
Abstract
Background/objectives
The transition to adolescence is characterised by considerable behavioural changes, including diet. This study describes the level of obesogenic eating behaviours in 10- and 15-year-olds, and their association with dietary intake.
Subjects/methods
Participants of the 10- and 15-year follow-ups of the German GINIplus and LISA birth cohort studies were included (N10 = 2257; N15 = 1880). Eating behaviours and dietary intake were assessed via self-report questionnaires. Sex-stratified, cross-sectional associations of “external eating”, “emotional eating” and “dietary restraint” (the latter at age 15 years only) with dietary intake (17 food groups—categorised into tertiles, macronutrients, and total energy) were assessed using multinomial logistic or multiple linear regression as required, adjusting for covariates and correcting for multiple testing.
Results
Reported levels of eating behaviours were low in both age-groups. External eating was higher in 10-year-old males than females, while all eating behaviours were most pronounced in 15-year-old females. At 10 years, emotional eating was associated with medium vegetable intake in females (Relative Risk Ratio (RRR) = 1.84, p = 0.0017). At 15 years, external eating was associated with total energy (kJ) in females (β = 718, p = 0.0002) and high butter intake in males (RRR = 1.96, p = 0.0019). Dietary restraint in females was inversely associated with total energy (β = −967, p < 0.0001) and omega-3 fatty acids (Means Ratio (MR) = 0.94, p = 0.0017), and positively associated with high fruit (RRR = 2.20, p = 0.0003) and whole grains (RRR = 1.94, p = 0.0013).
Conclusion
Obesogenic eating behaviour scores are low among children and adolescents of a predominantly high socioeconomic status population and present only few associations with specific aspects of diet, mainly among adolescent females.
Similar content being viewed by others


Introduction
Overweight and obesity among children and adolescents are major public health issues, impairing health and overall quality of life [1, 2]. In Germany, around 15% of children and adolescents are currently affected [3]. The aetiology of childhood obesity is multifactorial and complex [4]; however, diet is a known risk factor, e.g. through energy imbalance caused by overeating [5]. Acquired behaviours often have a strong influence on eating decisions compared to biological mechanisms, i.e. internal stimuli triggering hunger and satiety [6,7,8]. In particular, three eating behaviours are associated with low responsiveness to internal signals of food intake: external eating, which refers to a high susceptibility to external food cues [9]; emotional eating, implying food intake as a coping strategy for emotional distress [9]; and dietary restraint, the cognitive regulation of eating for weight control, often observed in individuals struggling to maintain control over their food intake and weight [10, 11]. These behavioural dimensions have been associated with overweight among children and adolescents [12,13,14]. Understanding what aspects of the diet are influenced by these behaviours is of major importance for nutritional education and obesity prevention. The period of pubertal development is of special interest, given the shift in diet, being highly controlled by parents at younger ages, to increased autonomy, influence of peers as well as body image and weight concerns in adolescence [15, 16]. Studies on the association of eating behaviours with diet in children and adolescents have reported mixed results [15, 17,18,19,20,21,22]. These predominantly focus on single aspects of eating behaviour [15, 17, 19,20,21,22] and dietary intake, the latter mostly limited to selected (obesity-related) food groups or nutrients [15, 18, 20,21,22]. This study aims to describe the levels of external eating, emotional eating and dietary restraint at two time-points representing late childhood and adolescence, and their cross-sectional association with usual dietary intake among participants of the population-based German birth cohorts, GINIplus and LISA.
Subjects and methods
Study participants
The study included participants from the 10- and 15-year follow-ups of two ongoing prospective German birth cohort studies, GINIplus (German Infant Nutritional Intervention plus environmental and genetic influences on allergy development) and LISA (Influence of Lifestyle related factors on the development of the Immune System and Allergies in East and West Germany). In GINIplus, 5991 healthy full-term newborns were recruited from obstetric clinics in Munich and Wesel, between 1995 and 1998. Newborns with a family history of atopic disease were invited for the intervention arm, investigating effects of different hydrolysed formulae on allergy development. All others, and those declining participation in the intervention, were invited for the observation arm. The LISA cohort included 3097 healthy full-term newborns recruited between 1997 and 1999 in Munich, Wesel, Leipzig and Bad Honnef. In both studies, participants underwent assessments at regular follow-ups. Details on study design, recruitment strategy and exclusion criteria have been described previously [23, 24]. Both studies were conducted in accordance with the ethical standards laid down in the Declaration of Helsinki and approved by the local ethics committees (Bavarian Board of Physicians, Medical Faculty of the University of Leipzig, Board of Physicians of Saxony, and Board of Physicians of North-Rhine-Westphalia). All participants and their families gave written informed consent.
Eating behaviour
Eating behaviour was assessed by the Eating Behaviour and Weight Problems Inventory for Children (EWI-C) [25], designed specifically for children and young adolescents and widely applied in other European countries [26]. At 10 and 15 years, the inventory was addressed directly to the participants. It includes 60 items assigned to 10 subscales, of which three were integrated in the GINIplus and LISA studies: “External eating” (subscale 1), “Emotional eating” (subscale 3), and “Dietary restraint” (subscale 5). While the first two subscales were assessed at both follow-ups, “Dietary restraint” was not assessed at the 10-year follow-up, as it was considered that the emphasis on food avoidance as a means for weight reduction, could potentially transfer negative beliefs, attitudes and behaviours related to weight and body image to the young participants. We assumed that at 10 years, participants may be more prone to adopt new attitudes and behaviours that could lead to later disordered eating, while such behaviours are likely to be already established in adolescence [27]. Each item is scored on a four-point Likert scale (0 = not at all, 1 = little, 2 = mostly, 3 = totally), and these are summed up to obtain subscale scores (subscale 1 and 3 (8 items each): score = 0–24, subscale 5 (7 items): score = 0–21). Given the highly skewed distribution of the EWI-C scores, these were categorised into age- and sex-specific tertiles (T1 = low, T2 = medium, T3 = high).
Dietary intake
Dietary intake was assessed at the follow-ups age 10- and 15-years by a self-completed food frequency questionnaire (FFQ) containing 80 food items, designed and validated to estimate usual food intake in school-aged children [28]. At 10 years, parents were asked to complete the FFQ alongside their children, whereas at 15 years participants were addressed directly. Reported consumption frequency and portion sizes were converted into average daily intakes (g/d). Corresponding energy and nutrient contents were calculated using the German Food Code and Nutrient Database (BLS), version II.3.1 [29]. As part of the data quality control procedure, participants were excluded if a complete block of food items was empty or more than 40 food items (50 % of the FFQ) were missing. To further reduce the risk of under- and over-reporting of food intake, participants were excluded if total daily energy intake was outside 500–3500 kcal (2093–14,654 kJ) for females or 800–4000 kcal (3349–16,747 kJ) for males [30]. Moreover, exclusions were made if provided values for %EI of specific food items were implausible (outliers visually detected by means of boxplots). Further information on the dietary assessment and quality control steps is provided in Supplementary Text S1. Foods were classified into 17 food groups [31]. The present analysis includes all food groups, total daily energy intake, and macronutrients: fat, protein, carbohydrate, fibres, total sugar (mono- and disaccharides), saturated fatty acids (SFA), monounsaturated fatty acids, polyunsaturated fatty acids (PUFA), and omega-3 and −6 PUFA. Food groups and nutrients are expressed as their percentage contribution towards total daily energy intake (%EI), except water and tea (ml/day), fibres (g/day) and total energy intake (kJ/day). Given the skewed distribution of many food groups, these were categorised into tertiles (T1 = low, T2 = medium, T3 = high). Nutrients and total energy intake were treated as continuous variables, with total, omega-3, and omega-6 PUFA naturally log-transformed due to their log-normal distribution.
Covariates
Covariates were selected based on existing literature or if relevant to the study design. Those correlated in the univariate analysis (p < 0.05) with any exposure or outcome were kept: exact age at dietary assessment; body mass index (BMI); pubertal status, defined at 10 years as pubertal onset (yes, no), and at age 15 years as pubertal stage (pre-mid, late, or post-pubertal); siblings (yes, no); moderate-to-vigorous physical activity (low, medium, high); screen time (low, high); total difficulties, assessed by the Strengths and Difficulties Questionnaire [32,33,34] (normal, borderline, abnormal); parental education (low-medium, high), parental BMI (kg/m²); study (GINIplus observation, GINIplus intervention, LISA), recruitment region (Munich, Leipzig, Bad Honnef, Wesel), and total daily energy or beverage intake. At both follow-ups, information on covariates was obtained through medical examination or questionnaires. Details on the assessment and categorisation of covariates are provided in Supplementary Table S1.
Statistical analysis
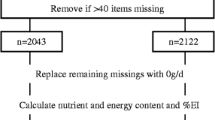
All statistical analyses were performed separately at each follow-up and stratified by sex, using R version 4.0.3 [35] (code available on request). Participants reporting cancer or medical dietary indications (reported only at 15 years), and those presenting dietary outliers (visually identified using boxplots) or with incomplete data for covariates were excluded (Fig. 1). Subject characteristics were described by medians (25th percentile; 75th percentile) or counts (%). Differences between sexes were tested by Wilcoxon’s rank sum test for continuous variables, and Pearson’s χ² test for categorical variables. Cross-sectional associations between eating behaviours and dietary intake were assessed by multinomial logistic regression for categorical outcome variables (ordinal logistic regression was not applied as the proportional odds assumption, tested using Brant test [36], was not fulfilled), and multiple linear regression for continuous outcome variables. All models were adjusted for the above-mentioned covariates. Total energy intake was included in all models except those with water and tea, which included total beverage intake. Results of multinomial logistic regression are presented as relative risk ratios (RRR), and of linear regression as beta coefficients (β) or means ratios (MR) for naturally log-transformed outcome variables, each with corresponding 95% confidence intervals (95% CI). Multinomial logistic regression was calculated using the “multinom” function in the R package “nnet” [37]. We corrected for multiple testing according to Nyholt [38]. Making use of the correlation pattern among all outcome variables, this method derives the number of effective variables, hence providing an estimate of the number of independent tests. The α-level was divided by this number, yielding a two-sided α-level of 0.0019 (0.05/26 = 0.0019). We performed various sensitivity analyses: First, excluding participants who reported a vegetarian or vegan diet. Second, we excluded participants with a BMI < 10th or >90th percentile. In the remaining sub-population, we further tested the interaction of each eating behaviour with BMI to detect possible BMI-specific effects. Significant interactions (p < 0.0019) were visualised applying the “plot_model” function in the R package “sjPlot” [39].

EWI-C Eating Behaviour and Weight Problems Inventory for Children, FFQ food frequency questionnaire. aThree families removed their consent to participate in the study. bMedical dietary indications included diabetes, coeliac disease, food allergies, food intolerances, and were assessed only at the 15-year follow-up. cDietary outliers: Clear outliers in diet variables were visually identified using descriptive plots and excluded from the analysis. dCovariates: age, BMI, pubertal status, siblings, moderate-to-vigorous physical activity, screen time, total difficulties, parental education, parental BMI, study, recruitment region, and total energy or total beverage intake.
Results
Study population
The study population included 1082 females and 1175 males at the 10-year follow-up, and 1000 females and 880 males at the 15-year follow-up (Fig. 1). Basic characteristics of the study population at each follow-up are described in Table 1. Median external eating scores averaged 6–7 at both time-points, with highest scores switching from males at 10 years to females at 15 years. The median score for emotional eating at 10 years was 1 in both sexes. At 15 years, both emotional eating and dietary restraint were 3 in females and 1 in males. Descriptive statistics of food group and nutrient intakes can be found in Supplementary Tables S2 and S3. Overall, females consumed more fruit and vegetables, while males consumed more meat and caloric drinks.
Association between eating behaviour and dietary intake
Results of regression analyses on the associations of eating behaviour and dietary intake in females and males at 10 and 15 years are presented in Fig. 2 (significant associations) and in Supplementary Tables S4–7. The first tertile (T1 = low) is the reference level for both exposure and categorical outcome variables.

Beta beta coefficient, CI confidence interval, MR means ratio, PUFA polyunsaturated fatty acids, RRR relative risk ratio; T1 tertile 1, T2 tertile 2, T3 tertile 3. Effect estimates of multinomial logistic regression are presented as relative risk ratio (95% CI). Effect estimates of multiple linear regression are presented as beta coefficient (95% CI). Effect estimates of multiple linear regression for naturally log-transformed outcome variables are presented as means ratio (95% CI). All models were adjusted for age, BMI, pubertal status, siblings, moderate-to-vigorous physical activity, screen time, total difficulties, parental education, parental BMI, study, and recruitment region. Food groups (except water and tea) and nutrients models were further adjusted for total daily energy intake. Water and Tea models were further adjusted for total daily beverage intake. Tertile 1 is the reference category. *Statistically significant (p < 0.0019).
External eating
External eating was not associated with dietary intake in females or males at 10 years. At 15 years, high external eating levels were linked to increased total energy intake in females (β = 718, 95% CI = (346;1090), p value = 0.0002) (Supplementary Table S6), and medium levels were positively associated with high butter intake in males (RRR = 1.96 (1.28; 2.99), p = 0.0019) (Supplementary Table S7).
Emotional eating
At the follow-up at age 10 years, medium levels of emotional eating were linked to medium vegetable intakes in females (RRR = 1.84 (1.26;2.69), p = 0.0017) (Supplementary Table S4). No association was found in males at the age of 10 years, nor at the age of 15 years in either sex.
Dietary restraint (15-year follow-up)
In females, high levels of dietary restraint were associated with high fruit intake (RRR = 2.20 (1.43;3.39), p = 0.0003) and lower total energy intake (β = −967 (−1,343; −591), p < 0.0001). Further, females with medium levels of dietary restraint were more likely to report high whole grain intakes (RRR = 1.94 (1.30;2.91), p = 0.0013), and lower omega-3 PUFA intakes (MR = 0.94 (0.91;0.98), p = 0.0017) (Supplementary Table S6). No associations with dietary restraint were observed in males.
After excluding participants who reported vegetarian or vegan diets (Supplementary Tables S8–11), the association of dietary restraint with fruit and whole grain intake in 15-year-old females was diminished (Supplementary Table S10).
Effect modification by BMI
Excluding participants with BMI < 10th or >90th percentile altered some associations (Supplementary Table S12–15): in females, the associations of emotional eating with vegetable intake at 10 years, and of external eating and dietary restraint with energy intake at 15 years remained significant; and a new positive association was observed at 15 years between emotional eating and medium water intake. In 15-year-old males, the association between external eating and butter was not significant, and an additional association with medium tea intake was observed. Significant interactions with BMI were observed for dietary restraint (with whole grain, oils and sugar-sweetened foods) and emotional eating (with dairy). These are depicted in plots of marginal effects stratified by BMI (low: <25th percentile; medium: ≥25th and <75th percentile; high: ≥75th percentile) in Supplementary Fig. S1. We observed positive associations among low-BMI participants and inverse associations among high-BMI participants with high dairy (10-year-old males) and high oil (15-year-old males). Different effect sizes with similar direction were observed for whole grains (15-year-old females) and sugar-sweetened foods (15-year-old males).
Discussion
The present analyses examined the extent of obesogenic eating behaviours (external eating, emotional eating, and dietary restraint) and their cross-sectional association with dietary intake, among 10- and 15-year-olds from the German GINIplus and LISA birth cohort studies. At both ages, external eating scores were higher than other eating behaviour scores. Males presented higher levels of external eating at 10 years, while all eating behaviours were more pronounced in females at the age of 15 years. Associations with dietary intake were mainly observed at the age of 15 years and among females. The most robust associations following sensitivity analyses were observed in females for emotional eating with vegetable intake at age 10 years, and for external eating and dietary restraint with total energy intake at 15 years.
Extent of obesogenic eating behaviour
In our study, the three EWI-C subscales ranged from median = 1–7, notably below those reported by Diehl (ranging 5–12) [25] in a representative sample of German schoolchildren (n = 923, 11–16 years) based on which the EWI-C was developed. Reasons for this discrepancy might be the overrepresentation of children from higher socioeconomic status, with a low prevalence of overweight and mental health problems in the GINIplus and LISA cohorts due to non-random loss-to-follow-up [24, 40]. However, our findings largely agree concerning sex and age differences: the increase in emotional eating levels from 10 to 15 years in females may be related to increased emotion-related problems such as anxiety, peer harassment or depression, which are often more present in adolescence [41, 42] and among females [43]. Furthermore, body weight and image dissatisfaction are also more common in females [13], reflected by their significantly higher score for dietary restraint. In males, however, impulsivity and less inhibitory control towards food cues might explain a higher score for external eating at 10 years [44, 45]. The observed increase in scores for all EWI-C subscales with age in our study may be related to the switch from a highly controlled child’s diet towards a more autonomous eating behaviour in adolescence [16]. On the other hand, at 10 years, children likely received support from their parents in completing the questionnaire, who possibly were not aware of or did not admit the extent of their child’s eating behaviour, leading to underreporting.
Association between eating behaviour and dietary intake
In regression analyses, external eating was associated with a significantly higher energy intake in 15-year-old females, although no association with specific food groups and nutrients was observed. This suggests external eating promotes an energy-rich diet irrespective of specific foods. An association with sweets and soft drinks as found in a Swedish study on 12-year-old children (n = 1441) [18] was not confirmed in the present analysis.
Existing studies investigating emotional eating in children and adolescents predominantly reported higher intakes of sweets, soft drinks, and energy-rich food [18,19,20, 22]. Although similar non-significant trends in 10- and 15-year-old females were indeed observed in our study, we could not substantiate these findings when considering only significant associations after correcting for multiple testing. Surprisingly, we also found that in 10-, but not in 15-year-old females, a medium level of emotional eating was linked to a medium level of vegetable intake with the high level of vegetable intake showing the same, though non-significant, tendency. Possibly, parents whose children show signs of emotional eating try to counteract this by providing healthier foods. Despite no effects seen for high levels of emotional eating, it should be noted that the range of scores in the high tertile (score = 3–18) is quite broad, possibly limiting the power to detect a significant association.
A high level of dietary restraint was significantly associated with lower total energy intake in females and a similar, albeit non-significant, trend in males in the present analysis, which might reflect a deliberate low-calorie weight-loss strategy [14]. Furthermore, our results indicate an association of dietary restraint with higher intakes of food groups considered healthy (whole grains, fruit) in 15-year-old females, corroborating previous research [15, 17, 18]. Excluding vegetarians and vegans weakened the observed associations with fruit and whole grains in females, thus suggesting that they were mainly driven by this subgroup. Reduced energy intake or more selective food choices, as was observed with dietary restraint [17], may negatively impact nutrient intake. An example is the lower intake of omega-3 PUFA associated with medium dietary restraint. Nevertheless, it should also be considered that restrained eaters are more prone to underreporting [46, 47].
Effect modification by BMI
Excluding participants with BMI < 10th or >90th percentile weakened some of the observed effects (e.g. with butter in males and omega-3 PUFA in females), suggesting that extreme body weight may present specific behaviour-diet relationships, and should be considered separate from the general population. Even after excluding these participants, numerous interactions with BMI were observed, indicating it is an important effect modifier. In males, associations of dietary restraint with high oil (at 15 years), and emotional eating with high dairy (at 10 years), occurred in opposite directions amongst the lowest (positive effect) and highest (inverse effect) BMI subgroups. In order to better understand eating behaviours in relation to diet, the interplay with BMI needs to be addressed in more depth in future studies.
Strengths and limitations
The present study benefits from a large study population of males and females aged 10 and 15 years. Addressing both time-points is a key aspect given the behavioural changes occurring during pubertal development and their long-term impact on health [48] and eating behaviour [49]. Rather than selecting specific dietary outcomes, we included all major food groups in our analysis, thus allowing for a comprehensive understanding of the relationship with diet as a whole. Despite the elevated number of tests this implies, we observed significant associations following correction for multiple testing. Several possible shortcomings of the study must be considered. Even though the sampling was primarily population-based, due to non-random loss-to-follow-up, the cohort overrepresents children from higher socioeconomic background, with a lower prevalence of overweight and obesity, which might limit generalisability. Moreover, our findings are observational and based on cross-sectional analyses, and thus cannot infer causality and reverse causation is conceivable. Categorisation of exposure and outcome variables, although considered necessary given the skewed distribution, implies certain loss of information and may reduce the power to detect associations particularly in the higher tertiles. The questionnaire applied to assess eating behaviour is not validated to our knowledge, but is commonly used in epidemiologic studies. Due to the lack of assessment of dietary restraint at the 10-year follow-up, no conclusions can be drawn about differences in this eating behaviour among children and adolescents. Unfortunately, only three subscales of the EWI-C were assessed in the GINIplus and LISA studies, as the full inventory is extensive. As the study assessments involve numerous comprehensive questionnaires and examinations relevant to common chronic diseases, we strive to keep the burden on participants to a minimum in order to avoid drop-out. Ideally, all ten subscales would have been analysed in this study, and since we observed interactions with BMI in our analysis, those explicitly referring to the attitude to (over-)weight and body figure would be relevant for future research.
Conclusion
The results of the present study indicate generally low reported levels of obesogenic eating behaviours among children and adolescents. Obesogenic eating behaviours present only few associations with diet, mainly with total energy intake and specific food groups among adolescent females. Numerous associations with diet were modified by BMI, indicating that future studies need to consider body weight even within a healthy weight population.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due to data protection reasons, but are available on reasonable request, provided it is consistent with the consent given by the study participants. In some cases, ethical approval can be obtained for the release. Lastly, a data transfer agreement must be accepted and the request must be approved by the studies’ steering committees. Requests should be addressed to MS (marie.standl@helmholtz-muenchen.de).
References
Friedemann C, Heneghan C, Mahtani K, Thompson M, Perera R, Ward AM. Cardiovascular disease risk in healthy children and its association with body mass index: systematic review and meta-analysis. BMJ 2012;345:e4759.
Tsiros MD, Olds T, Buckley JD, Grimshaw P, Brennan L, Walkley J, et al. Health-related quality of life in obese children and adolescents. Int J Obes. 2009;33:387–400.
Schienkiewitz A, Brettschneider A-K, Damerow S, Schaffrath, Rosario A. Overweight and obesity among children and adolescents in Germany. Results of the cross-sectional KiGGS Wave 2 study and trends. J Health Monit. 2018;3:15–22.
Ang YN, Wee BS, Poh BK, Ismail MN. Multifactorial Influences of Childhood Obesity. Curr Obes Rep. 2013;2:10–22.
Westerterp KR. Energy balance in motion. Heidelberg:Springer;2013.
Scaglioni S, De Cosmi V, Ciappolino V, Parazzini F, Brambilla P, Agostoni C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018;10:706.
Wardle J, Marsland L, Sheikh Y, Quinn M, Fedoroff I, Ogden J. Eating style and eating behaviour in adolescents. Appetite 1992;18:167–83.
Widhalm K, Zwiauer K, Eckharter I. [External stimulus dependence in food intake of obese adolescents: studies using a food dispenser]. Klin Padiatr. 1990;202:168–72.
van Strien T, Frijters JER, Bergers GPA, Defares PB. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int J Eat Disord. 1986;5:295–315.
Polivy J, Herman CP. Dieting and binging: a causal analysis. Am Psychol. 1985;40:193–201.
Hill AJ. Does dieting make you fat? Br J Nutr. 2004;92:S15–S18.
Braet C, Van Strien T. Assessment of emotional, externally induced and restrained eating behaviour in nine to twelve-year-old obese and non-obese children. Behav Res Ther. 1997;35:863–73.
Wardle J, Beales S. Restraint, body image and food attitudes in children from 12 to 18 years. Appetite 1986;7:209–17.
Schacht M, Richter-Appelt H, Schulte-Markwort M, Hebebrand J, Schimmelmann BG. Eating pattern inventory for children: a new self-rating questionnaire for preadolescents. J Clin Psychol. 2006;62:1259–73.
Bisset S, Gauvin L, Potvin L, Paradis G. Association of body mass index and dietary restraint with changes in eating behaviour throughout late childhood and early adolescence: a 5-year study. Public Health Nutr. 2007;10:780–9.
Bejarano CM, Cushing CC. Dietary motivation and hedonic hunger predict palatable food consumption: an intensive longitudinal study of adolescents. Ann Behav Med Publ Soc Behav Med. 2018;52:773–86.
Mulvihill CB, Davies GJ, Rogers PJ. Dietary restraint in relation to nutrient intake, physical activity and iron status in adolescent females. J Hum Nutr Diet J Br Diet Assoc. 2002;15:19–31.
Elfhag K, Tholin S, Rasmussen F. Consumption of fruit, vegetables, sweets and soft drinks are associated with psychological dimensions of eating behaviour in parents and their 12-year-old children. Public Health Nutr. 2008;11:914–23.
Lu Q, Tao F, Hou F, Zhang Z, Ren L-L. Emotion regulation, emotional eating and the energy-rich dietary pattern. A population-based study in Chinese adolescents. Appetite 2016;99:149–56.
Nguyen-Michel ST, Unger JB, Spruijt-Metz D. Dietary correlates of emotional eating in adolescence. Appetite 2007;49:494–9.
Michels N, Sioen I, Braet C, Eiben G, Hebestreit A, Huybrechts I, et al. Stress, emotional eating behaviour and dietary patterns in children. Appetite 2012;59:762–9.
Striegel-Moore RH, Morrison JA, Schreiber G, Schumann BC, Crawford PB, Obarzanek E. Emotion-induced eating and sucrose intake in children: the NHLBI Growth and Health Study. Int J Eat Disord. 1999;25:389–98.
von Berg A, Krämer U, Link E, Bollrath C, Heinrich J, Brockow I, et al. Impact of early feeding on childhood eczema: development after nutritional intervention compared with the natural course - the GINIplus study up to the age of 6 years. Clin Exp Allergy J Br Soc Allergy Clin Immunol. 2010;40:627–36.
Heinrich J, Bolte G, Hölscher B, Douwes J, Lehmann I, Fahlbusch B, et al. Allergens and endotoxin on mothers’ mattresses and total immunoglobulin E in cord blood of neonates. Eur Respir J. 2002;20:617–23.
Diehl JM. [Attitude to eating and body weight by 11-to 16-year-old adolescents]. Schweiz Med Wochenschr.1999;129:162–75.
Béghin L, Huybrechts I, Vicente-Rodríguez G, De Henauw S, Gottrand F, Gonzales-Gross M, et al. Main characteristics and participation rate of European adolescents included in the HELENA study. Arch Public Health. 2012;70:14.
de Castro JM, Goldstein SJ. Eating attitudes and behaviors of pre- and postpubertal females: clues to the etiology of eating disorders. Physiol Behav. 1995;58:15–23.
Stiegler P, Sausenthaler S, Buyken AE, Rzehak P, Czech D, Linseisen J, et al. A new FFQ designed to measure the intake of fatty acids and antioxidants in children. Public Health Nutr. 2010;13:38–46.
Hartmann BM, Bell S, Vásquez-Caicedo AL, Götz A, Brombach C. Der Bundeslebensmittelschlüssel. Karlsruhe:German Nutrient Data Base; 2005.
Willett W. Nutritional Epidemiology. 3rd ed. Oxford, New York:Oxford University Press;2012.
Harris C, Flexeder C, Thiering E, Buyken A, Berdel D, Koletzko S, et al. Changes in dietary intake during puberty and their determinants: results from the GINIplus birth cohort study. BMC Public Health. 2015;15:841.
Goodman R. The Strengths and Difficulties Questionnaire: a research note. J Child Psychol Psychiatry. 1997;38:581–6.
Woerner W, Becker A, Friedrich C, Klasen H, Goodman R, Rothenberger A. [Normal values and evaluation of the German parents’ version of Strengths and DIfficulties Questionnaire (SDQ): Results of a representative field study]. Z Kinder Jugendpsychiatr Psychother. 2002;30:105–12.
Woerner W, Becker A, Rothenberger A. Normative data and scale properties of the German parent SDQ. Eur Child Adolesc Psychiatry 2004;13:II3–10. Suppl 2
R Core Team. R: a language and environment for statistical computing. Vienna, Austria:R Foundation for Statistical Computing;2018.
Brant R. Assessing Proportionality in the Proportional Odds Model for Ordinal Logistic Regression. Biometrics 1990;46:1171.
Venables WN, Ripley BD, Venables WN. Modern applied statistics with S. 4th ed. New York:Springer;2002.
Nyholt DR. A Simple Correction for Multiple Testing for Single-Nucleotide Polymorphisms in Linkage Disequilibrium with Each Other. Am J Hum Genet. 2004;74:765–9.
Lüdecke D. sjPlot - Data Visualization for Statistics in Social Science. Zenodo, 2018 https://doi.org/10.5281/ZENODO.2400856.
Bühlmeier J, Harris C, Koletzko S, Lehmann I, Bauer C-P, Schikowski T, et al. Dietary Acid Load and Mental Health Outcomes in Children and Adolescents: Results from the GINIplus and LISA Birth Cohort Studies. Nutrients 2018;10:582.
Auerbach RP, Bigda-Peyton JS, Eberhart NK, Webb CA, Ho M-HR. Conceptualizing the Prospective Relationship Between Social Support, Stress, and Depressive Symptoms Among Adolescents. J Abnorm Child Psychol. 2011;39:475–87.
Zimmer-Gembeck MJ, Webb HJ, Farrell LJ, Waters AM. Girls’ and boys’ trajectories of appearance anxiety from age 10 to 15 years are associated with earlier maturation and appearance-related teasing. Dev Psychopathol. 2018;30:337–50.
Zimmer-Gembeck MJ, Webb HJ, Kerin J, Waters AM, Farrell LJ. Risk factors and temporal patterns of disordered eating differ in adolescent boys and girls: Testing gender-specific appearance anxiety models. Dev Psychopathol. 2021;33:856–67.
Hou R, Mogg K, Bradley BP, Moss-Morris R, Peveler R, Roefs A. External eating, impulsivity and attentional bias to food cues. Appetite 2011;56:424–7.
Chapple CL, Johnson KA. Gender Differences in Impulsivity. Youth Violence Juv Justice. 2007;5:221–34.
Black AE, Coward WA, Cole TJ, Prentice AM. Human energy expenditure in affluent societies: an analysis of 574 doubly-labelled water measurements. Eur J Clin Nutr. 1996;50:72–92.
Bingham SA, Cassidy A, Cole TJ, Welch A, Runswick SA, Black AE, et al. Validation of weighed records and other methods of dietary assessment using the 24 h urine nitrogen technique and other biological markers. Br J Nutr. 1995;73:531–50.
McDade TW, Chyu L, Duncan GJ, Hoyt LT, Doane LD, Adam EK. Adolescents’ expectations for the future predict health behaviors in early adulthood. Soc Sci Med. 2011;73:391–8.
Neumark-Sztainer D, Wall M, Larson NI, Eisenberg ME, Loth K. Dieting and disordered eating behaviors from adolescence to young adulthood: findings from a 10-year longitudinal study. J Am Diet Assoc. 2011;111:1004–11.
Acknowledgements
The authors thank all the families for their participation in the GINIplus and LISA studies. Furthermore, we thank all members of the GINIplus and LISA Study Groups for their excellent work. The GINIplus Study Group consists of the following: Institute of Epidemiology, Helmholtz Zentrum München, German Research Center for Environmental Health, Neuherberg (Heinrich J, Brüske I, Schulz H, Flexeder C, Zeller C, Standl M, Schnappinger M, Ferland M, Thiering E, Tiesler C); Department of Pediatrics, Marien-Hospital, Wesel (Berdel D, von Berg A); Ludwig-Maximilians-University of Munich, Dr von Hauner Children’s Hospital (Koletzko S); Child and Adolescent Medicine, University Hospital rechts der Isar of the Technical University Munich (Bauer CP, Hoffmann U); IUF- Environmental Health Research Institute, Düsseldorf (Schikowski T, Link E, Klümper C, Krämer U, Sugiri D). The LISA Study group consists of the following: Helmholtz Zentrum München, German Research Center for Environmental Health, Institute of Epidemiology, Munich (Heinrich J, Schnappinger M, Brüske I, Ferland M, Schulz H, Zeller C, Standl M, Thiering E, Tiesler C, Flexeder C); Department of Pediatrics, Municipal Hospital “St. Georg”, Leipzig (Borte M, Diez U, Dorn C, Braun E); Marien-Hospital Wesel, Department of Pediatrics, Wesel (von Berg A, Berdel D, Stiers G, Maas B); Pediatric Practice, Bad Honnef (Schaaf B); Helmholtz Centre of Environmental Research – UFZ, Department of Environmental Immunology/Core Facility Studies, Leipzig (Lehmann I, Bauer M, Röder S, Schilde M, Nowak M, Herberth G, Müller J); Technical University Munich, Department of Pediatrics, Munich (Hoffmann U, Paschke M, Marra S); Clinical Research Group Molecular Dermatology, Department of Dermatology and Allergy, Technische Universität München (TUM), Munich (Ollert M, J. Grosch).
Funding
The GINIplus study was mainly supported for the first 3 years of the Federal Ministry for Education, Science, Research and Technology (interventional arm) and Helmholtz Zentrum Munich (former GSF) (observational arm). The 4-year, 6-year, 10-year and 15-year follow-up examinations of the GINIplus study were covered from the respective budgets of the five study centres (Helmholtz Zentrum Munich (former GSF), Research Institute at Marien-Hospital Wesel, LMU Munich, TU Munich and from 6 years onwards also from IUF - Leibniz Research-Institute for Environmental Medicine at the University of Düsseldorf) and a grant from the Federal Ministry for Environment (IUF Düsseldorf, FKZ 20462296). Further, the 15-year follow-up examination of the GINIplus study was supported by the Commission of the European Communities, the 7th Framework Program: MeDALL project, and as well by the companies Mead Johnson and Nestlé. The LISA study was mainly supported by grants from the Federal Ministry for Education, Science, Research and Technology and in addition from Helmholtz Zentrum Munich (former GSF), Helmholtz Centre for Environmental Research - UFZ, Leipzig, Research Institute at Marien-Hospital Wesel, Pediatric Practice, Bad Honnef for the first 2 years. The 4-year, 6-year, 10-year and 15-year follow-up examinations of the LISA study were covered from the respective budgets of the involved partners (Helmholtz Zentrum Munich (former GSF), Helmholtz Centre for Environmental Research - UFZ, Leipzig, Research Institute at Marien-Hospital Wesel, Pediatric Practice, Bad Honnef, IUF – Leibniz-Research Institute for Environmental Medicine at the University of Düsseldorf) and in addition by a grant from the Federal Ministry for Environment (IUF Düsseldorf, FKZ 20462296). Further, the 15-year follow-up examination of the LISA study was supported by the Commission of the European Communities, the 7th Framework Program: MeDALL project. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
AM, CPH, JB, LL, MS were involved in the conception and design of the study; MS, SK, C-PB, TS, DB, AvB and GH in the data acquisition; AM, CPH and MS in the statistical analyses; AM, CPH, JB, LL, MS in the interpretation; AM drafted the paper; All authors revised it critically for important intellectual content and approved the final version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The GINIplus and LISA birth cohort studies were conducted in accordance with the ethical standards laid down in the Declaration of Helsinki and approved by the local ethics committees: Bavarian Board of Physicians (No. 05100 10-year follow-up GINIplus; No. 07098 10-year follow-up LISA; No. 10090 15-year follow-up GINIplus; No. 12067 15-year follow-up LISA), Medical Faculty of the University of Leipzig (No. 345-2007 10-year follow-up LISA), Board of Physicians of Saxony (No. EK-BR-02/13-1 15-year follow-up LISA) and Board of Physicians of North-Rhine-Westphalia (No. 2005407 10-year follow-up GINIplus; No. 2008153 10-year follow-up LISA; No. 2010424 15-year follow-up GINIplus; No. 2012446 15-year follow-up LISA). All participants and their families gave written informed consent before study onset.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Marb, A., Libuda, L., Standl, M. et al. Obesogenic eating behaviour and dietary intake in German children and adolescents: results from the GINIplus and LISA birth cohort studies. Eur J Clin Nutr 76, 1478–1485 (2022). https://doi.org/10.1038/s41430-022-01125-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41430-022-01125-2
- Springer Nature Limited