
Abstract
Introduction Dental implants are a predictable prosthetic option for replacement of missing teeth with good survival rates. Peri-implant diseases are the main reason for implant failure by causing bone loss around the implant leading to implant loss. General dental practitioners see patients with dental implants routinely and therefore, awareness of risk factors for peri-implant disease and early diagnosis is essential for appropriate management. The aim of this study is to assess the awareness of general dental practitioners in diagnosing peri-implantitis, with a view to identify any potential training needs.
Design, setting, materials and methods A quantitative study method was designed using an online questionnaire sent to closed social media groups in the UK. The significance level was taken as p <0.05. The chi-squared tests and Kruskal-Wallis tests were used with IBM SPSS software. Descriptive statistical analysis of data was also done.
Results and conclusion A total of 224 responses were received. The results show that there is lack of awareness of diagnostic criteria of peri-implantitis among general dental practitioners. However, majority of practitioners are aware of the legal implications of failing to diagnose this condition. There is a perceived need for more undergraduate training in diagnosing peri-implant diseases.
Key points
-
The available evidence suggests peri-implant diseases are the main reason for implant failure by causing bone loss around the implant leading to implant loss.
-
This questionnaire study aimed aim to assess the awareness of general dental practitioners in diagnosing peri-implantitis, with a view to identify any potential training needs.
-
This study has brought into light the lack of knowledge among general dental practitioners regarding the formal diagnostic criteria of peri-implantitis. A minority of practitioners do not probe around implants or specifically examine implants during a routine examination, which is a concern. This study reinforces that further CPD courses by education providers are needed in the diagnostic criteria, appropriate implant referral situations and risk factors of peri-implantitis in order to optimise patient care.
Similar content being viewed by others

Introduction
Implants are an ever-increasing treatment option for replacement of missing teeth. Implants generally have a high success rate of about 94.9% over ten years.1 However, peri-implantitis (PI) and peri-implant mucositis are pathological conditions affecting tissues around implants which can result in their failure. PI is characterised by inflammation in the peri-implant connective tissue and progressive loss of supporting bone which, if untreated, may result in implant failure.2 Although a study by Jemt et al.3 showed that there was no difference between patients with PI having surgical treatment and patients who were in the at-risk group and untreated, the ‘at-risk' group was not specified in that why they were at risk, whether they were diagnosed with PI and not treated, or just at risk of PI due to systemic or local conditions. In any case, it is important to be able to diagnose PI in order to then decide on the appropriate treatment. Studies have reported a prevalence of up to 22% for PI (ranging between 1-47%).4 A recent retrospective analysis showed that one in five implants showed signs of PI over time;5 however, Marcantonio et al. (2015)6 suggests a prevalence range of 4.7-43% at implant level and 8.9-56% at patient level. A systematic review and meta-analysis by Rakic et al.7 estimated the prevalence of PI to be 18.5% at patient level and 12.8% at implant level. There is a wide range quoted for the prevalence of PI in the literature. This is partly due to the varying diagnostic criteria used by different groups. However, since the consensus report,8 there is a consensus agreement on the diagnostic criteria for PI.
The main risk factors for PI are poor plaque control, periodontitis, systemic diseases and soft tissue defects.9 Diagnosis of PI requires measuring of probing depth, bleeding on probing and radiographic examination to analyse bone loss.10 Correct diagnosis of PI is critical for the appropriate clinical management of the condition.11 The studies in specialist settings have acknowledged the role of general dental practitioners (GDPs) in diagnosis, referral and long-term management of this condition.12 Knowledge of signs and symptoms of PI and peri-implant mucositis will ensure that patients are regularly monitored by their GDPs and recall regimes arranged to suit individual patients. The early diagnosis of PI and awareness of the risk factors will also help in successful treatment outcomes.13
Implant complications and periodontitis management and diagnosis form the majority of high-value claims settled by defence organisations. The average amount paid to claimants in cases of implant failures to settle the claim is around £30,000 as per the Dental Defence Union.14 Dental protection revealed that, in 2015, implant-associated claims account for the second highest after periodontal diseases, and post-treatment maintenance is a factor in these claims.15
There are limited studies in the literature regarding the awareness of GDPs to PI and its risk factors. Togashi et al.16 did a questionnaire study in Brazil, the results of which showed a lack of knowledge among dentists regarding PI, whereas Tripathi et al.17 cites increased awareness among dental practitioners in India. There is lack of studies specific to the UK that looks into the knowledge and awareness of general GDPs regarding diagnosing PI.
A survey of undergraduate dental implant teaching in UK dental schools18 found that it is important to ensure that newly qualified dentists are competent in clinical assessment of peri-implant health and preventing peri-implant diseases. The aim of this study was to analyse the awareness of PI among UK GDPs through a questionnaire study.
Materials and methods
An online questionnaire survey was devised to test the knowledge of GDPs on PI. The questionnaire survey is presented in the online Supplementary Information. The survey was peer-reviewed by the dental school faculty in Implantology. Ethical committee approval was obtained from the University of Central Lancashire Ethics Committee (HEALTH 0207) and the questionnaire was released on closed professional social media groups and was available for the GDPs for up to four months. The study included GDPs who practise within the UK and foundation dentists. Undergraduate students and dentists practising outside the UK were excluded. The responses were stored in secure, password-protected computer system. The GDPR regulations were fully complied in this study. Consent was obtained from participants and the design of the survey ensured their complete anonymity.
The null hypothesis assumed that there is no difference in the knowledge of diagnostic criteria and risk factors based on the number of years post-qualification experience. The significance level was taken as p <0.05 (Table 1). The chi-squared tests and Kruskal-Wallis tests were used with IBM SPSS software.
Results
There were 224 responses in total. Results of this study was reported using the RISQ (Reporting Items for Surveys and Questionnaires) guidelines.19 There was more or less equal distribution of participants with post-qualification experience, of which 32.7% have been practising between 0-10 years, 32.7% have been practising for 11-20 years, and 34.5% having >20 years' experience (Table 2). The oldest year of qualification was 1981 and the most recent graduate qualified in 2022. England accounted for 86% of the participants, followed by Scotland (8%), Wales (4%) and Northern Ireland (2%). The majority of participants worked in an NHS or mixed practice setting (62%), followed by a fully private (25%) setting. A hospital and university setting accounted for 8% and 4% of participants, respectively.
Of the overall respondents, 66.5% reported that they had no prior training in implants, whereas 33.5% responded positively to having had prior training. Of those who had prior training, 16.9% had a continuing professional development (CPD) certificate course, 14.4% had a Master's degree-level of training, 11.9% attended a post-graduate certificate course, and 6.8% had a postgraduate diploma. The majority of the participants (68%) were not involved in restoring or placing implants, whereas 32% of GDPs responded that they are either restoring or placing implants. Also, 14% of the respondents admitted that they do not examine dental implants routinely during check-up. This is concerning, since probing depth measurements are important in identifying implant failures.20 Additionally, 13% of participants do not probe around the implant. Probing around the implant is one of the main recommendations of the Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions.8 It recommends gentle probing to detect bleeding and measuring pocket depth so as to alert the clinician to potential peri-implant disease. Lack of probing will lead to underdiagnosing or missing an early sign of PI. The participants' fear of causing damage to the implant surface was cited as one of the main reasons for not probing around an implant, together with the potential medicolegal consequences (Table 3). A survey by Dental Protection has shown that nine out of ten dentists are fearful of being sued by patients.21 In total, 66% of respondents believe that they will be legally liable if their patients developed PI even if they did not carry out the treatment. Despite this, 13% do not probe and 14% do not examine the implant at all. This may reflect the lack of confidence in how to examine an implant correctly.22 Furthermore, 77% responded that they will refer patients if they suspect PI, while 23% would not. A total of 85% of the participants responded that they did not have any undergraduate training on PI.
Statistical results
The level of post-qualification experience years was compared against appropriate implant referral scenarios and the respondent's awareness of risk factors for PI. The Kruskal-Wallis test was applied to compare the difference in correct and incorrect responses. The results showed a statistically significant difference between the post-qualification experience groups in responses to the question on specific diagnostic criteria of PI. The group which had the maximum correct responses were in the 11-20-year post-qualification experience group. The Kruskal-Wallis test was applied to the results (Table 4 and 5) which showed a significantly higher familiarity in diagnostic criteria of PI in the group with more post-qualification experience, thus rejecting the null hypothesis.
Question 15 tested appropriate scenarios for implant treatment. Question 19 tested the major factors that predispose to PI: the correct answers for Question 19 are active periodontitis, not attending regular maintenance therapy and poor oral hygiene. Question 20 tested the diagnostic criteria for PI.
Prior training in implants was compared against familiarity with formal diagnostic criteria for PI and peri-implant mucositis. The results of chi-squared tests revealed that there is significant difference in familiarity of diagnostic criteria between those with prior training and ones who did not have training, with the group which had prior training showing more familiarity with diagnostic criteria of PI (see online Supplementary Information).
Discussion
The participants were in complete agreement (100%) regarding the need for training in implant referral criteria, and 99% agreed PI should be taught at undergraduate level. It is well-understood that appropriate implant training can help in preventing and managing complications and medicolegal consequences.23 A review of post-graduate implant study in the UK revealed that there were eight courses that offered training to a Master's degree level and eight courses that offered a diploma-level training.24 The review identified 13 CPD courses, of which two were certificate-only courses that did not provide any verifiable CPD. All the Master's and diploma-level courses complied with the Faculty of General Dental Practice guidelines on Training standards in implant dentistry; however, the same could not be confirmed for the CPD-only courses.
In total, 85% stated that they did not have any training in PI in the undergraduate curriculum. Some of the perceived barriers to incorporating PI in the undergraduate curricula include training of suitable staff, recruitment of patients and increased costs.25 An earlier survey of UK and Irish dental schools in 2008 revealed that even though a high percentage of schools (87%) provided implant education to undergraduates, only 46% gained experience in treatment planning for implants and observation of implant restoration.26 This survey did not identify a specific clinical training being given to undergraduates for peri-implant diagnosis and management.
The General Dental Council (GDC) document Preparing for practice - dental team learning outcomes for registration specifies that the registrants must be able to give implant treatment options, explain risks and be competent at maintaining peri-implant health.27 The GDC advice for undergraduate curriculum states that dental students should be able to see dental implants being maintained in a healthy state in tissues.28 Without training in diagnosis of peri-implant disease, this learning outcome will be difficult to achieve for undergraduate students. The comments provided by respondents show that there is an urgent need for CPD courses that specifically train in preventing, diagnosing and providing treatment options for PI.
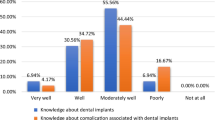
A total of 68.3% of the respondents did not have knowledge of the diagnostic criteria for PI, which may result in supervised neglect, or late referral and management. However, the majority of respondents (190) associate bleeding on probing with PI, which is one of the diagnostic criteria of peri-implant diseases; however, spot bleeding on probing can be due to probing causing minor trauma and alone is not indicative of disease. There was also a high number of responses to the other choices, especially correct probing depth (6 mm or more) and bone level (Fig. 1 - the correct answers are a, d and f).

GDP responses to diagnostic criteria for PI (a = presence of bleeding/suppuration on gentle probing; b = increased probing depth compared to previous examination; c = probing depth greater than or equal to 4 mm in the absence of previous examination data; d = probing depth greater than or equal to 6 mm in the absence of previous examination data; e = loosening of the abutment; f = bone loss of 3 mm or more from the neck [coronal margin] of the implant)
The survey also explored awareness of risk factors PI among GDPs (Table 6). Here, 94.2% selected periodontitis as one of the risk factors of PI. Poor oral hygiene was also selected as a risk factor by a high proportion of participants (94.6%). This shows that the participants are aware of the role of plaque in initiating this condition since plaque is an important aetiological risk factor. Smoking and uncontrolled diabetes were selected as risk factors by majority of participants (94.2% and 93.8%, respectively), although the evidence for these as risk factors is inconclusive.8 The Consensus report of the World Workshop on Periodontology and Implantology in 2017 set specific agreed diagnostic criteria and definitions of peri-implant diseases.8
Of the respondents, 77% agreed that they routinely refer patients if PI was suspected and 23% would not refer. The British Society of Periodontology and Implant Dentistry (BSP) has given guidelines regarding the referral pathway to be followed in PI patients.29 As per the BSP guidelines, peri-implant mucositis falls within Level 2 complexity and the advice is to treat it in general practice or to do a referral to specialist. PI however falls in the Level 3 complexity and BSP advices a referral after completing non-surgical treatment and addressing the risk factors in general practice. There need to be increased awareness that peri-implant disease can also be caused by the way the implant is restored. A study comparing association of restoration emergence angle and restoration profile with PI concluded that an emergence angle of >30 degrees is a significant risk factor for PI. This study also concluded convex profile is a risk factor for bone-level implants but not for tissue-level implants.30
This study elicited responses from a wide spectrum of GDPs in different regions and practice settings across the UK, which is one of the strengths. However, it may have limitations, such as sampling error and non-response error, as the study was released only on social media, which could have had an effect on the results.31
Conclusions
This study has brought into light the lack of knowledge among GDPs regarding the formal diagnostic criteria of PI, which varied across the post-qualification experience groups. People with previous implant training had more familiarity with the diagnostic criteria. Practitioners in the mid of their career (10-20 years) had more awareness of diagnostic criteria than practitioners with less than ten years' experience and ones with more than 20 years' experience. However, there was no difference between the groups with respect to recognising risk factors for PI or implant referral criteria. A minority of practitioners (13%) do not probe around implants or specifically examine implants during a routine examination, which is a concern. The majority of practitioners are aware of the legal implications if PI is not diagnosed and recognise that more training is required at undergraduate and post-graduate levels in diagnosing peri-implant diseases. This study reinforces that further CPD courses by education providers are needed in the diagnostic criteria, appropriate implant referral situations and risk factors of PI in order to optimise patient care. It also points out that there is a need for undergraduate training in diagnosing peri-implant diseases.
References
Albrektsson T, Donos N. Implant survival and complications. The Third EAO consensus conference 2012. Clin Oral Implants Res 2012; 23: 63-65.
Schwarz F, Derks J, Monje A, Wang H-L. Peri-implantitis. J Periodontol 2018; 89: 267-290.
Jemt T, Eriksson J. Implant failures before and after peri-implantitis surgery: a retrospective study on 207 consecutively treated patients. Clin Implant Dent Relat Res 2020; 22: 567-573.
Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol 2015; 42: 158-171.
Kordbacheh Changi K, Finkelstein J, Papapanou P N. Peri-implantitis prevalence, incidence rate, and risk factors: A study of electronic health records at a US dental school. Clin Oral Implants Res 2019; 30: 306-314.
Marcantonio C, Nicoli L G, Marcantonio Junior E, Zandim-Barcelos D L. Prevalence and possible risk factors of peri-implantitis: a concept review. J Contemp Dent Pract 2015; 16: 750-757.
Rakic M, Galindo-Moreno P, Monje A et al. How frequent does peri-implantitis occur? A systematic review and meta-analysis. Clin Oral Investig 2018; 22: 1805-1816.
Berglundh T, Armitage G, Araujo M G et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol 2018; 45: 286-291.
Smeets R, Henningsen A, Jung O, Heiland M, Hammächer C, Stein J M. Definition, aetiology, prevention and treatment of peri-implantitis - a review. Head Face Med 2014; 10: 34.
Padial-Molina M, Suarez F, Rios H F, Galindo-Moreno P, Wang H-L. Guidelines for the diagnosis and treatment of peri-implant diseases. Int J Periodontics Restorative Dent 2014; 34: 102-111.
Heitz-Mayfield L J. Peri-implant diseases: diagnosis and risk indicators. J Clin Periodontol 2008; 35: 292-304.
Russell A A, Tawse-Smith A, Broadbent J M, Leichter J W. Peri-implantitis diagnosis and treatment by New Zealand periodontists and oral maxillofacial surgeons. N Z Dent J 2014; 110: 6-10.
De Waal Y C, Raghoebar G M, Meijer H J, Winkel E G, van Winkelhoff A J. Prognostic indicators for surgical peri-implantitis treatment. Clin Oral Implants Res 2016; 27: 1485-1491.
Briggs L. Closing the gap. 2015. Available at https://ddujournal.theddu.com/issue-archive/issue-1/closing-the-gap (accessed October 2020).
Chin J S. Maintaining Peri-Implant Health: An Evaluation of Understanding Among Dental Professionals. 2018. Cardiff: Cardiff University, 2018. MPhil Thesis.
Togashi A Y, Carmelo R A, Pereira N C. Level of knowledge of dentists about the diagnosis and treatment of peri-implantitis. Dent Press Implantol 2014; 8.
Tripathi R, Vasudevan S, Palle A R, Gedela R K, Punj A, Vaishnavi V. Awareness and management of peri-implantitis and peri-mucositis among private dental practitioners in Hyderabad - A cross-sectional study. J Indian Soc Periodontol 2020; 24: 461-466.
Chin J S, Lynch C D, Rees J, Locke M, Thomas M B, Addy L D. Teaching of implant dentistry in undergraduate dental schools in the UK and Ireland. Br Dent J 2018; 225: 763-768.
Shelley A, Horner K. Questionnaire surveys - sources of error and implications for design, reporting and appraisal. Br Dent J 2021; 230: 251-258.
Park S-H, Wang H-L. Implant reversible complications: classification and treatments. Implant Dent 2005; 14: 211-220.
Dental Protection. Dental Protection survey reveals 9 in 10 dentists fear being sued by patients. 2018. Available at https://www.dentalprotection.org/uk/articles/dental-protection-survey-reveals-9-in-10-dentists-fear-being-sued-by-patients (accessed May 2022).
Barrak F, Caga D, Crean S. What every dental practitioner should know about how to examine patients with dental implants. Br Dent J 2023; 234: 309-314.
Wheeler S, Bollinger C M. Complication or substandard care? Risks of inadequate implant training. J Calif Dent Assoc 2009; 37: 647-651.
Kim N Y, Stagnell S. Postgraduate education in dental implantology in the United Kingdom: a review. Int J Implant Dent 2018; 4: 8.
McAndrew R, Ellis J, Lynch C D, Thomason M. Embedding implants in undergraduate dental education. Br Dent J 2010; 208: 9-10.
Addy L D, Lynch C D, Locke M, Watts A, Gilmour A S. The teaching of implant dentistry in undergraduate dental schools in the United Kingdom and Ireland. Br Dent J 2008; 205: 609-614.
General Dental Council. Preparing for Practice. 2015. Available at https://www.gdc-uk.org/docs/default-source/quality-assurance/preparing-for-practice-(revised-2015).pdf?sfvrsn=81d58c49_2 (accessed February 2024).
General Dental Council. The First Five Years - A Framework for Undergraduate Dental Education. 2nd ed. London: General Dental Council, 2002.
British Society of Periodontology and Implant Dentistry. BSP guidelines for periodontal patient referral. 2020. Available at https://www.bsperio.org.uk/assets/downloads/BSP_Guidelines_for_Patient_Referral_2020.pdf (accessed May 2022).
Katafuchi M, Weinstein B F, Leroux B G, Chen Y-W, Daubert D M. Restoration contour is a risk indicator for peri-implantitis: a cross-sectional radiographic analysis. J Clin Periodontol 2018; 45: 225-232.
Hoonakker P, Carayon P. Questionnaire survey nonresponse: A comparison of postal mail and internet surveys. Int J Hum Comput Interact 2009; 25: 348-373.
Author information
Authors and Affiliations
Contributions
Sonu Thomas and Fadi Barrak conceived the original concept and designed the study. Fadi Barrak supervised the project. Sonu Thomas designed the survey questionnaire with contributions from Fadi Barrak; obtained ethical clearance from the University of Central Lancashire Ethics team; carried out the survey and collected the data; analysed the data and obtained the results under the supervision of Fadi Barrak; drafted the manuscript; and designed the figures and tables. Both Fadi Barrak and Sonu Thomas contributed to the final version of the manuscript.
Corresponding author
Ethics declarations
Ethical committee approval was obtained from the University of Central Lancashire Ethics Committee (HEALTH 0207).
Consent was obtained from participants and the design of the survey ensured their complete anonymity.
Data availability
The data that support the findings of this study are available on request from the corresponding author Sonu Thomas. The data are not publicly available due to information it may contain which could compromise the anonymity of research participants.
Supplementary Information
Rights and permissions
Open Access. This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0.© The Author(s) 2024.
About this article

Cite this article
Thomas, S., Barrak, F. Awareness of peri-implantitis among general dental practitioners in the UK: a questionnaire study. Br Dent J (2024). https://doi.org/10.1038/s41415-024-7136-y
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41415-024-7136-y
- Springer Nature Limited
This article is cited by
-
Maintenance of peri-implant health in general dental practice
British Dental Journal (2024)