased likelihood (relative to grade 1) of ALBI grade worsening to grade 2b or 3 (odds ratio [95% CI]: 7.45 [2.90–19.16], p < 0.0001; Table 4). No other factors were significantly associated with ALBI grade worsening.
3.6 ALBI Grade at End of Index Line Treatment and Rate of Transition to Subsequent Line Treatment
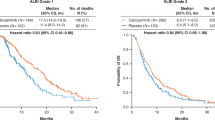
The relationship between end of index line treatment ALBI and transition to subsequent line treatment was examined only in the sorafenib B and lenvatinib cohorts; the sorafenib A cohort was not included in the analysis because of the limited selection of second-line options available to this cohort. Among patients in the combined lenvatinib and sorafenib B cohorts, the rate of transition to second-line treatment was greater in patients with lower ALBI grade at the end of index line treatment (i.e., 1 or 2a vs 2b or 3) (Table 5). Approximately two-thirds (67.7%) of patients with ALBI grade 1 or 2a at the end of index line treatment transitioned to subsequent line treatment, whereas only 34% of patients with ALBI grade 2b and 11% of patients with ALBI grade 3 transitioned.
3.7 Baseline ALBI Grade and Overall Duration of Systemic Treatment
There was a significant difference in the overall duration of treatment across the four baseline ALBI grade groups (log-rank test p < 0.0001; Fig. 4). Median (95% CI) overall treatment duration was shorter in patients with baseline ALBI grade 2b (4.5 [3.0–6.5] months) or 3 (3.0 [0.9–4.9] months) compared with those with grade 1 (7.1 [6.0–12.0] months) or 2a (6.7 [4.6–11.4] months). Cox regression analysis indicated that, relative to patients with ALBI grade 1, patients with ALBI grade 2b (hazard ratio [95% CI]: 1.70 [1.21–2.37], p = 0.0020) and patients with ALBI grade 3 (hazard ratio [95% CI]: 2.40 [1.33–4.35], p = 0.0039) had a significantly higher risk of discontinuing all systemic treatment (Table 2 of the ESM). There was also a statistically significant relationship between the Fibrosis-4 Index and overall treatment duration (hazard ratio [95% CI]: 1.04 [1.01–1.08], p = 0.0156). In an exploratory Cox regression analysis, which included TNM cancer stage as an additional covariate (n = 105), we observed that baseline ALBI grade remained an independent risk factor for treatment discontinuation (grade 2b or 3 vs 1 or 2a: hazard ratio [95% CI]: 1.80 [1.03–3.14], p = 0.04), whereas TNM cancer stage did not show a significant association with treatment duration (stage 3 or 4 vs 1 or 2: hazard ratio [95% CI]: 0.60 [0.30–1.21], p = 0.15).

Overall duration of all systemic treatment by baseline albumin-bilirubin grade. CI confidence interval, SoC standard of care
4 Discussion
The results of this observational cohort study using an administrative claims database indicate that baseline liver function, as assessed by ALBI score/grade, is associated with longer overall SoC treatment duration in real-world clinical practice in Japan. In addition, greater residual liver function at the end of index line treatment is associated with higher rates of transition to subsequent line SoC systemic therapy. These results suggest the importance of starting systemic therapy before liver function deteriorates and that efforts should be made to maintain liver function during systemic treatment to optimize patients’ ability to continue treatment. The rate of transition to subsequent line treatment was low, even after additional SoC options became available (i.e., in the lenvatinib and sorafenib B cohorts; Table 2). This was true also for those with greater residual liver function at the end of index line treatment (Table 5), indicating that other measures are needed to implement more successful sequential therapy in addition to maintaining liver function.
In this study, overall SoC treatment duration was significantly different across the four baseline ALBI grade groups. Median duration of treatment increased with lower ALBI grade and was shorter in patients with baseline ALBI grade 2b or 3 than in those with grade 1 or 2a, indicating that patients with better liver function are more likely to continue systemic therapy. Cox regression analysis confirmed that ALBI grade 2b and grade 3, as well as a higher Fibrosis-4 Index, were associated with shorter overall treatment duration, indicating that both liver function reserve and liver fibrosis affect prognosis. Similarly, the multinational GIDEON registry study reported that the duration of sorafenib treatment and overall survival were longer, and discontinuation because of adverse events was lower, in patients with Child–Pugh grade A than in those with Child–Pugh grade B [23]. Similar results were reported for the Japanese subset of the GIDEON study, whose patients closely resembled those of the current study in terms of age, sex, etiology of HCC, TNM cancer stage, and history of TACE before first-line treatment [24]. Several studies conducted in academic institutions in Japan have also demonstrated that baseline ALBI grade is a significant predictor of overall survival, as well as total duration of treatment [11, 13,14,15,16]. A study by Ueshima et al. reported that baseline ALBI grade was associated with the tumor response rate, as well as the rate of discontinuation because of adverse events [11]. In addition, several studies have reported an association between ALBI grade and overall survival regardless of tumor stage [22, 25, 26]. Because deaths are captured in the MDV database only if they occur during hospitalization, we have not evaluated overall survival in this study. Nevertheless, overall treatment duration with systemic therapies is reported to be associated with overall survival in patients with unresectable HCC [14]. Collectively, these studies, together with our results, indicate that better liver function at the initiation of systemic therapy is associated with longer treatment and better outcomes. As suggested by previous studies, to optimize the likelihood of receiving subsequent treatment lines and to improve survival, systemic treatment should ideally be initiated while patients are still at ALBI grade 1 or at least 2a [13,14,15]. Finally, although our study focused on current tyrosine kinase inhibitor SoC therapies, recent studies indicate that ALBI grade can also predict survival in patients treated with newer immuno-oncology drugs [27, 28], suggesting that preserving liver function will continue to be critical for successful sequential treatment as immuno-oncology drugs become more common.
Among patients who did not receive TACE during index line treatment, the transition rate to subsequent line treatment was higher in the sorafenib B cohort than in the sorafenib A cohort, as might be expected given the availability of second-line options after regorafenib was approved. For most patients in the sorafenib A cohort, no other SoC treatment options were available, and patients had to restart sorafenib as a subsequent line of therapy. The transition rate was also higher in the sorafenib B cohort compared with the lenvatinib cohort; this finding is consistent with previous Japanese studies suggesting that eligibility for second-line treatment was higher in patients treated with sorafenib (57.3% [29]) than in patients treated with lenvatinib (43.8% [15]). This difference in transition rate may partly be explained by a greater proportion of patients in the lenvatinib cohort (38.5%) with ALBI grade 3 at the end of index line treatment compared with the sorafenib cohorts (30.4% in sorafenib A, 23.5% in sorafenib B) [Fig. 2 of the ESM], given the observed association between ALBI grade at the end of the index line and the transition rate to the subsequent line (Table 5). Although it is not clear why the lenvatinib cohort had more ALBI grade 3 patients at the end of the index line, this finding potentially could be related to the longer treatment duration with lenvatinib than sorafenib that was seen in this study (data not shown) and reported in the randomized phase III REFLECT clinical trial (median 5.7 months for lenvatinib, 3.7 months for sorafenib [30]). Our study also found that patients with ALBI grade 1 or 2a at the end of index line treatment proceeded to subsequent line treatment more often than patients with ALBI grade 2b or 3, which may reflect the loss of patients with poorer liver function moving to palliative care or dying. Although these results are based on a relatively small number of patients, particularly with ALBI grade 1 or 2a, the findings suggest that maintenance of liver function during treatment may also improve patients’ ability to continue treatment. Our findings are consistent with those of Pinato et al., who reported that ALBI grade at the end of first-line sorafenib treatment was a predictor of post-sorafenib survival and could be used to guide the selection of patients most likely to benefit from second-line treatment [31]. A retrospective study from Taiwan also reported that more patients with ALBI grade 1 at the end of sorafenib treatment received subsequent therapies compared with patients with ALBI grade 2 (43.9% vs 28%) [32].
This study also documented the deterioration in liver function during index line treatment, even in the absence of TACE during the index line treatment, as shown by the change in ALBI score and grade. Between baseline and the end of index line treatment, mean ALBI score increased (worsened) by approximately 0.5 regardless of baseline ALBI grade. The ALBI grade also worsened during treatment; for example, the percentage of patients with ALBI grade 3 increased from 6.3% to 30.2% through the course of the index line treatment, whereas the percentage of patients with ALBI grade 1 decreased from 29.3% to 11.3%. These results are consistent with a retrospective study of patients in Taiwan in which the ALBI grade worsened in 54.1% of patients at the end of sorafenib therapy [32]. A more recent study conducted in Japan also reported significant ALBI score worsening from baseline to the end of sorafenib treatment (mean score − 2.42 vs − 2.02, p < 0.01), resulting in many patients being ineligible for second-line regorafenib [33]. Furthermore, a baseline ALBI score < − 2.53 (which roughly corresponds to ALBI grade 1/2a) was a significant predictor of regorafenib treatment initiation (p < 0.001) [33]. Deterioration of liver function during first-line lenvatinib treatment has also been reported [34]. However, these studies were not placebo controlled and thus a decline in liver function due to disease progression cannot be excluded. Our study also found that the ALBI grade was less likely to worsen during index line treatment in patients treated at designated cancer hospitals (Table 4), which may indicate the importance of consolidating care for patients with advanced HCC to experienced specialist hospitals.
The use of an administrative database covering approximately 22% of DPC hospitals in Japan allowed us to analyze a large number of patients with HCC being treated in real-world clinical practice, including from non-academic hospitals that are not usually involved in clinical research. The database also allowed us to understand changes in treatment sequences on a large scale, before and after post-sorafenib treatment options became available. The ability to assess liver function using only laboratory values is one of the advantages of the ALBI score compared with the Child–Pugh score, making it possible for us to evaluate liver function using the MDV database, in which clinical information necessary for the Child–Pugh score (presence and severity of ascites, hepatic encephalopathy) is not available. However, in the MDV database, laboratory test results were only available from hospitals that agreed to the use of test results for secondary research purposes. This limitation meant that baseline ALBI results were available for less than 10% of patients in each cohort, leading to smaller sample sizes for some analyses. Although this may have led to some selection bias in the analyzed population, we did not find any notable differences in available baseline characteristics between the full cohorts and the populations with baseline ALBI results. Another limitation is that only available variables were included in the regression models; therefore, confounding by unmeasured variables (e.g., performance status, tumor size, number of tumors, portal vein invasion) could not be excluded. Additional limitations of the MDV database include: (1) patients from smaller hospitals and clinics that have not adopted the DPC system are not included; (2) patients cannot be tracked beyond a single hospital; therefore, treatments outside that hospital cannot be captured, and patients who attend more than one hospital in the MDV database may be counted twice; and (3) certain information is not available, including reasons for treatment discontinuation (e.g., adverse events, tumor progression, liver dysfunction, death), tumor-related factors (e.g., tumor grade), deaths occurring outside of hospitalization, information on participation in outpatient-only clinical trials (information is available only when the trial requires hospitalization), and therapy line (therefore, index line treatment was assumed to be first-line treatment). In addition, some clinical information, such as body mass index and cancer stage, was available only from hospitalization discharge summaries and was therefore limited to patients who were hospitalized. Finally, although the transition rate to the subsequent line therapy in the lenvatinib cohort was low (Table 2), this may be biased by the shorter timeframe of lenvatinib availability (approximately 15 months from approval in March 2018 to the end of June 2019) compared with the sorafenib cohorts (approximately 24 months), resulting in a larger fraction of the lenvatinib cohort (approximately 50%) being excluded from the transition analysis, many of whom are likely to still be on index line treatment.
5 Conclusions
The results of this study using an administrative claims database suggest that better liver function reserve, as reflected by the ALBI score, at both the start and end of index line treatment is associated with successful sequential therapy in real-world clinical practice in Japan. Furthermore, despite the recent introduction of alternative systemic therapies, sequential treatment is not successfully implemented for many patients in real-world clinical practice in Japan. Because deterioration of liver function has a negative impact on sequential therapy, which in turn can adversely affect survival and quality of life, physicians should implement strategies to start systemic therapy while the patient still has good liver function and to maintain liver function as much as possible during systemic therapy.
References
Mak L-Y, Cruz-Ramón V, Chinchilla-López P, Torres HA, LoConte NK, Rice JP, Foxhall LE, et al. Global epidemiology, prevention, and management of hepatocellular carcinoma. Am Soc Clin Oncol Educ Book. 2018;38:262–79.
Yang JD, Hainaut P, Gores GJ, Amadou A, Plymoth A, Roberts LR. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol. 2019;16(10):589–604.
Kokudo N, Takemura N, Hasegawa K, Takayama T, Kubo S, Shimada M, Nagano H, et al. Clinical practice guidelines for hepatocellular carcinoma: the Japan Society of Hepatology 2017 (4th JSH-HCC guidelines) 2019 update. Hepatol Res. 2019;49(10):1109–13.
Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg. 1973;60(8):646–9.
Johnson PJ, Berhane S, Kagebayashi C, Satomura S, Teng M, Reeves HL, O’Beirne J, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-the ALBI grade. J Clin Oncol. 2015;33(6):550–8.
Hiraoka A, Kumada T, Michitaka K, Kudo M. Newly proposed ALBI grade and ALBI-T score as tools for assessment of hepatic function and prognosis in hepatocellular carcinoma patients. Liver Cancer. 2019;8(5):312–25.
Nakamura M. Utilization of MDV data and data quality control [in Japanese]. Jpn J Pharmacoepidemiol. 2016;21(1):23–5.
Pharmacoepidemiology & Database Taskforce, Japanese Society for Pharmacoepidemiology. Survey of Japanese databases in Japan available for clinical/pharmacoepidemiology. 2019. http://www.jspe.jp/committee/020/0210/. Accessed 14 Sep 2020.
Yamaguchi M, Inomata S, Harada S, Matsuzaki Y, Kawaguchi M, Ujibe M, Kishiba M, et al. Establishment of the MID-NET® medical information database network as a reliable and valuable database for drug safety assessments in Japan. Pharmacoepidemiol Drug Saf. 2019;28(10):1395–404.
Toyoda H, Lai PB, O’Beirne J, Chong CC, Berhane S, Reeves H, Manas D, et al. Long-term impact of liver function on curative therapy for hepatocellular carcinoma: application of the ALBI grade. Br J Cancer. 2016;114(7):744–50.
Ueshima K, Nishida N, Hagiwara S, Aoki T, Minami T, Chishina H, Takita M, et al. Impact of baseline ALBI grade on the outcomes of hepatocellular carcinoma patients treated with lenvatinib: a multicenter study. Cancers (Basel). 2019;11(7):E952.
Wang YY, Zhong JH, Su ZY, Huang JF, Lu SD, Xiang BD, Ma L, et al. Albumin-bilirubin versus Child-Pugh score as a predictor of outcome after liver resection for hepatocellular carcinoma. Br J Surg. 2016;103(6):725–34.
Hiraoka A, Kumada T, Atsukawa M, Hirooka M, Tsuji K, Ishikawa T, Takaguchi K, et al. Prognostic factor of lenvatinib for unresectable hepatocellular carcinoma in real-world conditions-multicenter analysis. Cancer Med. 2019;8(8):3719–28.
Hiraoka A, Kumada T, Atsukawa M, Hirooka M, Tsuji K, Ishikawa T, Takaguchi K, et al. Important clinical factors in sequential therapy including lenvatinib against unresectable hepatocellular carcinoma. Oncology. 2019;97(5):277–85.
Hiraoka A, Kumada T, Fukunishi S, Atsukawa M, Hirooka M, Tsuji K, Ishikawa T, et al. Post-progression treatment eligibility of unresectable hepatocellular carcinoma patients treated with lenvatinib. Liver Cancer. 2020;9(1):73–83.
Ogasawara S, Chiba T, Ooka Y, Suzuki E, Kanogawa N, Saito T, Motoyama T, et al. Liver function assessment according to the Albumin-Bilirubin (ALBI) grade in sorafenib-treated patients with advanced hepatocellular carcinoma. Investig New Drugs. 2015;33(6):1257–62.
Matsuda S, Fujimori K, Fushimi K. Development of casemix based evaluation system in Japan. Asian Pac J Dis Manag. 2010;4(3):55–66.
Yasunaga H, Matsui H, Horiguchi H, Fushimi K, Matsuda S. Clinical epidemiology and health services research using the Diagnosis Procedure Combination database in Japan. Asian Pac J Dis Manag. 2015;7(1–2):19–24.
Sterling RK, Lissen E, Clumeck N, Sola R, Correa MC, Montaner J, Sulkowski MS, et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology. 2006;43(6):1317–25.
Sumida Y, Yoneda M, Hyogo H, Itoh Y, Ono M, Fujii H, Eguchi Y, et al. Validation of the FIB4 index in a Japanese nonalcoholic fatty liver disease population. BMC Gastroenterol. 2012;12(1):2.
Badawy A, Seo S, Toda R, Fuji H, Fukumitsu K, Taura K, Kaido T, et al. Different clinical risk scores for prediction of early mortality after liver resection for hepatocellular carcinoma: which is the best? ANZ J Surg. 2019;89(10):1275–80.
Hiraoka A, Michitaka K, Kumada T, Izumi N, Kadoya M, Kokudo N, Kubo S, et al. Validation and potential of albumin-bilirubin grade and prognostication in a nationwide survey of 46,681 hepatocellular carcinoma patients in Japan: the need for a more detailed evaluation of hepatic function. Liver Cancer. 2017;6(4):325–36.
Marrero JA, Kudo M, Venook AP, Ye SL, Bronowicki JP, Chen XP, Dagher L, et al. Observational registry of sorafenib use in clinical practice across Child-Pugh subgroups: the GIDEON study. J Hepatol. 2016;65(6):1140–7.
Kudo M, Ikeda M, Takayama T, Numata K, Izumi N, Furuse J, Okusaka T, et al. Safety and efficacy of sorafenib in Japanese patients with hepatocellular carcinoma in clinical practice: a subgroup analysis of GIDEON. J Gastroenterol. 2016;51(12):1150–60.
Liu PH, Hsu CY, Hsia CY, Lee YH, Chiou YY, Huang YH, Lee FY, et al. ALBI and PALBI grade predict survival for HCC across treatment modalities and BCLC stages in the MELD era. J Gastroenterol Hepatol. 2017;32(4):879–86.
Pinato DJ, Sharma R, Allara E, Yen C, Arizumi T, Kubota K, Bettinger D, et al. The ALBI grade provides objective hepatic reserve estimation across each BCLC stage of hepatocellular carcinoma. J Hepatol. 2017;66(2):338–46.
Lee P-C, Chao Y, Chen M-H, Lan K-H, Lee C-J, Lee I-C, Chen S-C, et al. Predictors of response and survival in immune checkpoint inhibitor-treated unresectable hepatocellular carcinoma. Cancers. 2020;12(1):182.
Pinato DJ, Kaneko T, Saeed A, Pressiani T, Kaseb A, Wang Y, Szafron D, et al. Immunotherapy in hepatocellular cancer patients with mild to severe liver dysfunction: adjunctive role of the ALBI grade. Cancers. 2020;12(7):1862.
Kuzuya T, Ishigami M, Ito T, Ishizu Y, Honda T, Ishikawa T, Hirooka Y, et al. Clinical characteristics and outcomes of candidates for second-line therapy, including regorafenib and ramucirumab, for advanced hepatocellular carcinoma after sorafenib treatment. Hepatol Res. 2019;49(9):1054–65.
Kudo M, Finn RS, Qin S, Han KH, Ikeda K, Piscaglia F, Baron A, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–73.
Pinato DJ, Yen C, Bettinger D, Ramaswami R, Arizumi T, Ward C, Pirisi M, et al. The albumin-bilirubin grade improves hepatic reserve estimation post-sorafenib failure: implications for drug development. Aliment Pharmacol Ther. 2017;45(5):714–22.
Kuo YH, Wang JH, Hung CH, Rau KM, Wu IP, Chen CH, Kee KM, et al. Albumin-bilirubin grade predicts prognosis of HCC patients with sorafenib use. J Gastroenterol Hepatol. 2017;32(12):1975–81.
Yukimoto A, Hirooka M, Hiraoka A, Michitaka K, Ochi H, Joko K, Imai Y, et al. Using ALBI score at the start of sorafenib treatment to predict regorafenib treatment candidates in patients with hepatocellular carcinoma. Jpn J Clin Oncol. 2019;49(1):42–7.
Hiraoka A, Kumada T, Atsukawa M, Hirooka M, Tsuji K, Ishikawa T, Takaguchi K, et al. Early relative change in hepatic function with lenvatinib for unresectable hepatocellular carcinoma. Oncology. 2019;97(6):334–40.
Acknowledgements
Medical writing assistance was provided by Rebecca Lew, Ph.D., CMPP, and Serina Stretton, PhD, CMPP, of ProScribe—Envision Pharma Group, and was funded by Eli Lilly Japan K.K. ProScribe’s services complied with international guidelines for Good Publication Practice (GPP3).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was sponsored by Eli Lilly Japan K.K., manufacturer/licensee of ramucirumab, which was involved in the study design, data collection, data analysis, and preparation of the manuscript. The publication charges were paid for by Eli Lilly Japan K.K.
Conflicts of interest
AH has received speaker fees from Eisai, Bayer, and Otsuka. YT, Y-JH, ZC, and SS are employees and/or minor shareholders of Eli Lilly Japan K.K.
Ethics approval
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and Good Pharmacoepidemiology Practices. This observational study analyzed de-identified data from an administrative claims database; therefore, the study was exempt from ethical review and informed consent was not required.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Code availability
Not applicable.
Authors’ contributions
All authors participated in the interpretation of study results, and in the drafting, critical revision, and approval of the final version of the manuscript. YT and ZC conducted the statistical analysis.
Availability of data and material
The data in this study are commercially available from Medical Data Vision Co., Ltd and were used under licence. As restrictions apply to the availability of these data, they are not publicly available. Data can be made available from Medical Data Vision Co., Ltd upon request.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Hiraoka, A., Tanizawa, Y., Huang, YJ. et al. Association of Albumin-Bilirubin Grade and Sequential Treatment with Standard Systemic Therapies for Advanced Hepatocellular Carcinoma: A Retrospective Cohort Study Using a Japanese Administrative Database. Drugs - Real World Outcomes 8, 301–314 (2021). https://doi.org/10.1007/s40801-021-00245-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40801-021-00245-8