
Abstract
Background
Mobile phones are widely used in clinical settings and could be colonized by potential pathogenic bacteria which may lead to hospital-acquired infections (HAIs) transmission. This study aimed to determine the prevalence of bacterial contamination of healthcare workers’ (HCWs) mobile phones, identify bacterial isolates, and assess the factors associated with mobile phone contamination.
Methods
Self-administered questionnaire was used to collect the information on the demographic characteristics and the use of mobile phones. A total of 111 HCWs’ hands and their mobile phones were swabbed, then bacterial culture, isolation, and identification were performed. Univariate and multivariable logistic regression were applied to identify factors associated with mobile phone bacterial contamination.
Results
Totally 106 (95.5%) of the 111 mobile phones investigated were contaminated with bacteria. Staphylococcus epidermidis (13/111), Acinetobacter baumannii (4/111) and Staphylococcus aureus (3/111) were the predominant bacterial isolates from HCWs’ mobile phones. Univariate analyses showed that age, gender, profession and the frequency of mobile phone utilization were significantly associated with the number of bacterial colonization. Frequency of phone utilization (OR 8.366; 95% CI 1.496–46.797) was found to be the most significant factors associated with the qualified rate of mobile phones bacterial load. In addition, phone cover using was associated with the increased risk of mobile phone bacterial contamination.
Conclusion
There was cross-contamination between hands and phones. It is necessary to develop guidelines for mobile phone cleaning. Special attention needs to be paid to the disinfection of mobile phone covers to reduce contamination and transmission of pathogens.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Hospital-acquired infection (HAI) is the most frequent result of unsafe patient care worldwide [1], and it is deemed a global public health problem [2,3,4]. Not only patients, but also health care workers (HCWs) can have the possibility of acquiring and transmitting the infection in hospitals [5, 6]. HAIs give rise to increasing morbidity, mortality, length of stay, and hospital costs in many countries including China [7]. It is critical to control HAIs as the world battles with the COVID-19 pandemic.
Vast majority of HAIs are caused by bacteria, and it is well recognized that certain environments may facilitate the transmission of healthcare-associated pathogens [8]. HCWs’ fomites are highly predisposed to bacterial contamination in health care settings and are potential sources of HAIs [9]. Contaminated hands of HCWs play a critical role in spreading HAIs in hospitals [10]. Objects with frequent hand contact, such as stethoscopes and mobile phones, could serve as reservoirs from which HAIs can spread to the hands of HCWs and then to patients [11]. In health services, mobile phones are not only used in traditional fields such as registration and medical treatments but also used in healthcare facilities for better disease control [12]. Existing data have demonstrated the bacterial contamination of mobile phones in clinical settings and reported that the levels of contamination and the types of bacteria depended on the settings [13]. Some microbiologists share the opinion that the combination of constant handing and heat generated by mobile phones has created prime breeding ground for all sorts of microorganisms [12]. Previous studies described that microorganisms isolated from mobile phones and HCWs’ hands were similar [14, 15], and the mobile phone bacterial contamination rate ranged from 40 to 100% [16]. It was estimated that averagely a mobile phone harbored 25,107 bacteria per square inch [17], and mobile phones could be also colonized by fungi and even RNA viruses, such as SARS-CoV-2 [18]. A review of surveys showed that the rate of bacteria isolated from the mobile phones in descending order were Coagulase-negative staphylococci (CoNS), Micrococcus, Viridans streptococci, and Acinetobacter species [11]. The risk of cross-infection cannot be ignored if the HCWs are still using contaminated mobile phones without hand hygiene before medical activities.
Our study aimed to assess the prevalence of bacterial contamination on both HCWs’ mobile phones and their hands, identify the bacterial species, and define the factors associated with bacterial isolates from the mobile phones of HCWs working at municipal hospitals of Chongqing, China. The results may provide more evidence to support the promotion of HAI control.
2 Methods
2.1 Study Participants and Sampling Methods
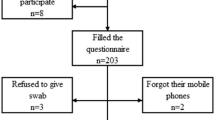
This cross-sectional study was conducted from April to June in 24 hospitals of Chongqing, China. Sample size was calculated based on a previous similar study [19]. We used the formula N=\({\mathrm{Z}}_{\mathrm{\alpha }/2}^{2}\) P(1−P)/d2, where N = sample size, Zα/2 = statistic for the level of confidence = 1.96,α = 0.05, P = expected prevalence = 50% (prevalence of mobile phone contamination with bacteria) [16], and d = allowable error = 0.1(10%). The calculated sample size was 96. Considering a 25% (24) non-response rate, the total sample size was 120. The study population was health care professionals working in nine different departments with high prevalence of HAIs, including nurses, doctors, laboratory technicians, healthcare assistants, and other HCWs. According to the degree of cleanliness requirement, these departments were divided into 4 types of environments: Class I (cleanliness best) included laminar flow operating room. Class II (cleanliness better) included general operating room, ICU, delivery room, and neonatal ward. Class III (cleanliness good) included hemodialysis room and central sterile supply department. Class IV (cleanliness normal) included consulting room for stomatology and therapeutic room. The sample size was allocated equally to the four environments to their total number. Only the mobile phones of the HCWs used for more than 1 week with the surface not being disinfected on the day of the investigation were selected as samples. A total of 120 HCWs were approached and invited to participate, and 111 of them agreed and completed the investigation (response rate = 92.5%).
2.2 Data Collection and Laboratory Methods
A self-administered questionnaire was administered to all participants to collect the information on demographic characteristics (age, gender, profession, educational status and department), with questions regarding their use of mobile phones and awareness of the presence of microorganisms on mobile phones. All questions were formulated by referencing previously validated questionnaires [11, 20, 21]. Before the formal investigation, 20 pre-survey questionnaires were collected and reviewed in one of the 24 hospitals, and the questionnaire was adjusted and revised based on the pre-survey results. In formal investigation stage, further explanations were provided if the participants were confused or had any questions. After completing the questionnaire and sampling, a fixed researcher was asked to observe and record whether the HCWs used/touched their mobile phones within 10 min after hand hygiene. The observation was stopped after 10 min.
Hand samples were collected before hand hygiene. The participants were asked to have their five fingers closed together and a sterile swab moistened with sterile saline was used to rub back and forth twice from the finger root to the finger end (the area was approximately 30 cm2). Mobile phone samples were collected simultaneously with hand samples. The screens, earpieces, sides, and backs of mobile phones were swabbed using sterile swabs (the area was approximately 100 cm2). Strict bacteriological sample collection procedure was followed at the time of swabbing. Sample collectors wore masks and used quick-drying hand disinfectant to avoid cross-contamination. Each sample was given unique identification number and labeled with the name of the department. The sampling time was between 9:00 and 10:00 AM. The collected samples were kept in the brain heart infusion broth as transport medium and transported to the laboratory for culture within 5 h after sampling. Samples were mixed and immediately inoculated onto agar plates, which were incubated for 48 h at 36 ± 1 ℃ aerobically. Colony count was calculated using the semi-quantitative colony-forming unit (CFU) count method in which the number of colonies isolated from each sample was divided by the area sampled [20]. To obtain a higher purity of pathogenic bacteria, the methods of enriching, separating, and identifying were adopted. Samples were inoculated on blood agar, MacConkey agar, Salmonella-Shigella agar, and Mannitol salt agar aerobically at 37 ℃ for 18–24 h. Primary isolation of bacteria was made based on their colony characteristics and Gram stain reaction microscopically. Further identification was performed by conventional biochemical tests (like catalase test, oxidase test, coagulase test, carbohydrate fermentation, H2S production, citrate utilization test, motility, indole test, lysine decarboxylase test, lysine deaminase test, and urea test) and automated system VITEK 2 (BioMerieux, France). All methods were performed following relevant guidelines and regulations. Any sample with microbial growth was defined as contaminated. To evaluate the cleanliness of samples, we defined the qualified sample as bacterial colonies on hands/phones ≤ 10 CFU/cm2 according to the “Disinfection in Hospital Health Standards” (GB15982-2012) available in China. The qualified sample rate was defined as the sum of the qualified samples/total number of samples × 100%.
2.3 Data Analysis
Median and interquartile range (IQR) was adopted for the statistical description of non-normal data. Differences in proportions between groups were assessed by Chi-Square test. Differences in the number of colonies among groups were assessed by non-parametric test including Wilcoxon test and Kruskal–Wallis test. The variables with statistical significance in univariate tests were further subjected to multivariable logistic regression analysis. The qualified rate of mobile phone of bacteria was the dependent variable. Differences were considered statistically significant at p < 0.05. All analyses were carried out using R (version 3.1.2, R Foundation for Statistical Computing, Vienna, Austria).
2.4 Ethics Approval
The study was approved by the Ethics Committee of Chongqing Center for Disease Control and Prevention, and complied with Declaration of Helsinki. Participation in the survey was voluntary and anonymous. All participants who agreed to participate in this study gave their oral consents, but were blinded to the follow-up observations.
3 Results
A total of 111 HCWs and 111 mobile phones belonging to them were assessed. The average age of the HCWs was 32 ± 9.0 years, mainly females (97; 87.4%) and nurses (85; 76.6%). The use rate of mobile phone was very high in hospital settings, high use (Once every 5 min) represented 10.8% of all participants, and moderate use (Once every 5–30 min) represented 21.6%. Seventy-eight of participants (70.3%) reported using mobile phone covers and 27 (24.3%) reported using phones at work, while 84 (75.7%) said that they never did so. However, of these 84 HCWs, 10 were found using/touching mobile phones in healthcare settings within 10 min after hand hygiene. Others were lost to follow-up or did not use/touch their phones. Seventy-one (64.0%) reported that it was forbidden to use mobile phones in their departments during work. Intriguingly, only two of them (2.8%) were observed to strictly obey the rules and put their phones at designated locations during the survey. Almost all participants (95.5%) believed that mobile phone should be cleaned and disinfected regularly, and wiping with alcohol was the most common methods of disinfection. The characteristics on the use of HCWs’ mobile phones and awareness of the presence of microorganisms on their phones are shown in Table 1.
The median of colony number of mobile phones was 2.9 (0.7–6.7) CFU/cm2. Out of these 111 mobile phones, 106 (95.5%) were contaminated, and the qualified rate of HCWs’ mobile phones of bacteria was 80.2%. The prevalence of mobile phone bacterial contamination was higher than that of hands, while the bacterial load on mobile phones was lower than that on hands (Table 2).
Twenty-three kinds of bacteria were isolated from 54 HCWs’ hands or their phones, while no significant bacterial pathogens were isolated from the samples of the remaining 57 HCWs. The bacterial isolates from HCWs’ mobile phones were similar to those from their hands (Fig. 1). Twenty-one of 54 participants (38.9%) had at least 1 identical bacterium (including pathogenic bacteria and conditionally pathogenic bacteria) simultaneously isolated from their hands and mobile phones. It was found that 55 bacterial strains were isolated from 44 mobile phones and 43 bacterial strains were isolated from 36 hands. About 31.5% (35/111) of phones grew one bacterial species, 7.2% grew 2 different species and 0.9% grew 4 different species. Staphylococcus epidermidis (S. epidermidis) was the most common bacterium isolated from mobile phones, with 13 (11.7%) mobile phones contaminated. Other frequently isolated bacteria included Pantoea (6; 5.4%), Acinetobacter baumannii (4; 3.6%), S. haemolyticus (4; 3.6%) and S. aureus (3; 2.7%). In addition, Escherichia coli (E. coli) was isolated from a HCW’s mobile phone.

Organisms identified from HCWs’ mobile phones and their hands
Results of the Chi-square test showed that the qualified rate of mobile phones bacterial load was significantly different between male and female HCWs (57.1% vs. 83.5%; p = 0.021), and the mobile phone qualified rate of nurses was higher than that of others (84.7 vs. 65.4%; p = 0.031). Those who used mobile phones more frequently had a lower qualified rate of mobile phone bacterial load. Non-parametric tests showed that the number of bacterial colonization varied between different ages, genders, and profession groups (p = 0.048, p = 0.004, and p = 0.045). The lower the frequency of mobile phone use, the fewer bacteria colonized on the surface (p = 0.005). The mobile phones with covers grew more bacteria than those without (p = 0.011) (Table 3). Different environments, educational levels, other mobile phone usage habits, and other variables were not significantly associated with the phone qualified rate of bacteria and the bacterial load (Table S1). Multivariable logistic regression analysis showed that, except the frequency of phone utilization (OR 8.366; 95% CI 1.496–46.797), all other included factors were not statistically associated with the qualified rate of mobile phone bacterial load (Table 4).
4 Discussion
Our investigation provided compelling evidence that HCWs’ mobile phones could be a potential reservoir for bacteria, including some pathogenic bacterial strains, as recognized by other scholars [22]. More interestingly, cover using was associated with increased risk of mobile phone bacterial contamination.
The present survey showed that touch-screen smartphones were widely used by HCWs in municipal hospitals in Chongqing, and the frequency of usage was high and the cumulative time was long. The use of mobile phones was not only used to phone calls, but also with social contacts, payments, and entertainments as well as shopping. During the investigation, we have observed that individual HCWs of the key departments still used or touched mobile phones after hand hygiene. Therefore, it is particularly important to take hand hygiene again before patient contact. Although 64.0% of people confirmed that it was forbidden to use mobile phones at their departments during work, only 2.8% of them were observed to obey the rules, suggesting that the mobile phone ban at work was not strictly implemented. About 32.4% of the HCWs had the habit of cleaning and disinfecting mobile phones regularly, which was higher than those in similar researches of Morvai et al. [16] and Mark et al. [23], but lower than the result of Kotris I et al.[24]. This may be related to the constant emphasis on the importance of HAI control in recent years in China. Similar to other reports [19, 24], most HCWs wiped their mobile phone surfaces with alcohol. On one hand, alcohol is simple, cheap, easy to get, and will not damage their phones. On the other hand, a previous study has shown that regular decontamination of phones with alcohol can reduce contamination rates [22]. The HCWs were highly acquainted that pathogenic bacteria are colonized on mobile phone surfaces and may cause HAIs, which was consistent with the results of the study by Evelyn et al. [25]. The general consensus was that mobile phones should be cleaned and disinfected regularly. Similarly, a cross-sectional study in Kuwait found that 63.0% of HCWs thought mobile phones could play a role in spreading infections in healthcare settings, but 68.0% of them opposed banning the use of mobile phones in their departments [11]. In the current study, 46.8% of HCWs opposed banning the use of mobile phones at work. A study aimed to investigate the level of phones contamination on surgical wards also showed that 75% of people felt that banning the use of phones would not be a practical or realistic solution to reduce infections [22]. Without HCWs’ support for the banning of mobile phone use in hospitals, it is rather important to improve infection control awareness and mobile phone hygiene practice than simply strict restrictions.
Although the HCWs’ phones were almost completely contaminated, the total number of colonies on the phones was lower than that on HCWs’ hands, which seemed to be different from what is usually thought. Contamination with bacterial pathogens was found in 95.5% of HCWs’ mobile phones, consistent with 94.6 [12] and 96.5% [15] of the bacterial contamination rates reported by other researchers. There was even a study performed in a tertiary-level Italian ICU found that all phones (100%) were positive for bacteria [26]. No molecular tests were conducted to determine the clonal relation in this survey, but the detection rate and the bacterial isolates from HCWs’ hands and mobile phones were highly similar (concordance rate = 38.9%). The cross-contamination between the surfaces of mobile phones and HCWs’ hands might exist. Similar bacterial contamination found on hands and phones is relational because most germs encountered are present in the healthcare environment, including dry surfaces not touched by hands [27]. Perhaps in the future study, we can estimate and predict the hand contamination through mobile phone contamination. A number of researches have demonstrated that the most common Gram-positive bacterium isolated from mobile phone surfaces was Staphylococcus and the most common Gram-negative bacterium was Acinetobacter [11, 16, 17, 28], consistent with our study. The preponderance of S. epidermidis in this study was in accordance with the findings of other researchers [29]. In addition, it has been reported that Klebsiella pneumoniae was the predominant pathogen isolated from HCWs’ mobile phones at Felege Hiwot Referral Hospital, northwest Ethiopia [9], but no such result was found in our study. In the hospital setting, although some bacteria which are normal floras on human skins or in the mouths, such as S. epidermidis, are considered to be non-pathogenic in normal circumstances, their high levels of presence on mobile phones with frequent hand contact may pose a risk of HAIs. S. aureus and Acinetobacter baumannii isolated from samples in our study were common causes of HAIs associated with high morbidity and mortality. In a previous study on the microbiome analyses of hospital mobile phones, pathogens including methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE) were isolated [30]. Galazzi A et al. have reported that the isolation rate of MRSA was up to 17% in ICU [26]. Another study from Ethiopia showed that Gram-negative bacteria were isolated from 8.3% of HCWs’ mobile phones and 79.4% of the isolates were multidrug resistant [31]. Antibiotic-resistant bacteria are the most serious health risk for hospitalized patients [32]. Besides, Enterococcus faecium and E. coli were isolated from mobile phones in this study, which suggested poor hygiene conditions of mobile phones and hands because these bacteria are part of the intestinal flora.
The non-parametric test showed that there were significant differences of colony count among subgroups of different ages, genders, professions, frequency of mobile phone use, and use of a phone cover. Similarly, for the evaluation of sample cleanliness, the qualified rate of mobile phones of female HCWs was higher than that of males, and the qualified rate of nurses was higher than that of others. It could be explained that most participants were nurses, and they were mainly females, who were better performers of nosocomial infection control measures, such as hand hygiene [33]. A study conducted in East Ethiopia also found that mobile phones of male HCWs were more contaminated [34]. Male HCWs seems to need more external reminders of mobile phone disinfection and hand hygiene than female HCWs. There was an association between mobile phone qualified rate of bacteria and utilization. With the high daily use rate of mobile phones and the less strict hygienic practices of users, it is reasonable to expect that cross-contamination of microorganisms from phones to hands will occur [35]. After adjusted by potential confounders, all the included factors were not statistically associated with phone qualified rate of bacteria except for the frequency of phone utilization. The results may be attributed to the limited sample size. Previous studies have shown that some factors can be related to phone bacterial contamination, including gender, phone usage frequency, type of phone, and medical specialty [13, 36, 37]. But Heyba et al. found that the only factor that was significantly associated with mobile phone bacterial contamination was whether a doctor had disinfected his mobile phone [11]. Japanese scholars have observed that the bacterial contamination rate was negatively correlated with the frequency of hand hygiene [38], so hand hygiene may be a protective factor against mobile phone bacterial contamination. Based on previous researches and our findings, we have reasons to believe that even if mobile phones are contaminated, the risk of HAIs will be significantly reduced in case HCWs take good hand hygiene before and after entering a patient room (or giving medical cares) [39].
For the first time to our knowledge, we found that the numbers of bacterium colonies on mobile phone surfaces with phone covers were significantly larger than those without. People are accustomed to using a phone cover to prevent mobile phone screen from breaking or bumping. If phone covers are not cleaned and disinfected regularly, they will be more conducive to bacterial colonization. We recommend that HCWs should remove mobile phone covers in their facilities, especially in medical activities. The materials of mobile phone covers are mostly silicone, polycarbonate (PC), and thermoplastic urethane (TPU), which are more conducive to microbial growth than glass materials. This may explain why the phone cover grows more bacteria. In future, phone surface coatings may be a promising option to prevent bacterial adhesion and biofilm formation given the prevalence of antibiotic-resistant bacterial strains [40].
5 Limitations
There are three limitations in our present study. Firstly, we did not perform antimicrobial susceptibility testing and homology analysis for the isolated organism. Some common bacteria like Pseudomonas aeruginosa were not isolated in this study. Secondly, an imbalance among HCWs in favor of nurses occurred within sampling procedure. It may impact the generalizability of our findings to other HCWs. Thirdly, some behavioral factors that may affect the transmission of pathogens were not considered, such as hand-to-mouth and other hand-to-face touching behaviors which may further the transfer of pathogenic microbial agents.
6 Conclusion
In conclusion, our study provided more evidence that HCWs’ mobile phones were highly contaminated with various bacteria in hospitals, and the bacterial contamination between mobile phones and hands was closely related. Most of the isolates were common pathogens or conditional pathogens related to HAIs. Age, gender, profession, phone cover and the frequency of mobile phone utilization were the significantly associated factors of bacterial contamination of mobile phones in this study. More contact with phone screens would increase the bacterial contamination of mobile phones.
Based on the above findings, we strongly recommend standardizing the use of mobile phones in key departments, formulating relevant cleaning guidelines, and increasing the awareness about mobile phone disinfection in healthcare settings. HCWs should remove mobile phone covers in medical activities, if possible. Furthermore, the disinfection of the mobile phone cover and strict hand hygiene are also essential.
Data Availability
All raw data are available upon reasonable request from the primary author.
Abbreviations
- HAIs:
-
Hospital-acquired infections
- HCWs:
-
Healthcare workers
- CoNS :
-
Coagulase-negative staphylococci
- ICU:
-
Intensive care unit
- CFU:
-
Colony-forming unit
- IQR:
-
Interquartile range
- S. :
-
Staphylococcus
- E.coli :
-
Escherichia coli
- MRSA:
-
Methicillin-resistant Staphylococcus aureus
- VRE:
-
Vancomycin-resistant Enterococcus
References
Allegranzi B, Bagheri Nejad S, Combescure C, Graafmans W, Attar H, Donaldson L, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet. 2011;377:228–41.
Burke JP. Infection control—A problem for patient safety. N Engl J of Med. 2003;348:651–6.
Bates DW, Larizgoitia I, Prasopa-Plaizier N, Jha AK. Global priorities for patient safety research. BMJ. 2009;338: b1775.
Benenson S, Cohen MJ, Schwartz C, Revva M, Moses AE, Levin PD. Is it financially beneficial for hospitals to prevent nosocomial infections? BMC Health Serv Res. 2020;20:653.
Morales-Contreras MF, Leporati M, Fratocchi L. The impact of COVID-19 on supply decision-makers: the case of personal protective equipment in Spanish hospitals. BMC Health Serv Res. 2021;21:1170.
Barry M, Al Amri M, Memish ZA. COVID-19 in the shadows of MERS-CoV in the Kingdom of Saudi Arabia. J Epidemiol Glob Health. 2020;10:1–3.
Li C, Duan J, Liu S, Meng X, Fu C, Zeng C, et al. Assessing the risk and disease burden of clostridium difficile infection among patients with hospital-acquired pneumonia at a university hospital in central China. Infection. 2017;45:621–8.
Jayaraman SP, Klompas M, Bascom M, Liu X, Piszcz R, Rogers SO, et al. Hand-hygiene compliance does not predict rates of resistant infections in critically ill surgical patients. Surg Infect (Larchmt). 2014;15:533–9.
Ayalew W, Mulu W, Biadglegne F. (2019) Bacterial contamination and antibiogram of isolates from health care workers' fomites at Felege Hiwot Referral Hospital, northwest Ethiopia. Ethiop J Health Dev. 33:128–41.
Mahfouz AA, Al-Zaydani IA, Abdelaziz AO, El-Gamal MN, Assiri AM. Changes in hand hygiene compliance after a multimodal intervention among health-care workers from intensive care units in Southwestern Saudi Arabia. J Epidemiol Glob Health. 2014;4:315–21.
Heyba M, Ismaiel M, Alotaibi A, Mahmoud M, Baqer H, Safar A, et al. Microbiological contamination of mobile phones of clinicians in intensive care units and neonatal care units in public hospitals in Kuwait. BMC Infect Dis. 2015;15:434.
Nwankwo EO, Ekwunife N, Mofolorunsho KC. Nosocomial pathogens associated with the mobile phones of healthcare workers in a hospital in Anyigba, Kogi state. Nigeria J Epidemiol Glob Hea. 2014;4:135–40.
Brady RR, Verran J, Damani NN, Gibb AP. Review of mobile communication devices as potential reservoirs of nosocomial pathogens. J Hosp Infect. 2009;71:295–300.
Brady RR, Wasson A, Stirling I, McAllister C, Damani NN. Is your phone bugged? The incidence of bacteria known to cause nosocomial infection on healthcare workers’ mobile phones. J Hosp Infect. 2006;62:123–5.
Elkholy MT, Ewees IE. Mobile(Cellular) phones contamination with nosocomial pathogens in intensive care units. Med J Cairo Univ. 2010;78:1–5.
Morvai J, Szabó R. The role of mobile communication devices in the spread of infections. Orv Hetil. 2015;156:802–7.
Selim HS, Abaza AF. Microbial contamination of mobile phones in a health care setting in Alexandria Egypt. GMS Hyg Infect Contr. 2015;10:Doc03.
Tony Ibrahim ANC. Maria Baz, mobile phones: a forgotten source of SARS-CoV-2 transmission. Am J Infect Control. 2020;48:971–2.
Lubwama M, Kateete DP, Ayazika KT, Nalwanga W, Kagambo DB, Nsubuga MD, et al. Microbiological contamination of mobile phones and mobile phone hygiene of final-year medical students in Uganda: a need for educational intervention. Adv Med Educ Pract. 2021;12:1247–57.
Koroglu M, Gunal S, Yildiz F, Savas M, Ozer A, Altindis M. Comparison of keypads and touch-screen mobile phones/devices as potential risk for microbial contamination. J Infect in Dev Count. 2015;9:1308–14.
Kordecka A, Krajewska-Kulak E, Lukaszuk C, Kraszynska B, Kulak W. Isolation frequency of Candida present on the surfaces of mobile phones and handsx. BMC Infect Dis. 2016;16:238.
Mark D, Leonard C, Breen H, Graydon R, O’Gorman C, Kirk S. Mobile phones in clinical practice: reducing the risk of bacterial contamination. Int J Clin Pract. 2014;68:1060–4.
Julian T, Singh A, Rousseau J, Weese JS. Methicillin-resistant staphylococcal contamination of cellular phones of personnel in a veterinary teaching hospital. BMC Res Notes. 2012;5:193.
Kotris I, Drenjancevic D, Talapko J, Bukovski S. Identification of microorganisms on mobile phones of intensive care unit health care workers and medical students in the tertiary hospital. Med Glas (Zenica). 2017;14:85–90.
Sanchez E, Perdigão-Neto L, Alves S, dos Santos C, Rizek MR, Gomez RM, et al. Healthcare professionals perception of mobile phone usage and hand hygiene adhesion in intensive care units. Infect Control Hosp Epidemiol. 2020;41(S1):s346.
Galazzi A, Panigada M, Broggi E, Grancini A, Adamini I, Binda F, et al. Microbiological colonization of healthcare workers’ mobile phones in a tertiary-level Italian intensive care unit. Intensive Crit Care Nurs. 2019;52:17–21.
Tajeddin E, Rashidan M, Razaghi M, Javadi SS, Sherafat SJ, Alebouyeh M, et al. The role of the intensive care unit environment and health-care workers in the transmission of bacteria associated with hospital acquired infections. J Infect Public Heal. 2016;9:13–23.
Ulger F, Dilek A, Esen S, Sunbul M, Leblebicioglu H. Are healthcare workers’ mobile phones a potential source of nosocomial infections? Review of the literature. J Infect Dev Count. 2015;9:1046–53.
Trivedi HR, Desai KJ, Trivedi LP, Malek SS, Javdekar TB. Role of mobile phone in spreading hospital acquired infection: a study in different group of health care workers. NJIRM. 2011;2:61–6.
Simmonds R. The microbiome analysis of hospital mobile phones: hidden contaminants revealed. Infect Control and Hosp Epidemiol. 2020;41: s409.
Araya S, Desta K, Woldeamanuel Y. Extended-spectrum beta-lactamase-producing gram-negative bacteria on healthcare workers’ mobile phones: evidence from Tikur Anbessa specialized hospital, Addis Ababa. Ethiopia Risk Manag Healthc Policy. 2021;14:283–91.
Alfouzan W, Dhar R, Abdo NM, Alali WQ, Rabaan AA. Epidemiology and microbiological profile of common healthcare associated infections among patients in the intensive care unit of a general hospital in Kuwait: a retrospective observational study. J Epidemiol Glob Health. 2021;11:302–9.
Chen P, Yuan T, Sun Q, Jiang L, Jiang H, Zhu Z, et al. Role of quality control circle in sustained improvement of hand hygiene compliance: an observational study in a stomatology hospital in Shandong. China Antimicrob Resist Infect Control. 2016;5:54.
Bodena D, Teklemariam Z, Balakrishnan S, Tesfa T. Bacterial contamination of mobile phones of health professionals in Eastern Ethiopia: antimicrobial susceptibility and associated factors. Trop Med Health. 2019;47:15.
Olsen M, Nassar R, Senok A, Albastaki A, Leggett J, Lohning A, et al. A pilot metagenomic study reveals that community derived mobile phones are reservoirs of viable pathogenic microbes. Sci Rep. 2021;11:14102.
Goldblatt JG, Krief I, Klonsky T, Haller D, Milloul V, Sixsmith DM, et al. Use of cellular telephones and transmission of pathogens by medical staff in New York and Israel. Infect Control Hospl Epidemiol. 2007;28:500–3.
Ustun C, Cihangiroglu M. Health care workers’ mobile phones: a potential cause of microbial cross-contamination between hospitals and community. J Occup Environ Hyg. 2012;9:538–42.
Morioka I, Tabuchi Y, Takahashi Y, Oda Y, Nakai M, Yanase A, et al. Bacterial contamination of mobile phones shared in hospital wards and the consciousness and behavior of nurses about biological cleanliness. Nihon Eiseigaku Zasshi. 2011;66:115–21.
Smiddy MP, Murphy OM, Savage E, Fitzgerald AP, FitzGerald S, Browne J. Impact of improved observed hand hygiene on bloodstream infection rates in Ireland. A prospective segmented regression analysis 2009–2016. Epidemiol Infect. 2020;148:e83.
McCumber AW, Volkoff SJ, Anderson DJ, Gunsch CK. Impacts of silver-coated antimicrobial screen covers on the cell-phone microbiome of resident physicians. Infect Control Hosp Epidemiol. 2019;40:1427–9.
Acknowledgements
We extend our sincere thanks to our colleagues, the microbiology team, and the HCWs from 24 hospitals for participating in our survey.
Funding
This work was supported by the Scientific Research Project of Chongqing Municipal Health and Family Planning Commission (No. 2015MSXM095).
Author information
Authors and Affiliations
Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Conflict Of Interest
The authors have no conflicts of interest in this work.
Supplementary Information
Below is the link to the electronic supplementary material.
44197_2022_57_MOESM1_ESM.docx
Supplementary file1 Table S1 Comparison of qualified rate and bacterial load of mobile phones according to other variables (DOCX 22 KB)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yao, N., Yang, XF., Zhu, B. et al. Bacterial Colonization on Healthcare Workers’ Mobile Phones and Hands in Municipal Hospitals of Chongqing, China: Cross-contamination and Associated Factors. J Epidemiol Glob Health 12, 390–399 (2022). https://doi.org/10.1007/s44197-022-00057-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s44197-022-00057-1