
Abstract
This study aimed to describe trends in prevalence, awareness, treatment, and control in hypertension in Chengdu from 2000 to 2010. Two community-based cross sectional surveys were conducted among those aged 40–79 years in 2000 (n = 4850) and 2010 (n = 5456). Demographic characteristics, blood pressure (BP) and associated risk factors were examined. Mean systolic and diastolic BP increased from 117.8 ± 33.9 to 132.1 ± 21.2 mmHg (P < 0.001), and 75.3 ± 19.1 to 79.3 ± 11.2 mmHg (P < 0.001) over past decade, respectively. The prevalence of hypertension increased from 27.7 to 29.4% (P < 0.001). Awareness increased from 37.7 to 42.5% (P < 0.001). The overall treatment rate increased from 20.9 to 28.0% (P < 0.0001), while among subjects aware of hypertension, treatment increased from 46.9 to 65.8% (P < 0.001). In hypertensives, control increased from 6.8 to 6.9% (P = 0.6684). Nevertheless, in hypertensives aware and treated, control decreased from 32.5 to 24.3% (P = 0.020). Hypertension prevalence increased in the last decade, while awareness, treatment and control remained considerably low in Chengdu.
Similar content being viewed by others


Introduction
Cardiovascular disease is the leading cause of death in Chinese people aged 40 years and older1, 2. In the Chinese population, more than a quarter of adults have two cardiovascular risk factors (i.e., smoking, overweight, hypertension, dyslipidaemia, or hyperglycaemia), and at least 17% adults have three risk factors3. As a major risk factor of cardiovascular diseases, hypertension has become a common health challenge with rising prevalence and morbidity in China4, of which the overall prevalence is about 30%5.
Chengdu is the capital city of Sichuan, which is in southwestern China with a population of 132 million. Accompanied by industrialization and urbanization of Chengdu, unhealthy changes in lifestyle have increased the risk of chronic cardiovascular disease. However, evidence in support of hypertension trend is still not available in Chengdu.
Two epidemiological surveys were conducted from 1998 to 2000 and from 2008 to 2010, separately, in the community population aimed to investigate the impact of lifestyle changes on hypertension and related cardiovascular risk factors. The present study is a retrospective analysis of two surveys on prevalence, awareness, treatment, and control, as well as related risk factors for adults aged 40–79 years in Chengdu over past decade.
Results
A total of 4850 and 5456 adults were included in two surveys, respectively. Of these included individuals, 243 and 251 (5.0% and 4.6%) refused to accept examination or had missing data. 4607 and 5205 (95.0% and 95.4%) were eligible for analysis, respectively.
Demographic characteristics and related risk factors
The characteristics and cardiovascular risk factors of all participants are summarized in Tables 1 and 2. More female than male (P < 0.001) were included in 2010. Current smokers decreased over the past ten years (P < 0.001). And participants with DM increased sharply (P < 0.001). Mean BMI increased nearly 4 units in past ten years (P < 0.001). And the prevalence of being overweight increased more than 6% (P < 0.001). Moreover, the prevalence of being obese doubled over time (P < 0.001). Mean levels of total cholesterol(TC), low-density lipoprotein cholesterol(LDL), triglycerides(TG) and fasting plasma glucose (FPG) increased in 2010 compared with those in 2000 (All P < 0.001).
Trends in BP over ten years
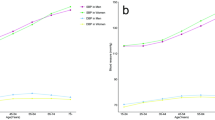
Both mean SBP and DBP increased over ten years (All P < 0.001). The mean levels of SBP/DBP were 117.8 ± 33.9/75.3 ± 19.1 mmHg (119.6 ± 38.8/76.8 ± 19.3 mmHg for men, 116.9 ± 31.0 mmHg/73.2 ± 18.2 mmHg for women) in 2000, and 132.1 ± 21.2/79.3 ± 11.2 mmHg (133.6 ± 20.4/80.8 ± 11.3 mmHg for men, 130.6 ± 22.0/77.7 ± 11.0 mmHg for women) in 2010, respectively. Mean levels of SBP and DBP were higher in 2010 than it in 2000 by age and sex (All P < 0.001). In both years, there was a trend that the levels of SBP and DBP were increasing with age (All P for trend < 0.05, Figs 1 and 2). Moreover, mean level of SBP in women aged 60 years and older was higher than that in men in both years. The highest DBP level in men was in the 50–59 year age group in both years, while in women, the highest DBP level was in the 70–79 year age group in 2000 and in the 60–69 year age group in 2010 (Figs 1 and 2).

Mean systolic blood pressure (SBP) across age groups by sex in 2000 and 2010.

Mean diastolic blood pressure (DBP) across age groups by sex in 2000 and 2010.
Trends in prevalence of hypertension and subtypes
The overall age-standardized prevalence of hypertension has increased nearly 2% in this population over past 10 years (P < 0.001, Table 3). The overall prevalence of hypertension was significantly higher in men than that in women (30.2% vs 23.4% in 2000, P < 0.001, and 31.0% vs 27.8% in 2010, P = 0.022, Table 3). In both surveys, the overall hypertension prevalence increased with age (Both P for trend < 0.001). In both surveys, the highest hypertension prevalence was among subjects aged 70 years and older.
The overall prevalence of pre-hypertension increased about 2% in past 10 years as well (P < 0.001, Table 3). It was different from hypertension that the prevalence was decreasing with age in both surveys (Both P for trend < 0.001). And the overall pre-hypertension prevalence was higher among men than women (35.3% vs 32.7% in 2000, P = 0.059, 41.7% vs 33.0% in 2010, P < 0.001, Table 3). In 2010, the highest pre-hypertension prevalence was in subjects aged 50–59 years, compared subjects aged 60-69 years in survey 2000.
The overall prevalence of isolated systolic hypertension (ISH) in 2010 was double that of the 2000 (Table 3). The overall ISH prevalence increased with age in both surveys. Moreover, in subjects aged 60 years and older, the ISH prevalence increased sharply significantly.
The overall prevalence of IDH in 2010 decreased almost 40% compared with that in 2000 (P < 0.001). In both surveys, there was a trend that the prevalence decreased with age. Moreover, the prevalence was the highest among subjects aged 40–49 years in both years and the prevalence in each age group in 2000 was higher than that in 2010 (Table 3).
The overall prevalence of SDH increased about 4% in past decade (10.8% in 2000 vs 14.9% in 2010, P < 0.001). In both surveys, the SDH prevalence increased with age and the prevalence of SDH was higher for men than women in each age group (Table 3).
Changes in constituent ratio
In 2000, the prevalence of IDH and SDH were higher than that of ISH. However, the prevalence of ISH and SDH were much higher than that of IDH in 2010 (All P < 0.001, Fig. 3). Over past 10 years, the prevalence of ISH and SDH increased while IDH prevalence decreased (All P < 0.001).

Changes in constituent ratio of hypertension subtypes (ISH = isolated systolic hypertension, IDH = isolated diastolic hypertension, SDH = systolic-diastolic hypertension) over decade.
Trends in awareness, treatment and control of hypertension
The overall awareness slightly increased from 37.7% in 2000 to 42.5% in 2010 (P < 0.001). This descent was present in both sexes, and especially noticeable in women (Table 4). While awareness of hypertension was higher among women compared with men. The overall treatment prevalence in overall community population increased nearly 8% over past ten years (P < 0.001). The increase was larger in women than in men.
Among those who were aware their hypertension, the treatment rose from 46.9% (in 2000) to 65.8% (in 2010) significantly (P < 0.001, Table 4). Among overall population who were aware of hypertension, treatment was higher in women than that in men in 2010, while it was lower in 2000. However, the increases of treatment rate among those aware was higher in women than it in men (men: 16.3%, women: 21.9%). Overall control increased only 0.1% with no significance (6.8% to 6.9%, P = 0.668) over the past ten years. Among treated hypertensives, control (BP < 140/90 mmHg) was 32.5% in 2000, compare to 24.3% in 2010 (P = 0.020, Table 2). Control was also higher in women than in men in both years. Moreover, there was more decreasing of control in men than in women (decreases for men vs women = 8.5% vs 7.8%).
Discussion
The main findings of this study are as follows: among Chengdu residents aged 40 to 79 years, 1). SBP and DBP levels increase over past decade, 2) prevalence of hypertension and pre hypertension increase steadily with slowly increasing awareness, while treatment and control remain considerably low.
There were more women in survey 2010, mainly because many younger and middle aged men moved to work in more developed east coastal areas (i.e. Guangdong, Fujian, Zhejiang provinces) over past decade. The steadily increased BP level and prevalence may be related to lifestyle changes accompanying with industrialization and urbanization, such as high salt food6, rich fat food intake (Sichuan cuisine is characterized by pungent, hot, and salty flavors), and higher BMI7. Smoking8, 9 and work related stress are associated with hypertension development10. Accompanying with the industrialization and urbanization, increased stressful workload may involve in the hypertension prevalence increasing. Limited knowledge of hypertension prevention, diagnosis treatment and its relevant risk factors among community physicians and general population may contribute to the low awareness. Treatment of hypertension was improved with economic development in past decade, especially apparently among those were aware of their hypertension. Higher socioeconomic status could positively improve the awareness and control of hypertension, and people would also have a better compliance of medicine treatment. Accompanying with the rapid economic development of Sichuan, people changed their dietary habits with more unhealthy fatty and salty food, while tended to be more dependent on morden transportation daily. Meanwhile, more people gradually became to care more about their health and generally could relatively afford the disease cost during past decade. It could be one reason for the increasing hypertension prevalence accompanying by increasing awareness and treatment. While during past decade, no apparent control improvement in smoking and drinking, increasing overweight and obesity, and increasing lipid and glucose levels could interact and potentially contribute to the poor hypertension control. Besides, poor compliance with medication and lack of health eduction could also be important reasons for poor BP control.
During past decade, there was no increasing trend of SBP and DBP levels in America11, 12 during the past two decades and in Japan13, while there was a consistent decreasing of BP in Germany14, Spain15, Italy16 and Korean17. From 1988 to 2008, there was an increasing trend of hypertension prevalence in Americans aged 40 years and older11, however, the prevalence of hypertension in Japan13, Germany14, Italy16 and Korea17 decreased. Other Chinese studies in other areas18,19,20 also have found that there is an increasing trend of prehypertension and hypertension prevalence. A recent study in Chongqing20, which is a neighbor city of Sichuan with similar geographic, culture, and dietary background, reported that hypertension prevalence in local adults (23.4% in 2012 and 12.0% in 2002) doubled during past decade. The increasing trend of hypertension prevalence in our study is in accordance with studies in other Chinese cities, especially cities with similar background, and other developing countries, such as India21 and Thailand22. During the same period, the hypertension awareness and treatment in America11, 12, Germany14 and Korean17 increased substantially, which contributed to a better BP control. And awareness of hypertension in other areas in China tended to increase consistently18,19,20. Nevertheless the treatment in Chengdu is unluckily lower than in Shandong18, Beijing19, while higher than in Chongqing20, India21 and Thailand22. In past decade, the hypertension control doubled in Germany14, Spain15 and nearly doubled in America11 and it increased steadily in developed couriers, such as Italy16 and Korean17. Unfortunately, the hypertension control in Chengdu was low, which was in accordance with studies in other Chinese cities5, 18,19,20. It is apparently that improvements in hypertension awareness, treatment contributed to better control in european countries11, 12, 14,15,16.
Lifestyle modification contributing to BP decrease is recommend to general population in Chengdu. People should increase their physical activity, improve levels of fruit and vegetable intake, consume less fatty diet and quit smoking. A better community based primary health care and primary prevention system focused on early diagnosis and treatment, patients management, hypertension knowledge education and lifestyle risk factors modification in general population is needed for better BP control.
This study has following limitations. First, results of this study should be interpreted with caution, since both surveys only focused on population in Chengdu, although main results are comparable to studies in other Chinese cities. Second, the gender constituents in two separate surveys were different and quantity of physical activity was not measured in 2000. Third, due to the different economical support by the government, the methods for diabetes mellitus diagnoses were different in both surveys. Fourth, smoking and alcohol consumption data are based on self-report with the possibility of misclassification of exposure.
In conclusion, hypertension prevalence increased steadily among residents aged 40 to 79 years in Chengdu from 2000 to 2010, while awareness, treatment and control remained considerably low. More efforts should be taken to improve hypertension awareness, treatment and control among middle aged and older residents. Future enhanced public health care program focused on these problems is needed.
Materials and Methods
Population
Two cross-sectional surveys were conducted from 1998 to 2000 and from 2008 to 2010 separately in communities of Chengdu, using a multistage cluster sampling. The study population included 4850 and 5456 subjects aged 40–79 years (All subjects were Han ethnicity) living in Chengdu more than 3 years in survey 2000 and survey 2010, respectively. The response rates for the subjects participating in the surveys of 1999 and 2009 were 95.1% and 95.4%, respectively. Ethics approval was obtained from the Ethics Committee of the Second People’s Hospital of Chengdu, China. The methods in the study were in accordance with relevant guidelines and the Declaration of Helsinki. All participants gave informed consent.
Data collection
Data were collected through a standard household questionnaire interview with additional interviewing and a physical examination in community hospitals in both 2000 and 2010, separately. In both years, all researchers were trained for questionnaire administration, correct cuff size selecting, BP measurement and other techniques needed in surveys with standard techniques. The information collection included demographic characteristics, smoking, alcohol consumption, history of hypertension, cardiovascular disease, diabetes, and administration of antihypertensive medication, physical examination, waist circumference, body weight, and height. In both years, participants had their blood pressure (BP) measurements with a validated mercury sphygmomanometer by trained researchers. Three consecutive BP readings were taken on the right arm with an appropriate cuff size (22 to 26 cm long and 12 to 14 cm wide), in a sitting position after a 10 minutes rest. Participants were not allowed to smoke cigarettes, drink tea/coffee, or do physical exercise half an hour before BP measurements. The room temperature was required to be between 18 °C and 25 °C for measurements. Overnight fasting blood specimens of participants were collected and tested in the central laboratory of our hospital in both years. The oral glucose tolerance test (OGTT) was tested in all subjects in 2010, while not in 2000.
Definitions
In both years, BP level was defined as the mean value of three measurements and hypertension was defined as systolic blood pressure (SBP) ≥ 140 mmHg, or/and diastolic blood pressure (DBP) ≥ 90 mmHg, and/or normotensives treated with antihypertensive medications. Prehypertension was defined as 120 ≤ SBP < 140 mmHg or/and 80 ≤ DBP < 90 mmHg23, 24. Hypertension subtypes in surveys include: isolated systolic hypertension(ISH), defined as 140 mmHg ≤ SBP and DBP < 90 mmHg; isolated diastolic hypertension(IDH), defined as SBP ≤ 140 mmHg and 90 mmHg ≤ DBP; systolic - diastolic hypertension(SDH), defined as 140 mmHg ≤ SBP and 90 mmHg ≤ DBP23, 24.
Based on the 1999 World Health Organization standards, diabetes mellitus (DM) was defined as fasting plasma glucose > 7.0 mmol/l (in 2000), and by OGTT (2-h plasma glucose ≥ 11.1 mmol/l, in 2010).
Awareness of hypertension was determined by definite response to question “Have you ever been told that your blood pressure was high or you had a hypertension” by a physician/heath care. Treatment of hypertension was confirmed by saying “yes” to this question, “Are you taking antihypertension medication during last three months, because of your high BP/hypertension?”, Control of hypertension was defined as the measured SBP < 140 mmHg and DBP < 90 mmHg in patients with hypertension under antihypertension treatment23, 24.
Body mass index (BMI) was defined as weight (kg)/height (m2). Overweight was define as 25 kg/m2 ≤ BMI < 28 kg/m2. Individuals with a BMI of 30 kg/m2 or greater are defined as obese.
Statistical analysis
Participants were subdivided into 4 age groups: 40 to 49, 50 to 59, 60 to 69, and 70 to 79 years old. Statistical analysis was performed by using of SPSS17.0 for Windows (Chicago, IL, USA). Continuous variables were expressed by mean ± standard deviation. Categorical variables were expressed by percentage (%). Rate of awareness, treatment and control of hypertension were standardized by the China national census. Comparisons between groups used the Chi - Square Test for categorical variables and one way ANOVA for continuous variables. The Cochran - Mantel - Haenszel test was used to analyze for the trend of prevalence over various age groups. A two-sided P value of < 0.05 was considered to be statistically significant.
References
He, J. et al. Major causes of death among men and women in China. N Engl J Med 353, 1124–1134 (2005).
Yang, G. et al. Rapid health transition in China, 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet 381, 1987–2015 (2013).
Yang, Z. J. et al. Prevalence of cardiovascular disease risk factor in the Chinese population: The 2007-2008 china national diabetes and metabolic disorders study. Eur Heart J 33, 213–220 (2011).
Lewington, S. et al. The Burden of Hypertension and Associated Risk for Cardiovascular Mortality in China. JAMA. Intern Med 176, 524–532 (2016).
Wang, Y. et al. Burden of hypertension in China over the past decades: Systematic analysis of prevalence, treatment and control of hypertension. Eur J Prev Cardiol 23, 792–800 (2016).
Alam, S. & Johnson, A. G. A meta-analysis of randomised controlled trials (RCT) among healthy normotensive and essential hypertensive elderly patients to determine the effect of high salt (NaCl) diet of blood pressure. J Hum Hypertens 13, 367–374 (1999).
Gu, D. et al. Body weight and mortality among men and women in China. JAMA 295, 776–783 (2006).
Niskanen, L. et al. Inflammation, abdominal obesity, and smoking as predictors of hypertension. Hypertension 44, 859–865 (2004).
Bowman, T. S., Gaziano, J. M., Buring, J. E. & Sesso, H. D. A prospective study of cigarette smoking and risk of incident hypertension in women. J Am Coll Cardiol 50, 2085–2092 (2007).
Bojar, I., Humeniuk, E., Owoc, A., Wierzba, W. & Wojtyla, A. Exposing women to workplace stress factors as a risk factor for developing arterial hypertension. Ann Agric Environ Med 18, 175–182 (2011).
Egan, B. M., Zhao, Y. & Axon, R. N. Us trends in prevalence, awareness, treatment, and control of hypertension, 1988-2008. JAMA 303, 2043–2050 (2010).
Yoon, S. S. et al. Trends in blood pressure among adults with hypertension United States, 2003 to 2012. Hypertension 65, 54–61 (2015).
Hata, J. et al. Secular trends in cardiovascular disease and its risk factors in Japanese half-century data from the Hisayama Study (1961–2009). Circulation 128, 1198–1205 (2013).
Neuhauser, H. K., Adler, C., Rosario, A. S., Diederichs, C. & Ellert, U. Hypertension prevalence, awareness, treatment and control in Germany 1998 and 2008-11. J Hum Hypertens 29, 247–253 (2015).
Barrios, V. et al. Evolution of clinical profile, treatment and blood pressure control in treated hypertensive patients according to the sex from 2002 to 2010 in Spain. J Hypertens 33, 1098–1107 (2015).
Di Lonardo, A., Donfrancesco, C., Palmieri, L., Vanuzzo, D. & Giampaoli, S. Time Trends of High Blood Pressure Prevalence, Awareness and Control in the Italian General Population Surveys of the National Institute of Health. High Blood Press Cardiovasc Prev 24, 193–200 (2017).
Kim, H. J., Kim, Y., Cho, Y., Jun, B. & Oh, K. W. Trends in the prevalence of major cardiovascular disease risk factors among Korean adults results from the Korea National Health and Nutrition Examination Survey, 1998–2012. Int J Cardiol 174, 64–72 (2014).
Yang, J. et al. Prevalence of prehypertension and hypertension in a Chinese rural area from 1991 to 2007. Hypertens Res 33, 331–337 (2010).
Li, G., Hu, H., Dong, Z., Xie, J. & Zhou, Y. Urban and suburban differences in hypertension trends and self-care three population-based cross-sectional studies from 2005-2011. PLoS One 10, e0117999 (2015).
Liu, X. et al. Hypertension prevalence, awareness, treatment, control, and associated factors in Southwest China an update. J Hypertens 35, 637–644 (2017).
Anchala, R. et al. Hypertension in India: a systematic review and meta-analysis of prevalence, awareness, and control of hypertension. J Hypertens 32, 1170–1177 (2014).
Aekplakorn, W. et al. Changes in prevalence, awareness, treatment and control of hypertension in Thai population, 2004–2009: Thai National Health Examination Survey III-IV. J Hypertens 30, 1734–1742 (2012).
Chobanian, A. V. et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 report. JAMA 289, 2560–2572 (2003).
The sixth report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Arch Intern Med. 157:2413–2446 (1997).
Acknowledgements
Authors thank all participants in both surveys. We also appreciate Ms. Huixing Yang for secretarial contribution. Survey in 2010 was supported by the Science and Technology Bureau of Chengdu (Grant number: 07YTYB959SF-020). This study was supported by the Science and Technology Bureau of Chengdu (Grant number: 11PPYB034SF-289). The sponsor played no role in the study.
Author information
Authors and Affiliations
Contributions
G. H. and J.B. X. contribute equally to this manuscript and are co-first authors. T.J. Z., G. H. and J.B. X. contributed to study concept and design, data analysis and interpretation, and manuscript draft. Y. L., Z.H. L., Y.L. Z., Y.L. W., R.L. W. and S. Z. contributed to study conduct and data acquisition.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Huang, G., Xu, Jb., Liu, Y. et al. Temporal trends in Prevalence, Awareness, Treatment, and Control of Hypertension from 2000 to 2010 in Chengdu, China. Sci Rep 7, 8964 (2017). https://doi.org/10.1038/s41598-017-09579-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-09579-2
- Springer Nature Limited
This article is cited by
-
Prevalence, awareness, treatment, and control of hypertension in southwestern China
Scientific Reports (2019)