
Abstract
Background:
It is unknown whether a history of breast cancer (BC) affects the outcome of BRCA1/2-associated epithelial ovarian cancer (EOC). This was investigated in the current analysis.
Methods:
We included 386 BRCA1/2-associated EOC patients diagnosed between 1980 and 2015. Progression-free survival (PFS), progression-free interval (PFI), overall survival (OS) and ovarian cancer-specific survival (OCSS) were compared between EOC patients with and without previous BC.
Results:
BRCA-associated EOC patients with, vs without, a BC history had a significantly worse PFS and PFI (multivariate hazard ratio (HRmult) 1.47; 95% confidence interval (CI) 1.03–2.08 and HRmult 1.43; 95% CI 1.01–2.03), and a non-significantly worse OS (HRmult 1.15; 95% CI 0.84–1.57) and OCSS (HRmult 1.18; 95% CI 0.85–1.62). Ovarian cancer-specific survival was significantly worse for the subgroup treated with adjuvant chemotherapy for BC (HRmult 1.99; 95% CI 1.21–3.31).
Conclusions:
Our results suggest that BRCA1/2-associated EOC patients with a previous BC have a worse outcome than EOC patients without BC, especially when treated with adjuvant chemotherapy.
Similar content being viewed by others


Main
It is assumed that 8–16% of all epithelial ovarian cancer (EOC) cases are due to BRCA1/2 germ line mutations (Risch et al, 2001; Thompson et al, 2002; Alsop et al, 2012). An improved survival after primary therapy has been reported for BRCA1/2-associated compared with sporadic EOC patients (Vencken et al, 2011; Yang et al, 2011; Hyman et al, 2012). This is thought to be explained by the crucial role of BRCA genes in homologous recombination, a mechanism to repair double-strand DNA breaks, which is deficient in patients without functional BRCA proteins. Platinum chemotherapy, like cisplatin or carboplatin, being a cornerstone in EOC treatment, typically induces double-strand DNA breaks leading to more cancer cell death in BRCA1/2 mutation carriers.
Around 30–50% of the BRCA1/2-associated EOC patients have been treated for previous breast cancer (BC; Alsop et al, 2012; Vencken et al, 2013), whereas data on the incidence of EOC after BC in BRCA1/2 mutation carriers are scarce. Metcalfe reported a 10-year actuarial risk of developing EOC after BC of 12.7% for BRCA1 and of 6.8% for BRCA2 mutation carriers (P=0.03) (Metcalfe et al, 2005). Currently it is unknown whether a BC history affects the outcome of subsequent EOC in BRCA1/2 mutation carriers, especially as treatment for early BRCA-associated BC frequently includes adjuvant chemotherapy.
In the current study we evaluated the outcome of EOC in BRCA1/2 mutation carriers with and without a BC history. In addition, we investigated the impact of adjuvant chemotherapy for BC on the outcome of BRCA1/2-associated EOC.
Materials and methods
Patients
Initially, we selected EOC patients identified with a BRCA1 or BRCA2 mutation, diagnosed between 1980 and 2008 from databases at all eight Dutch University Medical Centres, one Cancer Centre and the Netherlands Foundation for the Detection of Hereditary Tumours (STOET), as has been described previously (Vencken et al, 2013). In four centres both BRCA1 and BRCA2 patients were included, whereas in six centres, due to a lower prevalence, only BRCA2 patients were included. In addition, from the Erasmus MC in Rotterdam BRCA1/2-associated EOC patients treated between 2008 and 2015 were included. Exclusion criteria were a previous malignancy (except for BC and basal cell carcinoma), a borderline ovarian tumour and a primary or recurrent BC synchronous with EOC.
For the selected patients, data concerning tumour characteristics, treatment for BC and EOC, and follow-up were collected from medical records. The medical ethical committee of the Erasmus MC, Rotterdam (MEC-2014–429) approved the study.
Definitions
The main outcome measures were progression-free survival (PFS), progression-free interval (PFI), overall survival (OS) and ovarian cancer-specific survival (OCSS).
Progression-free survival was defined as the time between the date of EOC diagnosis and the date of progressive or recurrent disease. Progression-free interval was defined as the time between the last day of first-line treatment for EOC and the date of progressive/recurrent disease. The end date of chemotherapy was estimated if the last day of chemotherapy was unknown. Overall survival was defined as the time between date of EOC diagnosis and date of death. Ovarian cancer-specific survival was defined as the time between the date of EOC diagnosis and the date of death due to EOC.
Statistics
Differences in tumour and treatment characteristics between EOC patients with and without a history of BC were tested with the Pearson’s χ2-test or, in case of small numbers, with the Fisher’s exact test (categorical variables) or with the Student’s t-test (continuous variables). Progression-free survival, PFI, OS and OCSS were calculated using the Kaplan–Meier survival method for patients with and without a previous BC separately. Subsequent analyses were performed for the group of patients treated with and without adjuvant chemotherapy for a previous BC separately. To account for the time elapsed between EOC diagnosis and genetic testing, we performed left-truncated survival analyses. Patients were censored at date of loss to follow-up, or end date of the study (April 2015). For PFS, PFI and OCSS patients were also censored at date of death not due to EOC. Differences between the groups were tested by means of a log rank test. Univariate as well as multivariate Cox proportional hazard regression models were performed, to calculate hazard ratio’s (HRs) and 95% confidence intervals (95% CIs). Following confounding factors were included in the multivariate regression model: age at EOC diagnosis (continuous), year of EOC diagnosis (<2000; ⩾2000), CA-125 level at diagnosis (<35; 35–500; >500; unknown), differentiation grade (grade I and grade II; grade III; unknown), FIGO stage (I- IIa;>IIa; unknown), type of mutation (BRCA1; BRCA2) and chemotherapy regimen for EOC (platinum/paclitaxel; platinum without paclitaxel; non-platinum-based; unknown). Analyses were performed using SPSS (version 21.0; SPSS, Inc., Chicago, IL, USA) or Stata (version 14; Stat Corporation, College Station, TX, USA). A two-sided P-value< 0.05 was considered statistically significant.
Results
Patient, tumour and treatment characteristics of 116 EOC patients with previous BC and 270 without previous BC are presented in Table 1. In Supplementary Table 1, data on BC treatment are summarised. The median age at EOC diagnosis was 51.8 for BRCA1 and 56.3 years for BRCA2 patients, and 73% of the patients were diagnosed with advanced stage disease (⩾ FIGO stage IIb). CA-125 values at EOC diagnosis were lower in the group with previous BC (P=0.02). The patients with previous BC were less often tested for BRCA1/2 mutations after their EOC diagnosis (P<0.001). There were no other significant differences between the characteristics of the two patient groups, with and without previous BC, observed (Table 1).
Progression-free survival was not significantly different for patients with previous BC compared with patients without a previous BC (5-year PFS 22% vs 28%; Figure 1a and Supplementary Table 2). In the multivariate analysis, however, PFS was significantly lower in the group with previous BC (HR multivariate (HRmult) 1.47; 95% CI 1.03–2.08). Similar data were observed for PFI, at univariate analysis no significant difference was found between the two patient groups, whereas in the multivariate analysis the group with a history of BC had a shorter PFI (HRmult 1.43; 95% CI 1.01–2.03; Figure 1b and Supplementary Table 2). No significant difference was found regarding OS (HRmult 1.15; 95% CI 0.84–1.57) and OCSS (HRmult 1.18; 95% CI 0.85–1.62) between patients with and without a history of BC (Supplementary Table 2 and Figure 1c and d). The time between BC diagnosis and EOC diagnosis was not associated with PFS (HRmult 1.00; 95% CI 0.96–1.04), nor with OCSS (HRmult 0.99; 95% CI 0.95–1.04; data not shown).

Progression free survival (A), progression free interval (B), overall survival (C) and ovarian cancer-specific survival (D) for BRCA1/2 epithelial ovarian cancer patients with and without a BC history. BC, breast cancer; CI, confidence interval; HR, hazard ratio.
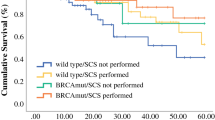
To address the possible impact of adjuvant chemotherapy administered for BC on the PFS and OCSS of subsequent EOC patients with BC before OC treated with chemotherapy and patients not treated with adjuvant chemotherapy for BC were separately analysed and compared with EOC patients without previous BC (Figure 2 and Supplementary Table 3). We observed that PFS and OCSS were especially worse for patients treated with adjuvant chemotherapy for previous BC vs patients without previous BC (median 1.5 vs 2.0, and median 5.0 vs 5.3 years, respectively). In the multivariate analyses these differences were significant (HRmult 2.38; 95% CI 1.40–4.02 and HRmult 1.99; 95% CI 1.21–3.31, respectively). The patients with a BC history not treated with adjuvant chemotherapy had similar PFS and OCSS compared with EOC patients without a BC history (HRmult 1.16; 95% CI 0.76–1.79 and HRmult 0.87; 95% CI 0.59–1.29, respectively; Figure 2 and Supplementary Table 3).

Progression free survival (A) and ovarian cancer-specific survival (B) for BRCA1/2 epithelial ovarian cancer patients with and without adjuvant chemotherapy for BC and without a BC history. BC, breast cancer; CT, chemotherapy.
Discussion
In the current study, we observed a significantly worse PFS and PFI, in BRCA-associated EOC patients with a BC history vs EOC patients without a previous BC, not yet resulting in a significantly worse survival. A significantly worse OCSS, however, was found in BRCA-associated EOC patients treated with adjuvant chemotherapy for BC compared with EOC patients without previous BC.
No differences in grade, stage and histology were observed between both groups. A first hypothetical explanation for this survival difference might be that chemotherapy induces mutations and alters the behaviour of already present malignant EOC cells, or induces chromosomal instability in stem cells with subsequent development of EOC. Another possible explanation might be that treatment for the initial BC aggravates the (bone marrow) condition of the patient and, therefore, optimal therapy for EOC cannot be given to these patients. However, the time between BC diagnosis and OC diagnosis was not associated with outcome, suggesting that the condition of the patients is not the main reason for the worse survival in patients with a BC history.
The retrospective nature of the study brings corresponding limitations, such as different treatments regimens, and some missing data. Another limitation includes that the majority of the patients were tested for a BRCA1/2 mutation after EOC diagnosis (64% and 82% in the groups with and without a BC history, respectively), this will select for survivors. To account for this possible survivorship bias we have conducted left-truncation survival analyses. Because of the retrospective design, no firm conclusions can be drawn and our results should be confirmed in other (prospective) studies with greater sample size.
The results of this study underline the importance of offering genetic testing to BC patients being at risk of BRCA1/2 mutation carriership. Newly diagnosed mutation carriers can then be informed about risk reducing salpingo-oophorectomy, which has been associated with improved survival (Finch et al, 2014). Further, we suggest that studies on survival in BRCA1/2-associated EOC should stratify for BC history.
References
Alsop K, Fereday S, Meldrum C, Defazio A, Emmanuel C, George J, Dobrovic A, Birrer MJ, Webb PM, Stewart C, Friedlander M, Fox S, Bowtell D, Mitchell G (2012) BRCA mutation frequency and patterns of treatment response in BRCA mutation-positive women with ovarian cancer: a report from the Australian Ovarian Cancer Study Group. J Clin Oncol 30: 2654–2663.
Finch AP, Lubinski J, Moller P, Singer CF, Karlan B, Senter L, Rosen B, Maehle L, Ghadirian P, Cybulski C, Huzarski T, Eisen A, Foulkes WD, Kim-Sing C, Ainsworth P, Tung N, Lynch HT, Neuhausen S, Metcalfe KA, Thompson I, Murphy J, Sun P, Narod SA (2014) Impact of oophorectomy on cancer incidence and mortality in women with a BRCA1 or BRCA2 mutation. J Clin Oncol 32: 1547–1553.
Hyman DM, Zhou Q, Iasonos A, Grisham RN, Arnold AG, Phillips MF, Bhatia J, Levine DA, Aghajanian C, Offit K, Barakat RR, Spriggs DR, Kauff ND (2012) Improved survival for BRCA2-associated serous ovarian cancer compared with both BRCA-negative and BRCA1-associated serous ovarian cancer. Cancer 118: 3703–3709.
Metcalfe KA, Lynch HT, Ghadirian P, Tung N, Olivotto IA, Foulkes WD, Warner E, Olopade O, Eisen A, Weber B, Mclennan J, Sun P, Narod SA (2005) The risk of ovarian cancer after breast cancer in BRCA1 and BRCA2 carriers. Gynecol Oncol 96: 222–226.
Risch HA, Mclaughlin JR, Cole DE, Rosen B, Bradley L, Kwan E, Jack E, Vesprini DJ, Kuperstein G, Abrahamson JL, Fan I, Wong B, Narod SA (2001) Prevalence and penetrance of germline BRCA1 and BRCA2 mutations in a population series of 649 women with ovarian cancer. Am J Hum Genet 68: 700–710.
Thompson D, Easton DF Breast Cancer Linkage, C. (2002) Cancer Incidence in BRCA1 mutation carriers. J Natl Cancer Inst 94: 1358–1365.
Vencken PM, Kriege M, Hoogwerf D, Beugelink S, van der Burg ME, Hooning MJ, Berns EM, Jager A, Collee M, Burger CW, Seynaeve C (2011) Chemosensitivity and outcome of BRCA1- and BRCA2-associated ovarian cancer patients after first-line chemotherapy compared with sporadic ovarian cancer patients. Ann Oncol 22: 1346–1352.
Vencken PM, Reitsma W, Kriege M, Mourits MJ, de Bock GH, de Hullu JA, van Altena AM, Gaarenstroom KN, Vasen HF, Adank MA, Schmidt MK, van Beurden M, Zweemer RP, Rijcken F, Slangen BF, Burger CW, Seynaeve C (2013) Outcome of BRCA1- compared with BRCA2-associated ovarian cancer: a nationwide study in The Netherlands. Ann Oncol 24: 2036–2042.
Yang D, Khan S, Sun Y, Hess K, Shmulevich I, Sood AK, Zhang W (2011) Association of BRCA1 and BRCA2 mutations with survival, chemotherapy sensitivity, and gene mutator phenotype in patients with ovarian cancer. JAMA 306: 1557–1565.
Acknowledgements
This study was supported by the Dutch Cancer Society (EMCR 2014–6699). We thank Petra Bos, Annemarie de Jong, Natalia Teixeira, Fon Kosterman and Kelly Kesselaar for their assistance in data collection.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on British Journal of Cancer website
Supplementary information
Rights and permissions
This work is licensed under the Creative Commons Attribution-Non-Commercial-Share Alike 4.0 International License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/4.0/
About this article

Cite this article
Zaaijer, L., van Doorn, H., Mourits, M. et al. Outcome of ovarian cancer after breast cancer in BRCA1 and BRCA2 mutation carriers. Br J Cancer 115, 1174–1178 (2016). https://doi.org/10.1038/bjc.2016.333
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2016.333
- Springer Nature Limited