
Abstract
Background
Newborns may be affected by maternal SARS-CoV-2 infection during pregnancy. We aimed to describe the epidemiology, clinical course and short-term outcomes of babies admitted to a neonatal unit (NNU) following birth to a mother with confirmed SARS-CoV-2 infection within 7 days of birth.
Methods
This is a UK prospective cohort study; all NHS NNUs, 1 March 2020 to 31 August 2020. Cases were identified via British Paediatric Surveillance Unit with linkage to national obstetric surveillance data. Reporting clinicians completed data forms. Population data were extracted from the National Neonatal Research Database.
Results
A total of 111 NNU admissions (1.98 per 1000 of all NNU admissions) involved 2456 days of neonatal care (median 13 [IQR 5, 34] care days per admission). A total of 74 (67%) babies were preterm. In all, 76 (68%) received respiratory support; 30 were mechanically ventilated. Four term babies received therapeutic hypothermia for hypoxic ischaemic encephalopathy. Twenty-eight mothers received intensive care, with four dying of COVID-19. Eleven (10%) babies were SARS-CoV-2 positive. A total of 105 (95%) babies were discharged home; none of the three deaths before discharge was attributed to SARS-CoV-2.
Conclusion
Babies born to mothers with SARS-CoV-2 infection around the time of birth accounted for a low proportion of total NNU admissions over the first 6 months of the UK pandemic. Neonatal SARS-CoV-2 was uncommon.
Study registration
ISRCTN60033461; protocol available at http://www.npeu.ox.ac.uk/pru-mnhc/research-themes/theme-4/covid-19.
Impact
-
Neonatal unit admissions of babies born to mothers with SARS-CoV-2 infection comprised only a small proportion of total neonatal admissions in the first 6 months of the pandemic.
-
A high proportion of babies requiring neonatal admission who were born to mothers with confirmed SARS-CoV-2 infection were preterm and had neonatal SARS-CoV-2 infection and/or other conditions associated with long-term sequelae.
-
Adverse neonatal conditions were more common in babies whose SARS-CoV-2-positive mothers required intensive care compared to those whose SARS-CoV-2-positive mothers who did not.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Although serious infection with SARS-CoV-2 is uncommon in children, maternal SARS-CoV-2 infection around the time of birth is associated with adverse outcomes, including preterm birth1,2 and neonatal infection.3,4,5 Swedish data demonstrate a higher risk of preterm birth, neonatal unit (NNU) admission and neonatal respiratory conditions following birth to a mother with SARS-CoV-2 at any time in pregnancy.6 Although studies show adverse pregnancy outcomes increased in those mothers with severe/critical disease,7 only limited data describe neonatal clinical courses and outcomes. Accumulating data indicate that the Alpha and Delta variants of SARS-CoV-2 may lead to more severe maternal COVID-19;1 for comparative purposes, it is important to establish neonatal impacts of the initial wave of predominantly ‘wildtype’ SARS-CoV-2 infection.
We aimed to describe the presentation, clinical course and short-term outcomes of babies born in the first wave of the pandemic to a mother with confirmed SARS-CoV-2 infection within 7 days of birth and who required NNU admission. Neonatal outcomes were examined by the severity of maternal COVID-19.
Methods
Study design and procedures
This was a national prospective cohort study using the British Paediatric Surveillance Unit (BPSU).8 From 1 April 2020, senior paediatricians in all 155 hospital trusts and health boards with their associated 190 NNUs in the UK received a weekly electronic BPSU reporting card asking them to notify any babies born to mothers with laboratory-confirmed SARS-CoV-2 infection in the 7 days before or after birth, and who required admission to an NNU between 1 March 2020 to 30 August 2020. This did not include routine newborn care provided on the postnatal ward by neonatal health professionals. An additional monthly card asked for confirmation both that all eligible babies had been reported and that zero reports were accurate (active negative surveillance). To maximise case ascertainment, the UK Obstetric Surveillance System (UKOSS) study of COVID-19 admission in pregnancy was also used to identify and link babies born to women with laboratory-confirmed SARS-CoV-2 infection using hospital site, date and time of delivery. Following a BPSU report, notifying clinicians were asked to complete a data collection form with details of the pregnancy, baby characteristics, neonatal management and outcomes. Data collection was supported by hospital-based research nurses from the UK’s National Institute of Health Research (NIHR) Clinical Research Network following the study’s adoption as an urgent public health priority study.
Cases identified were linked to routinely recorded neonatal clinical data held in the National Neonatal Research Database (NNRD) to describe neonatal treatments, clinical course and outcomes.8 Neonatal deaths were cross-checked with national perinatal mortality surveillance data from the Mother and Babies, Reducing Risk through Audits and Confidential Enquires across the UK (MBRRACE-UK) collaboration.9 Neonatal SARS-CoV-2 infection was cross-checked with national testing data from public health organisations as described previously.4
UK SARS-CoV-2 testing policy amongst pregnant women and babies evolved during the study. Initially, only symptomatic women and babies were tested. Routine screening of all obstetric admissions was recommended by the Royal College of Obstetricians and Gynaecologists on 29 May 2020 and neonatal testing was recommended for symptomatic babies of mothers with a SARS-CoV-2 infection; testing of asymptomatic babies varied.10 Confirmation of neonatal SARS-CoV-2 infection required at least two positive samples, including one at least 72 h after birth.10 UK policy was that well babies of SARS-CoV-2-infected mothers should be cared for alongside their mothers in the postnatal ward.
This report presents the characteristics and short-term outcomes for babies born to a mother with confirmed SARS-CoV-2 infection in the 7 days before or after birth between 1 March and 31 August 2020 and for whom complete data had been received by 14 January 2021.
Maternal admission criteria were based on locally defined clinical indications.11 Neonatal intensive care was defined using the British Association of Perinatal Medicine criteria.12 Denominator data for total NNU admissions over the study period were obtained from the NNRD and data describing maternal SARS-CoV-2 infections were taken from the UKOSS which recorded all pregnant women in hospitals with confirmed SARS-CoV-2 infection.11
Parent, patient and public involvement
Parents, patients and the public were consulted during the design of the study and presentation of the findings through the MBRRACE-UK and the NIHR Policy Research Unit in the Maternal and Neonatal Care third-sector stakeholder groups comprising representatives from all the relevant national mother and baby charities in the UK.
Statistical analysis
Descriptive statistics are presented as means with standard deviations and medians with interquartile ranges.
Results
There were 309,518 live births during the study period; 1019 babies were born in the UK to mothers known to have SARS-CoV-2 infection within 7 days of birth during the study period (634 symptomatic mothers, 385 asymptomatic mothers). All were singleton pregnancies. Monthly BPSU card returns were received from between 87.0% and 91.3% of 4091 UK paediatricians each month; 340 potentially eligible babies were reported through the BPSU system and 177 through UKOSS surveillance (Fig. 1). After de-duplication and exclusion of ineligible babies, 111/1019 (10.9%) were admitted to an NNU following maternal SARS-CoV-2 infection around birth.

This flowchart describes how cases were selected including the linkage between BPSU data and UKOSS data.
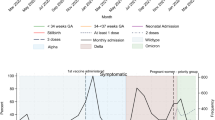
During the study period, 56,179 babies were admitted to an NNU for any reason. Therefore, overall 2 per 1000 (95% CI 1.6–2.4) neonatal admissions were of babies born to mothers with SARS-CoV-2 infection around the time of birth. The highest proportions were in March and April 2020 (3.4 and 6.7 per 1000 admissions, respectively) (Fig. 2). 74/111 babies (67%) were born preterm (<37 weeks’ gestation), including 26 (23%) born very preterm (<32 weeks’ gestation). Over the study period, 6 per 1000 (95% CI 4.4–9.4) very preterm neonatal admissions were babies born to mothers with perinatal SARS-CoV-2 infection. Among babies admitted for neonatal care, 55/111 babies (50%) were born to mothers from non-white ethnic groups (Table 1).

Babies admitted for neonatal care following maternal coronavirus as a proportion per 1,000 of total monthly neonatal admissions between March 2020 to 31st August 2020.
Severity of illness from SARS-CoV-2 infection among the mothers of the 111 admitted infants varied: 28/104 (27%) mother’s required intensive care, of whom four died from SARS-CoV-2; maternal intensive care data were missing for seven cases.
Forty of 111 (36%) babies required neonatal intensive care; 76 (68%) were treated with some form of respiratory support of whom 30 received mechanical ventilation. Four term babies received therapeutic hypothermia for hypoxic ischaemic encephalopathy (Table 2). Eleven (10%) babies had confirmed neonatal SARS-CoV-2. In total, babies born to mothers with SARS-CoV-2 infection around birth received 2456 days of neonatal care (median 13 days [IQR 5, 34] per baby), including 295 days of intensive care (median 0 days [IQR 0, 2] per baby). At the end of follow-up, 105 (95%) babies had been discharged home and two were still admitted to an NNU. Three babies died before discharge from the NNU; outcome data were missing for one baby. In no instance was the cause of death attributed to neonatal or maternal SARS-CoV-2 infection.
The large majority (25/28, 89%) of mothers requiring intensive care had a SARS-CoV-2-indicated caesarean birth, compared to 11% (8/76) for mothers not receiving intensive care. Twenty-six (93%) babies born to mothers requiring intensive care were preterm compared to 43% (33/76) of babies born to mothers who were less unwell or asymptomatic (Table 1). Seven (88%) of eligible mothers requiring intensive care were given magnesium sulfate but only 8/14 (44%) were recorded as having received a full course of antenatal steroids. Only three babies born to mothers who received intensive care were exclusively breastfed at discharge from the NNU. Apgar score was lower in babies born to mothers receiving intensive care (Table 2). A total of 61% (17/28) of babies born to mothers who received intensive care required neonatal intensive care and 54% (15/28) of these babies received mechanical ventilation. Short-term outcomes at neonatal discharge were similar between babies born to mothers who received intensive care and those who did not (Table 2).
Discussion
Using national population-level data collected through active surveillance, we found that babies born to a mother with confirmed SARS-CoV-2 infection around birth, made up a low proportion of total neonatal admissions during the first ‘wildtype’ wave of the pandemic. On average 2 per 1000 neonatal admissions in this wave of the pandemic in the UK were babies of mothers infected with perinatal SARS-CoV-2 infection;13 but there was variation throughout the year in the number of babies affected by maternal SARS-CoV-2 with a considerably higher proportion of neonatal admissions related to maternal SARS-CoV-2 in March and April 2020. This trend follows the epidemiology of community cases of SARS-CoV-2 in the UK, with cases rising in March and reaching a peak in April.14 it is not possible to determine from available data the degree to which this early increase in neonatal admissions additional may be related to additional precautions rather; however, this would be unlikely as national United Kingdom guidance from the start of the pandemic was to keep babies born to SARS-CoV-2-infected mothers with their mother when clinically possible. A total of 640 women with symptomatic SARS-CoV-2 infection gave birth during the study period; further details on maternal and perinatal care and outcomes have previously been described:11 hospitalised women with symptomatic were more likely to be admitted to intensive care but the absolute risk of poor outcomes was low. Neonatal data presented here support this that mortality in babies born to mothers with SARS-CoV-2 infection around birth was low with none of the three neonatal deaths directly attributed to SARS-CoV-2 infection in mother or baby.
Despite these apparently reassuring short-term outcomes, the longer-term implications of maternal SARS-CoV-2 around the time of birth may be more concerning. The rate of very preterm birth, which is strongly associated with long-term morbidity and later mortality, was 2.6% among all mothers with known perinatal SARS-CoV-2 infection who were in hospital, which is approximately double the UK national rate.9,15 Four term babies born to mothers with perinatal SARS-CoV-2 infection received therapeutic hypothermia for hypoxic ischaemic encephalopathy; numbers were low and preclude further formal analysis. Hypoxic ischaemic encephalopathy was not significantly more common in babies born to mothers with SARS-CoV-2 infection in pregnancy in Sweden, with only 3 cases seen among 2323 babies.6
This work highlights the importance of collaborative working between teams caring for pregnant women in intensive care and the maternity team.16 The low rate of administration of a full course of antenatal steroids to mothers receiving intensive care may be explained in part by the urgency of delivery, but is nevertheless concerning.
It is important that SARS-CoV-2 infection is recognised as a significant cause of maternal intensive care admission, particularly in unvaccinated mothers, and appropriate measures are put in place to optimise maternal and neonatal outcomes.1 The low rates of exclusive breastfeeding at neonatal discharge in mothers receiving intensive care are likely related to multiple factors including maternal ill-health and underline the need to follow national guidance to support breastfeeding and expression of breastmilk among mothers who are receiving intensive care.17 The well-established benefits of breastfeeding, including potential transfer of passive immunity against SARS-CoV-2 to the neonate, comprehensively outweigh any unproven risk of viral transmission.18
In keeping with studies in other age groups and populations in the first pandemic wave,3 babies born to mothers from black, Asian, and mixed or other ethnic groups were over-represented in this cohort.19 This has been attributed to socioeconomic differences and compounded by the impact of systemic structural and social inequity.20,21
The major strength of this study is that it reports UK-wide, population-level data from a national health service collected through an established active surveillance system with high reporting levels, linkage with national obstetric active surveillance to ensure high case ascertainment and the addition of routinely recorded neonatal data held in the NNRD. A weakness of the study is that the true incidence of SARS-CoV-2 infection within 7 days of birth is not known because national testing of all obstetric admissions was only introduced part way through this study in May 2020.
Other limitations include the absence of both longitudinal data on laboratory test results and results of neonatal imaging which may inform prognosis. Neither do we have outcomes for babies not admitted to an NNU. The long-term effects of early life exposure to SARS-CoV-2 are unknown, and ongoing data collection, linkage and follow-up are crucial.
Conclusions
Extremely preterm birth was more common among mothers with SARS-CoV-2 infection around the time of birth, but babies born to mothers with perinatal SARS-CoV-2 infection made up a low proportion of UK NNU admissions over the first 6 months of the UK pandemic and neonatal SARS-CoV-2 infection was uncommon in these babies.
Data availability
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.
References
Vousden, N. et al. Severity of maternal infection and perinatal outcomes during periods of SARS-CoV-2 wildtype, alpha, and delta variant dominance in the UK: prospective cohort study. BMJ Med. 1, e000053 https://bmjmedicine.bmj.com/lookup/doi/10.1136/bmjmed-2021-000053 (2022).
Gale, C. et al. National active surveillance to understand and inform neonatal care in COVID-19. Arch. Dis. Child Fetal Neonatal Ed. 105, 346–347 (2020).
Swann, O. V. et al. Clinical characteristics of children and young people admitted to hospital with covid-19 in United Kingdom: prospective multicentre observational cohort study. BMJ 370, m3249 (2020).
Gale, C. et al. Characteristics and outcomes of neonatal SARS-CoV-2 infection in the UK: a prospective national cohort study using active surveillance. Lancet Child Adolesc. Health 5, 113–121 (2021).
Smith, C. et al. Deaths in children and young people in England after SARS-CoV-2 infection during the first pandemic year. Nat. Med. 28, 185–192 (2022).
Norman, M. et al. Association of maternal SARS-CoV-2 infection in pregnancy with neonatal outcomes. JAMA 325, 2076 https://jamanetwork.com/journals/jama/fullarticle/2779586 (2021).
Khan, D. S. A. et al. Differences in pregnancy and perinatal outcomes among symptomatic versus asymptomatic COVID-19-infected pregnant women: a systematic review and meta-analysis. BMC Pregnancy Childbirth 21, 801 (2021).
Verity, C. Surveillance for rare disorders by the BPSU. Arch. Dis. Child 87, 269–271 (2002).
MBRRACE-UK. Perinatal Mortality Surveillance report for births in 2017 https://www.npeu.ox.ac.uk/mbrrace-uk/reports/perinatal-mortality-surveillance#perinatal-mortality-surveillance-report-for-births-in-2017 (2019).
BAPM. COVID-19 Pandemic Frequently Asked Questions within Neonatal Services https://www.bapm.org/pages/182-perinatal-covid-19-resourceshttp://hubble-liveassets.s3.amazonaws.com/bapm/redactor2_assets/files/1110/COVID_FAQs_10.1.21.pdf (2021).
Vousden, N. et al. The incidence, characteristics and outcomes of pregnant women hospitalized with symptomatic and asymptomatic SARS-CoV-2 infection in the UK from March to September 2020: a national cohort study using the UK Obstetric Surveillance System (UKOSS). PLoS One 16, e0251123 (2021).
BAPM. Categories of Care. London https://www.bapm.org/resources/34-categories-of-care-2011 (2011).
Office for National Statistics (ONS). Coronavirus (COVID-19) Infection Survey technical article: waves and lags of COVID-19 in England, June 2021. London https://www.ons.gov.uk/releases/coronaviruscovid19infectionsurveytechnicalarticlewavesandlagsofcovid19inenglandjune2021 (2021).
UK Government. Coronavirus (COVID-19) in the UK https://coronavirus.data.gov.uk/details/cases?areaType=nation&areaName=England (2022).
Pierrat, V. et al. Neurodevelopmental outcome at 2 years for preterm children born at 22 to 34 weeks’ gestation in France in 2011: EPIPAGE-2 cohort study. BMJ 358, j3448 (2017).
MBRACCE-UK. Saving Lives, Improving Mothers’ Care: lessons learned to inform maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2017–19 https://www.npeu.ox.ac.uk/assets/downloads/mbrraceuk/reports/maternal-report-2021/MBRRACE-UK_Maternal_Report_2021_-_FINAL_-_WEB_VERSION.pdf (2021).
Royal College of Obstetrics and Gynaecologists. Coronavirus (COVID-19) infection in pregnancy https://www.rcog.org.uk/guidance/coronaviruscovid-19-pregnancy-and-women-s-health/coronavirus-covid-19-infection-in-pregnancy/ (2021).
WHO. Breastfeeding and COVID-19 https://www.who.int/news-room/commentaries/detail/breastfeeding-andcovid-19 (2020).
Knight, M. et al. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: national population based cohort study. BMJ 369, m2107 (2020).
Office for National Statistics (ONS). Why have Black and South Asian people been hit hardest by COVID-19? London https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/whyhaveblackandsouthasianpeoplebeenhithardestbycovid19/2020-12-14 (2020).
Razai, M. S., Kankam, H. K. N., Majeed, A., Esmail, A. & Williams, D. R. Mitigating ethnic disparities in covid-19 and beyond. BMJ 372, m4921 (2021).
Acknowledgements
This research is funded by the UK NIHR Policy Research Programme, conducted through the Policy Research Unit in Maternal and Neonatal Health and Care (PR-PRU-1217-21202). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. We acknowledge the assistance of Jacob Avis and Richard Lynn at the BPSU, the BPSU reporting clinicians, the NIHR Clinical Research Networks, and other people without whose support this research would not have been possible in such a timely manner.
Funding
The BPSU COVID-19 study is funded by the National Institute for Health Research (NIHR) Policy Research Programme, conducted through the Policy Research Unit in Maternal and Neonatal Health and Care, PR-PRU-1217-21202. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. The UKOSS study was funded by the National Institute for Health Research HS&DR Programme (project number 11/46/12). M.K. is an NIHR Senior Investigator. The Maternal, Newborn and Infant Clinical Outcome Review Programme, delivered by MBRRACE-UK, is commissioned by the Healthcare Quality Improvement Partnership (HQIP) as part of the National Clinical Audit and Patient Outcomes Programme (NCAPOP). The Maternal, Newborn and Infant Clinical Outcome Review Programme is funded by NHS England, NHS Wales, the Health and Social Care division of the Scottish government, The Northern Ireland Department of Health, and the States of Jersey, Guernsey, and the Isle of Man. The study funder had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Author information
Authors and Affiliations
Contributions
S.A. wrote the first draft of the article. S.A., M.A.Q., C.G., J.J.K. and A.P. carried out the analyses. All authors edited and approved the final version of the article. C.G., M.K., S.N.L., E.S.D., D.S., C.D., H.M. and J.J.K. contributed to the development and conduct of the study. C.G. as guarantor accepts full responsibility for the conduct of the study, had access to the data, and controlled the decision to publish. C.G., M.A.Q. and J.J.K. have accessed and verified the data underlying the study.
Corresponding author
Ethics declarations
Competing interests
M.L., M.A.Q. and J.J.K. received grants from the UK NIHR Policy Research Programme in relation to the submitted work. S.A., A.M., M.H., A.P., S.N.L., E.S.D., D.S., C.D., H.M. and C.G. declare no competing interests.
Ethics approval and consent to participate
The study was approved by the North East – Newcastle & North Tyneside 2 Research Ethics Committee (IRAS ID 282127; REC 20/NE/0107). Data were collected in England and Wales without parental consent following Section 251 advice from the Confidentiality Advisory Group of the Health Research Authority (20/CAG/0058) and under the COVID-19 notice issued by the Secretary of State for Health and Social Care under Regulation 3(4) of the Health Service Control of Patient Information Regulations 2002. Data were collected in Scotland without parental consent following COVID-19 rapid review and advice from the Public Benefit and Privacy Panel for Health and Social Care (PBPP) (1920–0288) and with maternal consent following advice from the Privacy Commissioner in Northern Ireland. All NNUs agreed to the inclusion of their NNRD data in the study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ali, S., Mactier, H., Morelli, A. et al. Neonatal outcomes of maternal SARS-CoV-2 infection in the UK: a prospective cohort study using active surveillance. Pediatr Res 94, 1203–1208 (2023). https://doi.org/10.1038/s41390-023-02527-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-023-02527-z
- Springer Nature America, Inc.