
Abstract
Safely managed drinking water services (SMDWS) is the service ladder used for the Sustainable Development Goal (SDG) monitoring of drinking water and expands on the Millennium Development Goal metric (“improved water source”) with three additional criteria, namely: availability when needed, accessibility on premises, and safety (free from faecal and priority chemical contamination). Multiple Indicator Cluster Surveys (MICS) have been used for progress monitoring accounting for a significant fraction of the water, sanitation, and hygiene (WASH) indicator data. In its most recent iteration MICS now includes additional SMDWS indicators. The objective of this study was to report on recent SDG target 6.1 baseline data on SMDWS from the Democratic People’s Republic of Korea gathered from a MICS conducted in 2017. Survey results indicated that 93.7% of the population used an improved drinking water source, but when this was combined with the SDG criteria of water availability, accessibility, and safety, coverage was reduced to 92.3, 78.2, and 74.4%, respectively. This resulted in estimates that 60.9% of the population used a SMDWS. The survey results illustrate how the improved SDG indicators can highlight the required gaps to be overcome with regard to universal and equitable access to SMDWS. Further analysis and discussion regarding water quality deterioration between source and household as well as population residence, wealth group index, geographical distribution, and other characteristics relative to SMDWS indicators are also further analysed and discussed.
Similar content being viewed by others

Introduction
During the Millennium Development Goals (MDGs) era (2000–2015), access to drinking water was assessed using a simple “improved/unimproved” source type classification to monitor progress towards target 7C to halve, by 2015, “the proportion of the population without sustainable access to safe drinking water”1. According to the WHO/UNICEF Joint Monitoring Programme (JMP), an improved drinking water source is considered to be one that could adequately protect the source from outside (faecal) contamination by nature of its construction2. These indicators were used despite the recognition that an improved source can describe a level of sanitary protection, but it does not ensure water is “safe” (i.e., free of faecal contamination)3. For the Sustainable Development Goals (SDGs), the JMP has developed a new service ladder4 building on MDG source typology with additional criteria for safely managed drinking water services (SMDWS) for monitoring of the SDG aspirational global target 6.1, which aims to achieve universal and equitable access to safe and affordable drinking water for all by 2030.
The service ladder used for the SDG monitoring of drinking water culminates in a SMDWS and expands on the previous one with three additional criteria. A SMDWS is accessible on premises, available when needed, and that is free from faecal and priority chemical contamination4. In addition to safely managed, other household water service classifications are basic (i.e., improved source with collection time <30 min), limited (i.e., improved source with collection time >30 min), unimproved (i.e., unprotected dug well or spring as source), and no service (i.e., direct use of surface water source). These definitions are further detailed in Table 1. Monitoring SMDWS can be achieved using data provided by regulatory agencies or utilities. However, when such information is not available, as in many low- and middle-income countries, progress is estimated from censuses and household surveys such as the UNICEF-supported Multiple Indicator Cluster Surveys (MICS). In fact, such surveys, including USAID-supported Demographic and Health Surveys (DHS) and the World Bank-supported Living Standards Measurement Study (LSMS), were the major source of data for the MDG monitoring accounting for 84% of the water, sanitation, and hygiene (WASH) indicator data2 and will likely continue to be a major data source for the SDGs.
MICS were established to collect representative data on the situation of women and children and now include over 200 indicators. With over 300 surveys conducted since 1995 by implementing agencies in over 100 countries, it is now in its sixth round (occurring every 3–5 years) serving to collect baseline data for monitoring of some SDGs. In addition to the type and location of drinking water sources (captured through MDG indicators) improved SDG WASH indicators have been tested5 and incorporated to forthcoming MICS. These include source and household testing for Escherichia coli (E. coli) as well as a set of questions on drinking water availability.
Within the context of development goals, countrywide drinking water monitoring assessments in many countries such as the Democratic People’s Republic of Korea (DPRK) have previously relied on previous MICS (i.e., 19986, 20007, and 20098) or other household survey data. These reported close to universal access to an improved water source. The expanded indicators used for SDG progress monitoring as measured by MICS afford the possibility of a more accurate assessment of progress towards universal and equitable access to SMDWS; particularly for countries without other nationally representative data on service levels. The overall objective of this study was to provide further analysis and discussion on the new SDG target 6.1 indicators for SMDWS from a recent MICS conducted in the DPRK9. Here the findings from the more comprehensive MICS module, including water quality testing for faecal contamination of water, are presented alongside the availability and accessibility of drinking water services10.
Results
Water sources and location
A very high proportion of the population (93.7%) used an improved drinking water source. The main source was piped water (58.5%) followed by tube-well/bore-hole (15.8%), protected well or spring (11.3%), and water kiosks (7.8%). Over half (55.6%) the population used drinking water piped into dwelling, with pronounced differences between urban and rural residents (66.4 and 38.7%, respectively) and the 40% highest and the 20% lowest wealth index groups (WIGs) (76.2 and 23.6%, respectively). Three quarters (78.2%) of the population used an improved water source located on premises, but 16.6% used improved sources of drinking water requiring up to 30 min to collect water. Among households without drinking water on premises, women were disproportionately tasked with collecting water (65.2%) compared to men (29.9%), particularly in rural areas (71.6% in comparison to 61.2% in urban areas).
Availability of drinking water
The availability of water is almost universal, with 98.6% of the household population reporting drinking water available in sufficient quantities. There were also no substantial differences in the availability of drinking water by residence, provinces, and WIG.
Drinking water quality
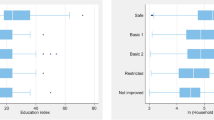
Overall, 76.5% of the population uses a drinking water source that was free from evidence of faecal contamination. Figure 1 shows the proportion of the population by thermotolerant coliforms (TTC) risk level in the source of drinking water and a glass of drinking water within the home. Such classification is based on a priori waterborne risk categories11. There were marked differences in the quality of drinking water sources (without TTC) used in urban (90.3%) and rural (54.8%) areas and between the 40% of the population from the highest WIG (90.0%) and the 20% of the population from the lowest WIG (54.8%). Among the provinces, Pyongyang (90.9%) had the highest percent of the household population without TTC in source water compared to South Hwanghae (63.7%), the province with the lowest percentage.

Source and household water quality risk levels. Percentages in brackets represent the proportion of the household population.
Piped water (15.1%) and water kiosks (9.0%) were less likely to be contaminated (TTC > 1 per 100 mL) than improved groundwater sources ranging from 33.1% (protected spring or well) to 37.7% (tube well/borehole). Most unimproved sources (unprotected wells and springs) were contaminated (64.0%). There was almost no (0.3%) reported direct use of surface water sources (not shown in Fig. 1).
Water quality was found to deteriorate between the water source and the glass within the home (Fig. 1). Overall 36.6% of the population consume drinking water in which TTC were detected. The proportion of the population exposed to high (TTC levels between 11 and 100 cfu/100 mL) or very high (TTC levels > 100 cfu/100 mL) risk drinking water increased from 15.4 to 27.1% between the source and the glass within the home. There was an increase in the proportion of the population in higher-risk categories for all water sources and WIGs.
Safely managed drinking water services
Figure 2 shows how the estimate for national coverage of drinking water services in DPRK changes with the shift from MDG to SDG indicators for drinking water. Most of the population (93.7%) used an improved source of drinking water (as per the MDG metric). Since few households spend more than 30 min roundtrip to collect drinking water, 93.2% use at least a basic drinking water service. The three SDG criteria for safely managed drinking water services reduce coverage to 92.3% improved and available when needed, 78.2% improved and accessible on premises, and 74.4% improved and free from contamination. Taking these three criteria into consideration, the MICS survey estimates that 60.9% of the population used a safely managed drinking water service.

Proportion of the population using improved, basic, and safely managed drinking water services in 2017 and SDG service ladder (proportion using surface water not shown −0.3%).
Table 2 provides a summary of estimates for use of improved drinking water, elements of safely managed drinking water services by area, province, type of water source, and wealth. Overall, the proportion of the population with access to the different levels of services was higher in urban areas when compared to rural ones and also increased with higher levels of wealth. The three provinces with the lowest levels of access to safely managed drinking water services were Kangwon with 52.0% (6.4% of DPRK population), South Pyongan with 50.0% (17.1% of DPRK population), and South Hwanghae with 48.3% (10.1% of DPRK population). Detected faecal contamination and lack of on-premise water accessibility were the major factors contributing to these levels of access to safely managed drinking water services. Interestingly, they represented provinces with a range of percent distribution of the household population by WIGs. Whereas Kangwon had an intermediary distribution of the household population by WIGs, South Pyongan had a relatively higher proportion in the middle 40% and South Hwanghae had a relatively higher proportion in the lowest 20%. South-Pyongan and South Hwanghae were also the provinces with the highest (14.3%) and second highest (13.4%) percentage of children (0–59 months) with an episode of diarrhoea reported by mother (or caretaker) within 2 weeks of survey9. Pyongyang is considered to have a relatively high degree of urbanisation and had one of the highest levels (74.7%) of access to safely managed drinking water services across all elements. It also had the lowest (6.8%) level of children (0–59 months) with a reported episode of diarrhoea within 2 weeks of survey9.
For piped water, tube-well/bore-hole, and water kiosks, the major limiting factor for attaining safely managed drinking water services was the presence of TTC in water quality assessments. For protected well or spring sources, both faecal contamination and accessibility on premises were limiting factors for safely managed drinking water services coverage. Lack of household water treatment in 83.2% of the household population may have contributed to increased levels of faecal contamination in the sampled glass of drinking water relative to the source (Fig. 1). 17.7% of the household population use an appropriate (e.g., boiling, water filter, purification tablets, etc.) method of water treatment, with boiling (14.2%) as the most frequently reported method.
Discussion
The Central Bureau of Statistics of DPRK with support from UNICEF integrated water quality testing (and other service indicators) for the first time allowing for the assessment of safely managed drinking water services. Currently, based on the latest census figures (population 24,052,231) and 2017 DPRK MICS results, it is estimated that around 19 million people utilise sources of water free from faecal contamination and that around 15 million people have access to safely managed drinking water services. Whereas universal access to drinking water is an ambitious goal set by SDG target 6.1, use of the new “safely managed drinking water service” indicator addressed many of the limitations of MDG monitoring by addressing water quality, accessibility, and availability.
Only a limited comparison to previous MICS (19986, 20007, and 20098) is possible as the survey has changed in its different editions regarding water-related questions. Notably, no previous survey had a dedicated water quality module as was done in 2017. The level of reported access to an improved water source in previous (MDG era) surveys was of 99.8% (1998), 100% (2000), and 99.9% (2009). A slight decrease in the 2017 survey was observed (93.7%); this may be attributed to a better and clearer set of definitions regarding improved water sources. At the same time, there is a noticeable drop in the use of piped water into own dwelling, into yard/plot and public taps between previous surveys, census and 2017 DPRK MICS. For instance, access to piped water was 89% during 2009 DPRK MICS and 59% in 2017 DPRK MICS. These differences may be due to changes in the methodology, training of field teams, and/or verification of water sources used by households afforded by the water quality module.
Despite these differences between surveys, access to improved sources is relatively high in comparison to household survey-based studies on other low and lower-middle-income countries12. Additionally, the level of access to improved sources in the DPRK was also comparable to upper-middle and high-income neighbouring countries regarding JMP estimates13; 96.7% for China, 97.0% for the Russian Federation, and 99.6% for the Republic of Korea.
The inclusion of testing for faecal contamination (at source and household) and a set of questions on drinking water availability allowed for an improved understanding of where efforts should be focused to achieve safely managed drinking water services. This is of particular importance in countries such as DPRK where most households use improved drinking water sources. As shown in Fig. 1, water quality often deteriorated between the water source and a glass of drinking water, a pattern observed in urban and rural areas and across provinces, WIGs and different types of water source. This situation is compounded with the fact that less than a fifth of households reported using an appropriate method of water treatment, of which boiling was the most frequently reported method.
Increasing accessibility and quality of drinking water are the key priorities for the DPRK to achieve universal access to safely managed drinking water sources and progress towards SDG target 6.1, with rural areas requiring the greatest improvements. Access to safe drinking water on premises will improve the quality of life especially for women who disproportionately shoulder the burden of fetching water. However, service delivery should also be augmented with behaviour change programming on the promotion of household water treatment and safe water storage, which is a potentially low-cost option for WASH programming in DPRK.
One difference between MICS and other similar surveys incorporating other SDG water-related indicators (faecal contamination and questions on water availability) was the method for water quality testing. Wagtech Potatest (Palintest, UK) water quality kits were used for this purpose in the 2017 DPRK MICS due to the unavailability of the standard MICS water quality test5 at the time of the survey. The standard MICS water quality testing also utilises a membrane filtration technique-based assay using a custom portable testing kit based on the EZ-Fit system (Millipore) and a selective enzymatic growth media for E. coli (Nissui Compact Dry EC). The choice for the DPRK survey was due to import restrictions of some materials necessary for the water quality testing typically used in MICS. The water quality test used in the 2017 DPRK MICS is based on a technique routinely used for water quality assessments in the field using the same14 and other commercial variants15,16,17 in a variety of contexts. It was felt that this decision did not compromise the quality of the water quality tests. Only 1.1% of the blank control testing resulted in faecally contaminated tests. This is consistent and within acceptable ranges of reported blank testing results of MICS recently conducted in other countries18,19,20,21 that included water quality testing.
The 2017 DPRK MICS allowed for a snapshot of safely managed drinking water service indicators to monitor progress towards SDGs at the national level. It does not provide a substitute for regular monitoring and risk assessments of water supplies. Furthermore, other relevant chemical water quality indicators (e.g., free chlorine residual) and contaminants (e.g., arsenic and fluoride) were not measured, as has been done in other surveys20,22. Given the relatively high use of piped water supplies, the former could be used to evaluate their state of disinfection. There had been no suspected risk of the latter to warrant monitoring of geogenic contaminants of concern. A further survey characteristic to be noted was that the self-reported availability of water in the previous month does not imply continuous availability throughout the day or throughout the year. This issue is a limitation of household surveys such as MICS that do not take into account seasonal effects on the availability of water. Finally, microdata from the 2017 DPRK MICS were not publicly available. This limited the present study to the data available in tabulated format9 and precluded a detailed assessment of correlations between safely managed drinking water service indicators and other factors (i.e., WIG, province, rural vs. urban, etc.).
Results indicated that 93.7% of the population used an improved drinking water source, but when this was combined with the SDG criteria of water availability, accessibility, and safety, coverage was reduced to 92.3, 78.2, and 74.4%, respectively. This resulted in estimates that 60.9% of the population used a SMDWS. The survey results illustrate how the improved SDG indicators can highlight the required gaps to be overcome with regard to universal and equitable access to SMDWS.
Methods
MICS survey design
The sample for the 2017 DPR Korea Multiple Indicator Cluster Survey (MICS) was designed to provide estimates for a large number of indicators on the situation of children and women at the national level, for urban and rural areas, and for all 10 provinces. This survey was implemented by Central Bureau of Statistics (CBS) with support from UNICEF. The urban and rural areas within each province were identified as the main sampling strata and the sample of households was selected in two stages. Within each stratum, a specified number of census enumeration areas were selected systematically with probability proportional to size. A total of 340 sample enumeration areas were selected at the first stage. After a household listing was carried out within the selected enumeration areas, a systematic sample of 25 households was drawn, for a total sample size of 8500 households. The 2017 DPR Korea MICS sample was not self-weighting. For reporting survey results, sample weights were used. A more detailed description of the sample design (including used questionnaires) can be found in Survey Findings Report9. Six questionnaires were used in the survey: (1) a household questionnaire which was used to collect basic demographic information on all de jure household members (usual residents), the household, and the dwelling; (2) a water quality testing questionnaire administered in four households in each cluster of the sample; (3) a questionnaire for individual women administered in each household to all women aged 15–49 years; (4) a questionnaire for individual men administered in every second household to all men aged 15–49 years; (5) an under-5 questionnaire, administered to mothers (or caretakers) of all children under 5 living in the household; and (6) a questionnaire for children aged 5–17 years, administered to the mother (or caretaker) of one randomly selected child aged 5–17 years living in the households5.
Analysis of SMDWS indicators was based on WASH questions in the standard MICS household questionnaire as well as results from water quality testing questionnaire. Table 3 summarises the questions, their characteristics, and respective sources used to assess SMDWS indicators of accessibility, availability, and water quality.
Water quality analysis
When provided, water samples were collected and then tested for faecal contamination. These samples consisted of the requested household glass of water and its originating source. To this end, a Wagtech Potatest (Palintest, UK) water quality kit was used to quantify thermotolerant coliform bacteria using a membrane filtration technique. Membrane lauryl sulfate broth (Oxoid, UK) was used as a selective media that was prepared and sterilised prior to distribution to the water quality measurers. Samples were analysed in the field within 30 min of collection and incubated at 44 °C for at least 18 h, as per the manufacturer’s instructions. Locally-available bottled mineral waters were tested to ensure they were free from TTC contamination and would be adequate for blank testing. One surveyed household per cluster was randomly selected for blank testing. Further details on water quality test method and sampling technique used in this study are available in the Supplementary Materials.
Data analysis
Data analysis was conducted by the Central Bureau of Statistics using SPSS, Version 22. Model syntax and tabulation plans developed by UNICEF were customised and used for this purpose. The analysis for the final report followed standard MICS templates for reporting on WASH indicators for the SDGs. Separate weights were calculated for the water quality sub-sample and these were used for the calculation of the safely managed services indicator. Further details are provided in the MICS report9.
Data availability
The data that support the findings of this study are available from the Multiple Indicator Cluster Survey 2017, Survey Findings Report9.
References
United Nations Development Group. Indicators for Monitoring the Millenium Development Goals (United Nations, 2003).
UNICEF & World Health Organization. Progress on Sanitation and Drinking Water—2015 Update and MDG Assessment (2015).
Bain, R. et al. Fecal contamination of drinking-water in low- and middle-income countries: a systematic review and meta-analysis. PLoS Med. 11, e1001644 (2014).
UNICEF & World Health Organization. Safely Managed Drinking Water (2017).
Khan, S. M. et al. Optimizing household survey methods to monitor the Sustainable Development Goals targets 6.1 and 6.2 on drinking water, sanitation and hygiene: a mixed-methods field-test in Belize. PLoS ONE 12, e0189089 (2017).
Anonymous. The Multiple Indicator Cluster Survey in the Democratic People’s Republic of Korea. http://mics.unicef.org/surveys (1998).
Central Bureau of Statistics of the DPR Korea. Report of the Second Multiple Indicator Cluster Survey 2000, DPRK. http://mics.unicef.org/surveys (2000).
Central Bureau of Statistics of the DPR Korea & UNICEF. Multiple Indicator Cluster Survey 2009, Final Report. http://mics.unicef.org/surveys (2010).
Central Bureau of Statistics of the DPR Korea & UNICEF. Multiple Indicator Cluster Survey 2017, Survey Findings Report. (2018).
Bain, R., Johnston, R., Mitis, F., Chatterley, C. & Slaymaker, T. Establishing sustainable development goal baselines for household drinking water, sanitation and hygiene services. Water 10, 1711 (2018).
Lloyd, B. & Helmer, R. Surveillance of Drinking Water Quality in Rural Areas (John Wiley & Sons, 1991).
Roche, R., Bain, R. & Cumming, O. A long way to go—estimates of combined water, sanitation and hygiene coverage for 25 sub-Saharan African countries. PLoS ONE 12, e0171783 (2017).
WHO & UNICEF. WHO/UNICEF JMP WASH Data. https://washdata.org/data (2019).
Osiemo, M. M., Ogendi, G. M. & M’Erimba, C. Microbial quality of drinking water and prevalence of water-related diseases in Marigat Urban Centre, Kenya. Environ. Health Insights 13, https://doi.org/10.1177/1178630219836988 (2019).
Dorea, C. C., Clarke, B. A. & Bertrand, S. Performance of a rural multi-stage filtration plant after its handover. Water Policy 6, 559–570 (2004).
Dorea, C. C., Luff, R., Bastable, A. & Clarke, B. A. Up-flow clarifier for emergency water treatment. Water Environ. J. 23, 293–299 (2009).
Shrestha, A. et al. Water quality, sanitation, and hygiene conditions in schools and households in Dolakha and Ramechhap Districts, Nepal: results from a cross-sectional survey. Int. J. Environ. Res. Public Health 14, 89 (2017).
Lao Statistics Bureau. Lao Social Indicator Survey II 2017, Survey Findings Report (2018).
National Bureau of Statistics & UNICEF. Multiple Indicator Cluster Survey 2016–17, Survey Findings Report (2017).
Central Statistical Agency of Ethiopia. Drinking Water Quality in Ethiopia—Results from the 2016 Ethiopia Socioeconomic Survey (2017).
Statistics Sierra Leone. Sierra Leone Multiple Indicator Cluster Survey 2017—Survey Findings Report (2018).
Sindh Bureau of Statistics & UNICEF. Sindh Multiple Indicator Cluster Survey 2014, Final Report (2015).
Acknowledgements
This research was supported by the Democratic People’s Republic of Korea, UNICEF, and the Netherlands Directorate-General for International Cooperation, through a grant to the WHO/UNICEF Joint Monitoring Programme. The authors would like to thank the Central Bureau of Statistics, Ministry of Urban Management (previous Ministry of City Management), and the Institute of Hygiene and Environment Staff that collected the DPRK MICS water quality data.
Author information
Authors and Affiliations
Contributions
C.C.D. led the drafting of the first version of the manuscript. All authors contributed to and revised subsequent versions of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dorea, C.C., Karaulac, T., Namgyal, K. et al. Safely managed drinking water services in the Democratic People’s Republic of Korea: findings from the 2017 Multiple Indicator Cluster Survey. npj Clean Water 3, 28 (2020). https://doi.org/10.1038/s41545-020-0074-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41545-020-0074-6
- Springer Nature Limited
This article is cited by
-
SDG 6 progress analyses in sub-Saharan Africa from 2015–2020: the need for urgent action
Discover Water (2024)
-
Trends and impacts of demographic disparity on JMP ladders for drinking water and sanitation services: further analysis of the Ethiopian demographic and health surveys
Discover Water (2023)
-
Effect of demographic disparities on the use of the JMP ladders for water, sanitation, and hygiene services in Bishoftu Town, Ethiopia
Discover Water (2022)
-
Long-term water conservation is fostered by smart meter-based feedback and digital user engagement
npj Clean Water (2021)
-
Drinking water quality and the SDGs
npj Clean Water (2020)