
Abstract
Background
The available evidence regarding the clinical characteristics, treatment patterns, adverse events (AEs), and costs of treating patients with stage IV non-small cell lung cancer (NSCLC) in Mexico is scarce.
Objective
Our objective was to describe the clinical characteristics, treatment patterns, and direct costs associated with Mexican patients diagnosed with stage IV NSCLC who had completed two or more lines of systemic antineoplastic treatment.
Methods
A multicenter retrospective cohort study was designed to collect data from the medical records of patients treated at tertiary-level public hospitals in Mexico (multicenter chart review). We calculated costs from the viewpoint of payers based on data regarding therapy and service utilization.
Results
A total of 115 patients were included. Median patient age was 61 years (interquartile range [IQR] 52.4–68.5), and 51.3% were female. The most common NSCLC type was non-squamous (92.2%), and the typical histology was adenocarcinoma (88.7%). All patients received first- and second-line therapy: 54.78% completed a third-line, 27.82% a fourth-line, 7.82% a fifth-line, 2.6% a sixth-line, and 1.7% a seventh-line active therapy. Carboplatin was the most frequently used therapy (28.6%) followed by docetaxel (23.3%), nivolumab (16.7%), and irinotecan (13.3%). AEs occurred in 53% of the patients and none was fatal. In total, 59 patients (51.3%) required hospitalization during the observation period. The median cost per patient was $US7039.40, with a minimum of $US628.30 and a maximum of $US3,557,364.20. Median overall survival of the cohort was 12 months (95% confidence interval 9.8–14.1).
Conclusions
In Mexico, NSCLC is usually diagnosed at stage IV. This study shows considerable variation in chemotherapy regimens, leading to a wide range in treatment cost. The understanding of NSCLC treatment patterns in Mexico will help to identify and address unmet needs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Lung cancer remains the leading cause of cancer death globally in both high-income and low- and middle-income countries, accounting for 1.6 million cancer deaths annually (approximately 20% of total cancer deaths), with an estimated 1.8 million new cases annually worldwide [1]. According to GLOBOCAN, in 2012 in Mexico, the highest incidence and mortality rates of lung cancer were for males (10.5 and 9.5 in 100,000; respectively), whereas for females the incidence rate was 4.9 and the mortality rate 4.3 in 100,000 [2]. Lung cancer was the third leading cause of death in men in 2012, with 4152 deaths [3]. Cigarette smoking or tobacco use continues to be the most important causal risk factor for development of lung cancer [4].
The two broad histological subtypes of lung cancer are small-cell lung cancer (SCLC), which is the cause of 15% of cases, and non-small cell lung cancer (NSCLC), which accounts for 85% of cases. NSCLC includes adenocarcinoma, squamous-cell carcinoma, and large-cell carcinoma [5]. The frequency of epidermal growth factor receptor (EGFR) mutations in NSCLC varies between different geographic regions, with a reported prevalence of 34.3% in Mexico [6].
Several clinical studies have determined the importance of systemic treatment in patients with metastatic lung cancer. The best evidence comes from two meta-analyses, which determined that palliative chemotherapy is justified in patients with advanced NSCLC, since it significantly increases survival, improves symptoms, and does not diminish quality of life [7, 8]. Before starting treatment in patients with a recent diagnosis of advanced NSCLC, EGFR mutation should be determined. Patients with adenocarcinoma and EGFR mutation should be treated with gefitinib, erlotinib, or afatinib in the front line instead of chemotherapy [9]. Osimertinib has also been shown to be an option in the first-line treatment of these type of disease [10]. In patients without EGFR mutation and with a good functional status, treatment with first-line chemotherapy should be a combination of two drugs; for patients with poor functional status, monotherapy is a treatment option [9]. According to the national consensus of diagnosis and treatment of NSCLC, several platinum-based treatment schemes are available for advanced NSCLC. The type of treatment must be individualized according to the comorbidities of each patient and the toxicity profile of each scheme. Combined treatment with bevacizumab and carboplatin + paclitaxel is appropriate in patients without contraindications, as is treatment with cetuximab in combination with cisplatin + vinorelbine. The second-line recommended therapeutic agents in patients with advanced NSCLC are docetaxel, pemetrexed, erlotinib, and gefitinib [9].
Despite the generally poor prognosis, there is substantial international variation in recently published 5-year relative survival estimates [4]. The low survival rate of patients with lung cancer is related to the stage of cancer at diagnosis. Lung cancer symptoms are nonspecific in nature, so most lung cancers are typically diagnosed after they have advanced (57% of lung cancers in the USA are detected with metastases), leading to a 5-year relative survival of 4.5% [11].
It is not only the human cost that one needs to consider but also the wider economic burden. A recent analysis of the costs associated with cancer care in the EU demonstrated that, relative to other cancers, lung cancer is associated with the highest economic costs (15% of total cancer care costs) [12]. The challenge becomes even greater in scenarios with inadequate funding, unequal distribution of resources and services, and/or increased need for investment in middle- and low-income countries such as Mexico. Knowledge regarding the cost of treatment and its determinants is crucial if better clinical decisions are to be made. The objectives of this study were to describe the clinical characteristics, treatment patterns, and direct costs associated with Mexican patients diagnosed with stage IV NSCLC. Overall survival was evaluated as an exploratory objective.
2 Methods
A multicenter retrospective cohort study was designed to collect data regarding patient characteristics, treatment patterns, and resource utilization from the medical records of patients treated at tertiary-level public hospitals in Mexico (multicenter chart review).
Patients aged > 18 years whose disease had progressed from a previous stage and patients newly diagnosed with stage IV disease on or after 1 January 2013 (the last diagnosis included was 10 August 2016) who had completed two or more lines of systemic antineoplastic treatment (each line including chemotherapy, targeted therapy, and/or immunotherapy) and were currently receiving palliative therapy, a better supportive treatment, or had died were included in the study. We excluded patients who had participated in a clinical trial related to NSCLC treatment based on its diagnosis and/or with a concurrent diagnosis of another malignant neoplasm (except for non-melanoma skin cancer).
2.1 Data Collection
Data were captured using a paper case report form (CRF) that had been validated by the principal investigators against patient files. The CRFs were monitored for completeness and accuracy by a third-party monitor and transferred to an electronic database. Variables collected included patient demographics and clinical characteristics, treatment received, adverse events (AEs), hospitalization and outpatient visits, and resource utilization. The medical records were reviewed in alphabetical order, and all patients who met the inclusion criteria at the participating hospitals were included.
Ethics approval was obtained from each of the participating hospitals, and data capture respected local and international patient privacy regulations. Patient consent was not required as the study was a retrospective, observational patient chart review.
2.2 Statistical Methods
Descriptive statistical analysis of each of the clinical variables and treatments was performed. Proportions for categorical variables and medians for continuous variables were reported, along with the 25–75% interquartile range (IQR).
For the final objective of the study, we calculated the estimated costs associated with cancer treatment based on data for therapy and service utilization. Cost estimation implied the identification and measurement of resources used and the valuation thereof.
Unit costs were collected on a spreadsheet specifically developed for this project. These costs were taken from the Jalisco Cancer Institute’s (IJC) and the National Institute of Respiratory Diseases’ (INER) unit costs lists for procedures and from the IJC’s list of medicine acquisition costs. We calculated costs from the viewpoint of payers based on data regarding therapy and service utilization. We analyzed the total cost of treatment throughout the entire observation period from the date of each patient’s hospital screening.
Only direct costs were included in the analysis: drugs, consultations, infusion administration protocols, services rendered and procedures performed, laboratory tests, imaging tests, blood transfusions, and hospitalization. Transportation and food costs were not considered, nor were indirect costs such as productivity loss due to disability or premature death.
All estimated costs were in 2017 Mexican pesos (MXN) and then converted to $US, year 2017 values. The exchange rate was MXN18 per $US1, calculated as the average exchange rate of 2017 according to the database of the Bank of Mexico (1 January to 31 December) [13].
Survival curves for overall survival (OS) were plotted using the Kaplan–Meier method. Medians and the associated 95% confidence intervals (CIs) were computed.
Analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
3 Results
The original chart review included information on 118 patients. We removed three patients who did not meet the selection criteria. The final sample size analyzed was 115 patients from three tertiary-level public hospitals (see patient flow chart, Fig. 1).

Selection of patients included in the study. IJC Jalisco Cancer Institute, INER National Institute of Respiratory Diseases, ISSEMYM Social Security Institute of the State of Mexico and Municipalities
Most of the patients were treated at the INER (n = 94; 81.7%), followed by the Social Security Institute of the State of Mexico and Municipalities (ISSEMYM) (n = 16; 13.9%), and the IJC (n = 5; 4.4%).
3.1 Demographic and Clinical Characteristics
The median age was 61.0 years (IQR 52.4–68.5), and 51.3% were female. The median weight at diagnosis was 63 kg (IQR 53.5–73). The maximum level of education reported was generally low: no schooling 10.4%; primary school (age 6–12 years) 30.4%; secondary school (age 12–14 years) 13.0%; high school 11.3%; university 8.7%; other 25.2%; unknown 0.9%. Most patients (60.9%) reported comorbidities. Of these, 38.6% reported diabetes mellitus, 7.1% obesity, and 50% cardiovascular diseases. All other comorbidities impacted < 5% of the sample.
The most common type of NSCLC was non-squamous (92.2%), and the most typical histology was adenocarcinoma (88.7%). Almost all patients were stage IV (97.4%) at first diagnosis. Half of the population had a history of smoking (49.6%), 43.48% had positive wood smoke exposure, and almost all had a negative family history of NSCLC (97.4%) (Table 1).
Almost all patients had metastases at the time of diagnosis (99.1%). The sites of metastasis location were lung (54 patients; 47.4%), followed by bone (36; 31.6%), brain (11; 9.7%), and distant lymph nodes (eight; 7%).
EGFR mutation was tested in only 85 (73.9%) patients, 31 (36.5%) of which were positive. Anaplastic lymphoma kinase (ALK) translocation was tested in 13 (11.3%) patients, two (15.4%) of which were positive. Patients had a median waiting time of 24 days (IQR 15.0–35.0) from diagnosis to first-line treatment.
3.2 Treatment Patterns
All patients received first- and second-line therapy (in accordance with the selection criteria), and 54.8% completed a third-line, 27.8% a fourth-line, 7.8% a fifth-line, 2.6% a sixth-line, and 1.7% a seventh-line active therapy (Table 2).
Only 32.2% of the patients received radiotherapy after diagnosis of NSCLC.
Within the 13 regimens observed in the first line of treatment, the carboplatin–paclitaxel combination was administered in 65.2% of the observed population. Ten different therapeutic agents were identified, and most patients were initially treated with platinum-based chemotherapy (87.8%) and paclitaxel (67.8%). Most of the first-line treatments (93.6%) were administered on an outpatient basis. Three patients (2.6%) achieved complete response (CR), 46 (40%) had partial response (PR), 24 (20.9%) had stable disease (SD), and the rest experienced progression or died.
Among the 13 therapeutic agents administered within the different second-line regimens, four were administered to > 15% of the patients, either as monotherapy or combined: docetaxel to 47.0%, carboplatin to 25.2%, paclitaxel to 15.7%, and nintedanib to 15.7%. Nivolumab was administered to 8.7% of the patients. A large proportion of the second-line treatments (80.4%) were administered on an outpatient basis. Two patients (1.7%) achieved CR, 27 (23.5%) had a PR, 35 (30.4%) had SD, and the rest (44%) experienced progression or died.
Only 63 (55%) patients completed third-line therapy, where carboplatin was the most frequently used drug (28.6%), followed by paclitaxel (25.4%), nivolumab (20.6%), and docetaxel (17.5%). No patient achieved CR, seven patients (11.1%) had a PR, 17 (27%) had SD, and the rest 39 (80%) showed progression or died.
In total, 30 (26%) patients received fourth-line therapy. The most frequently used therapy was docetaxel (23.3%), followed by nivolumab (16.7%) and irinotecan (13.3%). Only two (6.67%) patients achieved PR, and 20 SD (8%).
Nine (8%) patients received fifth-line therapy, three (3%) received sixth-line, and only two patients (2%) received seventh-line treatment.
In total, 59 patients (51.3%) required hospitalization during the observation period; there were 118 hospitalizations/medical emergencies in the patient population, and most of them were hospitalized more than once (76.3%), with an average length of stay of 69 days. Supportive care was most often associated with pain treatment (see Table 3 for details).
AEs occurred in 53.0% of the patients; none was fatal. Among these patients, 22 (19.1%) experienced fatigue, 12 (10.4%) diarrhea, 12 (10.4%) neuropathy, eight (6.7%) neutropenia, seven (6.1%) thrombocytopenia, and < 5% experienced other AEs.
3.3 Resource Utilization
The median cost per patient was $US7039.40, with a minimum of $US628.30 and a maximum of $US3,557,364.20. Estimated therapy costs per patient, per line, and per month are shown in Table 4.
3.4 Overall Survival
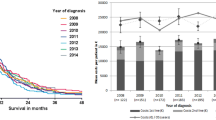
Median OS for the overall cohort (n = 115) was 12 months (95% CI 9.8–14.1). The Kaplan–Meier plot for patient OS is shown in Fig. 2.

Overall survival for all patients in the cohort
4 Discussion
Despite a doubling of the volume of lung cancer research worldwide between 2004 and 2013, it still only accounts for a small proportion (5.6%) of the overall oncology research publication output [14]. Currently, information on patients diagnosed with stage IV NSCLC in Mexico is limited; this study was designed to help us better understand patient characteristics, real-world treatment patterns, and healthcare resource use.
The patient population of Mexico follows international tendencies for advanced-stage diagnosis, with most patients diagnosed with stage IV, 99.1% according to our study. Systemic therapies are predominantly used in the management of stage IV disease, with only 32.2% of the patients receiving radiotherapy, almost always with palliative purpose. The findings of this study show a wide variety of regimens used, with a tendency to follow international guidelines for the time frame observed using platinum-based therapies as first-line treatment [15]. These results are similar to those observed in the study conducted by Nadler et al. [16], in which 71% of the observed population was initially treated with platinum-based chemotherapy, and to those observed in other smaller published real-world utilization studies of similar time frames reporting ranges from 61 to 85% utilization of platinum-based chemotherapy as first line-treatment [17, 18]. However, within the scenario of second-line treatment, the use of docetaxel in our study was much higher than that observed in the aforementioned studies, being used in 47% of our patients versus the observed range of 14–16% [16, 17].
Immunotherapy is already an important part of the treatment modalities in Mexico, with an increase in its use from the second line of treatment. This is in accordance with international trends, even for patients with advanced disease, building on progress in the understanding of antitumor immune responses [19].
Although a lack of biomarker testing may be observed, probably due to its cost and the need for tumor tissue to perform these tests, the numbers for EGFR status were much higher than those recorded in other observational studies. EGFR mutation was tested in 73.9% of our population and was positive in 36.5% of these patients; ALK translocation was tested in 11.3% and was positive in 15.4%. In the study by Nadler et al. [16] in the USA, EGFR and ALK status was available in approximately 40% and 35% of the patients, respectively. Among those with documented results, EGFR and ALK status was positive in 13% and 3% of the patients, respectively [16]. In another study that evaluated the frequency and clinical characteristics of ALK rearrangements in Latin America, Arrieta et al. [20] reported that ALK translocation was positive in 7.6% (79/1034) of the Mexican patients included. Although these numbers vary greatly from those in our study, it has been stated previously that the frequency of EGFR mutations and ALK translocations varies geographically. Higher frequencies of EGFR mutations are found in Asia, as shown by Shi et al. [21] (51.4%), which represents several regions in that continent. In Latin America, intermediate frequencies (26.0%) are found in Argentina, Colombia, Mexico, Peru, Panama, and Costa Rica [6].
An increase in biomarker testing could resolve an area of opportunity by identifying subsets of patients who would benefit from targeted molecular therapies. For example, a large consortium study showed that patients with oncogenic drivers treated with targeted therapies had improved survival over those who did not (median survival 3.5 vs. 2.4 years; hazard ratio 0.69; 95% CI 0.53–0.9; P = 0.006) [22]. Nadler et al. [16] also observed that patients with actionable mutations derived greater survival benefit from targeted therapies: 24.3 months in patients who received first-line targeted therapy versus 11.7 months for chemotherapy. As stated by Arrieta et al. [23], following diagnosis, Mexican patients should be genotyped to identify predisposing mutations and receive personalized treatment.
A retrospective chart review in Italy found that costs associated with second-line therapy for stage IV NSCLC appeared to be greater than those for first-line therapy, regardless of histological subtype [24]. In our study, the median cost per patient in first- and second-line therapy was very similar ($US869.30 and 834.30, respectively), but the median estimated cost per patient increased significantly for patients who received sixth- and seventh-line treatment.
The cost estimates demonstrated that most costs were related to the use of chemotherapy/targeted therapy and/or immunotherapy agents and not to the use of other health resources. This is similar to what was observed in a retrospective chart review conducted in several European countries (Germany, Spain, France, and the UK), in which the cost of chemotherapy contributed to a high cost burden compared with other resources in the UK, Spain, and Germany [25]. Without further investigation, we can only hypothesize that the high costs of medical therapies probably reflect the incorporation of increasingly expensive new drugs.
It should be noted that, due to the high probability that patients diagnosed with stage IV NSCLC will be unable to complete an active line of treatment, only patients who had completed a second line of treatment were included in the study, to ensure a sample size that could adequately show treatment patterns in the second line. One study reported that only 24% of patients with NSCLC received first-line chemotherapy [26]. This means that the percentages of patients in this study who completed further treatment lines probably do not reflect the behavior of the entire population diagnosed with stage IV NSCLC.
Our data show an expected median OS of 12.0 months. This is similar to that reported in a retrospective cohort analysis of patients with NSCLC screened for EGFR mutations between October 2009 and July 2013, in which the median survival of the global population was 12.0 months, with a better OS in mutated than in nonmutated patients (20.0 vs. 11.0 months, respectively; P = 0.007) [27]. However, the populations of both studies are not comparable, since our population was preselected to have completed two lines of active treatment.
Data collected from the medical records represent actual treatment information documented as part of routine medical care and therefore show real-world clinical treatment patterns. The limitations of this study include the retrospective nature of the evaluation and that the data were obtained from only three major public hospitals, so they may not be representative of treatment patterns at the national level. The lack of homogeneity in the data of the medical records is another limiting factor. Missing data cannot confirm the absence of a condition or value in the patients’ medical histories, only that it was not documented. As 82.6% of the patients died within the study observation period, cost underestimation for the remaining 17.4% is likely. The observation period for the study started in 2013; therefore, the data presented may not reflect current treatment patterns in Mexico.
Future investigations should look to increase the study size to allow stratified analyses and include additional public institutes of interest to calculate more universally applicable results. Because many of the clinical files were still in paper format, collecting the information was a resource-intensive task. Retrospective chart reviews in Mexico would benefit from the use of more standardized electronical medical records among the different institutions.
5 Conclusion
To the best of our knowledge, this is the first study to look at patient management and resource utilization for patients with stage IV NSCLC in Mexico, with results showing considerable variation in active treatment regimens. Understanding NSCLC treatment patterns and costs in Mexico will help measure the impact of innovations in treatment practice and create opportunities to harmonize treatment options.
References
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–86. https://doi.org/10.1002/ijc.29210.
Ferlay J, Soerjomataram I, Ervik M, et a. GLOBOCAN 2012 v1.0. Cancer incidence and mortality worldwide. IARC CancerBase No. 11. http://globocan.iarc.fr/Pages/fact_sheets_population.aspx. Accessed 10 Mar 2018.
INEGI. Mortality, 2012. http://www.inegi.org.mx/est/contenidos/proyectos/registros/vitales/mortalidad/tabulados/PC.asp?t=14&c=11817. Accessed 2 Mar 2018.
Cheng TY, Cramb SM, Baade PD, Youlden DR, Nwogu C, Reid ME. The international epidemiology of lung cancer: latest trends, disparities, and tumor characteristics. J Thorac Oncol. 2016;11(10):1653–71. https://doi.org/10.1016/j.jtho.2016.05.021.
Sher T, Dy GK, Adjei AA. Small cell lung cancer. Mayo Clin Proc. 2008;83(3):355–67. https://doi.org/10.4065/83.3.355.
Arrieta O, Cardona AF, Martin C, Mas-Lopez L, Corrales-Rodriguez L, Bramuglia G, et al. Updated frequency of EGFR and KRAS mutations in nonsmall-cell lung cancer in latin America: the Latin-American Consortium for the Investigation of Lung Cancer (CLICaP). J Thorac Oncol. 2015;10(5):838–43. https://doi.org/10.1097/JTO.0000000000000481.
Chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trials. Non-small Cell Lung Cancer Collaborative Group. BMJ (Clinical research ed). 1995;311(7010):899–909.
Group NM-AC. Chemotherapy in addition to supportive care improves survival in advanced non-small-cell lung cancer: a systematic review and meta-analysis of individual patient data from 16 randomized controlled trials. J Clin Oncol. 2008;26(28):4617–25. https://doi.org/10.1200/jco.2008.17.7162.
Arrieta O, Guzman-de Alba E, Alba-Lopez LF, Acosta-Espinoza A, Alatorre-Alexander J, Alexander-Meza JF, et al. National consensus of diagnosis and treatment of non-small cell lung cancer. Rev Invest Clin. 2013;65(Suppl 1):S5–84.
Soria J-C, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378(2):113–25. https://doi.org/10.1056/NEJMoa1713137.
National Cancer Institute. SEER stat fact sheets: lung and bronchus cancer. https://seer.cancer.gov/statfacts/html/lungb.html. Accessed 9 Mar 2018.
Luengo-Fernandez R, Leal J, Gray A, Sullivan R. Economic burden of cancer across the European Union: a population-based cost analysis. Lancet Oncol. 2013;14(12):1165–74. https://doi.org/10.1016/S1470-2045(13)70442-X.
Bank of Mexico. Exchange market. http://www.banxico.org.mx/portal-mercado-cambiario/index.html. Accessed 25 Feb 2018.
Aggarwal A, Lewison G, Idir S, Peters M, Aldige C, Boerckel W, et al. The state of lung cancer research: a global analysis. J Thorac Oncol. 2016;11(7):1040–50. https://doi.org/10.1016/j.jtho.2016.03.010.
National Comprehensive Cancer Network (NCCN). NCCN guidelines for non-small cell lung cancer version 4. 2014.
Nadler E, Espirito JL, Pavilack M, Boyd M, Vergara-Silva A, Fernandes A. Treatment patterns and clinical outcomes among metastatic non-small-cell lung cancer patients treated in the community practice setting. Clin Lung Cancer. 2018. https://doi.org/10.1016/j.cllc.2018.02.002.
McKay C, Burke T, Cao X, Abernethy AP, Carbone DP. Treatment patterns for advanced non-small-cell lung cancer after platinum-containing therapy in U.S. community oncology clinical practice. Clin Lung Cancer. 2016;17(5):449–60 e7. https://doi.org/10.1016/j.cllc.2016.03.008.
Abernethy AP, Arunachalam A, Burke T, McKay C, Cao X, Sorg R, et al. Real-world first-line treatment and overall survival in non-small cell lung cancer without known EGFR mutations or ALK rearrangements in US community oncology setting. PLoS One. 2017;12(6):e0178420. https://doi.org/10.1371/journal.pone.0178420.
Davies M. New modalities of cancer treatment for NSCLC: focus on immunotherapy. Cancer Manag Res. 2014;6:63–75. https://doi.org/10.2147/CMAR.S57550.
Arrieta O, Cardona AF, Bramuglia G, Cruz-Rico G, Corrales L, Martin C, et al. Molecular epidemiology of ALK rearrangements in advanced lung adenocarcinoma in latin America. Oncology. 2019;96(4):207–16. https://doi.org/10.1159/000493733.
Shi Y, Au JS, Thongprasert S, Srinivasan S, Tsai CM, Khoa MT, et al. A prospective, molecular epidemiology study of EGFR mutations in Asian patients with advanced non-small-cell lung cancer of adenocarcinoma histology (PIONEER). J Thorac Oncol. 2014;9(2):154–62. https://doi.org/10.1097/jto.0000000000000033.
Kris MG, Johnson BE, Berry LD, Kwiatkowski DJ, Iafrate AJ, Wistuba II, et al. Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA J Am Med Assoc. 2014;311(19):1998–2006. https://doi.org/10.1001/jama.2014.3741.
Arrieta O, Lopez-Mejia M, Macedo-Perez EO, Corona-Cruz JF. Proposals for the prevention of lung cancer in the health system of Mexico. Salud Publica Mex. 2016;58(2):274–8.
Degli Esposti L, Saragoni S, Brown J, Kiiskinen U, Blini V, Muschera S. Real world data analysis of treatment patterns and costs associated with non-small cell lung cancer (NSCLC) in Italy. ISPOR 22nd Annual International Meeting May, 2017; Boston, MA, USA.
Kurosky S, Lorenzo M, Cuyun Carter G, Parikh RC, Winfree K, Kaye JA. Health care resource utilization and costs of metastatic non-small cell lung cancer in select European countries. ISPOR 22nd Annual International Meeting May, 2017; Boston, MA, USA.
Sacher AG, Le LW, Lau A, Earle CC, Leighl NB. Real-world chemotherapy treatment patterns in metastatic non-small cell lung cancer: are patients undertreated? Cancer. 2015;121(15):2562–9. https://doi.org/10.1002/cncr.29386.
Aguiar F, Fernandes G, Queiroga H, Machado JC, Cirnes L, Souto Moura C, et al. Overall survival analysis and characterization of an EGFR mutated non-small cell lung cancer (NSCLC) population. Arch Bronconeumol. 2018;54(1):10–7. https://doi.org/10.1016/j.arbres.2017.07.012.
Author information
Authors and Affiliations
Contributions
JAA, SC, EDM made substantial contributions to conception and design of the study and to the acquisition of data, critically revised the manuscript for important intellectual content, and provided final approval of the version to be published. DN made substantial contributions to conception and design of the study and to the acquisition, analysis, and interpretation of data; critically revised the manuscript for important intellectual content; and provided final approval of the version to be published. AC made substantial contributions to conception and design of the study and to the analysis and interpretation of data, critically revised the manuscript for important intellectual content, and provided final approval of the version to be published. JMIC made substantial contributions to conception and design of the study and to the analysis and interpretation of data, drafted the manuscript, and provided final approval of the version to be published.
Corresponding author
Ethics declarations
Data availability
The data are not made available at this time as they are currently being analyzed for further publication.
Ethics approval
Ethics approval was obtained from the ethics committees at each of the participating institutes. This article does not contain any studies with animals performed by any of the authors.
Informed consent
Patient consent was not required as the study was a retrospective, observational patient chart review.
Consent for publication
The data capture respected international patient privacy regulations. Data that allowed for patient identification were not collected.
Funding
Funding for this study was provided by Eli Lilly and Company.
Conflict of interest
Jorge Arturo Alatorre has received professional fees for acting as a speaker and scientific advisor for Eli Lilly. Saúl Campos And Emmanuel De la Mora have no conflicts of interest that are directly relevant to the content of this article. Diego Novick and Angélica Cruz are employees of Eli Lilly and Company. Jimena María Iglesias-Chiesa has received professional fees to conduct this study for Eli Lilly and Company.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Alatorre, J.A., Campos-Gómez, S., De la Mora, E. et al. Treatment Patterns and Costs Associated with Stage IV Non-Small Cell Lung Cancer in a Mexican Population: A Chart Review. PharmacoEconomics Open 4, 381–388 (2020). https://doi.org/10.1007/s41669-019-00174-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41669-019-00174-x