
Abstract
To evaluate the change over time of vision-related quality of life (QoL) and glaucoma symptoms in a population of newly-diagnosed primary open angle glaucoma (POAG) patients. Multicenter, prospective study. Consecutive newly-diagnosed POAG patients were enrolled and followed-up for one year. Follow-up visits were scheduled at 6 and 12 months from baseline. At each visit, vision-related QoL and glaucoma-related symptoms were assessed by the means of the 25-item National Eye Institute Visual Function Questionnaire (NEI-VFQ-25) and the Glaucoma Symptom Scale (GSS), respectively. Trends over time for NEI-VFQ-25 and GSS scores were evaluated with longitudinal linear mixed models. One-hundred seventy-eight patients were included in the analysis. At baseline, early to moderate glaucoma stages were associated with higher scores for most GSS and NEI-VFQ-25 items, while lower best-corrected visual acuity was associated with lower scores for 4 of the 12 NEI-VFQ-25 items. During the follow-up, all the GSS scores, the NEI-VFQ-25 total score, and 7 of the 12 NEI-VFQ-25 scores significantly improved (p < 0.05). In multivariate model, higher increases of most GSS and NEI-VFQ-25 scores were modeled in patients with low scores at baseline. Vision-related QoL and glaucoma-related symptom perception significantly improved during the one-year follow-up in this population of newly diagnosed POAG patients.
Similar content being viewed by others


Introduction
Glaucoma, one of the leading causes of blindness in the world1, is characterized by progressive visual field (VF) deterioration and optic disc damage2. Primary open angle glaucoma (POAG), the most common type of glaucoma in white populations3, has a chronic course with functional impairment developing over years. Although glaucoma is an irreversible disease, its progression may be delayed with appropriate medical and surgical management4,5,6.
In recent years, quality of life (QoL) has assumed a leading role in health-care, and its preservation is now one of the main goals of treatment7,8. As a chronic disease, POAG may affect QoL9,10,11,12,13,14. VF loss and central visual acuity impairment may limit daily activities, such as reading15,16, walking17 or driving18,19. Additionally, topical medications20,21, surgical interventions22,23 and the need for long-term care are additional factors that can significantly affect QoL.
Several studies have evaluated QoL in glaucoma and the association with its clinical aspects, such as VF damage (VFD)9,10,24,25 and best corrected visual acuity (BCVA) deterioration24,26, or the presence of unilateral versus bilateral disease27,28. A significant correlation between disease severity and the impairment of QoL has been found using either generic or vision-specific instruments14. However, the majority of these studies had a cross-sectional design, whereby data collected at a single time-point were analyzed. Differently, the Collaborative Initial Glaucoma Treatment Study (CIGTS) prospectively evaluated QoL changes in newly-diagnosed glaucoma patients, randomized to medical or surgical treatment, over a 5-year follow-up23. As a result, the overall trend was a decline in the percent of participants of both groups reporting the presence of functional and local symptoms over time, suggesting an improvement of patient’s QoL perception. However, the CIGTS used a proprietary multidimensional instrument developed by the CIGTS investigators, and interviews were performed by phone. No other study subsequently applied the same QoL instrument.
The Italian Primary Open Angle Glaucoma Study (IPOAGS) is a multicenter study designed to evaluate vision-related QoL in Italian POAG patients29,30,31. The IPOAGS consists of a cross-sectional and a prospective part. The present report describes the results of the prospective part, the aim of which was to assess possible changes in vision-related QoL and symptom perception over time, and to identify patterns of QoL modification according to the characteristics of the disease.
Material and Methods
The design and methods of the IPOAGS have been described elsewhere29,30,31. Briefly, previously or newly diagnosed POAG patients aged 18 or more were consecutively enrolled during routine visits at 21 academic and non-academic centers in Italy. In the cross-sectional part of the study, vision-related QoL data were collected and their association with both clinical and socio-demographic variables was investigated29,30. In the prospective part of the study, consecutive newly-diagnosed glaucoma patients were evaluated at baseline and were followed-up for one year.
Informed consent was obtained from all the participants before any study-related procedure and after the nature and the purpose of the investigation were fully explained. The study was conducted in accordance with the tenets of the Declaration of Helsinki and the Guidelines for Good Clinical Practice. The Institutional Review Board of Brescia (Brescia, Italy) and of each participating center approved the protocol. The study was registered at clinicaltrials.gov (NCT01742104).
Interventions
Newly-diagnosed POAG patients underwent a comprehensive ophthalmological examination at baseline and at each follow-up visit. Follow-up study visits were scheduled at 6 and 12 months from baseline, however interim visits were allowed at clinician discretion, to adjust therapy and evaluate target IOP. Treatment was initiated, at the end of the baseline visit, to avoid an influence of drugs and interventions on QoL assessment. At baseline and at 6- and 12-month follow-up visits, VF examination was performed and vision-related QoL and glaucoma symptom perception questionnaires were administered.
POAG was defined as a typical optic neuropathy with a focal, generalized or focal/generalized neuroretinal thinning or an inter-eye cup/disc ratio asymmetry >0.2. The presence of typical glaucomatous VF defects was not a prerequisite for inclusion, if the investigator’s clinical judgment was strongly in favor of POAG (e.g. due to high intraocular pressure (IOP), retinal nerve fiber layer defects or optic disc hemorrhages)32.
Vision-related QoL was assessed using the validated Italian version of the 25-item National Eye Institute Visual Function Questionnaire (NEI-VFQ-25)33, while glaucoma-related symptoms were assessed using the validated Italian version of the Glaucoma Symptom Scale questionnaire (GSS)34.
The NEI-VFQ-25 is a self-administered questionnaire, developed to investigate vision-related QoL35. It consists of 25 vision-targeted questions, representing 11 vision-related constructs (general vision, ocular pain, near activities, distance activities, social functioning, mental health, role difficulties, dependency, driving, color vision and peripheral vision), plus an additional single-item question for general health rating. The scoring procedure converts the pre-coded numeric values of each item to a score ranging from 0 to 100. Higher scores reflect better vision-related QoL. The total score is the mean of all the vision-targeted subscales scores.
The GSS is a glaucoma-specific tool designed for the investigation of symptoms in patients with glaucoma36. It was developed as a modified instrument from a checklist of symptoms applied in the Ocular Hypertension Treatment Study36. It includes 10 items grouped in two domains: Symp-6 for non-visual symptoms (burning/smarting/stinging, tearing, dryness, itching, soreness/tiredness, feeling of something in the eye) and Func-4 for visual symptoms (blurry/dim vision, hard to see in daylight, hard to see in darkness, and halos around the lights). Each item can take a score from 0 to 100, where 0 indicates very bothersome symptoms and 100 the absence of symptoms. The domain score is the mean from the items of the relative domain, while the total GSS score is the mean from all items of both domains. Each eye is tested separately.
Visual field and stage of the disease
A reliable VF examination at baseline (i.e. false-positive responses <15% with a clear blind-spot at the VF printout, threshold value <10 dB) was required for study inclusion. Severity of VF impairment was classified at baseline and at each follow-up visit according to the Glaucoma Staging System 2 (GStag2)37,38. GStag2 is a classification method using Mean Deviation (MD) or Mean Defect and Pattern Standard Deviation/Corrected Pattern Standard Deviation (PSD/CPSD) and Loss Variation/Corrected Loss Variation (LV/CLV) values (from either the 30-2/24-2 Zeiss-Humphrey tests or the G1/G1X/G2 Octopus programs) to create a Cartesian coordinate diagram. VF is classified into seven different stages by curvilinear lines from stage 0 (normal VF) to stage 5 (low threshold readings, with only small remnants of sensitivity). GStag2 has been validated in population-based studies39,40,41,42,43 and has been shown to be similar or superior to other VF classification systems44. The improvement of performance in perimetric tests is a well-known phenomenon, called “learning effect”. To prevent bias, the “worst value carry backward” method was used: for each eye, the highest value of glaucoma stage during the follow-up replaced the earlier values.
Statistical analysis
All the tests were performed considering patient as unit of analysis. In patients with bilateral disease, arithmetical means of BCVA and MD were computed, while the lowest GSS score and the worst stage of the disease were chosen.
For statistical purposes, stage of the disease was categorized as follows: early (stage 0, borderline and 1), moderate (stage 2 and 3) and severe (stage 4 and 5). BCVA was dichotomized as ≤ or >0.15 LogMar. Since the information on prescribed treatments were collected at fixed time-points (baseline, 6 and 12-month visits), but treatment variation was at clinician’s discretion during the follow-up, data from 6-month visit were taken as a representative proxy of the entire follow-up.
Vision-related QoL and symptom scores expressed as a mean of different subscale scores (e.g. total NEI-VFQ-25 or total GSS scores) were treated as continuous variables. Single-item scores and scores with a value of 100 for more than 50% of the interviewed subjects were treated as dichotomous variables. In this case, “1” was assigned to the maximum score of 100, and “0” to other values. Dichotomized variables, exclusively for the NEI-VFQ-25 were: distance activities, color vision, peripheral vision, social functioning, role difficulties and dependency.
NEI-VFQ-25 and GSS scores at baseline were investigated by the means of multivariable general linear models and logistic models. Vision-related QoL and symptom scores over time were modeled as a linear function of time. A multivariable analysis including time, baseline QoL scores and their interaction with time and covariates was performed. The adjustment for baseline QoL scores and interaction with time was performed taking into account regression toward the mean and ceiling effect. Longitudinal linear mixed models and generalized longitudinal mixed models for binary data with a marginal logit link function (modeled the probability of score = “100”) were used for the analyses of dichotomized scores. The effect of time was modeled as a linear function. Random intercepts and random slopes for time effect were introduced to interpolate the subject-specific deviations from the score trends.
A significance level of p < 0.05 was set. All the analyses were performed with SAS software (version 9.4).
Results
From March 2012 to July 2013, one hundred ninety-seven newly-diagnosed POAG patients were enrolled. Nineteen patients were then excluded from the analysis, 11 because they did not have follow-up data and 8 because they did not have data on anti-glaucoma prescriptions. Therefore, analyses were performed on 178 subjects.
Demographic characteristics of the study participants are presented in Table 1. Mean age was 61.7 years (SD 14.3), and 52.8% of the participants were females. Mean values for MD and BCVA were −4.5 dB (SD 5.3) and 0.1 LogMar (SD 0.1). According to the GStag2, disease severity was classified as early (stage 0, borderline ad 1) in 95 patients (53.3%), moderate (stage 2 and 3) in 56 patients (31.5%) and severe (stage 4 and 5) in 27 patients (15.2%). After the baseline visit, all the patients were administered one or more hypotensive topical medications (Table 2). Eighty-nine patients (50%) were administered a prostaglandin analogue alone, while a β-blocker was administered in 53 patients (29.8%). Thirty patients (16.8%) received more than one topical agent as a first-line therapy. During the follow-up, 8 patients (4.4%) underwent surgery and 27 patients received laser treatment (i.e. selective laser trabeculoplasty, 15.2%), in addition to medical therapy.
Vision-related QoL scores at baseline
Results of multivariable analyses on baseline QoL scores are showed in Table 3. Being a man (p = 0.03) and having an early/moderate vs. severe stage of the disease (p < 0.01) were variables associated with higher values of GSS Func-4 score at baseline. Early or moderate vs. severe stages of the disease were associated with higher values of most NEI-VFQ-25 scores, with the exception of general health (p = 0.06) and ocular pain (p = 0.11). BCVA was significantly related to total NEI-VFQ-25 score and to 3 of the 12 NEI-VFQ-25 subscale scores (near activities: p = 0.01, role difficulties: p < 0.01 and driving: p < 0.01). Being a man was associated with higher NEI-VFQ-25 driving score (p < 0.01).
Vision-related QoL and symptom score change over time
GSS and NEI-VFQ-25 scores at baseline and at all follow-up visits are presented in Table 4. Mean baseline scores were higher than 75 in all the subscales, with the exception of NEI-VFQ-25 general health (60.4, SD 17.0), and NEI-VFQ-25 general vision (65.8, SD 15.4) scores. Color vision had the highest score (94.2, SD 8.0), followed by social functioning (97.7, SD 6.9) and dependency (95.5, SD 12.6). NEI-VFQ-25 and GSS total scores were 88.3 (SD 11.3) and 78.1 (SD 18.0), respectively. Over the 1-year follow-up, both the NEI-VFQ-25 and the GSS scores increased. The increase of all the GSS scores, the NEI-VFQ-25 total score and 7 of the 12 NEI-VFQ-25 subscale scores (general health, general vision, ocular pain, near activities, mental health, role difficulties and driving) was significant. Trends over time for the GSS and the NEI-VFQ-25 total scores and for the main subscale scores are presented in Fig. 1.

Trends over time of Glaucoma Symptom Scale (GSS) and 25-item National Eye Institute Visual Function Questionnaire (NEI-VFQ-25) scores. (A) Trends over time of GSS total score, Function-4 and Symptoms-6 subscale scores; (B) Trends over time of NEI-VFQ-25 total score, general health and general vision subscale scores.
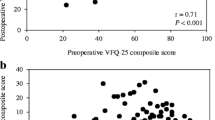
Results of multivariable analyses on NEI-VFQ-25 and GSS scores over time are reported in Table 5. A significant negative interaction was observed between time and all the GSS scores, the NEI-VFQ-25 total score and 8 of the 12 NEI-VFQ-25 subscale scores at baseline (general health, general vision, ocular pain, near activities, social functioning, mental health, role difficulties and dependency). As a result, a lower baseline score was related to a higher increase of the score during the follow-up (Fig. 2). A negative interaction between time and baseline stage of the disease was found for GSS Func-4 score (p < 0.01) and NEI-VFQ-25 ocular pain score (p = 0.02) (Fig. 3). In thise case, lower glaucoma stages at baseline (i.e. early or moderate disease) were associated with higher increase of QoL score over time. With regard to NEI-VFQ-25 dichotomized scores, a significant interaction between stage of the disease and time was detected on vision-specific role difficulties (p = 0.01, Fig. 4A) and peripheral vision (p = 0.016, Fig. 4B, available online) scores. This means that patients without a maximum score (<100) and with an early to moderate disease at baseline, had a high probability to achieve the maximum score during the follow-up. Patients with a maximum QoL score (100) at baseline and a severe disease, more easily experienced a QoL score reduction over time.

Estimated quality of life scores by time and covariates (multivariable analysis). (A) Estimated GSS Symp-6 (Symptoms), Func-4 (Function) and Total score variations over time, according to score at baseline; (B) Estimated NEI-VFQ-25 General Health, General Vision and Total score variations over time, according to score at baseline.

Estimated quality of life scores by time and covariates (multivariable analysis). (A) Estimated GSS Func-4 score variation over time, according to score at baseline and baseline stage of the disease; (B) Estimated NEI-VFQ-25 Ocular Pain score variation over time, according to score at baseline and baseline stage of the disease.

Estimated probability to achieve maximum qualitative QoL score (100) by time and covariates. (A) Probability over time to achieve NEI-VFQ-25 Vision-specific Role Difficulties maximum score (100), according to score at baseline and baseline stage of the disease; (B) Probability to achieve NEI-VFQ-25 Peripheral Vision maximum score (100), according to score at baseline and baseline stage of the disease.
Discussion
Several cross-sectional studies have found a significant association between VF and BCVA deterioration and vision-related QoL in glaucoma patients”. However, only a few studies investigated QoL with a prospective design23,24. The present study aimed to evaluate vision-related QoL and glaucoma-related symptom perception both at baseline and prospectively, in a group of newly-diagnosed glaucoma patients followed-up for one year. As a result, GSS and NEI-VFQ-25 scores were generally high at baseline (i.e. >75), indicating that this population of newly-diagnosed glaucoma patients perceived a high level of QoL. Stage of the disease and BCVA were the most important determinants of QoL at baseline. As GStag2 resides entirely on VFD, these findings are not surprising and are in agreement with previous cross-sectional studies, where a significant correlation between both VF and BCVA with QoL was found9,10,23. In a recent study analyzing QoL of patients enrolled in the Early Manifest Glaucoma Trial and followed-up for 20 years, visual acuity and VF index were the only significant variables influencing QoL, accounting for nearly 40% of NEI-VFQ-25 scores9. On the other hand, both visual acuity and VF scores were weakly but significantly associated with QoL measures in newly-diagnosed glaucoma patients enrolled in the CIGTS10. Beside these data, it is unknown if QoL in glaucoma is more affected by VFD or BCVA deterioration. In the present study, stage of the disease was associated with 2 of the 3 GSS scores at baseline, and with all the NEI-VFQ-25 scores, with the exception of general health and ocular pain. BCVA was associated with only 3 of the 12 NEI-VFQ-25 scores and with total NEI-VFQ-25 score. These results probably suggest a prominent role of VFD as a determinant of QoL in newly-diagnosed glaucoma patients, albeit further researches are needed to confirm these findings.
Men showed a higher perception of their visual function at baseline (GSS Func-4 score), and were more confident at driving than women (NEI-VFQ-25 driving score). Sex-related psychological profiles are likely involved in these results. Previous studies have found women to be more prone to reporting symptoms than men45,46 and to engage more easily in illness behaviors46. Nevertheless, anxiety and depression, two common responses to the diagnosis of a chronic illness47 are more common in women than men48,49,50. Our results about driving are in agreement with the conclusions of previous studies, where women with glaucoma were more likely to cease driving than men18,51.
In our study NEI-VFQ-25 total score and most of the NEI-VFQ-25 subscale scores significantly increased from baseline to the 1-year follow-up visit, which suggests a general pattern of improvement in vision-related QoL. Similarly, the GSS total score as well as symptom and function subscale scores improved, which suggests a blunting of glaucoma-related symptom perception over time. Reason of this change is unknown, however adaptation to glaucoma diagnosis may be involved. Adaptation to a chronic illness is a well-known phenomenon in general medicine, and has been extensively investigated52,53,54,55. Several reports from different disciplines have highlighted the role of adaptation to the diagnosis and its impact on QoL of various chronic diseases and disabilities56,57,58. Adaptation theories have been also translated into clinically meaningful rehabilitation programs57. Little is known about the effects of adaptation to the diagnosis of glaucoma, and a few studies have investigated this phenomenon. Interestingly, in many participants of the CIGTS, the diagnosis of glaucoma engendered an immediate response of fear of blindness59. However, the percentage of respondents who reported moderate or significant apprehension dropped from 34% at baseline to less than 15% after 12 months. In the same study, a slight but significant decline in symptom scale scores was recorded during the follow-up, indicating an improvement in the perception of glaucoma-related symptoms23. Psychological adaptation to the diagnosis of glaucoma was offered as an explanation of these results, while less convincing was the hypothesis of a diminution or cessation of the particular problem.
Two variables greatly influenced QoL score change over time in our study: QoL score at baseline and stage of the disease. While the interaction of time with baseline QoL scores was significant over most GSS and NEI-VFQ-25 scores, the interaction of baseline stage with time was significant only for GSS Function-4 score and NEI-VFQ-25 ocular pain, role difficulties and peripheral vision scores. According with this analysis, higher QoL score increase over time was modeled in patients with lower QoL score at baseline and less advanced disease. Both psychological and clinical factors are likely to be involved in these results. Psychological impact of the diagnosis of a chronic illness is quite different according to personality traits and life expectation60,61. The process of adaptation may mitigate the initial response over time, and a greater increase in QoL scores may be expected in patients that initially negatively reacted to the diagnosis. While psychological factors may be alleviated over time, functional factors persist, and their effect on QoL is likely to be permanent. As a consequence, patients with severe disease at baseline had a trend towards a stabilization or a reduction of their QoL scores over time, irrespectively of score values at baseline.
All the patients included in this study were administered topical hypotensive medications after the baseline visit. Moreover, 27 patients underwent laser treatment and 8 patients underwent surgery during the follow-up. Glaucoma medications may affect QoL, due to the local side effects (burning, stinging, blurred vision, etc.), and the bothersomeness of time-fixed administrations, potentially interfering with daily routine62,63. In our study a trend towards an increase in the number of topical agents per patient was found over time. This is not surprising, as it’s common practice to initiate glaucoma therapy with a single agent and add further medications if target IOP is not achieved. Despite the raise in medication number, QoL scores increased over the follow-up, including the GSS Symp-6 score, that specifically evaluates local symptoms (burning/smarting/stinging, tearing, dryness, itching, soreness/tiredness, feeling of something in the eye). Moreover, when patients were dichotomized according to the number of topical treatments received (one vs. more than one), no significant interaction with time was found. These results are somehow unexpected. However, it is possible that the mechanism of adaptation may be valid not only for the psychological burden of a new diagnosis, but also for the symptoms of the disease and its treatment23.
Our study has a number of limitations. First, no rigorous methodology for VF progression evaluation was adopted, as the follow-up was considered too short for a such analysis. However, taking into account the mild VFD at baseline (mean MD: −4.5 ± 5.3), it is unlikely that VF changes had an effect on QoL, with the obvious exception of patients with very fast progression and very high IOP. Second, data from both eyes were included in the analysis, when available. It is debated if vision-related QoL in glaucoma patients is more dependent on the patients’ better eye, worse eye or a combination thereof9,17,27,64. The decision to include data from both eyes of participants with bilateral disease was made in an attempt to obtain a model that reflects the real-life perception of patients as closely as possible. Third, patients were treated at physician’s discretion during the follow-up, in order to delay the progression of the disease. A precise evaluation of QoL and symptoms in surgically-treated patients was not feasible, due to the low number of patients that underwent surgery during the follow-up. On the other hand, all the patients receiving laser treatment were simultaneously treated with topical medical therapy, so it is reasonable to suppose that QoL and symptoms in this group were similar to the rest of the studied population.
In conclusion, this study has demonstrated an increase in vision-related QoL scores and a reduction in glaucoma-related symptom perception over one-year follow-up in a population of newly-diagnosed glaucoma patients. Although the precise explanation for these findings is uncertain, psychological processes and adaptation to the diagnosis of a chronic illness might have played a role. Future research is warranted in order to evaluate possible changes of vision-related QoL in a larger sample of glaucoma patients with a more extended follow-up.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Change history
06 March 2020
An amendment to this paper has been published and can be accessed via a link at the top of the paper.
References
Tham, Y. C. et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology 121, 2081–2090, https://doi.org/10.1016/j.ophtha.2014.05.013 (2014).
Goldberg, I. Optic disc and visual field changes in primary open angle glaucoma. Aust J Ophthalmol 9, 223–229 (1981).
Giangiacomo, A. & Coleman, A. L. In Glaucoma (eds Franz Grehn & Robert Stamper) Ch. 2, 13–21 (Springer-Verlag, 2009).
The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration.The AGIS Investigators. Am J Ophthalmol 130, 429–440 (2000).
Heijl, A. et al. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol 120, 1268–1279 (2002).
Musch, D. C. et al. Visual field progression in the Collaborative Initial Glaucoma Treatment Study the impact of treatment and other baseline factors. Ophthalmology 116, 200–207, https://doi.org/10.1016/j.ophtha.2008.08.051 (2009).
Prum, B. E. Jr. et al. Primary Open-Angle Glaucoma Preferred Practice Pattern((R)) Guidelines. Ophthalmology 123, P41–P111, https://doi.org/10.1016/j.ophtha.2015.10.053 (2016).
European Glaucoma Society. Terminology and Guidelines for Glaucoma, IV Edition, (PubliComm, 2014).
Peters, D., Heijl, A., Brenner, L. & Bengtsson, B. Visual impairment and vision-related quality of life in the Early Manifest Glaucoma Trial after 20 years of follow-up. Acta Ophthalmol 93, 745–752, https://doi.org/10.1111/aos.12839 (2015).
Janz, N. K. et al. Quality of life in newly diagnosed glaucoma patients: The Collaborative Initial Glaucoma Treatment Study. Ophthalmology 108, 887–897; discussion 898 (2001).
Wolfram, C., Lorenz, K., Breitscheidel, L., Verboven, Y. & Pfeiffer, N. Health- and vision-related quality of life in patients with ocular hypertension or primary open-angle glaucoma. Ophthalmologica 229, 227–234, https://doi.org/10.1159/000350553 (2013).
McKean-Cowdin, R. et al. Impact of visual field loss on health-related quality of life in glaucoma: the Los Angeles Latino Eye Study. Ophthalmology 115, 941–948 e941, https://doi.org/10.1016/j.ophtha.2007.08.037 (2008).
Gupta, V. et al. Utility values among glaucoma patients: an impact on the quality of life. Br J Ophthalmol 89, 1241–1244, https://doi.org/10.1136/bjo.2005.068858 (2005).
Quaranta, L. et al. Quality of Life in Glaucoma: A Review of the Literature. Adv Ther 33, 959–981, https://doi.org/10.1007/s12325-016-0333-6 (2016).
Ramulu, P. Glaucoma and disability: which tasks are affected, and at what stage of disease? Curr Opin Ophthalmol 20, 92–98, https://doi.org/10.1097/ICU.0b013e32832401a9 (2009).
Freeman, E. E., Munoz, B., West, S. K., Jampel, H. D. & Friedman, D. S. Glaucoma and quality of life: the Salisbury Eye Evaluation. Ophthalmology 115, 233–238, https://doi.org/10.1016/j.ophtha.2007.04.050 (2008).
Turano, K. A. et al. Association of visual field loss and mobility performance in older adults: Salisbury Eye Evaluation Study. Optom Vis Sci 81, 298–307 (2004).
Ramulu, P. Y., West, S. K., Munoz, B., Jampel, H. D. & Friedman, D. S. Driving cessation and driving limitation in glaucoma: the Salisbury Eye Evaluation Project. Ophthalmology 116, 1846–1853, https://doi.org/10.1016/j.ophtha.2009.03.033 (2009).
Gilhotra, J. S., Mitchell, P., Ivers, R. & Cumming, R. G. Impaired vision and other factors associated with driving cessation in the elderly: the Blue Mountains Eye Study. Clin Exp Ophthalmol 29, 104–107 (2001).
Balkrishnan, R., Bond, J. B., Byerly, W. G., Camacho, F. T. & Anderson, R. T. Medication-related predictors of health-related quality of life in glaucoma patients enrolled in a medicare health maintenance organization. Am J Geriatr Pharmacother 1, 75–81 (2003).
Hugues, F. C. & Le Jeunne, C. Systemic and local tolerability of ophthalmic drug formulations. An update. Drug Saf 8, 365–380 (1993).
Burr, J., Azuara-Blanco, A., Avenell, A. & Tuulonen, A. Medical versus surgical interventions for open angle glaucoma. Cochrane Database Syst Rev, CD004399, https://doi.org/10.1002/14651858.CD004399.pub3 (2012).
Janz, N. K. et al. The Collaborative Initial Glaucoma Treatment Study: interim quality of life findings after initial medical or surgical treatment of glaucoma. Ophthalmology 108, 1954–1965 (2001).
Hyman, L. G. et al. Treatment and vision-related quality of life in the early manifest glaucoma trial. Ophthalmology 112, 1505–1513, https://doi.org/10.1016/j.ophtha.2005.03.028 (2005).
Iester, M. & Zingirian, M. Quality of life in patients with early, moderate and advanced glaucoma. Eye (Lond) 16, 44–49, https://doi.org/10.1038/sj.eye.6700036 (2002).
Kobelt, G. et al. Cost-effectiveness analysis in glaucoma: what drives utility? Results from a pilot study in Sweden. Acta Ophthalmol Scand 84, 363–371, https://doi.org/10.1111/j.1600-0420.2005.00621.x (2006).
van Gestel, A. et al. The relationship between visual field loss in glaucoma and health-related quality-of-life. Eye (Lond) 24, 1759–1769, https://doi.org/10.1038/eye.2010.133 (2010).
Sawada, H., Yoshino, T., Fukuchi, T. & Abe, H. Assessment of the vision-specific quality of life using clustered visual field in glaucoma patients. J Glaucoma 23, 81–87, https://doi.org/10.1097/IJG.0b013e318265bbdc (2014).
Floriani, I. et al. Health-related quality of life in patients with primary open-angle glaucoma. An Italian multicentre observational study. Acta Ophthalmol, https://doi.org/10.1111/aos.12890 (2015).
Rulli, E. et al. Visual field loss and vision-related quality of life in the Italian Primary Open Angle Glaucoma Study. Sci Rep 8, 619, https://doi.org/10.1038/s41598-017-19113-z (2018).
Riva, I. et al. Influence of Socio-demographic Factors on Disease Characteristics and Vision-related Quality of Life in Primary Open Angle Glaucoma Patients. The Italian Primary Open Angle Glaucoma Study (IPOAGS). J Glaucoma, https://doi.org/10.1097/IJG.0000000000000989 (2018).
Topouzis, F. et al. Factors associated with undiagnosed open-angle glaucoma: the Thessaloniki Eye Study. Am J Ophthalmol 145, 327–335, https://doi.org/10.1016/j.ajo.2007.09.013 (2008).
Rossi, G. C., Milano, G. & Tinelli, C. The Italian version of the 25-item National Eye Institute Visual Function Questionnaire: translation, validity, and reliability. J Glaucoma 12, 213–220 (2003).
Rossi, G. C. et al. The Italian version of the Glaucoma Symptom Scale Questionnaire: translation, validation, and reliability. J Glaucoma 22, 44–51, https://doi.org/10.1097/IJG.0b013e318225406c (2013).
Mangione, C. M. et al. Development of the 25-item National Eye Institute Visual Function Questionnaire. Arch Ophthalmol 119, 1050–1058 (2001).
Lee, B. L. et al. The Glaucoma Symptom Scale. A brief index of glaucoma-specific symptoms. Arch Ophthalmol 116, 861–866 (1998).
Brusini, P. Clinical use of a new method for visual field damage classification in glaucoma. Eur J Ophthalmol 6, 402–407 (1996).
Brusini, P. & Filacorda, S. Enhanced Glaucoma Staging System (GSS 2) for classifying functional damage in glaucoma. J Glaucoma 15, 40–46 (2006).
Zheng, Y. et al. Diagnostic ability of Heidelberg Retina Tomography in detecting glaucoma in a population setting: the Singapore Malay Eye Study. Ophthalmology 117, 290–297, https://doi.org/10.1016/j.ophtha.2009.07.018 (2010).
Le, P. V. et al. Advanced imaging for glaucoma study: design, baseline characteristics, and inter-site comparison. Am J Ophthalmol 159, 393–403 e392, https://doi.org/10.1016/j.ajo.2014.11.010 (2015).
Roh, K. H., Jeoung, J. W., Park, K. H., Yoo, B. W. & Kim, D. M. Long-term reproducibility of cirrus HD optical coherence tomography deviation map in clinically stable glaucomatous eyes. Ophthalmology 120, 969–977, https://doi.org/10.1016/j.ophtha.2012.11.008 (2013).
Fogagnolo, P. et al. Long-term perimetric fluctuation in patients with different stages of glaucoma. Br J Ophthalmol 95, 189–193, https://doi.org/10.1136/bjo.2010.182758 (2011).
Frezzotti, P. et al. Association between primary open-angle glaucoma (POAG) and WDR36 sequence variance in Italian families affected by POAG. Br J Ophthalmol 95, 624–626, https://doi.org/10.1136/bjo.2009.167494 (2011).
Ng, M. et al. Comparison of visual field severity classification systems for glaucoma. J Glaucoma 21, 551–561, https://doi.org/10.1097/IJG.0b013e31821dac66 (2012).
Barsky, A. J., Peekna, H. M. & Borus, J. F. Somatic symptom reporting in women and men. J Gen Intern Med 16, 266–275 (2001).
Verbrugge, L. M. Sex differences in complaints and diagnoses. J Behav Med 3, 327–355 (1980).
Turner, R. J. & Noh, S. Physical disability and depression: a longitudinal analysis. J Health Soc Behav 29, 23–37 (1988).
Murphy, J. M. Trends in depression and anxiety: men and women. Acta Psychiatr Scand 73, 113–127 (1986).
Weissman, M. M. & Klerman, G. L. Sex differences and the epidemiology of depression. Arch Gen Psychiatry 34, 98–111 (1977).
Linzer, M. et al. Gender, quality of life, and mental disorders in primary care: results from the PRIME-MD 1000 study. Am J Med 101, 526–533 (1996).
van Landingham, S. W. et al. Driving patterns in older adults with glaucoma. BMC Ophthalmol 13, 4, https://doi.org/10.1186/1471-2415-13-4 (2013).
Pollock, S. E. Adaptation to chronic illness: a program of research for testing nursing theory. Nurs Sci Q 6, 86–92, https://doi.org/10.1177/089431849300600208 (1993).
Roy, C. An explication of the philosophical assumptions of the Roy adaptation model. Nurs Sci Q 1, 26–34, https://doi.org/10.1177/089431848800100108 (1988).
Heijmans, M. et al. The stress of being chronically ill: from disease-specific to task-specific aspects. J Behav Med 27, 255–271 (2004).
Moss-Morris, R. Adjusting to chronic illness: time for a unified theory. Br J Health Psychol 18, 681–686, https://doi.org/10.1111/bjhp.12072 (2013).
Devins, G. M. Illness intrusiveness and the psychosocial impact of lifestyle disruptions in chronic life-threatening disease. Adv Ren Replace Ther 1, 251–263 (1994).
Crewe, N. M. Quality of life–the ultimate goal in rehabilitation. Minn Med 63, 586–589 (1980).
Livneh, H. & Antonak, R. Psychosocial adaptation to chronic illness and disability. (Aspen Publishers, 1997).
Janz, N. K. et al. Fear of blindness in the Collaborative Initial Glaucoma Treatment Study: patterns and correlates over time. Ophthalmology 114, 2213–2220, https://doi.org/10.1016/j.ophtha.2007.02.014 (2007).
Izci, F. et al. Impact of Personality Traits, Anxiety, Depression and Hopelessness Levels on Quality of Life in the Patients with Breast Cancer. Eur J Breast Health 14, 105–111, https://doi.org/10.5152/ejbh.2018.3724 (2018).
Turner, J. & Kelly, B. Emotional dimensions of chronic disease. West J Med 172, 124–128 (2000).
Nordmann, J. P., Auzanneau, N., Ricard, S. & Berdeaux, G. Vision related quality of life and topical glaucoma treatment side effects. Health Qual Life Outcomes 1, 75, https://doi.org/10.1186/1477-7525-1-75 (2003).
Jampel, H. D. et al. Patient preferences for eye drop characteristics: a willingness-to-pay analysis. Arch Ophthalmol 121, 540–546, https://doi.org/10.1001/archopht.121.4.540 (2003).
Asaoka, R. et al. Patients have two eyes!: binocular versus better eye visual field indices. Invest Ophthalmol Vis Sci 52, 7007–7011, https://doi.org/10.1167/iovs.11-7643 (2011).
Acknowledgements
Associazione Italiana Studio del Glaucoma (AISG) supported this study with an unrestricted grant. The contribution of the Fondazione Bietti in this study was supported by Ministry of Health and Fondazione Roma.
Author information
Authors and Affiliations
Author notes
A comprehensive list of consortium members appears at the end of the paper
Consortia
Contributions
I.R., L.L., E.R., A.G.K., A.K., F.O., R.N.W. and L.Q. participated in the design of the study and in the preparation of the paper. All the members of the Italian Study Group on Quality of Life were involved in the research, and are to be considered co-authors.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Riva, I., Legramandi, L., Rulli, E. et al. Vision-related quality of life and symptom perception change over time in newly-diagnosed primary open angle glaucoma patients. Sci Rep 9, 6735 (2019). https://doi.org/10.1038/s41598-019-43203-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-43203-9
- Springer Nature Limited
This article is cited by
-
The effects of age-related macular degeneration on quality of life in a Brazilian population
International Journal of Retina and Vitreous (2021)
-
Comparison of visual performance between monofocal and multifocal intraocular lenses of the same material and basic design
Scientific Reports (2020)