
Abstract
Increased brachial systolic blood-pressure (BP) predicts diabetes (T2DM) but is not fully effective. Value of absolute ankle systolic BP for T2DM compared to brachial systolic BP is not known. Our objectives were to assess independent relationships of ankle-systolic BP with T2DM and cardiovascular disease in Europeans and south Asians. Cross-sectional studies of anonymised data from registered adults (n = 1087) at inner city deprived primary care practices. Study includes 63.85% ethnic minority. Systolic BP of the left and right-brachial, posterior-tibial and dorsalis-pedis-arteries measured using a Doppler probe. Regression models’ factors were age, sex, ethnicity, body mass index (BMI) and waist height ratio (WHtR). Both brachial and ankle systolic-BP increase with diabetes in Europeans and south Asians. We demonstrated that there was a significant positive independent association of ankle BP with diabetes, regardless of age and sex compared to Brachial. There was stronger negative association of ankle blood pressure with cardiovascular disease, after adjustment for BMI, WHtR and ethnicity. Additionally, we found that ankle BP were significantly associated with cardiovascular disease in south Asians more than the Europeans; right posterior tibial. Ankle systolic BPs are superior to brachial BPs to identify risks of Type 2DM and cardiovascular diseases for enhanced patient care.
Similar content being viewed by others


Introduction
Ninety percent of people with prediabetes are unaware of their condition and 30% of patients will have cardiovascular diseases, retinal, renal, neural complication of type 2 diabetes (T2DM) at the time of diagnosis of1. Therefore, it is imperative that timely screening of increased risk is carried out with simple, yet efficient tools for prevention of overt T2DM.
Currently, the diabetes screening tools for T2DM are based on age, gender (gestational diabetes), family-history of T2DM (FHoD), high brachial blood-pressure (BP), ethnicity, physical activity and body-mass-index (BMI). These do not perform well and miss 50% of patients with T2DM2,3. Ethnicity an underlying risk factor, since the risk profile of south Asians (originally from Indian, Pakistan, Nepal, Sri Lanka or Bangladesh) is different4,5. Greater increases in ankle systolic BP and cardiovascular disease have been reported in south Asians compared to Europeans with a history of T2DM6,7.
Type 2 diabetes is more closely associated with metabolic or visceral obesity and waist-to-height-ratio (WHtR) and insulin resistance8. Cardiovascular risk in south Asians is principally due to greater hyperglycaemia9,10. Insulin resistance-related local vascular changes are more common in the lower limb than the upper limb11.
We hypothesized that ankle systolic BP will be a more significant discriminator for T2DM and cardiovascular disease than brachial systolic BP, especially in south Asians.
Results
Characteristics of participants
The characteristics of the participants were classified as having (1) no T2DM & no cardiovascular disease (2) T2DM (3) cardiovascular disease (4) T2DM & cardiovascular disease (Tables 1 and 2)12. Interestingly, we noted that south Asians were younger than Europeans across all four subsets of health conditions. The percentage with known hypertension was greater in Europeans than south-Asians in all four subsets. Similar results were observed for measured raised brachial systolic BP. Furthermore, ankle systolic BP was higher in patients with T2DM (diagnosed at an average age of 48 years in south Asians and 58 years in Europeans) (Tables 1 and 2).
Systolic BP were associated with cardiovascular disease and diabetes status in Europeans
The linear regression models using beta unstandardized coefficients (B) were used to estimate the association of six systolic BP levels to cardiovascular disease and T2DM status (Table 3). There were significant linear association between both systolic brachial, as well as the dorsalis pedis BP and cardiovascular disease (brachial right, P < 0.001; brachial left, P < 0.001; dorsalis pedis right leg, P < 0.018; dorsalis pedis left leg, P < 0.001). Among these four BP measurements, dorsalis pedis left leg was highly associated with cardiovascular disease (B = 7.82 [3.82–11.81]). Intriguingly, all six systolic BP (brachial, dorsalis pedis and posterior tibial) were significantly associated with T2DM. All beta coefficients were positive, indicating a positive association between BP and T2DM. In General model B, posterior tibial right leg and dorsalis pedis left leg are both strongly associated with T2DM (B = 14.63 [10.67–18.58] and B = 14.30 [10.49–18.12]). Therefore, ankle systolic and brachial systolic BP were strongly correlated with cardiovascular disease and T2DM in Europeans.
Negative association between blood pressures and cardiovascular disease status
To further extend the analysis from general model presented in Table 3, the linear regression models were divided to three models adjusted to the respective parameters; model 1, adjusted for age and sex; model 2, adjusted to age, sex, BMI, WHtR and six ethnicity groups; and model 3, adjusted to age, sex, BMI, WHtR and two ethnic groups as categorical variable (Table 4). In model 1, after adjusting for age and sex, no association was found between right brachial, left brachial, right dorsalis pedis and left dorsalis pedis (P > 0.05) BP. However, there was a negative association of right posterior tibial BP with cardiovascular disease (B = − 4.98 [− 9.22 to − 0.075]). In model 2 and model 3, the analyses were similar to model 1 but additionally adjusted to BMI, WHtR and ethnicity. Consistently, we found that the posterior tibial right leg BP negatively associated with cardiovascular disease in model 2 and model 3 (P < 0.05). Additionally, when the ethnicity was restricted to European and south Asian populations, brachial right, left posterior tibial and left dorsalis pedis BP were negatively associated with cardiovascular diseases. Right posterior tibial BP was significantly different across all 3 models. The association of ankle BP was more significant than brachial BP with cardiovascular diseases. Therefore, ankle BP showed independent negative association with CVD.
Positive associations between ankle blood pressures and diabetes status
Based on the General Model B in Table 3, the analysis was adjusted for age and sex (model 1) and BMI, WHtR and ethnicity (model 2) to analyse the association of ankle BP with T2DM. (Table 5). Additionally, ethnic group was subcategorised into Europeans and south Asians (model 3). In model 1, positive associations were evidenced in right posterior tibial (B = 6.06 [1.73–10.40]) and left dorsalis pedis BP (B = 4.26 [0.14–8.37]). However, no association was found when the analyses were adjusted for BMI, WHtR and ethnicity. Therefore, there was a significant positive independent association of ankle BP with T2DM, regardless of ethnicity, BMI and WHtR, indicating that ankle BP is better discriminator than brachial for T2DM.
Associations between blood pressures and cardiovascular disease status in European and South Asian populations
Based on model 3 in Table 4 we, further refined the results by investigating the associations between BP and cardiovascular disease; specifically, in Europeans and south Asians (Table 6). Generally, no association was found in all analyses involving Europeans. Ankle BP were significantly associated with cardiovascular disease in south Asians; right posterior tibial (B = − 7.05 [− 12.26 to − 1.83]), left posterior tibial (B = − 5.05 [− 10.00 to − 0.11]) and right dorsalis pedis (B = − 5.53 [− 10.58 to − 0.47]) BP. This result indicate that ankle BP is a better determinant than brachial BP for T2DM and CVD in this cross-sectional study.
Discussion
Our datasets provide a novel insight that ankle systolic BP is a statistically significant, independent determinant for T2DM, especially in south Asians when compared to brachial. Ankle systolic BP are also associated with cardiovascular disease more than the brachial.
This is a first study of comparison of associations of brachial and ankle BP with diabetes and cardiovascular disease. We demonstrated a significant and positive independent association of ankle BP with diabetes, regardless of ethnicity. Our findings are biologically plausible since metabolic alterations due to insulin resistance cause structural and functional changes in arteriolar and capillary systems and are more pronounced in the lower extremities13,14,15,16. Peripheral arterial resistance is possibly increased in the arterioles of the lower limb, which may lead to the increase in BP in the arteries of the legs prior to the onset of prediabetes15. Furthermore, athero-thrombotic occlusive changes in arteries leads to lower leg amputations and adverse pathological changes rarely affect upper limbs14. Increased brachial BP are probably reflective of only central pathological changes, whereas increased ankle BP might be indicative of initial local lower limb vascular perturbations15. These local changes may even precede changes in glycosylated haemoglobin8.
In the current study, we observed a negative association of ankle BP with cardiovascular disease, independent of age, gender, BMI, WHtR and ethnicity17.
Ankle BP were significantly associated with cardiovascular disease status in south Asian population compared to Europeans6. It is plausible that ankle systolic BP are highly related to insulin resistance than brachial BP in south Asians. In south Asians, insulin resistance has been observed to be mainly responsible for myocardial infarction and stroke16,18,19. It is well-documented that south Asians probably have predominately, micro-circulatory adverse perturbances compared to macro-circulatory changes, as evidenced by very low prevalence of both peripheral arterial disease (defined by ankle brachial index of < 0.9) and abdominal aortic aneurysms20,21. It is plausible that although the prevalence of hypertension is not higher in south-Asians without diabetes, the BP increases (higher in the ankle than in the brachial arteries) are related to increased risks of cardiovascular diseases22. South Asians have increased diabetic nephropathy, which might also contribute to the development of differential increases in blood pressures of arms and legs19. The United Kingdom government funds general practitioners to screen subjects for cardiovascular disease, over the age of 40 within the National Health Service Health Check programme23. However, screening at this age is too late for south Asians since their risks for cardiovascular diseases, are already established.
Technologically advanced equipment is also available currently for quick and easy automatic systolic BP measurement in lower limbs24. A threshold for ankle systolic BP that predicts a high risk of developing diabetes (or represents HbA1c in the risk of prediabetes range), and assessment of the strength of the associations between WHtR and ankle systolic BP will be clinically useful especially in young south Asians25. Blood pressure measurement is non-invasive and more practical as a population screening tool even in low and middle income countries as it can be done easily using a Doppler machine.
This was the first operational and observational study in primary care to investigate if ankle systolic BPs were better independent discriminators of T2DM and cardiovascular disease compared to brachial. Outcome measures were complete in this cohort, to allow for comprehensive analysis. We compared our results with those of relatively small number of Europeans to learn the impact of south Asian ethnicity increasing the chances of greater impact.
We did not have diet details which might have strengthened our risk models. We cannot establish any causal relationships in the current cross-sectional study design. The left–right bias in blood pressures and differences in proximal and distal arterial blood pressures was not adjusted for in our analysis.
Implications for research and/or practice
Therefore, ankle systolic BPs are superior to brachial BPs to identify risks of Type 2DM and cardiovascular diseases for enhanced patient care. It is important that the novel utilisation of ankle BP in scoring systems for early, cost-effective detection of at-risk individuals in the general population is tested further; especially since early detection is imperative for Covid-19 patients, as well26.
Methods
Participants and study design
The design was cross-sectional and conducted as described before6. The project was performed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement12.
Patient and public involvement
Although patients were not directly involved in the development of the research question, design and outcome measures of this study, patients who participated have helped in the recruitment process of the study by informing their family and relatives. The results will be disseminated to study participants by local Clinical Commissioning Group reports.
Clinical assessment
A standard questionnaire was administered to all participants. Cardiovascular disease was defined as previous history of any of the following: myocardial infarction, stroke, transient ischaemic attack, peripheral arterial disease, angioplasty, coronary artery bypass surgery or heart failure. Participants with a diagnosis of diabetes were identified by review of medical records. History of T2DM was established according to WHO criteria 1999. T2DM duration, cardiovascular risk factors and complications were recorded. Hypertension and hyperlipidaemia were defined as either previously diagnosed or currently taking antihypertensive or cholesterol-lowering medications. Height and weight were recorded (to the nearest 0.01 m and kg, respectively) to calculate each participant’s BMI, calculated as weight/(height)2 (kg/m2). Waist circumference was measured at the midpoint between the lowest rib and iliac crest (to nearest cm) to calculate each participant’s WHtR.
Blood pressure measurements
Participants were rested in the supine position for 5 min before BP measurements were taken using appropriately sized cuffs and a handheld continuous wave Doppler instrument (Huntleigh Super Dopplex II, Huntleigh Healthcare, Cardiff, UK) with an 8 MHz probe and a calibrated mercury sphygmomanometer (http://www.framinghamheartstudy.org/share/protocols/ankle1_8s_protocol.pdf).
Brachial systolic BP was taken in both arms by placement of the cuff in the upper arm and measuring the systolic BP by placing the Doppler probe over the brachial artery in the antecubital fossa. For ankle systolic BP, the blood pressure cuff was positioned superior to the medial malleolus in each leg. Systolic BP was measured over the dorsalis pedis and posterior tibialis arteries on right and left limbs. For each BP measurement, the cuff was inflated until the pulse was no longer audible. The cuff was inflated a further 20 mmHg above the approximate value, at which the pulse was obliterated then deflated slowly, with the pressure being recorded when the pulse became audible using the Doppler probe again.
Should the strength of the relationship between disease (T2DM or cardiovascular disease) depend on factors, such as ethnicity or gender our conclusions will depend on the variations among the participants in our project. We have deliberately recruited from a population enriched for south Asians and those with the relevant conditions studied. Consequently, the effects in our sample may be stronger than those in the general population.
Statistical analysis
For descriptive purposes, patient characteristics based on disease status and ethnicity were summarised and tabulated. Continuous measurements were presented as means ± SDs, categorical measures as absolute numbers and percentages. Data with p values less than 0.05 was considered significantly different and exact values, presented.
R Software version 4.0.2 was used to perform all analysis. Descriptive demographic characteristics were calculated for all subjects. In the first analysis, linear regression models were built to assess the association between six systolic BP and cardiovascular disease and T2DM status. These univariate analyses were named “General model”. The systolic BP measurements were continuous variable while the cardiovascular disease and T2DM status was categorical variable. To extend the analysis, the general model analyses were adjusted to a set of covariates such as age, sex, BMI, waist height ratio and ethnicity. Model 1 was adjusted for age and sex. Model 2 linear regression analysis was adjusted to age, sex, BMI, WHtR and six ethnicity groups. Model 3 was adjusted to age, sex, BMI, WHtR and two major ethnicity groups (European and South Asian). In the final analysis, we aimed to investigate the association of between six systolic BP and cardiovascular disease and T2DM status in two ethnic groups (European and South Asian). A two-tailed P < 0.05 threshold was set as the significant level for all analysis. Since missing data was low, complete case analysis without imputations was carried out.
Ethical approval
The project was approved by the Leeds-Bradford Research Ethics Committee (REC 10/H1302/28) and local Research and Development. All methods and experimental protocols were carried out in accordance with the Declaration of Helsinki (2013). In addition, all methods and experimental protocols were reviewed and approved by the Leeds-Bradford Research Ethics Committee, equivalent to the present 2016 Integrated Research Application System UK. Written informed consent was obtained from each participant according to Good Clinical Practice guidelines. The response rate for recruitment was 60%.
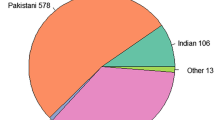
A purposive sample of 1087 consecutive consenting patients were recruited at an inner-city primary care practice in West Yorkshire, UK, as described previously6. Indians, Pakistanis and Bangladeshis, White Europeans, other Asians and different ethnics (e.g. Afro-Caribbean), were the 6 groups. Recruitment of adults was consecutive from all primary care clinics. Inclusion criteria were participants aged ≥ 18 years. There were 694 south Asians (originally from India, Pakistan, Bangladesh or one or more of their grandparents born in one of these countries).
Participant’s ethnicity was based on electronic medical record data or ascertained from demographic data collected at recruitment which were self-reported, surname assignment and country of birth of grandparents. All clinical assessments (i.e., medical history and measurements) were performed at the same visit.
Data availability
The datasets generated during and/or analysed during the current study are not publicly available since patient permission was not sought for the sharing of data, at the time of recruitment.
References
Geiss, L. S. et al. Diabetes risk reduction behaviors among U.S. adults with prediabetes. Am. J. Prev. Med. 38, 403–409 (2010).
Hippisley-Cox, J., Coupland, C., Robson, J., Sheikh, A. & Brindle, P. Predicting risk of type 2 diabetes in England and Wales: Prospective derivation and validation of QDScore. BMJ 338, b880 (2009).
Casagrande, S. S., Cowie, C. C. & Fradkin, J. E. Utility of the U.S. Preventive services task force criteria for diabetes screening. Am. J. Prev. Med. 45, 167–174 (2013).
Wild, S. H., Fischbacher, C., Brock, A., Griffiths, C. & Bhopal, R. Mortality from all causes and circulatory disease by country of birth in England and Wales 2001–2003. J. Public Health. (Oxf) 29, 191–198 (2007).
Joshi, P. et al. Risk factors for early myocardial infarction in South Asians compared with individuals in other countries. JAMA 297, 286–329 (2007).
Kain, K. et al. Ankle pressures in UK South Asians with diabetes mellitus: A case control study. Heart 99, 614–619 (2013).
Kain, K. Absolute systolic ankle blood pressure versus ankle-brachial index. Ann. Intern. Med. 160, 140–141 (2014).
Ashwell, M., Gunn, P. & Gibson, S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: Systematic review and meta-analysis. Obes. Rev. 13, 275–286 (2012).
Bathula, R. et al. South Asians have adverse cerebrovascular haemodynamics, despite equivalent blood pressure, compared with Europeans. This is due to their greater hyperglycaemia. Int. J. Epidemiol. 40, 1490–1498 (2011).
Kain, K. The NHS lacks cardiovascular screening tools suitable for patients of South Asian descent. BMJ 350, h52 (2015).
Britton, K. A. et al. Insulin resistance and incident peripheral artery disease in the cardiovascular health study. Vasc. Med. 17, 85–93 (2012).
STROBE statement--checklist of items that should be included in reports of observational studies (STROBE initiative). Int. J. Public Health 53, 3–4 (2008).
Viswambharan, H. et al. Selective enhancement of insulin sensitivity in the endothelium in vivo reveals a novel proatherosclerotic signaling loop. Circ. Res. 120, 784–798 (2017).
Imrie, H. et al. Novel role of the IGF-1 receptor in endothelial function and repair: Studies in endothelium-targeted IGF-1 receptor transgenic mice. Diabetes 61, 2359–2368 (2012).
Hile, C. & Veves, A. Diabetic neuropathy and microcirculation. Curr. Diab. Rep. 3, 446–451 (2003).
Ahmad, N., Thomas, G. N., Chan, C. & Gill, P. Ethnic differences in lower limb revascularisation and amputation rates. Implications for the aetiopathology of atherosclerosis?. Atherosclerosis 233, 503–507 (2014).
Kain, K. et al. Metabolic obesity and ankle pressures. Diabetes; American Diabetes Association. A523 (2014).
Alshamsan, R. et al. Ethnic differences in diabetes management in patients with and without comorbid medical conditions: a cross-sectional study. Diabetes Care 34, 655–657 (2011).
Eastwood, S. V., Tillin, T., Chaturvedi, N. & Hughes, A. D. Ethnic differences in associations between blood pressure and stroke in south Asian and European men. Hypertension 66, 481–488 (2015).
Kent, K. C. et al. Analysis of risk factors for abdominal aortic aneurysm in a cohort of more than 3 million individuals. J. Vasc. Surg. 52, 539–548 (2010).
Chaturvedi, N. et al. Indian Asian men have less peripheral arterial disease than European men for equivalent levels of coronary disease. Atherosclerosis 193, 204–212 (2007).
Kain, K. Blood pressure lowering for cardiovascular disease. Lancet 388, 126 (2016).
Robson, J. et al. NHS health check comorbidity and management: An observational matched study in primary care. Br. J. Gen. Pract. 67, e86–e93 (2017).
Fowkes, F. G. et al. Ankle brachial index combined with Framingham risk score to predict cardiovascular events and mortality: A meta-analysis. JAMA 300, 197–208 (2008).
Emdin, C. A., Anderson, S. G., Woodward, M. & Rahimi, K. Usual blood pressure and risk of new-onset diabetes: Evidence from 4.1 million adults and a meta-analysis of prospective studies. J. Am. Coll. Cardiol. 66, 1552–1562 (2015).
Muniyappa, R. & Gubbi, S. COVID-19 pandemic, coronaviruses, and diabetes mellitus. Am. J. Physiol. Endocrinol. Metab. 318, E736–E741 (2020).
Acknowledgements
We acknowledge all subjects who participated in this study; medical students of University of Leeds for recruitments and data collection, Leeds Institute of Medical Education (LIME) for sponsoring the students to carry out the project and staffs at Kensington Street Surgery, Bradford.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. Leeds Institute of Medical Education (LIME), University of Leeds sponsored the study.
Author information
Authors and Affiliations
Contributions
It was K.K.'s research concept and data was obtained by K.K. H.V. and K.K. wrote the main manuscript text. C.W.C. analysed data. K.K. and C.W.C. prepared the Tables. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Viswambharan, H., Cheng, C.W. & Kain, K. Differential associations of ankle and brachial blood pressures with diabetes and cardiovascular diseases: cross-sectional study. Sci Rep 11, 9406 (2021). https://doi.org/10.1038/s41598-021-88973-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-88973-3
- Springer Nature Limited
This article is cited by
-
Relationships between ankle blood pressure indices and major adverse cardiovascular events in people with and without type 2 diabetes
Cardiovascular Diabetology (2024)
-
Disparity in association of obesity measures with ankle and brachial systolic blood pressures in Europeans and South Asians
Scientific Reports (2022)