
Abstract
The resection of nodules by thoracoscopic surgery is difficult because the nodules may be hard to identify. Preoperative localization of pulmonary nodules is widely used in the clinic. In this study, we retrospectively compared CT-guided hook wire localization and electromagnetic navigation bronchoscopy (ENB) localization of small pulmonary nodules before resection. Patients who underwent localization with CT-guided hook wire or ENB followed by video-assisted thoracoscopic surgery (VATS) at Qilu Hospital of Shandong University between January 2016 and December 2019 were retrospectively included. Clinical parameters, complication and failure rate, and localization time were compared between two groups. A total of 157 patients underwent the localization procedure successfully. Pulmonary nodules were localized by CT-guided hook wire in 105 patients and by ENB in 52 patients. The nodule size in ENB group was smaller than that in CT-guided localization group (P < 0.001). Both CT-guided localization and ENB localization were well tolerated in all patients, while ENB localization leaded to less complications (P = 0.0058). In CT-guided localization group, 6 patients failed to be located while none failed in ENB group (P = 0.079). The procedure time was 15.15 ± 3.70 min for CT-guided localization and 21.29 ± 4.00 min for ENB localization (P < 0.001). CT-guided localization is simple and feasible for uncertain pulmonary nodules before surgery. ENB localization could identify small lung nodules with high accuracy and achieve lower incidence of complications.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Lung cancer is the most lethal disease worldwide. It accounts for one-quarter of all cancer deaths around the world. Although the diagnosis and treatment technologies have improved rapidly in recent years, the prognosis of lung cancer remains poor. The 5-year survival rate of lung cancer is only 18%, which is the lowest among all kinds of cancers1. With widespread use of computed tomography (CT) in the clinic, the discovery of small or faint lesions on CT become fesible2. However, the resection of nodules by thoracoscopic surgery is difficult because the nodules may be hard to identify, especially for deep pulmonary small nodules. If the location of nodules cannot be accurately determined during the operation, it will increase the possibility of thoracotomy. Currently, preoperative localization of pulmonary nodules is widely used in the clinic, including CT-guided transthoracic approach, hook-wire and coil embolization. However, these methods increase radiation exposure and cause complications3.
Electromagnetic navigation bronchoscope (ENB) could reach further peripheral lung compared to conventional electronic bronchoscopy4,5. Combined with the path constructed by ENB, we can mark the location of small pulmonary nodules. This method has better safety and effectiveness. Several studies have reported that ENB-guided transbronchial needle biopsy achieves better accuracy and lower complication rates, compared to conventional percutaneous core needle biopsy6,7,8. In this study, we retrospectively compared CT- and ENB-guided localization of small pulmonary nodules before resection.
Methods
We retrospectively analyzed patients who underwent localization with CT or ENB followed by Video-assisted thoracoscopic surgery (VATS) at Qilu Hospital of Shandong University from January 2016 to December 2019. Patients were included based on the following criteria: patients with only one pulmonary nodule smaller than 10 mm, preoperative localization were conducted, undergone VATS after localization and received pathology diagnosis. Clinical parameters were recorded, including the gender, age, smoking status, histology, and stage. CT findings were recorded, including lesion size, location, density, and distance from pleural distance (PD). The nodule size was measured directly on CT images, and the longest diameter was the nodule size. The nodule was classified according to the density as pure nodular ground-glass opacity (GGO), 0–50% GGO and > 50% GGO.
Percutaneous CT-guided localization
CT scan was performed to confirm the presence of nodules before the localization. We used metal markers on the body surface to determine the missing line. Then we used CT and the laser to determine the coronal line. Coronal line represents the CT coronal plane of the lesion, and the intersection of two lines is used to determine the specific location of the nodule (Fig. 1).

(A) Coronal localization by CT and Sagittal marking with steel needles. (B) The picture of steel needle. (C) Measuring the distance of puncture point and locating the distance between steel needle and puncture point in coronal position of CT image. (D) The results of puncture were confirmed by CT and the complications were detected.
ENB planning and surgical procedures
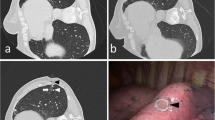
ENB-guided dye-marking was performed for subsolid nodules less than 10 mm near the pleura, or nodules with volume less than 20 mm located more than 10 mm from the pleural surface. The axial, sagittal and coronal views of CT images were used for planning using super Dimension system (Medtronic, Minneapolis, MN, USA). After general anesthesia with intubation, patients were navigated using the 7th edition Super Dimension Navigation System (Covidien, Minneapolis, MN, USA) to localize and plan a route to the nodules one day before the operation. (Fig. 2).

(A) A small pulmonary nodule is located in the right upper lobe. (B) Before operation, magnetic navigation software was used to design magnetic navigation localization path. (C) According to the designed path, the magnetic navigation probe was stained with methylene blue after reaching the lesion location. (D) The accuracy of localization was verified after thoracoscopic surgery.
Thoracoscopic pulmonary surgery was performed immediately after the completion of magnetic navigation surgery. The primary lung cancer and lymph nodes were dissected by VATS. All patients underwent segmental or combined segmental resection, and the pathological examination was performed quickly after operation. All patients received postoperative care. The clinicopathological data, procedure parameters, and complications were evaluated.
This study was approved by the Ethics Committee of Qilu Hospital of Shandong University. The research was performed in accordance with relevant guidelines. Informed consent was obtained from all participants.
Statistical analyses
Measurement data were presented as mean ± standard deviation and analyzed by ANOVA method. Count data were presented as percentage and analyzed by Chi-square test. Statistical analysis was performed using SPSS 23.0 software (SPSS Inc., Chicago, Il, USA). P < 0.05 was regarded as significance.
Results
Characteristics of the patients
We included a total of 157 patients (88 males and 69 females) who underwent the localization procedure successfully. The nodules were localized by CT guidance in 105 patients and by ENB in 52 patients. Among 157 patients, 95 were smokers and 62 were non-smokers. Clinical characteristics of the patients and lung nodules were listed in Table 1. The mean value of nodule size was 6.99 ± 1.37 mm (range 5.0–12.0 mm). The nodule size of ENB localization was smaller than that of CT-guided localization (P < 0.001). The nodule depth in ENB localization group was smaller than CT-guided localization (P = 0.007). Each patient had only one nodule, and the 157 nodules included 74 pure GGO nodules, 66 part solid nodules with GGO < 50%, and 17 part-solid nodules with GGO > 50%. The nodules distributed in each lobe of the lung. Sixteen nodules were in the left upper lobe, 26 nodules were in the left lower lobe, 58 nodules were in the right upper lobe, 17 nodules were in the right middle lobe, and 40 nodules were in the right lower lobe. The pathology diagnoses of 157 nodules were as follows: 29 benign nodules, 76 adenocarcinomas in situ (AIS), 44 minimally invasive adenocarcinomas (MIA) and 8 invasive adenocarcinomas (IA). Standard lobectomy was performed again in 8 IA patients. pTNM stages of 128 malignant tumors were T1aN0M0 (Fig. 3).

Characteristics of pulmonary nodular lesion in two localization groups. (A) Nodule depth. (B) Nodule size. (C) Localization time.
Localization of the nodules
Both CT-guided and ENB localization were well tolerated in all patients, without mortality or major complications, such as tension pneumothorax, massive hemoptysis and active intrathoracic hemorrhage. In CT-guided localization group, the incidence of asymptomatic hemopneumothorax was 7.6% (8/105), symptomatic hemopneumothorax was 3.8% (4/105), hemoptysis was 0.9% (1/105) and decoupling was 0.9% (1/105). ENB localization leaded to less complications (0/52) compared with CT-guided localization (14/105) (P = 0.0058). In addition, in CT-guided localization group, 6 patients failed to be located due to deviation of the puncture hook position, while none failed in ENB group (P = 0.079). The procedure time for CT-guided localization was 15.15 ± 3.70 min (range 10–26 min), while the procedure time for ENB localization was 21.29 ± 4.00 min (range 12–29 min) (P < 0.001). In CT-guided hook wire localization group, 6 hook wires passed through the nodule and 99 hook wires passed beside the nodule. The time of needle-carrying time for patients receiving CT-guided localization was 37.12 ± 17.29 min (P < 0.001) (Table 2, Fig. 3).
Discussion
The application of high resolution CT increases the rate of detecting small pulmonary lesions. Therefore, it is important to accurately locate the sublobar or non-anatomical resection using a variety of approaches9,10,11,12. Currently used localization methods have several advantages and disadvantages. For example, percutaneous hook wire implantation has the advantages of simple operation, accurate localization and less complications, however, it is an invasive operation. ENB, a new technique developed recently, could accurately access peripheral lung lesions beyond the reach of conventional bronchoscopy. ENB-guided localization could reduce complications such as pneumothorax, hemothorax and hemoptysis, compared with traditional localization methods. Therefore, ENB-guided localization is regarded as a promising tool in thoracic surgery13,14. In this study, we compared CT-guided localization and ENB localization for lung nodules in patients.
In our study, 52 patients in ENB localization group had no complications, while 14 in 105 patients with CT-guided puncture hook localization had complications. The most common complication was hemopneumothorax and no catastrophic complications occurred. ENB localization technology achieved higher safety and operability, because all operations can be carried out in the operating room. Patients in CT-guided puncture hook localization group needed to be transported from CT room to operating room, which increases the risk of whole localization process. In addition, 6 (5.7%) patients in CT-guided localization group failed to be located, mostly because of the deviation of the puncture hook position. Localization time was longer in ENB group because path setting has to be conducted before localization. ENB achieves lower complication and failure rate and increases localization time compared with CT-guided puncture hook localization.
As for the size of pulmonary nodules in our inclusion criteria, we only included nodules less than 10 mm. For 6–12 mm pulmonary nodules, the volume or solid components increased during the follow-up period according to NCCN guidelines. Patients with pulmonary nodules ≥ 12 mm should be diagnosed and treated as early as possible according to the Chinese Consensus on diagnosis and treatment of pulmonary nodules. If the diagnosis cannot be confirmed, multidisciplinary team (MDT) discussion is recommended. It is difficult to locate the pulmonary nodules smaller than 10 mm in clinical operation. Therefore, the size of pulmonary nodules in our retrospective study is smaller than 10 mm.
The operation cannot be performed after localization immediately in CT-guided hook wire localization method. Patients need to wait for surgical resection with a puncture hook which increases the complexity and risks of the operation. However, the procedure does not require additional facilities such as radiotracer, contrast injection or coil insertion. Therefore, CT-guided puncture hook localization is widely used in clinical applications for this method is simple, feasible and less costly. ENB method requires more labor and experience to master and is low cost-effectiveness, while it achieves smaller trauma, more accurate localization and higher safety. ENB also has potential to conduct interventional lung surgery13,15,16,17,18. Therefore, ENB localization technology has a good application prospect.
Conclusions
In conclusion, CT-guided localization is simple and feasible for uncertain pulmonary nodules before surgery. ENB localization could identify small lung nodules with high accuracy and low incidence of complications.
Abbreviations
- CT:
-
Computed tomographic imaging
- ENB:
-
Electromagnetic navigation bronchoscopy
- VATS:
-
Video-assisted thoracoscopic surgery
- PD:
-
Distance from pleural distance
- GGO:
-
Ground-glass opacity
- AIS:
-
Adenocarcinoma in situ
- MIA:
-
Minimally invasive adenocarcinoma
- IA:
-
Invasive adenocarcinoma
References
Siegel, R. L., Miller, K. D. & Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 68, 7–30. https://doi.org/10.3322/caac.21442 (2018).
Rubin, G. D. Lung nodule and cancer detection in computed tomography screening. J. Thorac. Imaging 30, 130–138. https://doi.org/10.1097/RTI.0000000000000140 (2015).
Park, C. H. et al. Comparative effectiveness and safety of preoperative lung localization for pulmonary nodules: a systematic review and meta-analysis. Chest 151, 316–328. https://doi.org/10.1016/j.chest.2016.09.017 (2017).
Arenberg, D. Electromagnetic navigation guided bronchoscopy. Cancer Imaging 9, 89–95. https://doi.org/10.1102/1470-7330.2009.0016 (2009).
Seijo, L. M. Electromagnetic navigation bronchoscopy: clinical utility in the diagnosis of lung cancer. Lung Cancer (Auckl) 7, 111–118. https://doi.org/10.2147/LCTT.S98643 (2016).
Arias, S. et al. Use of electromagnetic navigational transthoracic needle aspiration (E-TTNA) for sampling of lung nodules. J. Vis. Exp. 5, 2723. https://doi.org/10.3791/52723 (2015).
Narsule, C. K. et al. The efficacy of electromagnetic navigation to assist with computed tomography-guided percutaneous thermal ablation of lung tumors. Innovations (Phila) 7, 187–190. https://doi.org/10.1097/IMI.0b013e318265b127 (2012).
Makris, D. et al. Electromagnetic navigation diagnostic bronchoscopy for small peripheral lung lesions. Eur. Respir. J. 29, 1187–1192. https://doi.org/10.1183/09031936.00165306 (2007).
Lee, N. K. et al. CT-guided percutaneous transthoracic localization of pulmonary nodules prior to video-assisted thoracoscopic surgery using barium suspension. Korean J. Radiol. 13, 694–701. https://doi.org/10.3348/kjr.2012.13.6.694 (2012).
Bellomi, M. et al. Computed tomography-guided preoperative radiotracer localization of nonpalpable lung nodules. Ann. Thorac. Surg. 90, 1759–1764. https://doi.org/10.1016/j.athoracsur.2010.08.016 (2010).
Kondo, R. et al. Intraoperative ultrasonographic localization of pulmonary ground-glass opacities. J. Thorac. Cardiovasc. Surg. 138, 837–842. https://doi.org/10.1016/j.jtcvs.2009.02.002 (2009).
Doo, K. W. et al. Needlescopic resection of small and superficial pulmonary nodule after computed tomographic fluoroscopy-guided dual localization with radiotracer and hookwire. Ann. Surg. Oncol. 22, 331–337. https://doi.org/10.1245/s10434-014-3884-2 (2015).
Munoz-Largacha, J. A., Ebright, M. I., Litle, V. R. & Fernando, H. C. Electromagnetic navigational bronchoscopy with dye marking for identification of small peripheral lung nodules during minimally invasive surgical resection. J. Thorac. Dis. 9, 802–808. https://doi.org/10.21037/jtd.2017.03.18 (2017).
Pearlstein, D. P., Quinn, C. C., Burtis, C. C., Ahn, K. W. & Katch, A. J. Electromagnetic navigation bronchoscopy performed by thoracic surgeons: one center’s early success. Ann. Thorac. Surg. 93, 944–949. https://doi.org/10.1016/j.athoracsur.2011.11.006 (2012) ((Discussion 949–950)).
Xie, F. et al. Navigation bronchoscopy-guided radiofrequency ablation for nonsurgical peripheral pulmonary tumors. Respiration 94, 293–298. https://doi.org/10.1159/000477764 (2017).
Banovac, F. et al. Radiofrequency ablation of lung tumors in swine assisted by a navigation device with preprocedural volumetric planning. J. Vasc. Interv. Radiol. 21, 122–129. https://doi.org/10.1016/j.jvir.2009.09.012 (2010).
Amalou, H. & Wood, B. J. Electromagnetic tracking navigation to guide radiofrequency ablation of a lung tumor. J. Bronchol. Interv. Pulmonol. 19, 323–327. https://doi.org/10.1097/LBR.0b013e31827157c9 (2012).
Zhao, Z. R., Lau, R. W. H. & Ng, C. S. H. Catheter-based alternative treatment for early-stage lung cancer with a high-risk for morbidity. J. Thorac. Dis. 10, S1864–S1870. https://doi.org/10.21037/jtd.2018.03.151 (2018).
Acknowledgements
None.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
L.M. designed research; T.Y., L.M., W.C., Y.W.M. and T.H. conducted research; T.H. and Y.W.M. analyzed data; T.Y. and W.C. wrote the paper; L.M. had primary responsibility for final content. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tian, Y., Wang, C., Yue, W. et al. Comparison of computed tomographic imaging-guided hook wire localization and electromagnetic navigation bronchoscope localization in the resection of pulmonary nodules: a retrospective cohort study. Sci Rep 10, 21459 (2020). https://doi.org/10.1038/s41598-020-78146-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-78146-z
- Springer Nature Limited
This article is cited by
-
Comparison of laser guidance and freehand hook-wire for CT-guided preoperative localization of pulmonary nodules
Journal of Cardiothoracic Surgery (2024)