
Abstract
Purpose
To monitor the progression of diseases such as Parkinson’s disease (PD) or essential tremor (ET), there is a growing interest in understanding their side effects and continuously monitoring the deterioration or progress of patients’ health conditions. The objective of this study was to investigate the feasibility of a wearable monitoring device constructed from compact MEMS for robust tremor detection in the upper limb using three different storage and monitoring techniques.
Method
Four subjects (2 PD and 2 ET) with varying stages of disease and treatment willingly provided offline, online, and live modes of tremor data using a low-cost, miniaturized accelerometer and microelectromechanical device.
Results
The results demonstrated differences in voluntary and non-voluntary characteristics of various activities and the distinct separation between them in the vibration spectrum at the limit of 2 Hz. Online and live monitoring provided the best alternatives to continuous in-home tracking combined with extensive post-processing techniques to detect tremor segments. The findings also highlighted the emergence of noticeable peaks, in the range between 3 and 8 Hz, for the PD’s frequency response, compared to the ET case, where the broadband behavior dominates.
Conclusion
The possibility of using a dynamic tuned mass damper tuned with dominant peaks to be canceled opens opportunities for PD passive tremor suppression.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Tremors are unintentional and uncontrollable rhythmic alternating agonist and antagonist muscle contractions leading to shaking movements in one or more body parts. The size, frequency, and course of tremors might change over time depending on the disease. Tremors can be sporadic or persistent and may occur independently or due to an underlying health problem and can be classified by their appearance and cause or origin [1]. Most of the 20 distinct tremors are either resting or activity tremors. The former occurs when muscles are relaxed; the latter when the muscles are active.
Essential tremors are characterized by involuntary, rhythmic shaking characterized by action tremors with or without purposeful movement. Even though many people connect tremors with Parkinson's disease, ETs are eight times more prevalent [2]. The tremor usually appears on both sides of the body but is often noticed more in the dominant hand because it is an action tremor. As ETs are action tremors, they can lead to problems with writing, drawing, drinking from a cup, or using tools or a computer. About 50% of cases of ET are caused by a genetic risk factor [3]. Although there is no cure for ET, therapies may help lessen the frequency and amplitude of tremors. Parkinsonian tremor is a common symptom of Parkinson’s disease, which causes shaking when the brain cells that govern movement are destroyed. As the illness develops, shaking may begin with one hand and move to another. Trembling may become more noticeable at times of stress or intense emotion. Parkinson's disease relates to various issues, including impaired balance, trouble swallowing, and a stooped posture. Parkinson's tremors occur primarily during rest (resting tremor). In most situations, they vanish during movement but reappear when the limb is at rest. More than 25% of people with Parkinson’s disease also have an associated action tremor [3].
Drug and surgical therapy can regulate the muscle and reduce tremors. However, serious side effects, such as severe nausea, vomiting, diarrhea, and painful or difficult urination, are usually encountered. Therefore, a non-invasive solution to tremor suppression has become increasingly important in research and literature [4]. The adoption of a wearable suppression devices such as tuned mass damper (TMD) can be used to alleviate tremor symptoms and help with performing daily tasks. Since it is a passive suppression technique, its unique proposition is done on a ‘case-by-case’ nature to ensure that the tremor type, amplitude, and frequency are correctly identified and tuned.
PD is a neurological condition marked by movement symptoms such as tremors, stiffness, and bradykinesia that vary throughout the day. The symptoms and disease progression are now well documented by doctors and assessed for research purposes via the MDS-UPDRS [5, 6]. Nevertheless, there are certain drawbacks to this. First, the symptoms and disease progression are evaluated infrequently, providing only a glimpse into the patient's condition, and potentially introducing adverse selection. Second, patients may present themselves in a more favorable light during clinical assessments than at home. To alleviate the previous drawbacks, we intend to develop a continuous monitoring data acquisition (DAQ) device that is lightweight, easy to use, low-cost, and efficient in the continuous reading of symptoms and disease progression [7, 8]. In addition, such a device can monitor the clinical signs more accurately during patients' everyday routines. It could also be used as an input signal for compatible technologies, such as active and passive vibration controllers or closed-loop deep brain stimulation [9].
To customize a wearable TMD device for patients, the first step of this multi-disciplinary project required designing and building a vibration data acquisition device to gather appropriate experimental measurements (i.e., frequency and severity) for characterizing, monitoring, and controlling involuntary hand vibrations [10, 11]. Because of technological advancements, inertial measurement units and other wearable sensors can detect tremors, resulting in compact, low-cost, power-efficient, and precise sensors [12,13,14]. A variety of wearable sensors can easily identify tremors [15, 16], gait freezing [17], bradykinesia [18], and dyskinesia [18]. Several monitoring systems have been designed and tested, with positive results [19,20,21]. However, these experiments examined specific motor activities in a lab or simulated home context, representing only a tiny portion of the actual patient’s life. Furthermore, these routine medical assessments sometimes cannot be carried out consistently in a real-life setting. Recently, Channa et al. [22] adopted a wearable bracelet and incorporated machine learning to differentiate between Parkinsonian tremor, dystonia tremor, and essential tremor by adopting features related to Unified Parkinson’s Disease Rating Scale (UPDRS).
The proposed device in this study uses microelectromechanical systems (MEMS) as an inertial measurement unit (IMU) to measure and report hand orientation through a combination of accelerometers and gyroscopes [23, 24]. MEMS combines mechanical and electrical components to create tiny integrated devices [25]. They blend micromachining technology with silicon-based microelectronics and can perceive, regulate, actuate, and create effects on the micro-scale. According to the MEMS research institute, they can improve people's lives for the better [26]. Bilski et al. [27] developed a real-time virtual spectrum analyzer to understand the procedures needed for developing equipment and software to provide the same functionality as complex devices. Additionally, Swiszcz et al. [28] carried out extensive work to create and develop a DAQ platform for monitoring wind turbine conditions with a maximum sampling frequency of 20 kHz. The data were stored in an Ethernet-based hard drive through the MySQL database. Zhang et al. [29] developed a vibration DAQ system for monitoring tools with a sampling frequency of 300 Hz. That system was connected to a PC interface through a USB cable. In addition, an 8-bit microcontroller was used to interrupt data with serial communications [30, 31]. Recently, Florin et al. [32] designed a DAQ system that used an analog to digital converter that reached 400-kilo samples per second and saved the data on a 16-Mb non-volatile static random-access memory. They also used the MySQL database for data storage but with a different communication protocol. Furthermore, Jamil et al. [33] proposed a new vibration and visualization DAQ system by implementing a MEMS accelerometer and a peripheral interface controller microcontroller that communicated with a PC. Experimental tests were performed on an electrical induction motor and a plastic stand. They proved the readings' stability and the system's reliability for a frequency range up to 5 kHz.
The remainder of the paper is structured as follows: The proposed monitoring system's technique is presented in Sect. 2. Section 3 shows the findings of PD and ET tremors. Finally, Sect. 4 discusses the results and concludes the paper.
Methodology
The main goal of the current work was to develop an innovative method of gathering motion data for hand tremors without any interaction between the patient and the analyst. This section explores different methods used in data acquisition and the development of a wearable tremor sensor. The calibration methodology and testing flowchart is shown in Fig. 1.

Methodology for development of wearable sensor device
Offline Monitoring Device
An offline monitoring device was constructed by connecting an Arduino, an inertial measurement unit, a micro-SD module, and a LiPo battery. Low-cost accelerometers, such as the MPU6050, offer excellent performance up to 80 Hz, providing exceptionally accurate readings with a maximum normalized root mean square error (NRMSE) of 1.8% in laboratory tests compared with professional piezoelectric accelerometers [34]. To process the input of this sensor, a microcontroller is required. The Arduino works well with a 3.3–9-V battery as a portable power source [34, 35]. However, we can extend the battery's life by appropriately altering the code. The Intel Galileo controller has an inbuilt Ethernet shield for Internet of Things (IoT) applications. Storing data requires the use of a micro-SD module. However, because of the acquisition speed constraint, there are losses in some of the signal peaks at higher frequencies (> 80 Hz) [34]. A DAQ with an offline storage circuit is shown in Fig. 2. This circuit was constructed with an Arduino Nano and mounted inside a suitable casing.

Circuit connection for offline monitoring data acquisition device with inertial measurement unit
Online and Live Monitoring Devices
To upgrade the DAQ system, a new online monitoring system was implemented. This system was used to measure tremor accelerations and send the data to an IoT platform. The received data were stored in a searchable database that could be accessed or downloaded whenever needed. The device was equipped with a six-axis accelerometer sensor and a Wi-Fi connection chip provided by the Arduino Nano 33 IoT chip. With an inertial measurement unit accelerometer and Wi-Fi connectivity on one low-power printed circuit board, the only action left was to configure it to communicate the values to the server. The final development step consisted of using LabView to create a code for direct serial monitoring appropriate for live clinical assessment. The same offline monitoring device was used, but the micro-SD module was disconnected because the data were not stored.
Experimental Results
Calibration
In an initial check of the frequency and amplitude reading accuracy, the accelerometer was mounted on a calibration shaker at a frequency of 159.2 Hz and a peak magnitude of 1.0 g [36]. The double-sided adhesive mounting tape was used to secure the accelerometer. The setup shown in Fig. 3 clearly shows how the system could read the shaking-induced vibration with an accuracy of 0.75% for the frequency and 5.8% for the amplitude; this frequency lies within the error margin specified by the manufacturer. However, the relatively large error in the amplitude reading was caused by the mounting condition of the accelerometer (adhesive tape). For example, a more convenient mounting (permanently with a stud) would improve reading accuracy.

Frequency response of handheld calibration shaker and MPU6050 sensor
Once calibrated, the wearable sensor and storage device were placed inside a wearable 3D-printed casing, as shown in Fig. 4. The case provided housing for the electronics and went through different prototypes toward an ergonomic shape. A control switch and locking mechanism for the case were added for convenience and security. Here, the tight-fitting tolerances ensured that the sensors with minimal damping could directly measure the transmissibility of frequency from the upper limb excitation through the housing structure.

Offline monitoring device; a Arduino Uno Prototype beside Casing; b Updated prototype in smaller form factor
Mounting Test
Once the reading accuracy had been confirmed, the system was ready to be attached to the patient’s hand for a final test of comfort and efficiency. To assess the convenience of several fastening solutions, the test subject was asked to wear the DAQ device and hold a vibrating bar activated by a DC motor. Of different fastening solutions, the most convenient one (which perfectly matches the geometry of the hand, minimizes the gap between the device and the wrist, and does not tighten excessively) was the one made of elastic bands.
Online and Live Monitoring Results
The goal of designing a continuous monitoring DAQ device is to correctly collect symptoms during patients' daily routines, without the need for intervention or supervision, so that data may be retrieved from afar. First, the data are stored in a RAM storage chip and transferred to the website. Even though the readings were taken at the desired frequency, the issue of transfer rate limitations remained, as this depends on the host’s location. The live monitoring device was tested with the same apparatus described previously, and a LabVIEW-based code allowed us to display the reading.
Tremor Evaluation in Parkinson’s and Other Disorders
The next step was to test the ability of the monitoring DAQ to detect and measure tremors in patients. Access to study population with a developed tremor symptom were limited to willing participants. Table 1 reports the tremor type and medication used for PD and ET patients that were currently being monitored and receiving medical treatment.
We concentrated on the specifics of each test as much as possible to obtain detailed data that would aid in determining the association between the patients’ medical information and tremor severity and frequency. Prototypes of the devices were tested by four volunteers experiencing different types of tremors. The prototype was tested by the authors beforehand on a vibrating apparatus as well to ensure good measurements when worn on the upper limb. Informed consent was obtained from the volunteers, and the research was carried out in line with appropriate ethical standards. These experiments were conducted in a busy medical clinic, so the recordings were taken for 10–20 s only because of time constraints. The DAQ was placed around each patient’s wrist so that all types of motion could be recorded, including voluntary and involuntary activities. During this short test, the volunteers wore the device while holding a cup full of water for 10–20 s and when their hands were at rest. The testing with the patients was the same as that used in the lab apparatus to ensure that calibration and measured data was not affected by extraneous factors.
The wearable device was first tested and calibrated using a shaker and then tested and verified on an accurate and well-instrumented test rig. An excellent matching between the readings of different devices was observed. Afterward, all the prototypes were tested on the authors’ hands to ensure their ergonomics, esthetics, and functionality. Our device was able to detect all the characteristic sampling frequency features in a short period. Table 1 summarizes all the medical data collected before the test. Due to the small demographic size and cases of tremors in Qatar, the authors assumed that the classification results could be performed with a relatively good accuracy that can be scaled to the rest of the population.
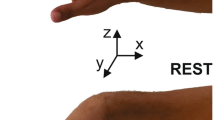
The sensor measured the frequency and amplitude of linear and angular accelerations along the three axes x, y, and z to generate six readings in total for each measurement (x is the longitudinal direction of the hand, and y is the transverse direction pointing outwards from the palm of the hand). According to the literature, Parkinsonism tremors have a frequency range of 3–8 Hz without pharmacological treatment. However, for ETs, the frequency fluctuates between 4 and 12 Hz. Having a 6-degree-of-freedom (DOF) sensor for the collected dataset ensures that all the contribution from translation and rotation motion were accounted for. While the results tested confirm the ‘pill-rolling’ motion associated with Parkinsonian tremors, the 6 channels are used to continue monitoring the progression of tremor response.
The DAQ was placed around each patient’s wrist to record all types of motion, including voluntary and involuntary activities. As per the investigation of Mann et al. [26] on a large sample of people, voluntary gestures corresponding to routine activities lay within 1–2 Hz. Thus, the different voluntary limb/wrist motions can be found in that zone of low frequency during everyday routines. In general, the tremors are characterized by being more frequent and having a smaller amplitude than voluntary movements. Therefore, the frequency spectrum may be considered an effective tool to differentiate between the various hand movement types in line with this concept. Numerous vibration readings were taken from patients with essential and Parkinsonism tremors under various conditions: during rest and while holding an object. Resting tremors were defined as involuntary motions when the limbs were not supported against gravity. For example, tremors were measured while the patient was sitting on a chair. Ideally, measurements should be taken without additional mental stress on patients or encouraging movement in other body parts, increasing the resting tremors’ amplitude [37].
Typical results for patients (1) and (4) are displayed in Figs. 5, 6, 7, 8, whereas Figs. 9, 10, 11, 12 depict the behaviors of patients (2) and (3). As seen in Figs. 5, 6, 7, 8, the meaningful information associated with the peak of significant amplitudes in the hand vibration spectra is found between 4 and 12 Hz, matching previously published results [30].

Patient (4): resting hand. a Linear motion along the x-axis; b linear motion along the y-axis; c rotational motion around the x-axis (roll); d rotational motion around the y-axis (pitch)

Patient (4): holding an object. a Linear motion along the x-axis; b linear motion along the y-axis; c rotational motion around the x-axis (roll); d rotational motion around the y-axis (pitch)

Patient (1): resting hand. a Linear motion along the x-axis; b linear motion along the y-axis; c rotational motion around the x-axis (roll); d rotational motion around the y-axis (pitch)

Patient (1): holding an object. a Linear motion along the x-axis; b linear motion along the y-axis; c rotational motion around the x-axis (roll); d rotational motion around the y-axis (pitch)

Patient (2): resting hand. Linear motion along the x-axis; b linear motion along the y-axis; c rotational motion around the x-axis (roll); d rotational motion around the y-axis (pitch)

Patient (2): holding an object. a Linear motion along the x-axis; b linear motion along the y-axis; c rotational motion around the x-axis (roll); d rotational motion around the y-axis (pitch)

Patient (3): resting hand. a Linear motion along the x-axis; b linear motion along the y-axis; c rotational motion around the x-axis (roll); (d) rotational motion around the y-axis (pitch)

Patient (3): holding an object. a Linear motion along the x-axis; b linear motion along the y-axis; c rotational motion around the x-axis (roll); d rotational motion around the y-axis (pitch)
Moreover, Patient 4 (affected by ET) clearly shows that the prominent peaks are in the “voluntary” zone. Beyond that limit, the spectrum is flat, which indicates that the energy is not focused on a particular frequency, and the response is more of a “broadband” type. Essential tremor is mostly seen during the action and substantially increases when the patient holds an object. Generally, ET signs are worse when moving than when at rest. The fact that this shaking is worse when in action (i.e., a moving tremor) is a key difference between ET and Parkinson’s [38, 39]. When the patient holds an object, the energy is shifted to a higher frequency range. Quickly, the muscle becomes tired, and fatigue generates an irregular signal shape. For patient 1 (also affected by ET), the spectra show no dominant peaks in the “involuntary” zone. The response has a broadband pattern as well. Similarly, the tremor is mostly seen during the action: the tremor substantially decreased when the patient held an object. The duration of illness (20 years for patient 4 and 10 years for patient 1) is also visible in both sets of results, as more perturbation could be seen in the spectra of patient 4.
The absence of dominant peaks in the spectrum is a clear indication that the use of TMD, the very principle of which is based on tuning on specific values, cannot be technically considered to absorb the hand tremors. Figures 9, 10, 11, 12 represent the spectrum of tremors associated with Parkinson’s Disease experienced by patients 2 and 3.
A glance at Figures 9, 10, 11, 12, which shows the vibrations produced by patients suffering from Parkinsonism, reveals noticeable peaks between 3 and 8 Hz. The dominance of such peaks in the spectral response is a clear indication, from an engineering perspective, that the use of TMD can seriously be considered to absorb the hand tremors and provide more stability for the patient. Voluntary vibrations were detected in a lower frequency range (1–2 Hz). This could be related to fluctuating muscle rigidity. Moreover, the reading from patient 2 showed that the tremors were manifest during the action but got noticeably amplified when the patient was at rest. However, it is essential to note that not every patient exhibits this symptom, making diagnosis more difficult. Although not as common, patients with Parkinson’s disease can also experience action tremors. However, the readings for the patient (3) are more complicated. The spectra show fluctuating peaks. This is probably a result of the long duration of experiencing the tremor (around 18 years). More investigation is needed in this case, with a careful medical history analysis to reach reliable conclusions. The results show the effects of tremors when comparing medication versus no medication case basis. The data collected can also be used to categorize and identify the types of tremors and the type of medication used. Further investigation is required with a focus on comprehensive tests for large samples to understand and be able to categorize tremors' nature more accurately and avoid any misleading results.
Conclusions
This paper proposed implementing wearable device technology in monitoring upper limb tremor detection for Parkinson’s disease and essential tremor. A data acquisition framework was built on information collected from patients by wearable bracelets using microelectromechanical sensors. Results obtained from offline, online, and live monitoring were analyzed to classify tremors based on an engineering perspective. Analysis of the vibration spectrum highlighted significant findings in automated data monitoring:
-
Hand tremors can be classified as either voluntary or involuntary motions based on the relative position of their significant peaks on the vibration spectrum with respect to the critical limit of 2 Hz.
-
Essential tremors exhibit maximum amplitude during voluntary motions. Measured ET shifted to a higher frequency when performing activities, and muscles quickly fatigue to produce an irregular spectrum.
-
Parkinsonian tremors are usually characterized by a vibration peak located between 3 and 8 Hz, with visible dominance of rotational over axial motion.
A low-cost MEMS accelerometer monitoring offers the flexibility of a compact wearable sensing device for tremor detection and measurement. The data collected here will be used later to design a dynamic tuned mass damper intended to suppress tremors associated with all types of syndromes, particularly Parkinson’s disease. Future work can also be extended to increase the study population and expanding the scope of the tremor study.
References
Deuschl G, Petersen I, Lorenz D et al (2015) Tremor in the elderly: Essential and aging-related tremor. Mov Disord 30:1327–1334
(2010) Essential Tremor (ET) How do they differ? Parkinsonian tremor signs & symptoms essential tremor signs & symptoms. www.essentialtremor.org. Accessed 30 June 2021
Tremor Fact Sheet | National Institute of Neurological Disorders and Stroke. https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Tremor-Fact-Sheet. Accessed 30 June 2021
Huen D, Liu J, Lo B (2016) An integrated wearable robot for tremor suppression with context aware sensing. In: BSN 2016—13th Annu Body Sens Networks Conf 2016, pp 312–317
Goetz CG, Tilley BC, Shaftman SR et al (2008) Movement disorder society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord 23:2129–2170
Dai H, Cai G, Lin Z et al (2021) Validation of inertial sensing-based wearable device for tremor and bradykinesia quantification. IEEE J Biomed Heal Inform 25:997–1005
Delrobaei M, Baktash N, Gilmore G et al (2017) Using wearable technology to generate objective Parkinson’s disease dyskinesia severity score: possibilities for home monitoring. IEEE Trans Neural Syst Rehabil Eng 25:1853–1863
Delrobaei M, Memar S, Pieterman M et al (2018) Towards remote monitoring of Parkinson’s disease tremor using wearable motion capture systems. J Neurol Sci 384:38–45
Habets JGV, Heijmans M, Kuijf ML et al (2018) An update on adaptive deep brain stimulation in Parkinson’s disease. Mov Disord 33:1834–1843
Hallil H, Dejous C, Hage-Ali S et al (2021) Passive resonant sensors: trends and future prospects. IEEE Sens J 21:12618–12632
Dutoit NE, Wardle BL, Kim S-G (2005) Desin considerations for MEMS-scale piezoelectric mechanical vibration energy harvesters. Integr Ferroelectr 71:121–160
Thorp JE, Adamczyk PG, Ploeg HL et al (2018) Monitoring motor symptoms during activities of daily living in individuals with Parkinson’s disease. Front Neurol 9:1036
Rovini E, Maremmani C, Cavallo F (2017) How wearable sensors can support Parkinson’s disease diagnosis and treatment: a systematic review. Front Neurosci 11:555
Sánchez-Ferro Á, Elshehabi M, Godinho C et al (2016) New methods for the assessment of Parkinson’s disease (2005 to 2015): a systematic review. Mov Disord 31:1283–1292
Basu I, Graupe D, Tuninetti D et al (2013) Pathological tremor prediction using surface electromyogram and acceleration: potential use in ‘ON-OFF’ demand driven deep brain stimulator design. J Neural Eng 10:36019
Khobragade N, Graupe D, Tuninetti D (2015) Towards fully automated closed-loop deep brain stimulation in Parkinson’s disease patients: a LAMSTAR-based tremor predictor. In: Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS. Institute of Electrical and Electronics Engineers Inc., pp 2616–2619
Rodríguez-Martín D, Samà A, Pérez-López C et al (2017) Home detection of freezing of gait using support vector machines through a single waist-worn triaxial accelerometer. PLoS ONE 12:e0171764
Griffiths RI, Kotschet K, Arfon S et al (2012) Automated assessment of bradykinesia and dyskinesia in Parkinson’s disease. J Parkinsons Dis 2:47–55
Cancela J, Mascato SV, Gatsios D, et al (2016) Monitoring of motor and non-motor symptoms of Parkinson’s disease through a mHealth platform. In: Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS. Institute of Electrical and Electronics Engineers Inc., pp 663–666
Angeles P, Tai Y, Pavese N, et al (2017) Automated assessment of symptom severity changes during deep brain stimulation (DBS) therapy for Parkinson’s disease. In: IEEE Int Conf Rehabil Robot, pp 1512–1517
Bayés À, Samá A, Prats A et al (2018) A “HOLTER” for Parkinson’s disease: validation of the ability to detect on-off states using the REMPARK system. Gait Posture 59:1–6
Channa A, Ifrim RC, Popescu D et al (2021) A-wear bracelet for detection of hand tremor and bradykinesia in parkinson’s patients. Sensors (Switzerland) 21:1–23
de Arriba-Pérez F, Caeiro-Rodríguez M, Santos-Gago JM (2016) Collection and processing of data from wrist wearable devices in heterogeneous and multiple-user scenarios. Sensors (Switzerland) 16:1538. https://doi.org/10.3390/s16091538
Yang H, Shen Y, Zhuang W et al (2021) A smart wearable ring device for sensing hand tremor of parkinson’s patients. C Comput Model Eng Sci 126:1217–1238
Madhava Reddy S, Anudeep Kumar A (2013) Study on MEMS fabrication techniques and applications. Int J Eng Sci Res Technol 2:2300–2305
Dadafshar M (2021) Accelerometer and gyroscopes sensors: operation, sensing, and applications. https://www.maximintegrated.com/en/design/technical-documents/app-notes/5/5830.html. Accessed 30 June 2021
Bilski P, Winiecki W (2007) A low-cost real-time virtual spectrum analyzer. IEEE Trans Instrum Meas 56:2169–2174
Swiszcz G, Cruden A, Booth C, et al (2008) A data acquisition platform for the development of a wind turbine condition monitoring system. In: Proceedings of 2008 International Conference on Condition Monitoring and Diagnosis, CMD 2008. IEEE Computer Society, pp 1358–1361
Zhang JZ, Chen JC (2008) Tool condition monitoring in an end-milling operation based on the vibration signal collected through a microcontroller-based data acquisition system. Int J Adv Manuf Technol 39:118–128
Adeyeri MK, Mpofu K, Kareem B (2016) Development of hardware system using temperature and vibration maintenance models integration concepts for conventional machines monitoring: a case study. J Ind Eng Int 12:93–109
Katalin A (2008) Microcontroller based system for vibration analysis. In: IEEE International Conference on Automation, Quality and Testing, Robotics, AQTR 2008—THETA 16th Edition—Proceedings, pp 171–174
Florin G, Luminita P, Constantin C (2008) Novel algorithms and techniques in telecommunications, automation and industrial electronics. Springer, Dordrecht, pp 89–92
Jamil IA, Abedin MI, Sarker DK, et al (2014) Vibration data acquisition and visualization system using MEMS accelerometer. In: 1st International Conference on Electrical Engineering and Information and Communication Technology, ICEEICT 2014. Institute of Electrical and Electronics Engineers Inc. Doi: https://doi.org/10.1109/ICEEICT.2014.6919090. Epub ahead of print 8 Oct 2014
González A, Olazagoitia JL, Vinolas J (2018) A low-cost data acquisition system for automobile dynamics applications. Sensors (Switzerland) 18:366
Vidhyotma, SJ (2019) Comparative analysis of existing latest microcontroller development boards. In: Proceedings of International Conference ICERECT 2018. Springer Verlag, pp 1011–1025
PCB Piezotronics (2018) Hand-held shaker model:394C06, https://www.pcb.com/products?model=394C06
Deuschl G, Bain P, Brin M et al (1998) Consensus statement of the Movement Disorder Society on tremor. Mov Disord 13:2–23
Papengut F, Raethjen J, Binder A et al (2013) Rest tremor suppression may separate essential from parkinsonian rest tremor. Park Relat Disord 19:693–697
Cohen O, Pullman S, Jurewicz E et al (2003) Rest tremor in patients with essential tremor. Arch Neurol 60:405–410
Acknowledgements
This work was partially supported by the College of Engineering at Qatar University [Grant reference: QUST-1-CENG-2020-14].
Funding
Open Access funding provided by the Qatar National Library.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there are no conflicts of interest.
Informed consent
Informed consent was obtained from all subjects involved in this study. This study was conducted according to the guidelines of the Declaration of Helsinki and in accordance with the Qatar Supreme Council of Health Policies, Regulations, and Guidelines for Research Involving Human Subjects.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yousef, M., Hafizh, M., Sassi, S. et al. Development of a Wearable Wireless Sensing Device for Characterization of Hand Tremors Through Vibration Frequency Analysis. J. Vib. Eng. Technol. 11, 3109–3120 (2023). https://doi.org/10.1007/s42417-022-00734-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42417-022-00734-2