
Abstract
Current research regarding the association between body mass index (BMI) and altered clinical outcomes of sepsis in Asian populations is insufficient. We investigated the association between BMI and clinical outcomes using two Japanese cohorts of severe sepsis (derivation cohort, Chiba University Hospital, n = 614; validation cohort, multicenter cohort, n = 1561). Participants were categorized into the underweight (BMI < 18.5) and non-underweight (BMI ≥ 18.5) groups. The primary outcome was 28-day mortality. Univariate analysis of the derivation cohort indicated increased 28-day mortality trend in the underweight group compared to the non-underweight group (underweight 24.4% [20/82 cases] vs. non-underweight 16.0% [85/532 cases]; p = 0.060). In the primary analysis, multivariate analysis adjusted for baseline imbalance revealed that patients in the underweight group had a significantly increased 28-day mortality compared to those in the non-underweight group (p = 0.031, adjusted odds ratio [OR] 1.91, 95% confidence interval [CI] 1.06–3.46). In a repeated analysis using a multicenter validation cohort (underweight n = 343, non-underweight n = 1218), patients in the underweight group had a significantly increased 28-day mortality compared to those in the non-underweight group (p = 0.045, OR 1.40, 95% CI 1.00–1.97). In conclusion, patients with a BMI < 18.5 had a significantly increased 28-day mortality compared to those with a BMI ≥ 18.5 in Japanese cohorts with severe sepsis.
Similar content being viewed by others

Introduction
Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection1; the excessive spillover of humoral mediators, including interleukin (IL)-6, into the systemic circulation is a well-known component of the dysregulated response2. Body mass index (BMI), which is a measure of body fat, is associated with an altered inflammatory response3. BMI is a non-invasively measurable physical characteristic and clinically practical variable; therefore, greater understanding of the relationship between BMI and altered clinical outcomes may contribute to improvements in basic sepsis care4.
A recent systematic review found eight studies investigating whether BMI was associated with altered outcome of sepsis; however, all studies were conducted in either Europe or North America5. The systematic review concluded that patients with an increased BMI improved survival following sepsis4,6. By contrast, patients with a low BMI significantly increased blood IL-6 levels compared to those with a high BMI in North America3. However, studies regarding BMI in sepsis in Asian populations are limited; after the publication of the systematic review, a single-center study of sepsis with a small sample size in China reported that patients with a low BMI had increased mortality7. Non-obese patients were more common in Asian countries than in Europe and North America8,9,10.
Thus, we tested the hypothesis that patients with a lower BMI have worse clinical outcomes through an altered inflammatory response using large Japanese cohorts of severe sepsis. The primary outcome was 28-day mortality, and blood IL-6 levels were measured in the derivation cohort.
Methods
Study setting and patients
This observational study deployed the following severe sepsis cohorts. The methods were conducted in accordance with the Declaration of Helsinki and relevant guidelines.
Derivation cohort: a single-center cohort
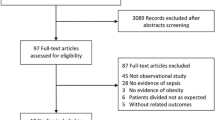
Patients admitted to the intensive care unit (ICU) at Chiba University Hospital, Japan, between October 2012 and May 2019 were retrospectively screened, and patients with severe sepsis were assessed for eligibility11. Patients who had missing data regarding BMI and mortality were excluded.
Validation cohort: multicenter cohorts
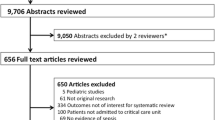
The validation cohort consisted of Japanese Association for Acute Medicine Sepsis Registry (JAAMSR) and Focused Outcomes Research in Emergency Care in Acute Respiratory Distress Syndrome, Sepsis, and Trauma (FORECAST) cohorts. These two cohorts were multicenter, prospective, observational studies conducted by the Japanese Association for Acute Medicine (JAAM) without an overlapping duration for patient enrollment. JAAMSR recruited patients with severe sepsis from 15 ICUs in Japan between June 2010 and May 2011. FORECAST, which followed JAAMSR and was conducted by the JAAM, enrolled study participants with severe sepsis from 59 ICUs in Japan between January 2016 and March 2017. We made the decision to combine the two cohorts with the aim of strengthening the robustness. Because our institution had participated in FORECAST, the population that overlapped with the derivation cohort was removed from the validation cohort.
Data collection and definition
We chose our normal BMI range in accordance with the World Health Organization (WHO) classification (18.5 ≤ BMI < 25.0). The WHO classification has two high BMI categories (25.0 ≤ BMI < 30.0 and BMI ≥ 30.0). However, due to the small sample size of the highest BMI category (BMI ≥ 30.0, 7.3% in the derivation cohort), we combined the two high BMI categories. We first screened for differences in mortality between the abnormal BMI (underweight, BMI < 18.5 or overweight, BMI ≥ 25.0) and normal (18.5 ≤ BMI < 25.0) groups in the derivation cohort. Significant discovery results were tested for replication and generalizability in a multicenter validation cohort.
Blood IL-6 levels in the derivation cohort were rapidly measured after blood sample collections on days 1, 2, and 3 at the clinical laboratory in Chiba University Hospital using rapid measurement systems (IL-6, Roche Diagnostics, Tokyo, Japan)12. Raw data were converted into a logarithmic scale for analysis.
Severe sepsis and septic shock were defined according to the Sepsis-2 criteria11. All patients received treatment according to the international guidelines for the management of severe sepsis and septic shock13,14.
Statistical analysis
Data are presented as medians (quartiles). Categorical data were analyzed using the Pearson’s chi-square test. The Mann–Whitney U test or Kruskal–Wallis test was used for unpaired comparisons depending on the number of groups.
Multivariate logistic regression was used to analyze 28-day mortality by the BMI category. We selected this approach to adjust for potential baseline imbalances, including age, sex, the Sequential Organ Failure Assessment (SOFA) score, and site of infection. We compared blood IL-6 levels measured on days 1, 2 and 3 between the BMI categories using a generalized estimating equation.
Statistical significance was determined by a two-tailed p value < 0.05. Data were analyzed using SPSS software version 24.0 (IBM Corporation, Armonk, NY, USA) and GraphPad Prism 6 (GraphPad Software, San Diego, CA, USA).
Ethical approval and consent to participate
The institutional review board at Chiba University Graduate School of Medicine approved this study and waived the need for written informed consent from subjects or their legal surrogates.
Results
Baseline patient characteristics
Of the 785 patients treated during the study period, 614 were included in this analysis (Supplementary Fig. S1 online). Participants were categorized by BMI into the following groups: underweight (n = 82), normal weight (n = 350), and overweight (n = 182). No significant differences were observed in baseline characteristics, except increased probability of diabetes mellitus, higher white blood cell counts, and serum creatinine levels in the overweight group (Supplementary Table S1 online).
Primary outcome in the derivation cohort
The 28-day mortality rate was 24.4%, 15.7%, and 16.5% in the underweight, normal, and overweight groups, respectively. According to the screening analysis, we chose the potential threshold of BMI 18.5 and further analyzed between the underweight (BMI < 18.5) and non-underweight (BMI ≥ 18.5) groups (Table 1). Univariate analysis revealed a non-significant trend of increased 28-day mortality in the underweight group (24.4%) compared to the non-underweight group (16.0%) (p = 0.060).
Multivariate logistic regression analysis to adjust for potential baseline imbalances including age, male sex, the SOFA score, and site of infection indicated that patients with severe sepsis in the underweight group had a significantly increased 28-day mortality compared to those in the non-underweight group (p = 0.031, adjusted odds ratio [OR] 1.91, 95% confidence interval [CI] 1.06–3.46) (Table 2A).
Primary outcome in the validation cohort
To validate the increased mortality of the underweight group, we deployed a validation cohort enrolling 1561 patients (underweight n = 343, non-underweight n = 1218) (Supplementary Fig. S2 online). There were significant differences in age, site of infection, proportion of patients with diabetes mellitus and chronic lung disease, white blood cell count, and serum creatinine levels according to BMI classifications (Supplementary Table S2 online). A repeated multivariate analysis indicated that patients with severe sepsis in the underweight group had a significantly increased 28-day mortality compared to those in the non-underweight group (p = 0.045, adjusted OR 1.40, 95% CI 1.00–1.97) (Table 2B). To rule out the bias due to the comorbidities, we performed another logistic regression model using Charlson co-morbidities index with the data set of FORECAST study. As a result, the underweight group showed consistent worse outcome after correction with comorbidities.
Primary outcome in the combined cohorts
To investigate the accuracy of the findings in the derivation and validation cohorts, we combined the two cohorts enrolling 2175 patients (underweight n = 425, non-underweight n = 1750). There were significant differences in age, site of infection, proportion of patients with diabetes mellitus, stroke, and chronic lung disease, white blood cell count, and serum creatinine levels between the underweight and non-underweight group (Supplementary Fig. S3 online). The underweight group remained a significant predictor for 28-day mortality in the logistic regression model (p = 0.006, adjusted OR 1.50, 95% CI 1.12–2.00) (Table 2C).
IL-6 analysis in the derivation cohort
Data regarding blood IL-6 levels were available for 413 of the 614 study subjects. There was a non-significant trend of increased blood IL-6 levels in the underweight group compared to the non-underweight group, as determined through a generalized estimating equation using log-converted blood IL-6 levels from days 1, 2, and 3 (p = 0.088, adjusted OR 1.24, 95% CI 0.96–1.60) (Fig. 1). To evaluate the predictive accuracy of the logistic regression model after adjustment with blood IL-6 levels, we performed another analysis predicting 28-day mortality. While the underweight group showed a consistent significance as an independent predictor for 28-day mortality with either of IL-6 levels, only IL-6 levels at day3, but not IL-6 levels at day1 and day2, was a significant variable for predicting the outcome during sepsis (Supplementary Table S4 online).

Comparison of blood IL-6 levels between the underweight (BMI < 18.5) and non-underweight (BMI ≥ 18.5) group at days 1, 2, and 3. There was a non-significant trend of increased blood IL-6 levels in the underweight group compared to the non-underweight group in a generalized estimating equation using log-converted serum IL-6 concentration at days 1, 2, and 3 (p = 0.088, adjusted OR 1.24, 95% CI 0.96–1.60). IL interleukin, BMI body mass index.
Discussion
The present study of severe sepsis, using two large Japanese cohorts, found that patients with a BMI < 18.5 had an increased 28-day mortality. There was a trend of increased blood IL-6 levels in patients with a BMI < 18.5 during the initial 3 days.
Over the years, whether BMI was associated with altered mortality of patients with severe sepsis has been rarely reported in Asian population; we only found one single-center study with a small sample size (sepsis n = 178) conducted in a Chinese population. In the Chinese study, patients with a BMI < 18.5 had the highest 90-day mortality (66.7%) compared to the other subgroups with BMI ≥ 18.5 (18.2–48.0%)7. In accordance with these findings, the present study that enrolled 2175 patients with severe sepsis in total verified the increased mortality in patients with a BMI < 18.5. While the recent meta-analysis of BMI studies in Europe, North America, and Australia highlighted the benefit of obesity in sepsis15, two sepsis studies in North America revealed patients with a low BMI had increased mortality, which were in line with the results of this study16,17. Notably, the underweight group only accounted for 4.9–6% of the North American study, whereas our two cohorts included more than three times (19%) the percentage of patients with low BMI16,17. Therefore, our study is potentially more robust with regard to the conclusions derived from the data.
Differences in physical characteristics between the Asian and Western population, including body fat and muscle mass, have been widely recognized8,9. As such, the average BMI of 22.1 in the present study was lower than the BMI reported in previous European and North American studies (range 25.1–26.1)18,19 but similar to the median BMI of 22.5 that was previously reported in critically ill Japanese patients20. A single-center Japanese study including all critically ill patients (n = 1,616, sepsis fraction unknown) revealed that patients with a BMI < 18.5 had a significantly increased mortality compared to those with a BMI ≥ 18.520, thus supporting the use of the BMI < 18.5 threshold for distinguishing low BMI groups in Asian populations10.
Plausible mechanisms postulated by bench studies could strengthen the relationship between low BMI populations and worse outcomes following sepsis. Lipoproteins and adipose tissue have a protective effect on the survival of sepsis patients through binding pathogen lipids and sequestering lipopolysaccharide (LPS), which could decrease systemic inflammation21,22. As proof of these interactions, our study highlighted the trend of higher blood IL-6 levels in patients with a lower BMI. An elevation of blood IL-6 levels, used for classifying severity of sepsis23,24,25, reinforces the plausibility of poor outcomes in patients with a low BMI. Furthermore, in accordance with our results, Wacharasint et al. also found that in Canadian population, patients with a BMI < 25 had worse outcomes and higher blood IL-6 levels3.
This study has limitations that need to be addressed. First, we analyzed data retrospectively. Second, we used BMI as a surrogate value to assess the percentage of body fat, but this might not be accurate for the evaluation of metabolic status without more detailed information. Therefore, adding other measurements, such as muscle volume or lipid markers, would be greatly beneficial to further understand the effect of metabolism on clinical outcomes following sepsis.
Conclusions
In Japanese cohorts of severe sepsis, patients with a BMI < 18.5 had a significantly increased 28-day mortality compared to those with a BMI ≥ 18.5.
Data availability
The datasets used and analyzed during our study are available from the corresponding author upon reasonable request.
References
Singer, M. et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 315, 801–810. https://doi.org/10.1001/jama.2016.0287 (2016).
Vincent, J. L., Opal, S. M., Marshall, J. C. & Tracey, K. J. Sepsis definitions: time for change. Lancet 381, 774–775. https://doi.org/10.1016/S0140-6736(12)61815-7 (2013).
Wacharasint, P., Boyd, J. H., Russell, J. A. & Walley, K. R. One size does not fit all in severe infection: obesity alters outcome, susceptibility, treatment, and inflammatory response. Crit. Care 17, R122. https://doi.org/10.1186/cc12794 (2013).
Ng, P. Y. & Eikermann, M. The obesity conundrum in sepsis. BMC Anesthesiol. 17, 147. https://doi.org/10.1186/s12871-017-0434-z (2017).
Wang, S. et al. The role of increased body mass index in outcomes of sepsis: a systematic review and meta-analysis. BMC Anesthesiol. 17, 118. https://doi.org/10.1186/s12871-017-0405-4 (2017).
Schetz, M. et al. Obesity in the critically ill: a narrative review. Intensive Care Med. 45, 757–769. https://doi.org/10.1007/s00134-019-05594-1 (2019).
Zhou, Q. et al. Impact of body mass index on survival of medical patients with sepsis: a prospective cohort study in a university hospital in China. BMJ Open 8, e021979. https://doi.org/10.1136/bmjopen-2018-021979 (2018).
Consultation, W. H. O. E. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 363, 157–163. https://doi.org/10.1016/S0140-6736(03)15268-3 (2004).
Lee, K. Metabolically obese but normal weight (MONW) and metabolically healthy but obese (MHO) phenotypes in Koreans: characteristics and health behaviors. Asia Pac. J. Clin. Nutr. 18, 280–284 (2009).
Zheng, W. et al. Association between body-mass index and risk of death in more than 1 million Asians. N. Engl. J. Med. 364, 719–729. https://doi.org/10.1056/NEJMoa1010679 (2011).
Levy, M. M. et al. 2001 SCCM/ESICM/ACCP/ATS/SIS international sepsis definitions conference. Crit. Care Med. 31, 1250–1256. https://doi.org/10.1097/01.CCM.0000050454.01978.3B (2003).
Shimazui, T. et al. Association between serum levels of interleukin-6 on ICU admission and subsequent outcomes in critically ill patients with acute kidney injury. BMC Nephrol. 20, 74. https://doi.org/10.1186/s12882-019-1265-6 (2019).
Dellinger, R. P. et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit. Care Med. 41, 580–637. https://doi.org/10.1097/CCM.0b013e31827e83af (2013).
Rhodes, A. et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 43, 304–377. https://doi.org/10.1007/s00134-017-4683-6 (2017).
Pepper, D. J. et al. Increased body mass index and adjusted mortality in ICU patients with sepsis or septic shock: a systematic review and meta-analysis. Crit. Care 20, 181. https://doi.org/10.1186/s13054-016-1360-z (2016).
Pepper, D. J. et al. Does obesity protect against death in sepsis? A retrospective cohort study of 55,038 adult patients. Crit. Care Med. 47, 643–650. https://doi.org/10.1097/CCM.0000000000003692 (2019).
Li, S. et al. Increased body mass index linked to greater short- and long-term survival in sepsis patients: a retrospective analysis of a large clinical database. Int. J. Infect. Dis. 87, 109–116. https://doi.org/10.1016/j.ijid.2019.07.018 (2019).
Gaulton, T. G. et al. A retrospective cohort study examining the association between body mass index and mortality in severe sepsis. Intern. Emerg. Med. 10, 471–479. https://doi.org/10.1007/s11739-015-1200-1 (2015).
Sakr, Y. et al. Obesity is associated with increased morbidity but not mortality in critically ill patients. Intensive Care Med. 34, 1999–2009. https://doi.org/10.1007/s00134-008-1243-0 (2008).
Yatabe, T., Yamashita, K. & Yokoyama, M. Lower body mass index is associated with hospital mortality in critically ill Japanese patients. Asia Pac. J. Clin. Nutr. 25, 534–537. https://doi.org/10.6133/apjcn.092015.21 (2016).
Walley, K. R. et al. PCSK9 is a critical regulator of the innate immune response and septic shock outcome. Sci. Transl. Med. 6, 258ra143. https://doi.org/10.1126/scitranslmed.3008782 (2014).
Shimada, T. et al. Very low density lipoprotein receptor sequesters lipopolysaccharide into adipose tissue during sepsis. Crit. Care Med. 48, 41–48. https://doi.org/10.1097/CCM.0000000000004064 (2020).
Shimazui, T., Matsumura, Y., Nakada, T. A. & Oda, S. Serum levels of interleukin-6 may predict organ dysfunction earlier than SOFA score. Acute Med. Surg. 4, 255–261. https://doi.org/10.1002/ams2.263 (2017).
Takahashi, W., Nakada, T. A., Yazaki, M. & Oda, S. Interleukin-6 levels act as a diagnostic marker for infection and a prognostic marker in patients with organ dysfunction in intensive care units. Shock 46, 254–260. https://doi.org/10.1097/SHK.0000000000000616 (2016).
Oda, S. et al. Sequential measurement of IL-6 blood levels in patients with systemic inflammatory response syndrome (SIRS)/sepsis. Cytokine 29, 169–175. https://doi.org/10.1016/j.cyto.2004.10.010 (2005).
Acknowledgements
We thank all contributors of the JAAM FORECAST group.
Author information
Authors and Affiliations
Consortia
Contributions
T.O., S.K., T.S., and T.N., study concept and design, acquisition of data, statistical analysis and interpretation of data, drafting the manuscript, and critical revision of the manuscript for important intellectual content. All other authors, acquisition of data and interpretation of data, and revising the article critically for important intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
This work was supported by the Japanese Association for Acute Medicine (JAAM). The JAAM had no role in the study design, analysis of the data, or preparation of the manuscript. Tadanaga Shimada is currently receiving a grant (FDN 20K09301) from “Japan Society for the Promotion of Science”. The remaining authors have disclosed that they do not have any conflicts of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Oami, T., Karasawa, S., Shimada, T. et al. Association between low body mass index and increased 28-day mortality of severe sepsis in Japanese cohorts. Sci Rep 11, 1615 (2021). https://doi.org/10.1038/s41598-020-80284-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-80284-3
- Springer Nature Limited
This article is cited by
-
Association of body mass index with mortality of sepsis or septic shock: an updated meta-analysis
Journal of Intensive Care (2023)
-
Management of intoxicated patients – a descriptive outcome analysis of 4,267 ICU patients
BMC Emergency Medicine (2022)
-
Underweight but not overweight is associated with excess mortality in septic ICU patients
Wiener klinische Wochenschrift (2022)
-
Expert consensus on the monitoring and treatment of sepsis-induced immunosuppression
Military Medical Research (2022)