
Abstract
Around one-third of people develop depression following ischaemic stroke, yet the underlying mechanisms are poorly understood. Post-stroke depression has been linked to frontal infarcts, mainly lesions in the left dorsolateral prefrontal cortex (DLPFC). But depression is a network disorder that cannot be fully characterised through lesion-symptom mapping. Researchers of depression in non-stroke populations have successfully tapped into the cognitive control network (CCN) using the bilateral DLPFC as a seed, and found that CCN resting-state connectivity is reduced in even mildly depressed subjects, compared to healthy controls. Hence, we aimed to investigate the association between post-stroke depressive features and the CCN resting-state connectivity in a stroke population. We analysed DLPFC resting-state connectivity in 64 stroke participants, 20 of whom showed depressive features assessed with the Patient Health Questionnaire (PHQ-9) at 3 months after stroke. We directly compared groups showing symptoms of depression with those who did not, and performed a regression with PHQ-9 scores in all participants, controlling for age, gender, lesion volume and stroke severity. Post-stroke depression was associated with lower connectivity between the left DLPFC and the right supramarginal gyrus (SMG) in both group and regression analyses. Neither the seed nor the results overlapped with stroke lesions. These findings confirm an important role of the left DLPFC in post-stroke depression, but now show that large-scale network disruptions following stroke associated with depressive features occur without lesions in the DLPFC.
Similar content being viewed by others

Introduction
Depression is a psychiatric disorder associated with persistent sadness, loss of energy and cognitive impairment1,2. It develops in about 30% of stroke patients, regardless of stroke site or severity3. Post-stroke depression has been shown to negatively impact on stroke recovery, worsening cognitive outcomes and reducing motivation4.
The neuroanatomical changes that underlie the clinical manifestation of post-stroke depression remain unclear5. In the acute post-stroke phase, frontal and temporal lesions have been related to depressed mood6,7. Among the frontal regions, lesions to the dorsolateral prefrontal cortex (DLPFC) have been frequently associated with depression8,9. Both left or right DLPFC lesions have been implicated, depending on the post-stroke stage studied (i.e., acute, subacute or chronic)10. However, a recent study by Grajny et al. directly correlated depression severity to the extent of damage in the left DLPFC8. Information about the prevalence of lesions is crucial for understanding post-stroke depression; however, lesion-based characterisation has major limitations. The explanatory power of stroke lesion size and location in accounting for the depressive phenotype is higher in the acute stroke phases, while at later stages lesion mapping might be less reliable due to brain plasticity during the recovery process11,12. In addition, while lesion location is a worse predictor for higher cognitive functions, such as attention and memory, network-based connectivity measures are better suited to describe impairment in more complex behaviours13. Many authors posit that complex psychiatric disorders such as depression would be better characterised using brain network measures that also account for functional and structural brain reorganisation in the subacute and chronic stroke phases.
Resting-state functional magnetic resonance imaging (rs-fMRI) has been shown to be valuable for characterising stroke and recovery14. rs-fMRI was utilised in several studies to identify differences between depressed and healthy subjects or to correlate brain changes to depression severity. They found that post-stroke depression is associated with decreased connectivity in the default mode network15,16 and increased connectivity in the affective network17. Cognitive control network (CCN) is a set of brain regions, localised primarily in the frontal and parietal cortices, that interact in a coupled manner to implement cognitive control in a variety of tasks18. Despite the evidence from lesion studies pointing to the significant role of the DLPFC in post-stroke depression, the CCN has not been investigated. Yet, studies in non-stroke depressed patients with cognitive deficits suggest that bilateral DLPFC connectivity plays an important role in both major19 and subthreshold depression20. We investigated resting-state connectivity in the CCN in participants with and without depressive features 3 months after stroke. In light of the suggested specificity of the left DLPFC in depressed stroke participants, we considered the left and right DLPFC connectivity separately.
Materials and methods
Participants
Participants with ischaemic stroke were recruited from the Stroke Units at three Melbourne hospitals: Austin Hospital, Box Hill Hospital and the Royal Melbourne Hospital as part of the Cognition and Neocortical Volume after Stroke (CANVAS) study21. Each hospital’s ethics committee approved the study in line with the Declaration of Helsinki. The details of the protocol are described in detail in ref. 21. Participants with psychiatric history prior to stroke were excluded from the study. This was a core exclusion criterion for the entire CANVAS study.
Outcome measures
The severity of participants’ stroke was assessed with the National Institutes of Health Stroke Scale (NIHSS) examination performed at hospital admission. The severity of participants’ depression was assessed with the Patient Health Questionnaire-922 specifically validated for the use in stroke populations23. The PHQ-9 scores each of the nine DSM-5 criteria as 0 (not at all) to 3 (nearly every day); scores of 0–27 are possible. The scores of 5–9, 10–14, 15–19 and ≥20 represent mild, moderate, moderately severe and severe depression, respectively (scores correlate with depression severity). DSM-5 defines post-stroke mood disorders as mood disorders due to stroke with depressive features, major depressive-like episode or mixed-mood features24. While the PHQ-9 is not a clinical diagnostic tool for depression, it allows identifying the presence of depressive features. Participants in this study did not have previous history of depression and were not medicated for depression at the time of the study.
Imaging data acquisition and pre-processing
All images were acquired on a Siemens 3 T Tim Trio scanner (Erlangen, Germany) with a 32-channel head coil. As part of an ongoing longitudinal study, participants were assessed at 3 months after their stroke. A high-resolution anatomical MPRAGE was collected (volume of 160 sagittal slices with 1 mm isotropic voxels, repetition time (TR) = 1900 ms, echo time (TE) = 2.55 ms, 9° flip angle, 100% field of view in the phase direction and 256 × 256 acquisition matrix). A high-resolution 3D SPACE-FLAIR image was acquired (with 160 1-mm-thick sagittal slices, TR = 6000 ms, TE = 380 ms, 120° flip angle, 100% field of view in the phase direction and 256 × 254 acquisition matrix). Resting-state data were obtained (132 volumes taking ~7 min, with axial oriented, interleaved slices, 3 mm isotropic voxels, 3 mm slice gap, TR = 3000 ms, TE = 30 ms and 85° flip angle, 100% field of view in phase direction and 72 × 72 acquisition matrix). During resting-state acquisition participants were instructed to keep their eyes closed.
Functional images were pre-processed in SPM8 (Wellcome Department of Imaging Neuroscience, London, UK, http://www.fil.ion.ucl.ac.uk/spm/). The pre-processing pipeline included slice-time correction, with the middle slice as a reference, six-parameter rigid body realignment to estimate and correct for movement, and co-registration to the high-resolution structural image.
Lesions were manually traced on the high-resolution FLAIR image. A stroke neurologist (A.B.) visually inspected and verified the manually traced images. A binary lesion mask was created to improve patient image segmentation and normalisation to the MNI152 template using the Clinical Toolbox SPM extension25 to improve tissue segmentation and preserve the lesion size. Tissue segmentations were manually inspected for quality assurance. Functional images were smoothed with an 8-mm full width half maximum Gaussian kernel.
Pre-processed images were imported into the Conn Toolbox version 16b. Additional head motion analysis was performed using the artefact detection toolbox (ART; https://www.nitrc.org/projects/artifact_detect/). Time points were marked as outliers if global signal exceeded three SDs from the mean and if movement exceeded 0.5 mm of scan-to-scan deviation. ART regressors were added to the six-rigid body motion regressors for motion estimation. Lesion-masked segmentations were used for noise correction. Data were bandpass-filtered between 0.008 and 0.09 Hz. Nuisance regression and bandpass-filtering were performed simultaneously using the Simult function in the Conn Toolbox.
Total intracranial volumes (TIV) were estimated using FreeSurfer automatic segmentation (http://surfer.nmr.mgh.harvard.edu/). White matter hyperintensities (WMHs) were segmented using a Bayesian probabilities approach from the combined information of the T1 and FLAIR images26.
Seeds for the rs-fMRI analysis
For the rs-fMRI analysis we used the seed applied in several resting-state connectivity studies for elucidating the CCN network in major depression19 and subthreshold depression20: the bilateral dorsolateral prefrontal cortex (DLPFC), MNI coordinates ±36, 27, 29, spheres with a 3-mm radius. However, unlike in the previous studies using one seed combining left and right DLPFC, we computed the left and right DLPFC connectivity networks separately. Both region of interest (ROIs) were drawn in WFU Pickatlas27.
Lesion analysis
Lesion overlap images were prepared using MRIcron software28. We created the overlap maps for 20 DEP and 44 NONDEP participants (Fig. 1).

Lesion overlap for DEP (scale 0–4 overlapping subjects) and NONDEP (scale 0–4 overlapping subjects) participants
Statistical analysis
Behavioural data
We identified participants who had PHQ-9 score of ≥5 as a cutoff for mild depression at 3 months post stroke. We divided all stroke participants into two groups: those with depressive features (DEP; ≥5) and those without (NONDEP; <5), and compared the two groups on a number of behavioural variables, as well as brain measures including TIV and the extent of WMH, which have been associated with stroke and depression29,30,31. We used a two-sample t-test for age, PHQ-9 at 3 months, TIV, WMH volume, Boston naming test, Digit Span test, Hopkins Verbal Learning test, Star cancellation test, Complex figure test (copy), Complex figure test (recall); Wilcoxon Test for NIHSS at baseline and a Χ2-test for sex. Full details on these group comparisons are reported in Table 1.
Imaging data
We directly compared the connectivity of the right and left DLPFC between stroke participants showing depressive features (DEP) and those who did not (NONDEP). We also performed a whole-brain regression analysis of DLPFC connectivity with PHQ-9 scores, controlling for age, gender and baseline NIHSS scores in all participants. The threshold of voxel-wise p < 0.001 corrected for multiple comparisons at the cluster level pFDR < 0.05 was used for assessing statistical significance of results.
Results
Behavioural results
The first 64 participants in the CANVAS study who completed assessment at 3 months and had a full set of imaging data and depression scores available were included in the analysis. On average, subjects in this study had a stroke of minor severity, as is evident in the baseline NIHSS scores (median = 2, range 0–10). At 3 months, when depression was measured, median NIHSS score was 0 (range 0–5): i.e., no stroke symptoms. Twenty participants presented with mild-to-moderate depressive features (DEP, PHQ-9 score of above 5) at 3 months. This equated to an expected 30% prevalence rate. Forty-four participants had the score of less than 5 and were considered ‘non-depressed’ (NONDEP). The groups were not different on age or NIHSS baseline scores—see Table 1. Stroke participants in our sample presented with minor stroke, as assessed by the NIHSS. There were significantly more women in the DEP group compared to the NONDEP group (see Table 1). This is consistent with previous literature32. The groups were also not different in their performance on several cognitive tests, including the Boston naming test, Digit Span test, Hopkins Verbal Learning test, Star cancellation test, Complex figure test (copy), Complex figure test (recall), see Table 1.
rs-fMRI group comparison at 3 months
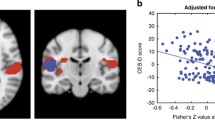
Using the right DLPFC seed, no significant differences in connectivity were observed between groups. Using the left DLPFC seed, significantly lower connectivity with a cluster (k = 103) in the right supramarginal gyrus (SMG) was observed in the DEP group (cluster centre (MNI:+66, −24, 15) voxel-wise p = 0.001, cluster-corrected pFDR = 0.007). Figure 2 shows the significant cluster in red. In addition, we found that the groups did not differ in TIV, as well as in the extent of WMHs.

Lesion overlap in all stroke participants N = 64 shown in cyan. A cluster in the right supramarginal gyrus (MNI: + 66, −24, 15; p = 0.001, cluster-corrected pFDR = 0.007, k = 103) shows lower connectivity of the left DLPFC in a direct comparison between the DEP (N = 20) vs. NONDEP (N = 44) participants (shown in red); shown in blue is a negative association between the connectivity of the left DLPFC and right supramarginal gyrus with the PHQ-9 scores at 3 months in all subjects (MNI: 57, −21, 21, p < 0.001, cluster-corrected at pFDR = 0.01, k = 110); shown in purple is an overlap between the group results and the regression results
Assessing depression severity in all participants
We also performed a regression analysis with the PHQ-9 score for all 64 participants, regardless of depressive feature status, controlling for age, gender, and baseline NIHSS for the left and right DLPFC seeds separately. Higher PHQ-9 scores at 3 months were associated with lower connectivity between the left DLPFC and the right SMG (cluster centre (MNI: 57, −21, 21) significant at the voxel level p < 0.001, cluster-corrected at pFDR = 0.01, k = 110). Figure 2 shows the cluster in blue; note the overlap between the group and correlation results in purple.
Overlap with stroke lesions
No overlap between the stroke lesions and the right DLPFC seed was observed. One participant presented with a lesion in the left DLPFC overlapping with the seed. This particular participant had a PHQ-9 score of 6, placing them in the DEP (‘mild’ depression based on the PHQ-9 severity scale) group. Removing this participant’s data from all analyses did not change the results. The cluster in the right SMG observed in both correlation and group comparison results did not overlap with lesions in any subject (Fig. 2). Lesion volume did not significantly differ between groups (Table 1).
Discussion
We investigated the CCN connectivity in participants with and without depressive features at 3 months post stroke and found that left DLPFC–right SMG connectivity was lower in DEP subjects compared to the NONDEP group. Importantly, the connectivity values negatively correlated with depressive feature severity in all participants at 3 months.
Specifically left-lateralised DLPFC connectivity in post-stroke depression
On the one hand, evidence from prior lesion studies attested to the crucial role of the left DLFPC in post-stroke depression8,33, especially depression characterised by cognitive impairment34. On the other hand, findings from non-stroke populations demonstrated aberrant connectivity of the DLPFC and the CCN in depression19,20,35,36. The results of our study provide a bridge between these previous findings, demonstrating that even in the absence of lesions in the left DLPFC, stroke participants can experience depressive symptoms related to lower DLPFC connectivity with the SMG. These results are also consistent with our recent report of aberrant low-frequency fluctuations specifically in the left DLPFC in post-stroke depression37.
Lower connectivity at 3 months post stroke in the left, but not in the right, DLPFC represents additional evidence for using left DLPFC over right DLPFC as a target for clinical interventions, for instance, in non-invasive brain stimulation. In fact, in non-stroke participants, the left DLPFC has already been a preferred target for transcranial magnetic stimulation as a treatment of depression, although the efficacy was shown to depend on the exact location and potential functional connectivity with the subgenual anterior cingulate cortex38. The left DLPFC has also been a target for transcranial direct current stimulation, specifically aimed at ameliorating cognitive control in depression39. Based on the relevance of the left DLPFC connectivity to the severity of post-stroke depression in our study, we speculate that the left DLPFC might be a suitable target for neuromodulation in post-stroke depression.
Sensitivity to mild post-stroke depression
Lower resting-state CCN connectivity found to correlate with depressive feature severity in this study could be a sensitive biomarker of even mild post-stroke depression. Most subjects in our DEP group endorsed features of only mild-to-moderate depression. Lower DLPFC–SMG connectivity using the same DLPFC seed has been previously reported in subjects with subthreshold depression compared to healthy controls, albeit using bilateral seeds20. In the study by Hwang et al., the depressed vs. non-depressed group comparison of DLPFC connectivity revealed a bilateral SMG cluster overlapping with the right SMG cluster reported here. The depression severity regression in their study, however, showed a left-lateralised SMG, unlike our right SMG result. Taken together, the results of both studies suggest that DLPFC connectivity to both left and right SMG could be important in mild depression, with the laterality differences likely explained by the use of the bilateral vs. left DLPFC seed.
Reported CCN connectivity differences have been observed, despite no significant differences in the level of cognitive performance between groups. Previous studies, such as those in Alzheimer’s disease, showed that brain changes often precede behavioural cognitive decline40. Given that changes in CCN connectivity were sensitive to relatively mild depressive symptoms, future studies could investigate feasibility of using CCN connectivity for predicting cognitive decline in depressed stroke participants.
DLPFC–SMG connectivity
Cognitive dysfunction in depression has been described in terms of both cognitive biases, such as fixation on negative information41, as well as impaired general executive functions; e.g., deficits in cognitive control that prevent depressed patients from overcoming maladaptive biases. CCN is known to be critically involved in top–down modulation of attention and working memory and comprises the lateral prefrontal and inferior parietal cortices42. Little is known how the interaction between these regions emerges to produce higher cognitive function. It is likely shaped by both the underlying physical neuroanatomical connections between frontal and parietal areas (structural connectivity) and by correlated activity in distinct distant regions (functional connectivity). The DLPFC is an important node of this network, frequently used to derive the functional CCN in resting-state studies, and was therefore used as a seed here. The SMG is located at the border of the parietal and temporal cortices, and together with the angular gyrus forms the temporoparietal junction, which has been shown to be involved in memory, language, attention and social processing43. The DLPFC is known to have long-range structural connections with the parietal cortex, and the SMG in particular44. Equally, both DLPFC and SMG are highly connected functionally. For example, the right SMG and lower DLPFC–rSMG connectivity have been previously linked to egocentricity45,46 that can be related to self-focus observed in depression, and to depression in general20,47. The patterns of intrinsic connectivity of the temporoparietal junction (including to the DLPFC) reveal connections to salience, attention and social networks48. Therefore, the DLPFC–SMG connectivity could be particularly vulnerable to depression. Both DLPFC and temporoparietal junction represent so-called ‘rich-club’ nodes in the brain network organisation, and are postulated as being affected following stroke49.
Limitations
The main limitation of our study is that correlation analyses between depression and functional connectivity cannot reveal the direction of influence of each factor. We cannot resolve whether disruption of the CCN connectivity following stroke causes depressive features, or whether depressive features result in the decrease in connectivity within the network. Future studies should investigate causal relationships between depression and connectivity.
In addition, depression correlates of post-stroke depression have been shown to change over time11,50. Here we present resting-state correlates of depressive features at only one time point, 3 months post stroke. However, this time point represents an early period post stroke. Resting-state markers in later post-stroke stages should be further explored to understand the disorder trajectory relative to the CCN state.
Summary
We examined the resting-state connectivity of the CCN in a stroke population with depressive features, compared to those without. We show that lower connectivity between the left DLPFC and the right SMG is associated with post-stroke depressive features. While the left DLPFC has been previously associated with cognitive impairment in depression in several lesion-symptom mapping studies, we now show that post-stroke depressive features are associated with a network connectivity problem, without necessarily involving a stroke lesion in DLPFC. We provide new clues about what represents a CCN resting connectivity marker in stroke participants with and without depressive features.
References
Papakostas, G. I. Cognitive symptoms in patients with major depressive disorder and their implications for clinical practice. J. Clin. Psychiatry 75, 8–14 (2014).
Gotlib, I. H. & Joormann, J. Cognition and depression: current status and future directions. Annu. Rev. Clin. Psychol. 6, 285–312 (2010).
Hackett, M. L., Yapa, C., Parag, V. & Anderson, C. S. Frequency of depression after stroke: a systematic review of observational studies. Stroke 36, 1330–1340 (2005).
Robinson, R. G. & Spalletta, G. Poststroke depression: a review. Can. J. Psychiatry 55, 341–349 (2010).
Loubinoux, I. et al. Post-stroke depression: mechanisms, translation and therapy. J. Cell Mol. Med. 16, 1961–1969 (2012).
Metoki, N. et al. Relationship between the lesion location of acute ischemic stroke and early depressive symptoms in Japanese patients. Ann. Gen. Psychiatry 15, 12 (2016).
Starkstein, S. E. & Robinson, R. G. Affective disorders and cerebral vascular disease. Br. J. Psychiatry 154, 170–182 (1989).
Grajny, K. et al. Depression symptoms in chronic left hemisphere stroke are related to dorsolateral prefrontal cortex damage. J. Neuropsychiatry Clin. Neurosci. 28, 292–298 (2016).
Hama, S. et al. Post-stroke affective or apathetic depression and lesion location: left frontal lobe and bilateral basal ganglia. Eur. Arch. Psychiatry Clin. Neurosci. 257, 149–152 (2007).
Wei, N. et al. Post-stroke depression and lesion location: a systematic review. J. Neurol. 262, 81–90 (2015).
Shimoda, K. & Robinson, R. G. The relationship between poststroke depression and lesion location in long-term follow-up. Biol. Psychiatry 45, 187–192 (1999).
Corbetta, M. Functional connectivity and neurological recovery. Dev. Psychobiol. 54, 239–253 (2012).
Siegel, J. S. et al. Disruptions of network connectivity predict impairment in multiple behavioral domains after stroke. Proc. Natl Acad. Sci. USA https://doi.org/10.1073/pnas.1521083113 (2016).
Carter, A. R., Shulman, G. L. & Corbetta, M. Why use a connectivity-based approach to study stroke and recovery of function? Neuroimage 62, 2271–2280 (2012).
Lassalle-Lagadec, S. et al. Subactute default mode network dysfunction in the prediction of post-stroke depression severity. Radiology 264, 218–224 (2012).
Liu, J. et al. Altered spontaneous activity in the default-mode network and cognitive decline in chronic subcortical stroke. J. Neurol. Sci. 347, 193–198 (2014).
Zhang, P., et al. Dysfunction of affective network in post ischemic stroke depression: a resting-state functional magnetic resonance imaging study. Biomed. Res. Int. 2014, 846830 (2014). http://doi:org/10.1155/2014/846830
Cole, M. W. & Schneider, W. The cognitive control network: integrated cortical regions with dissociable functions. Neuroimage 37, 343–360 (2007).
Sheline, Y. I., Price, J. L., Yan, Z. & Mintun, M. A. Resting-state functional MRI in depression unmasks increased connectivity between networks via the dorsal nexus. Proc. Natl Acad. Sci. USA 107, 11020–11025 (2010).
Hwang, J. W. et al. Subthreshold depression is associated with impaired resting-state functional connectivity of the cognitive control network. Transl. Psychiatry 5, e683 (2015).
Brodtmann, A. et al. Charting cognitive and volumetric trajectories after stroke: protocol for the Cognition and Neocortical Volume After Stroke (CANVAS) study. Int. J. Stroke 9, 824–828 (2014).
Kroenke, K., Spitzer, R. L. & Williams, J. B. W. The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613 (2001).
Williams, L. S. et al. Performance of the PHQ-9 as a screening tool for depression after stroke. Stroke. 36, 635–638 (2005).
Robinson, R. G. & Jorge, R. E. Post-stroke depression: a review. Am. J. Psychiatry 173, 221–231 (2016).
Rorden, C., Bonilha, L., Fridriksson, J., Bender, B. & Karnath, H.-O. Age-specific CT and MRI templates for spatial normalization christopher. Neuroimage 61, 957–965 (2012).
DeCarli, C., Fletcher, E., Ramey, V., Harvey, D. & Jagust, W. J. Anatomical mapping of white matter hyperintensities (WMH): exploring the relationships between periventricular WMH, deep WMH, and total WMH burden. Stroke 36, 50–55 (2005).
Maldjian, J. A., Laurienti, P. J., Kraft, R. A. & Burdette, J. H. An automated method for neuroanatomic and cytoarchitectonic atlas-based interrogation of fMRI data sets. Neuroimage 19, 1233–1239 (2003).
Rorden, C., Karnath, H.-O. & Bonilha, L. Improving lesion-symptom mapping. J. Cogn. Neurosci. 19, 1081–1088 (2007).
Taylor, W. D. et al. White matter hyperintensity progression and late-life depression outcomes. Arch. Gen. Psychiatry 60, 1090–1096 (2003).
Stebbins, G. T. et al. Gray matter atrophy in patients with ischemic stroke with cognitive impairment. Stroke 39, 785–793 (2008).
Werden, E. et al. Structural MRI markers of brain aging early after ischemic stroke. Neurology 89, 116–124 (2017).
Paradiso, S. & Robinson, R. G. Gender differences in poststroke depression. J. Neuropsychiatry Clin. Neurosci. 10, 41–47 (1998).
Rajashekaran, P., Pai, K., Thunga, R. & Unnikrishnan, B. Post-stroke depression and lesion location: a hospital based cross-sectional study. Indian J. Psychiatry 55, 343–348 (2013).
Downhill, J. E. & Robinson, R. G. Longitudinal assessment of depression ad cognitive impairment following stroke. J. Nerv. Ment. Dis. 182, 425–431 (1994).
Alexopoulos, G. S. et al. Functional connectivity in the cognitive control network and the default mode network in late-life depression. J. Affect. Disord. 139, 56–65 (2012).
Kaiser, R. H, Andrews-Hanna, J. R., Wager, T. D., Pizzagalli, D. A. Large-scale network dysfunction in major depressive disorder: a meta-analysis of resting-state functional connectivity. JAMA Psychiatry 72, 603–611 (2015). http://doi.org/10.1001/jamapsychiatry.2015.0071
Egorova, N., Veldsman, M., Cumming, T. & Brodtmann, A. Fractional amplitude of low-frequency fluctuations (fALFF) in post-stroke depression. NeuroImage Clin. 16, 116–124 (2017).
Fox, M. D., Buckner, R. L., White, M. P., Greicius, M. D. & Pascual-Leone, A. Efficacy of transcranial magnetic stimulation targets for depression is related to intrinsic functional connectivity with the subgenual cingulate. Biol. Psychiatry 72, 595–603 (2012).
Wolkenstein, L. & Plewnia, C. Amelioration of cognitive control in depression by transcranial direct current stimulation. Biol. Psychiatry 73, 646–651 (2013).
Burggren, A. & Brown, J. Imaging markers of structural and functional brain changes that precede cognitive symptoms in risk for Alzheimer’s disease. Biophys. Chem. 8, 251–261 (2014).
Joormann, J. & Quinn, M. E. Cognitive processes and emotion regulation in depression. Depress. Anxiety 31, 308–315 (2014).
Vincent, J. L., Kahn, I., Snyder, A. Z., Raichle, M. E. & Buckner, R. L. Evidence for a frontoparietal control system revealed by intrinsic functional connectivity. J. Neurophysiol. 100, 3328–3342 (2008).
Carter, R. M. & Huettel, S. A nexus model of the temporal-parietal junction. Trends Cogn. Sci. 17, 328–336 (2013).
Jung, J. Y., Cloutman, L. L., Binney, R. J. & Lambon Ralph, M. A. The structural connectivity of higher order association cortices reflects human functional brain networks. Cortex, https://doi.org/https://doi.org/10.1016/j.cortex.2016.08.011 (2016).
Steinbeis, N., Bernhardt, B. C. & Singer, T. Age-related differences in function and structure of rSMG and reduced functional connectivity with DLPFC explains heightened emotional egocentricity bias in childhood. Soc. Cogn. Affect. Neurosci. 10, 302–310 (2015).
Silani, G., Lamm, C., Ruff, C. C. & Singer, T. Right supramarginal gyrus is crucial to overcome emotional egocentricity bias in social judgments. J. Neurosci. 33, 15466–15476 (2013).
Buchanan, A., Wang, X. & Gollan, J. K. Resting-state functional connectivity in women with major depressive disorder. J. Psychiatr. Res. 59, 38–44 (2014).
Kucyi, A., Hodaie, M. & Davis, K. D. Lateralization in intrinsic functional connectivity of the temporoparietal junction with salience- and attention-related brain networks. J. Neurophysiol. https://doi.org/10.1152/jn.00674.2012 (2012).
Lim, J. & Kang, D. Stroke connectome and its implications for cognitive and behavioral sequela of stroke. J. Stroke 17, 256–267 (2015).
Yamaguchi, S., Kobayashi, S., Koide, H. & Tsunematsu, T. Longitudinal study of regional cerebral blood flow changes in depression after stroke. Stroke 23, 1716–1722 (1992).
Acknowledgements
This work was supported by the National Health and Medical Research Council project grant number APP1020526, the Brain Foundation, Wicking Trust, Collie Trust, and Sidney and Fiona Myer Family Foundation.
Author information
Authors and Affiliations
Contributions
N.E., T.C., C.S., M.V., E.W., A.B.—study concept and design; N.E.—analysis, manuscript and figure preparation; N.E., T.C., C.S., M.V., E.W., A.B.—interpretation and critical revision of the manuscript for important intellectual content; A.B.—study supervision.
Corresponding authors
Ethics declarations
Competing interests
The authors declare that they have no competing financial interest.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Egorova, N., Cumming, T., Shirbin, C. et al. Lower cognitive control network connectivity in stroke participants with depressive features. Transl Psychiatry 7, 4 (2017). https://doi.org/10.1038/s41398-017-0038-x
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41398-017-0038-x
- Springer Nature Limited
This article is cited by
-
Post-Stroke Depression in Older Adults: An Overview
Drugs & Aging (2024)
-
Artificially-reconstructed brain images with stroke lesions from non-imaging data: modeling in categorized patients based on lesion occurrence and sparsity
Scientific Reports (2022)
-
Lesions in the right Rolandic operculum are associated with self-rating affective and apathetic depressive symptoms for post-stroke patients
Scientific Reports (2020)