
Abstract
Epidermal growth factor receptor (EGFR) and its ligands are involved in cancer pathogenesis. The emerging role of treatments co-targeting the EGFR system in breast cancer has increased the need to identify companion biomarkers. The aim of this study is to investigate whether pretreatment serum levels of EGFR and EGFR ligands in early-stage breast cancer patients might provide prognostic information as a stepping stone for further investigation. The study, which included 311 early-stage breast cancer patients, investigated associations between preoperative serum levels of EGFR and EGFR ligands (epidermal growth factor, heparin-binding epidermal growth factor (HBEGF), amphiregulin, transforming growth factor-α and betacellulin) and survival. Cutoffs were determined using Youden’s method, and overall survival (OS) and invasive disease-free survival (IDFS) were evaluated using Cox regression. Preoperative S-EGFR < 60.3 ng/mL was associated with shorter OS and IDFS in both univariate analyses and when adjusting for standard prognostic factors (p < 0.05). Preoperative S-HBEGF < 21.4 pg/mL was associated with shorter OS in both univariate and multivariate analyses, whereas association with shorter IDFS could only be demonstrated in the univariate analysis. In conclusion, our study demonstrated shorter survival in early-stage breast cancer patients who had low pretreatment levels of either S-EGFR or S-HBEGF.
Similar content being viewed by others
Introduction
The family of epidermal growth factor receptors, which consists of four related transmembrane receptors (EGFR, HER2, HER3 and HER4), is involved in cancer pathogenesis1. EGFR is activated upon by ligand binding, resulting in the activation of a complex intracellular pathway1. Among the ligands that activate EGFR are epidermal growth factor (EGF), heparin-binding epidermal growth factor (HBEGF), amphiregulin (AREG), transforming growth factor α (TGF-α) and betacellulin (BTC)1. EGFR-targeted therapies have well-established roles in the treatment of subgroups of lung cancer patients and colorectal cancer patients2,3. In breast cancer, however, most studies conducted so far could not identify benefits from applying EGFR targeted treatments and one of the hypotheses explaining the disappointing results is the heterogeneous nature of breast cancer and lack of valid predictive biomarkers to enable selection of patients who are most likely to respond to treatment4,5,6. Whereas the potential role of EGFR-targeted treatments in breast cancer is still undetermined, treatments targeting HER2 have radically improved outcomes for breast cancer patients with tumors overexpressing HER27,8. Furthermore, recently, dual and pan-targeted EGFR inhibitors have also been implemented to treat breast cancer patients9,10,11. As more EGFR-targeted treatments are developed, there is an increasing need to identify companion biomarkers to predict treatment response and monitor treatment effect to improve patient outcomes. In colorectal and lung cancer, research indicates that blood levels of EGFR and EGFR ligands might serve as companion biomarkers for EGFR-targeted treatments12,13,14,15.
We conducted a systematic review to investigate whether EGFR and EGFR ligands might serve as prognostic or predictive blood-based biomarkers in breast cancer16. Several studies have investigated S-EGFR in the metastatic breast cancer setting, three of which report associations between low S-EGFR and shorter survival and reduced response to certain treatments17,18,19. EGFR ligands have been investigated to a much lesser extent, and several ligands have not been investigated at all16. In the systematic review, we identified only a single study that evaluated the prognostic value of S-EGFR in early-stage breast cancer patients, which included only 119 patients20, and we found no studies that evaluated the prognostic or predictive value of any of the EGFR ligands in early-stage breast cancer patients16. We recently repeated the literature search performed in 2017 when conducting our systematic review16 and found no additional studies in early-stage breast cancer patients. Thus, the prognostic and predictive significance of EGFR and EGFR ligands as blood-based biomarkers in early-stage breast cancer remains undetermined.
The primary aim of the present study was to investigate whether preoperative serum levels of EGFR and EGFR ligands were associated with overall survival and invasive disease-free survival in early-stage breast cancer patients.
Methods
Study design and patients
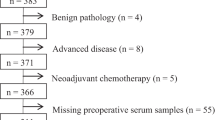
From 2004 to 2013, 383 newly diagnosed breast cancer patients gave written informed consent to participate in a prospective biomarker study at Lillebaelt Hospital, Vejle, Denmark. In the present study we conducted additional retrospective analyses of serum levels of EGFR and EGFR ligands. The inclusion criterion for the present study was primary diagnosed early-stage breast cancer, which could be surgically removed. Exclusion criteria included ducal carcinoma in situ (n = 4), primary advanced disease (n = 8) and neoadjuvant treatment (n = 5) (Table 1). Furthermore, patients with no available preoperative serum sample (n = 55) were excluded, leaving a total of 311 early-stage breast cancer patients to be included in the study (Table 1).
Patients underwent primary breast cancer surgery according to the guidelines of the Danish Breast Cancer Cooperative Group (DBCG) and subsequently received adjuvant treatment according to existing guidelines.
Histopathological data were obtained from the local pathology database at Lillebaelt Hospital, Denmark. Clinical information was obtained from local electronic medical records at Lillebaelt Hospital, Denmark. The study period ended on April 24, 2019.
The study was approved by the Regional Committees on Health Research Ethics for Southern Denmark (S-20170119) and the Danish Data Protection Agency (journal number 8/56003) and was conducted in accordance with the Helsinki Declaration.
The study adheres to the Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK)21.
Samples
Baseline and follow-up blood samples were collected using standard venipuncture procedure performed by skilled phlebotomists, centrifuged, aliquoted and stored at − 80 °C in a biobank at Lillebaelt Hospital, Vejle, Denmark.
Baseline serum samples were obtained 1–42 days (mean 7 days) prior to primary surgery for breast cancer. A postoperative sample was obtained between 14 and 30 days after primary surgery. Serum samples were subsequently obtained at standard clinical control visits. In the present study we included follow-up samples from patients who experienced metastatic recurrence. These samples were obtained within three months prior to a diagnosis of a systemic recurrence of breast cancer.
Assays
Serum levels of EGFR (S-EGFR) and EGF (S-EGF) were measured using sandwich enzyme-linked immunosorbent assay (ELISA) testing. HBEGF (S-HBEGF), AREG (S-AREG), TGF-α (S-TGFα) and BTC (S-BTC) were analyzed using ultra-sensitive Single Molecule Array (Simoa) technology22. S-AREG, S-TGFα and S-BTC were analyzed using a three-plex assay23. All assays used in the present study have previously been described in detail23,24. During analysis, the serum samples from the individual patients were analyzed in the same run. Each run included at least three assay controls. The total coefficients of variation (CV%) were: S-EGFR 8–17%, S-EGF 8–12%, S-HBEGF 15–29%, S-AREG 12–21%, S-TGFα 8–14% and S-BTC 11–25%. The limits of detection were: S-EGFR 0.014 ng/mL, S-EGF 0.03 pg/mL, S-HBEGF 0.05 pg/mL, S-AREG 0.16 pg/mL, S-TGFα 0.2 pg/mL and S-BTC 0.2 pg/mL.
The estrogen receptor (ER) status and progesterone receptor (PR) status of the breast cancer tumor was determined using immunohistochemical staining (IHC) and, according to contemporary guidelines, the tumor was considered positive if ≥ 10% of nuclei were stained. The HER2 status of the tumor was determined using IHC and fluorescence in situ hybridization (FISH). The tumor was considered HER2-positive in cases with IHC3 + or IHC 2 + and FISH > 2, whereas the tumor was considered HER2-negative in cases with IHC 0, IHC 1 + , or IHC 2 + and FISH < 2.The ER and HER2 assays have been described in a previous study by Kjær et al25.
The laboratory technicians performing analysis of the serum samples were blinded for all clinical information including outcome for the patients.
Clinical end points
Outcome measures were defined according to the Proposal for Standardized Definitions for Efficacy End Points in Adjuvant Breast Cancer Trials: The STEEP system26. Invasive Disease-Free Survival (IDFS) was defined as the time from primary breast cancer surgery until the occurrence of one of the following events: invasive ipsilateral breast tumor recurrence; local/regional invasive recurrence; distant recurrence; invasive contralateral breast cancer; second primary invasive non-breast cancer (with the exception of squamous or basal cell skin cancers) or death by any cause. All in-situ cancer events, from both breast and non-breast sites, are excluded from the IDFS definition26. Overall Survival (OS) was defined as the time from primary breast cancer surgery to death, including death from breast cancer, any other cause or unknown cause26.
Statistical methods
As the prognostic value of EGFR and EGFR ligands in breast cancer is investigated to a very limited extend16, the present study was conducted with an explorative approach and no specified effect size was expected.
First, an optimal cutoff for each biomarker was estimated using Youden’s method with logistic regressions27. The logistic regressions were conducted with 5-year overall survival as a dependent variable and baseline biomarker level as an independent variable. In the S-AREG, S-TGFα and S-BTC variables, but not in the S-EGFR, S-EGF and S-HBEGF variables, outliers were identified in the baseline samples of seven patients and removed. These outliers could be due to heterophilic antibodies, rheumatoid factors or non-specific binding that caused interference specifically in the three-plex Simoa assay. The distributions of data for S-AREG, S-TGFα and S-BTC showed highly skewed distributions; hence, logistic regressions were conducted using log-transformed independent variables. The cutoff for S-AREG, S-TGFα and S-BTC were then back-transformed to the original scale.
Second, univariate Cox regressions were performed for all biomarkers using Youden cutoffs, and for the standard prognostic covariates including age, type of surgery, pathology and adjuvant treatment. The two endpoints, OS and IDFS, were evaluated. We created Kaplan Meier curves depicting OS in the groups delineated by Youden cutoffs for S-EGFR and S-HBEGF. Multivariate Cox regressions were performed for each of the biomarkers using Youden cutoffs. The models were adjusted for all standard prognostic covariates. The two endpoints, OS and IDFS, were evaluated. The assumption of proportional hazards was investigated using Schoenfeld residuals.
Third, Cox regressions for OS and IDFS were performed for all six biomarkers in the subgroups defined as hormone receptor positive patients (ER-positive and/or PR-positive), HER2-positive patients and triple negative patients (hormone receptor negative and HER2-negative).
Stata IC 16.1 software package (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC) was used for the statistical analysis.
Results
Patient characteristics
A total of 311 women with early-stage breast cancer were included in the study. The clinical-pathological characteristics, including standard prognostic parameters, are presented in Table 2. The population of women with early-stage breast cancer included in the present study has previously been described in a study by Kjær et al25. As reported, the clinical-pathological characteristics of the study population are considered to be representative of patients with early-stage breast cancer25. The adjuvant therapy is presented in Table 2. A total of 269 patients (86.5%) received adjuvant radiotherapy, 146 patients (46.9%) received adjuvant chemotherapy, 220 patients (70.7%) received endocrine treatment and 38 patients (12.2%) received HER2-targeted treatment. Median and interquartile range of the preoperative serum levels of EGFR and EGFR ligands are presented in Table 2. Furthermore, the optimal cutoff for each biomarker, estimated using Youden’s method, is presented, including the number of patients with levels above and below these cutoffs.
Overall survival
The median follow-up time for OS was 11.0 years, and a total of 78 of the 311 patients included in the study died at some point during the study period. The five-year OS rate was 90%.
S-EGFR: Univariate Cox regression showed that baseline S-EGFR below 60.3 ng/mL (Youden-estimated cutoff) was associated with shorter OS (p = 0.002) (Table 3). Kaplan–Meier curves are presented in Fig. 1. Moreover, in multivariate Cox regression (adjusted for all covariates), baseline S-EGFR < 60.3 ng/mL was associated with shorter survival (p = 0.01). Cox analyses were conducted in subgroups defined as hormone receptor positive patients, HER2-positive patients and triple negative patients (Table 4a). Hormone receptor positive patients with S-EGFR < 60.3 ng/mL showed a significantly shorter OS (p = 0.01) than patients with S-EGFR ≥ 60.3 ng/mL. However, when adjusting for HER2 status, the association did not reach statistical significance (p = 0.06). HER2-positive patients with S-EGFR < 60.3 ng/mL showed a significantly shorter OS (p = 0.002) in both univariate analysis and when adjusting for hormone receptor status (p = 0.007). In the triple negative subgroup, no association between OS and S-EGFR was observed.

Kaplan–Meier curves showing overall survival in 311 early-stage breast cancer patients. Patients were divided into groups based on preoperative level of S-EGFR (a) or S-HBEGF (b). Cutoffs were determined using Youden’s method for estimation of optimal cutoff. P-values were determined using Cox-regressions.
S-HBEGF: Baseline S-HBEGF < 21.4 pg/mL was associated with shorter OS in univariate Cox regression (p = 0.003), and this association persisted after adjusting for all covariates (p = 0.01). Kaplan–Meier curves are presented in Fig. 1. Hormone receptor positive patients with S-HBEGF < 21.4 pg/mL were found to have a significantly shorter OS both when performing univariate analysis (p = 0.02) and when adjusting for HER2 status (p = 0.01). No associations were found in the subgroup of HER2-positive patients or triple negative patients (Table 4a).
S-EGF, S-BTC, S-AREG and S-TGFα: No associations between preoperative serum levels of these biomarkers and OS were found in either univariate or multivariate Cox regression in the entire study population (Table 3). In the hormone receptor positive subgroup S-EGF < 296 pg/mL was associated with shorter OS both in univariate analysis (p = 0.02) and when adjusting for HER2 status (p = 0.04). In the HER2-positive subgroup S-AREG ≥ 5.3 pg/mL was associated with a significantly shorter OS both in univariate analysis (p = 0.02) and when adjusting for hormone receptor status (p = 0.001) (Table 4a).
Invasive disease-free survival
The median follow-up time for IDFS was 10.6 years. During the follow-up period, 108 patients had one or more IFDS events (69 patients had recurrence of breast cancer as a first event, 19 patients had a second primary non-breast cancer as a first event and for 20 patients death was the first event). Five-year IDFS rate for the study population was 82%.
S-EGFR: Univariate Cox regression showed that baseline S-EGFR < 60.3 ng/mL was associated with shorter IDFS (p = 0.004) (Table 3). This association remained significant after applying a multivariate Cox regression (adjusted for all covariates) (p = 0.015). Hormone receptor positive patients with S-EGFR < 60.3 ng/mL showed a significantly shorter IDFS (p = 0.02) than patients with S-EGFR ≥ 60.3 ng/mL; however, when adjusting for HER2 status, the association did not reach statistical significance (p = 0.06). HER2-positive patients with S-EGFR < 60.3 ng/mL showed a significantly shorter IDFS (p = 0.02) in univariate analysis, but not when adjusting for hormone receptor status (p = 0.06). (Table 4b).
S-HBEGF: Baseline S-HBEGF < 21.4 pg/mL was associated with shorter IDFS in univariate Cox regression (p = 0.008) (Table 3). However, when adjusting for all covariates the association did not reach statistical significance (p = 0.05). Hormone receptor positive patients with S-HBEGF < 21.4 pg/mL were found to have significantly shorter IDFS both when performing univariate analysis (p = 0.02) and when adjusting for HER2 status (p = 0.01). No associations were found in the subgroup of HER2-positive patients (Table 4b).
S-EGF, S-BTC, S-AREG and S-TGFα: No associations between preoperative serum levels of these biomarkers and IDFS were found in either univariate or multivariate Cox regression in the entire study population (Table 3). In the HER2-positive subgroup S-AREG ≥ 5.3 pg/mL was associated with a significantly shorter IDFS both in univariate analysis (p = 0.046) and when adjusting for hormone receptor status (p = 0.008) (Table 4b).
Pre- to postoperative changes of EGFR and EGFR ligands in serum
To evaluate whether pre- to postoperative changes in serum levels of EGFR and EGFR ligands might provide prognostic information in early-stage breast cancer patients, we conducted plots depicting the pre- to postoperative changes of each biomarker for the individual patients. The postoperative serum sample was obtained 14–30 days after primary breast cancer surgery and was available from 113 patients. Spaghetti plots depicting pre- to postoperative changes in patients alive and dead after five years showed no tendencies in the pre- to postoperative changes of any of the biomarkers and no relation to 5-year overall survival (Online Appendix 1). Moreover, waterfall plots illustrating pre- to postoperative delta-values showed no tendencies towards associations with 5-year overall survival (Online Appendix 2).
Changes in serum levels of EGFR and EGFR ligands before systemic recurrence of breast cancer
To evaluate the potential of EGFR and EGFR ligands as predictive biomarkers in relation to earlier detection of metastatic recurrence of breast cancer, we conducted plots depicting the changes in serum levels of each biomarker before systemic recurrence of breast cancer. The recurrence serum sample was obtained within three months before systemic recurrence of breast cancer and was available from 14 individual patients. For each biomarker the preoperative level, postoperative level and level at time of systemic recurrence of breast cancer were depicted for these 14 patients (Online Appendix 3). The changes in biomarker levels during the course of disease varied between the individual patients and showed no distinct patterns, nor were distinct changes at time of recurrence observed.
Discussion
The present study investigated the prognostic value of EGFR and EGFR ligands in the serum of 311 patients with early-stage breast cancer and demonstrated significantly shorter survival in patients with low pretreatment levels of either S-EGFR or S-HBEGF.
S-EGFR below the defined cut-off at 60.3 ng/mL was associated with shorter OS and IDFS in both univariate and multivariate analysis in the entire population. Subgroup analysis showed, that in the hormone receptor positive subgroup, patients with S-EGFR < 60.3 ng/mL had shorter OS and IDFS; however, when adjusting for HER2 status, the associations did not reach statistical significance. Similar analysis in the HER2-positive subgroup also showed shorter OS and IFDS in patients with low S-EGFR and here the association remained significant for OS after adjustment for hormone receptor status. Only one study has previously investigated the prognostic value of S-EGFR in early-stage breast cancer patients and found no association between preoperative S-EGFR and disease-free survival; however, the study included only 119 patients20. Furthermore, no subgroup analysis was conducted in the study20. Several studies have investigated the prognostic significance of S-EGFR in metastatic breast cancer patients16,28. Overall, the results of these studies indicate associations between low levels of S-EGFR and shorter survival17,18,19,28. Though some studies found no significant associations, no studies reported opposing results16. Few of the studies have investigated the prognostic significance of S-EGFR in subgroups: In relation to the hormone receptor positive subgroup two studies reported shorter survival in patients with low baseline S-EGFR17,19, which is in accordance to the findings of the present study. One other study found no correlation29. In relation to the HER2-positive subgroup, two previous studies found no association between S-EGFR and survival10,30. In conclusion, the results of the present study indicate shorter survival in patients with low S-EGFR not only in metastatic breast cancer as shown in previous studies, but also in early-stage breast cancer. Several potential mechanisms explaining the associations between low S-EGFR and shorter survival have been proposed and were discussed thoroughly in a study by Banys–Paluchowski28. However, current evidence is inconclusive, and further investigations into these mechanisms are recommended.
Preoperative S-HBEGF < 21.4 pg/mL was associated with shorter OS in both univariate and multivariate Cox regression, whereas association with shorter IDFS could only be demonstrated in the univariate analysis. No associations with OS or IFDS were found in the subgroup of HER2-positive patients, whereas hormone receptor positive patients with S-HBEGF < 21.4 pg/mL were found to have significantly shorter OS and IDFS in both univariate data analysis and when adjusting for HER2 status. No previous studies have investigated the prognostic value of S-HBEGF in breast cancer.
Regarding the remaining EGFR-ligands, we found no associations between preoperative level of either S-EGF, S-BTC, S-AREG or S-TGFα and OS or IDFS in the entire study population. However, when performing subgroup analysis, results showed that S-AREG ≥ 5.3 pg/mL was associated with shorter OS and IDFS in HER2-positive patients, both in univariate analysis and after adjusting for hormone receptor status. In addition, in the subgroup of hormone receptor positive patients S-EGF < 296 pg/ml was associated to shorter OS in both univariate analysis and when adjusting for HER2 status. Previous research investigating EGFR ligands in breast cancer are sparse and included solely HER2-positive patients16,31. Only S-EGF, S-TGFα and S-AREG have previously been investigated, whereas no investigation of S-BTC or S-HBEGF have been performed, to our best knowledge16. Furthermore, the study populations included advanced breast cancer patients and evaluated mainly the biomarkers in relation to treatment response16,31. Thus, to our best knowledge, this study is the first to evaluate the prognostic value of serum levels of EGFR ligands in early-stage breast cancer patients and across subgroups.
Pre-to postoperative changes in EGFR or EGFR ligand levels in serum showed no tendencies towards associations with 5-year overall survival (Online Appendices 1 and 2). Moreover, changes in EGFR and EGFR ligands during the course of disease varied between the individual patients and showed no distinct patterns or distinct changes at the time of systemic recurrence (Online Appendix 3). However, due to the low number of patients in these additional investigations, these findings should be interpreted with caution.
The present study has some limitations. First, breast cancer is known to be a heterogeneous disease with regard to hormone receptor status and HER2 status. In the present study distinct subgroups as defined by hormone receptor positive patients, HER2-positive patients and triple negative patients were too small to apply a complete multivariate analysis and the results of these subgroup analyses should be interpreted with utmost caution, in particular the triple negative subgroup. Thus, further studies investigating EGFR and EGFR ligands in large distinct subgroups of breast cancer patients are recommended. Second, because EGFR and EGFR ligands have been investigated as serological biomarkers to such a limited extent, reference methods and reference materials are unavailable. Whereas S-EGFR and S-EGF could be quantified using ELISA-testing, we developed highly sensitive immunoassays for S-HBEGF, S-AREG, S-TGFα and S-BTC on the Simoa platform23,24. CV%s of the assays were 8–29%, which shows the need to improve the analytical performance of the assays. However, in the clinically relevant levels of S-EGFR and S-HBEGF, the CV%s were 11% and 15%, respectively, which is comparable to commonly used biomarker assays. Furthermore, standardized cut-offs for EGFR and EGFR ligands have not yet been established, so in the current study we estimated cutoffs using Youden’s method for optimal cutoffs. Finally, the 5-year OS for the entire study population of early-stage breast cancer patients was 90%, whereas the 5-year OS for early-stage breast cancer patients in Denmark in a national database was 77% in the period 2005–200932. Thus, 5-year OS rate is higher in the present study population as compared to the national population of early-stage breast cancer patients. However, when considering specific age-groups, the 5-year OS are overall comparable between age-groups and the difference in 5-year OS might, thus, reflect differences in age distribution between the present study population and the nationwide study population25,32. For instance, in the age-category 65–74 years the 5-year OS is 80% in both the study population and nationwide population32.
The study was conducted in accordance with REMARK21 and used outcome measures as recommended in the Proposal for Standardized Definitions for Efficacy End Points in Adjuvant Breast Cancer Trials: The STEEP system26, thus enabling researchers to assess and compare results in future studies.
In conclusion, the present study demonstrated significantly shorter survival in early-stage breast cancer patients with low pretreatment levels of either S-EGFR (< 60.3 ng/mL) or S-HBEGF (< 21.4 pg/mL). Thus, the findings indicate shorter survival in patients with low S-EGFR not only in metastatic breast cancer, as shown in previous studies, but also in early-stage breast cancer. The prognostic value of S-HBEGF in breast cancer patients has not previously been investigated. The findings indicate that in subgroups of breast cancer patients, the EGFR-pathway is more involved in the malignant potential than in others. The current study results need validation in well-defined independent study populations including subgroup populations defined as hormone receptor positive patients, HER2-positive patients and triple negative patients. Furthermore, it would be of interest to investigate predictive value of these biomarkers in populations that include breast cancer patients receiving EGFR-co-targeted treatments. Overall, the results of this study indicate a prognostic value of S-EGFR and S-HBEGF in early-stage breast cancer and could be a stepping stone for further investigation of S-EGFR and S-HBEGF as prognostic biomarkers in breast cancer. Furthermore, it would be of interest to investigate the predictive value of EGFR and EGFR ligands, which is undetermined in breast cancer.
Data availability
The dataset contains person-sensitive data that were used under license for the study. Thus, the data are not publicly available. Upon reasonable request and with permission from the relevant legal authorities under existing laws, the data may be made available by the authors.
References
Yarden, Y. & Sliwkowski, M. X. Untangling the ErbB signalling network. Nat. Rev. Mol. Cell. Biol. 2, 127–137. https://doi.org/10.1038/35052073 (2001).
Rosell, R. et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 13, 239–246. https://doi.org/10.1016/S1470-2045(11)70393-X (2012).
Van Cutsem, E. et al. Fluorouracil, leucovorin, and irinotecan plus cetuximab treatment and RAS mutations in colorectal cancer. J. Clin. Oncol. 33, 692–700. https://doi.org/10.1200/JCO.2014.59.4812 (2015).
Gonzalez-Conchas, G. A. et al. Epidermal growth factor receptor overexpression and outcomes in early breast cancer: a systematic review and a meta-analysis. Cancer Treat Rev. 62, 1–8. https://doi.org/10.1016/j.ctrv.2017.10.008 (2018).
Masuda, H. et al. Role of epidermal growth factor receptor in breast cancer. Breast Cancer Res. Treat. 136, 331–345. https://doi.org/10.1007/s10549-012-2289-9 (2012).
Baselga, J. et al. Randomized phase II study of the anti-epidermal growth factor receptor monoclonal antibody cetuximab with cisplatin versus cisplatin alone in patients with metastatic triple-negative breast cancer. J. Clin. Oncol. 31, 2586–2592. https://doi.org/10.1200/JCO.2012.46.2408 (2013).
Slamon, D. et al. Adjuvant trastuzumab in HER2-positive breast cancer. N. Engl. J. Med. 365, 1273–1283. https://doi.org/10.1056/NEJMoa0910383 (2011).
Slamon, D. J. et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N. Engl. J. Med. 344, 783–792. https://doi.org/10.1056/NEJM200103153441101 (2001).
Chan, A. et al. Neratinib after trastuzumab-based adjuvant therapy in patients with HER2-positive breast cancer (ExteNET): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 17, 367–377. https://doi.org/10.1016/S1470-2045(15)00551-3 (2016).
Cameron, D. et al. A phase III randomized comparison of lapatinib plus capecitabine versus capecitabine alone in women with advanced breast cancer that has progressed on trastuzumab: updated efficacy and biomarker analyses. Breast Cancer Res. Treat. 112, 533–543. https://doi.org/10.1007/s10549-007-9885-0 (2008).
Swain, S. M. et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N. Engl. J. Med. 372, 724–734. https://doi.org/10.1056/NEJMoa1413513 (2015).
Haghgoo, S. M. et al. Prognostic value of rare and complex mutations in EGFR and serum levels of soluble EGFR and its ligands in non-small cell lung carcinoma patients. Clin. Biochem. 50, 293–300. https://doi.org/10.1016/j.clinbiochem.2016.11.033 (2017).
Ishikawa, N. et al. Increases of amphiregulin and transforming growth factor-alpha in serum as predictors of poor response to gefitinib among patients with advanced non-small cell lung cancers. Cancer Res. 65, 9176–9184. https://doi.org/10.1158/0008-5472.CAN-05-1556 (2005).
Gregorc, V. et al. Effects of gefitinib on serum epidermal growth factor receptor and HER2 in patients with advanced non-small cell lung cancer. Clin. Cancer Res. 10, 6006–6012. https://doi.org/10.1158/1078-0432.CCR-03-0770 (2004).
Ma, B. B. et al. Intermittent versus continuous erlotinib with concomitant modified “XELOX” (q3W) in first-line treatment of metastatic colorectal cancer: correlation with serum amphiregulin and transforming growth factor alpha. Cancer 119, 4145–4153. https://doi.org/10.1002/cncr.28327 (2013).
Kjaer, I. M., Bechmann, T., Brandslund, I. & Madsen, J. S. Prognostic and predictive value of EGFR and EGFR-ligands in blood of breast cancer patients: a systematic review. Clin. Chem. Lab. Med. 56, 688–701. https://doi.org/10.1515/cclm-2017-0592 (2018).
Muller, V. et al. Prognostic and predictive impact of soluble epidermal growth factor receptor (sEGFR) protein in the serum of patients treated with chemotherapy for metastatic breast cancer. Anticancer Res. 26, 1479–1487 (2006).
Sandri, M. T. et al. Serum EGFR and serum HER-2/neu are useful predictive and prognostic markers in metastatic breast cancer patients treated with metronomic chemotherapy. Cancer 110, 509–517. https://doi.org/10.1002/cncr.22825 (2007).
Souder, C. et al. Serum epidermal growth factor receptor/HER-2 predicts poor survival in patients with metastatic breast cancer. Cancer 107, 2337–2345. https://doi.org/10.1002/cncr.22255 (2006).
Rocca, A. et al. Perioperative serum VEGF and extracellular domains of EGFR and HER2 in early breast cancer. Anticancer Res. 29, 5111–5119 (2009).
Sauerbrei, W., Taube, S. E., McShane, L. M., Cavenagh, M. M. & Altman, D. G. Reporting recommendations for tumor marker prognostic studies (REMARK): an abridged explanation and elaboration. J. Natl. Cancer Inst. 110, 803–811. https://doi.org/10.1093/jnci/djy088 (2018).
Rissin, D. M. et al. Single-molecule enzyme-linked immunosorbent assay detects serum proteins at subfemtomolar concentrations. Nat. Biotechnol. 28, 595–599. https://doi.org/10.1038/nbt.1641 (2010).
Olsen, D. A., Kjaer, I. M. & Brandslund, I. Development of a three-plex single molecule immunoassay enabling measurement of the EGFR ligands amphiregulin, betacellulin and transforming growth factor alpha simultaneously in human serum samples. J. Immunol. Methods 459, 63–69. https://doi.org/10.1016/j.jim.2018.05.002 (2018).
Kjaer, I. M. et al. EGFR and EGFR ligands in serum in healthy women; reference intervals and age dependency. Clin. Chem. Lab. Med. https://doi.org/10.1515/cclm-2019-0376 (2019).
Kjaer, I. M. et al. Dysregulated EGFR pathway in serum in early-stage breast cancer patients: a case control study. Sci. Rep. 10, 6714. https://doi.org/10.1038/s41598-020-63375-z (2020).
Hudis, C. A. et al. Proposal for standardized definitions for efficacy end points in adjuvant breast cancer trials: the STEEP system. J. Clin. Oncol. 25, 2127–2132. https://doi.org/10.1200/JCO.2006.10.3523 (2007).
Fluss, R., Faraggi, D. & Reiser, B. Estimation of the Youden Index and its associated cutoff point. Biom. J. 47, 458–472. https://doi.org/10.1002/bimj.200410135 (2005).
Banys-Paluchowski, M. et al. Evaluation of serum epidermal growth factor receptor (EGFR) in correlation to circulating tumor cells in patients with metastatic breast cancer. Sci. Rep. 7, 17307. https://doi.org/10.1038/s41598-017-17514-8 (2017).
Lafky, J. M. et al. Serum soluble epidermal growth factor receptor concentrations decrease in postmenopausal metastatic breast cancer patients treated with letrozole. Cancer Res. 65, 3059–3062. https://doi.org/10.1158/0008-5472.can-05-0067 (2005).
Hudelist, G. et al. Serum EGFR levels and efficacy of trastuzumab-based therapy in patients with metastatic breast cancer. Eur. J. Cancer (Oxford Engl. 1990) 42, 186–192. https://doi.org/10.1016/j.ejca.2005.08.036 (2006).
Bianchini, G. et al. Biomarker analysis of the NeoSphere study: pertuzumab, trastuzumab, and docetaxel versus trastuzumab plus docetaxel, pertuzumab plus trastuzumab, or pertuzumab plus docetaxel for the neoadjuvant treatment of HER2-positive breast cancer. Breast Cancer Res. 19, 16. https://doi.org/10.1186/s13058-017-0806-9 (2017).
Jensen, M. B., Ejlertsen, B., Mouridsen, H. T., Christiansen, P. & Danish Breast Cancer Cooperative, G. Improvements in breast cancer survival between 1995 and 2012 in Denmark: the importance of earlier diagnosis and adjuvant treatment. Acta Oncol. 55(Suppl 2), 24–35. https://doi.org/10.3109/0284186X.2015.1128119 (2016).
Creative Commons Attribution 4.0 International License. https://creativecommons.org/licenses/by/4.0/
Acknowledgements
Camilla Davidsen and Sara Egsgaard are acknowledged for analyzing the serum samples and Jannie Møller for assisting in the composition of the database. The authors thank Mads Nikolaj Olesen and Sören Möller for statistical advice and Jude Pedersen for language proofreading. Open Patient data Explorative Network (OPEN) are acknowledged for the collaboration on data management.
Funding
The Research Committee, Lillebaelt Hospital, Vejle, Denmark; The Region of Southern Denmark; The University of Southern Denmark; Danmarks Sundhedsfond; Overlæge Alfred Skov Jensen og hustrus Fond, and Fabrikant Einer Willumsens Mindelegat funded the study.
Author information
Authors and Affiliations
Contributions
The study was designed by I.M.K., J.S.M., I.B., T.B. and D.A.O. and I.M.K., T.B., E.H.J. and D.A.O. collected data. I.M.K. and S.B.B. performed the statistical analysis. IMK wrote the manuscript and it was reviewed by all authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kjær, I.M., Olsen, D.A., Brandslund, I. et al. Prognostic impact of serum levels of EGFR and EGFR ligands in early-stage breast cancer. Sci Rep 10, 16558 (2020). https://doi.org/10.1038/s41598-020-72944-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-72944-1
- Springer Nature Limited
This article is cited by
-
The Multiple Functions of HB-EGF in Female Reproduction and Related Cancer: Molecular Mechanisms and Targeting Strategies
Reproductive Sciences (2024)
-
Consultation on UTUC II Stockholm 2022: diagnostic and prognostic methods—what’s around the corner?
World Journal of Urology (2023)