
Abstract
High risk and geriatric patients are supposed to suffer higher risks of hypotension underwent painless endoscopic procedures. This study evaluated different biomarkers associated with hypotension in off-site patients and aimed to determine the most relevant risk factors in space and monitoring limited environment. The inclusions of this observational cohort study underwent complex endoscopic procedures were sedated with age-adjusted doses of target-controlled infusion of propofol. The following pre-sedative parameters were analysed: time domain, frequency domain, and Deceleration capacity (DC) of heart rate variability, estimated cardiac output data and the index of cardiac contractility from the cardiometer. Patients were divided into hypotension group (blood pressure < 90 mmHg or a > 35% decrease) and non-hypotension group according to peri-sedative blood pressure, regression analysis is used to examine the association between factors and hypotension. Total data from 178 patients (age range: 33–94 years) were analysed. Age was not significantly different between the hypotension and non-hypotension groups (p = 0.978). Among all the factors, DC was most associated with hypotension (p = 0.05), better than cardiometer, age, and ASA status. In conclusion, DC, which can be interpreted as the indicator of parasympathetic activity and was significantly and negatively correlated with sedation-related hypotension. Pre-sedative measuring DC from routine ECG monitoring is simple and cost-effective and should be added to haemodynamic monitoring in the endoscopic room.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
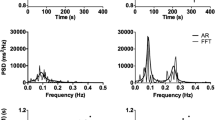
Deceleration capacity (DC), derived from heart rate variability (HRV), represents the capacity of the cardiovascular system for dynamic changes while responding to physical and psychological stimuli. HRV is the physiological phenomenon of variation in the time interval between heartbeats; the time-domain HRV parameters include the standard deviation of Normal-to-Normal intervals (SDNN) and the root mean square power of the successive differences (RMSSD) between adjacent NN intervals. The low frequency/high frequency (LF/HF) ratio represents frequency-domain HRV1. Phase-rectified signal averaging (PRSA) is an efficient method for analysing quasi-periodicities in noisy and nonstationary time series, such as the HRV time series2. The central deflection of the PRSA curve characterises the average capacity of the heart to decelerate the cardiac rhythm, denoted as DC, which represents the ability of the parasympathetic nervous system to regulate cardiovascular modulation and thus serves as a functional biomarker for parasympathetic capacity. Evidence from experimental and clinical studies indicates that reduced DC is a better predictor of mortality than SDNN or left-ventricular ejection fraction in post-infarction patients3,4. DC and RMSSD of successive r–r intervals better represent parasympathetic modulation ability5. As a nonstationary time-series (such as a heartbeat time series), interruptions that might be caused by internal or external perturbations usually lead to phase jumps, and their frequency is not constant. Both phase jumps and frequency variations disrupt the auto-coherency of the signal. PRSA allows us to solve these issues in the quantification of the typical coherence time for each frequency band and to separate processes occurring during increasing and decreasing parts of the signal6.
Electrical cardiometry (EC) is a new noninvasively method of continuous cardiac output (CO) monitoring based on the measurement of thoracic electrical bioimpedance. The increasing velocity of red blood cell alignment in the thoracic aorta cause concomitant decreases in electrical impedance in the chest7. Compared with other portable noninvasive cardiometers, the EC monitor (ICON Cardiotronics, Inc.) has many benefits including low power, low cost, and convenient access to haemodynamic parameters8. It produces reliable data under various clinical conditions9,10 and estimates CO and the index of contractility (ICON), which are crucial physiological parameters for patient care11.
Invasive upper gastrointestinal endoscopic procedures require moderate to severe sedation instead of conscious sedation12,13 because the endoscopic insertion is painful (outer diameter, 13.7 mm). As the sedation level increases, patients lose the ability to protect the airway and sympathetic response to nociceptive stimulation14; other sedative-related complications can also occur12,15,16, including sedation-related hypotension. Because of the state of relative hypovolemia in patients after fasting and colon preparation17, combined with patient illness and diminution of the sympathetic effect due to sedation, hypotension often occurs, especially in elderly patients18,19. The short-term spasmolytic agent butylscopolamine (buscopan) can inhibit the parasympathetic regulation, leading to increased heart rate, thus decreasing homeostatic ability in elderly patients20,21. Propofol and opioids may cause vasodilation, which may deteriorate the already unpredictable perioperative haemodynamic of elderly patients17,22. Diabetes mellitus is a typical disease causing autonomic dysfunction, so clarification of the diseases that affect the autonomic nerves is important.
The aim of this study was to propose a reliable predictor of sedation-related hypotension for anaesthesiologists while performing sedation of off-site patients with limited space and restricted conditions. This research evaluated the risk of sedation-related hypotension due to age and compared related parameters to determine the most relevant factor predicting sedation-related hypotension.
Results
Demographic data
Twenty-two cases were missed because of incomplete physiological data. Table 1 presents the comparison of demographic data between the patients with and without hypotension (hypotension and no hypotension groups, respectively). The total incidence of hypotensive events was 42%. Sex and age were not significantly different between the two groups. The age range in the hypotension group was 33–94 years. No differences were observed in BMI and procedure time between the two groups; however, the hypotension group had a higher ASA class (p = 0.019). Also the HRV derivatives (DC, RMSD, HF/LF ratio) and EC derivatives (ICON, CO) was also compared. The t-test of ICON and CO showed that there were no differences between two groups (p = 0.165 and 0.925). The other analysis results of the hypotension group revealed the following: the mean DC was 4.68 ± 2.48, the mean RMSD was 26.2 ± 18.36; and the mean HF/LF ratio was 6.41 ± 1.68. The analysis results of non-hypotension group revealed the following: the mean DC was 6.16 ± 2.68 (p = 0.000); the mean RMSD was 32.9 ± 19.13 (p = 0.023); and the mean HF/LF ratio was 5.80 ± 1.88 (p = 0.03).
The history of chronic or systemic diseases was also compared between the groups. Of all the conditions evaluated, only hypertension was related to hypotensive events (p = 0.049). Other conditions, including bedridden status, cerebrovascular accident, haemodialysis (HD), cancer, and > 5% loss of bodyweight, were equivalent between the two groups. In the biochemical examination, albumin level, which represents the blood oncotic pressure, was significantly different between groups. ALT and AST showed large fluctuations between inclusions, are not related between groups. Haemoglobin level was not significantly different between groups. The total number of patients with type 2 DM was 34 out of 178, the number of patients with DM and hypotensive event was 17 out of 74 (23.0%), and the number of patients with DM in control group (normal pressure) was 17 out of 101 (16.8%). The univariate analysis of DM showed that there was no difference in hypotension events (p = 0.313). The other analysis results of the DM group revealed the following: the mean DC was 4.95 ± 2.71, the mean RMSD was 33.88 ± 24.29; the ICON was 41.63 ± 14.65, and the mean AC was 5.60 ± 3.05. The analysis results of non-DM group revealed the following: the mean DC was 5.68 ± 2.68 (p = 0.743); the mean RMSD was 29.07 ± 17.48 (p = 0.092); the ICON was 49.66 ± 17.55 (p = 0.103); and the mean of AC was 5.95 ± 2.97 (p = 0.826). The results of the DM group comparison are showed in Table 2.
Risk factor analysis
Table 3 presents the results logistic regression analysis of factors related to hypotension. We used logistic regression to examine patients’ DC, RMSD, LF/HF ratio, from HRV; ICON and CO from EC, and the factors ASA, HTN and albumin which showed significant differences, as listed in Table 1. The beta coefficient value of DC was negatively related to hypotension; this means the lower the DC, the higher the risk of hypotension. No other variable significantly predicted the outcome of hypotension. As shown in Fig. 1, the area under the curve (AUC) for predicting hypotension was 0.7 ± 0.05, 0.6, 0.56, and 0.46 for DC, RMSD, ICON, and age, respectively. According the DC data, the minimum DC is 0.62, the maximum is 13.15, with mean 5.54 and SD 2,697; according to the result of logistic regression, DC was negatively related to outcome, the DC decrease 1 will increase the hypotension incidence 19%, the cut-off value would be 5.15.

Receiver operating characteristic (ROC) curve for the factors predicting hypotension. The area under the curve (AUC) for deceleration capacity (DC) for the prediction of hypotension is 0.7 ± 0.05. The ideal AUC is 1.0. The reference line (yellow) represents an AUC of 0.5, which is based on chance alone. DC = deceleration capacity, RMSD = root mean square density, ICON = index of contractility.
Discussion
Our results reveal that DC was the best independent predictor of sedation-related hypotension in patients undergoing an endoscopic procedure compared with other parameters of HRV, bioimpedance, or biochemistry; DC was negatively correlated with hypotension. We also used the ROC curves (Fig. 1) to reveal the differences between age, DC, RMSD, and ICON. DC, with an AUC of 0.7, was the most correlated predictor, with acceptable discrimination. We concluded that DC is a reliable predictor of sedation-related hypotension for anaesthesiologists while administering sedation in off-site patients under limited space and restricted conditions. If the DC data can be shown on the haemodynamic monitor along with ECG data, it would be providing convenient and useful information for anaesthesiologists.
Between the hypotension and non-hypotension groups, the basic clinical and demographic data including age, sex, BMI, and procedure time were not significantly different. Age does not represent physiological ageing, and a patient should be evaluated sedative risk according to his or her organ function. No significant differences were observed in past or present history items such as cancer, renal failure, and CVA, except hypertension. In the biochemistry examination, low albumin level was related to hypotension due to low oncotic pressure; the ASA class was also significantly different between groups. This shows that a higher ASA class and lower oncotic pressure is related to hypotension, which is compatible with the risk factors of perioperative hypotension. After the data survey, inclusions with a history of DM had larger incidence of hypotension during sedation without significance. This is because diabetes mellitus with poor control may causes systemic deterioration, including autonomic dysfunction and may not be suitable for the protocol of this study. Anesthesiologists may prefer to use other hypnotics for those patients.
There are two major artefacts in bioimpedance cardiographs: motion artefacts and arrhythmia. During data collection, well-controlled conditions are required to obtain accurate and reliable measurements, which is time consuming. Each time the patient changes position, it takes approximately 2 min to recalculate the parameters. The leads are placed at the left side of patient, and they may have no signal in the decubitus position due to the increased resistance offered by the skin fold. Moreover, the bioimpedance monitor cannot calculate data when a patient has arrhythmia, which is common in elderly patients. In this study, the bioimpedance monitor was not convenient to use or suitable for off-site anaesthesia. Neither EC nor electrocardiography can be used to calculate cardiac biomarkers in patients who have arrhythmia, so we skipped the arrhythmia episode. We waited until the patient has normal sinus rhythm to obtain the first calculable data.
Our patients received invasive procedures with ERCP, EUS, or ERBD. For these procedures, not only is the outer endoscopic diameter larger (13.7 mm) but also the procedure is longer and more invasive; moreover, it is often performed in patients who are weaker. In contrast to panendoscopy, our anaesthetic regimens include opioid, midazolam, and propofol. When the patient is heavily sedated, irregular respiratory pattern and profound vasodilation might occur; sometimes, partial upper airway obstruction is observed, which requires a chin-lift manoeuvre or nasal airway insertion for a while. In our cohort, the overall hypotension incidence during sedation was 42%, which reverted to within the normal range in all cases after initial induction. The age-adjusted dosage maintained with a TCI was convenient for sedation during the endoscopic procedure.
According to the results, the cut-off point of DC is 5.15, patients who need invasive endoscopic procedure with DC less than 5.15 could inform anaesthesiologist for poetical hypotension, whether the patient requires an alternative sedative regimen or volume expansion before sedation. In conclusion, DC was negatively correlated with sedation-related hypotension, and age was not a predictor of sedation-related hypotension.
Methods
Ethics statement
This observational study was approved by the Institutional Review Board of National Taiwan University Hospital with registered number 201612030RIN and was also registered on ClinicalTrials.gov with registered number NCT03292627 (date of registration 25/09/2017). All participants provided written informed consent after careful discussion. We confirmed that all methods were carried out in accordance with relevant guidelines and regulations.
Clinical inclusion
We included 200 patients who underwent endoscopic retrograde cholangiopancreatography (ERCP), an endoscopic ultrasound-guided procedure (EUS), or endoscopic retrograde biliary drainage (ERBD) between March 2017 and July 2019 in National Taiwan University Hospital.
Prior to endoscopic insertion, the standard equipment for vital signs was employed: ECG, a blood pressure cuff used with a 2.5-min inflation interval, and a nasal cannula with 3 L min−1 oxygen. An EC monitor (ICON Cardiotronics, Inc., La Jolla, CA 92,307; Osypka Medical GmbH, Berlin, Germany) was set up, with electrodes placed around the neck and laterally on the thorax as well. The sampling rate of this machine was 1 Hz, and it calculated the patient’s cardiac output data and ICON value every second, which was displayed on the screen. Our data collection can only record inclusions who can have cardiac bioimpedance data; if the patient had arrhythmia such as atrial fibrillation or frequent ventricular premature complex so that the physiological cardiac parameter could not be calculated, it was marked as missing data. Butylscopolamine (buscopan) was administered after the patient was well postured, and 2 min later, sedation was initiated using midazolam (dormicum) (0.025 mg kg−1) and alfentanil (5 ng kg−1) combined with propofol infusion through a target control infuser (TCI). The TCI settings (Schneider mode) were as follows: plasma propofol concentration for patients < 50 years old was 2.9 ng mL−1, that for patients 50–70 years old was 2.4 ng mL−1, and for patients > 70 years old it was 1.6 ng mL−123. The endoscopic procedure started 2 min after propofol infusion, and the investigators collected all the clinical hemodynamic data including NBP, HR and saturation until the end of the procedure (Fig. 2). Data related to body weight loss of > 5%, ambulation capacity, systemic disease, patient demographics, and biochemistry results were also collected.

Flowchart of clinical protocol.
Data analysis
The original electrocardiogram data were analysed using a commercial software package (MATLAB for Windows Ver4.2) for HRV profile. Pre-sedative two minute electrocardiogram data were analyzed. For the peri-sedative hemodynamic data, the criteria for hypotension were either systolic blood pressure < 90 mmHg12 or a decrease in mean blood pressure of > 35% during the first 10 min of the endoscopic procedure22. The fundamental feature of phase-rectified signal averaging is the alignment of the tachogram of HRV relative to selected anchor points followed by signal averaging. PRSA involves four main steps as followed Fig. 32.

Flowchart of DC processing, further biophysics calculation equations are in the supplement.
Statistical analysis
We compared the supine baseline heart rate variability data with clinical hemodynamic data during sedation. SPSS (IBM SPSS Statistics Data Editor version 20) was used for data analysis. Demographic data, including age, height, weight, and presence of cancer, were compared using an independent t test. We also divided the breakdown of these diseases into a hypotensive patient group and a nonhypotensive patient group and summarized them in a table. Logistic regression was used to evaluate the relationship of risk factors (predictors), we choose potential candidate including DC, ICON, RMSD, HF/LF ratio, ASA, HTN and Albumin with hypotension (dependent variable). The p value less than 0.05 was set as significant.
References
Mietus, J. E., Peng, C.-K., Henry, I., Goldsmith, R. L. & Goldberger, A. L. The pNNx files: Re-examining a widely used heart rate variability measure. Heart 88, 378–380 (2002).
Bauer, A. et al. Phase-rectified signal averaging detects quasi-periodicities in non-stationary data. Phys. A 364, 423–434 (2006).
Bauer, A. et al. Deceleration capacity of heart rate as a predictor of mortality after myocardial infarction: Cohort study. Lancet 367, 1674–1681 (2006).
Demming, T. et al. Deceleration capacity: A novel predictor for total mortality in patients with non-ischemic dilated cardiomyopathy. Int. J. Cardiol. 221, 289–293 (2016).
Stein, P. K. et al. Higher levels of inflammation factors and greater insulin resistance are independently associated with higher heart rate and lower heart rate variability in normoglycemic older individuals: The Cardiovascular Health Study. J. Am. Geriatr. Soc. 56, 315–321 (2008).
Bauer, A. et al. Phase-rectified signal averaging detects quasi-periodicities in non-stationary data. Phys. A 364, 423–434 (2006).
Stevanović, P. Thoracic electrical bioimpedance theory and clinical possibilities in perioperative medicine. Signa Vitae 3, 22–27 (2008).
Rajput, R. S., Das, S., Chauhan, S., Bisoi, A. K. & Vasdev, S. Comparison of cardiac output measurement by noninvasive method with electrical cardiometry and invasive method with thermodilution technique in patients undergoing coronary artery bypass grafting. World J. Cardiovasc. Surg. 04, 123–130 (2014).
Kamath, S. A. et al. Correlation of impedance cardiography with invasive hemodynamic measurements in patients with advanced heart failure: The BioImpedance CardioGraphy (BIG) substudy of the Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness (ESCAPE) Trial. Am. Heart J. 158, 217–223 (2009).
Vorwerk, C., Jeyanithi, H. & Coats, T. J. Thoracic electrical bioimpedance: A tool to determine cardiac versus non-cardiac causes of acute dyspnoea in the emergency department. Emerg. Med. J. 27, 359–363 (2010).
Saugel, B., Cecconi, M., Wagner, J. Y. & Reuter, D. A. Noninvasive continuous cardiac output monitoring in perioperative and intensive care medicine. Br. J. Anaesth. 114, 562–575 (2015).
Wadhwa, V. et al. Similar risk of cardiopulmonary adverse events between propofol and traditional anesthesia for gastrointestinal endoscopy: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 15, 194–206 (2017).
McQuaid, K. R. & Laine, L. A systematic review and meta-analysis of randomized, controlled trials of moderate sedation for routine endoscopic procedures. Gastrointest. Endosc. 67, 910–923 (2008).
Garewal, D. & Waikar, P. Propofol sedation for ERCP procedures: A dilemna? Observations from an anesthesia perspective. Diagn. Ther. Endosc. 2012, 639190 (2012).
Conway, A. & Sutherland, J. Depth of anaesthesia monitoring during procedural sedation and analgesia: A systematic review and meta-analysis. Int. J. Nurs. Stud. 63, 201–212 (2016).
Vargo, J. J., Niklewski, P. J., Williams, J. L., Martin, J. F. & Faigel, D. O. Patient safety during sedation by anesthesia professionals during routine upper endoscopy and colonoscopy: An analysis of 138 million procedures. Gastrointest. Endosc. 85, 101–108 (2017).
Committee, ASo. P. et al. Bowel preparation before colonoscopy. Gastrointest. Endosc. 81, 781–794 (2015).
Pih, G. Y. et al. Risk factors for complications and mortality of percutaneous endoscopic gastrostomy insertion. BMC Gastroenterol. 18, 101 (2018).
Zakeri, N., Coda, S., Webster, S., Howson, W. & Thillainayagam, A. V. Risk factors for endoscopic sedation reversal events: A five-year retrospective study. Frontline Gastroenterol. 6, 270–277 (2015).
Sundra, T. M., Harrison, J. L., Lester, G. D., Raidal, S. L. & Phillips, J. K. The influence of spasmolytic agents on heart rate variability and gastrointestinal motility in normal horses. Res. Vet. Sci. 93, 1426–1433 (2012).
Ristikankare, M. & Karinen-Mantila, H. The role of routinely given hyoscine-N-butylbromide in colonoscopy: A double-blind, randomized, placebo-controlled, clinical trial. Scand. J. Gastroenterol. 51, 368–373 (2016).
Reich, D. L. et al. Predictors of hypotension after induction of general anesthesia. Anesth. Analg. 101, 622–628 (2005).
Kazama, T. et al. Optimal propofol plasma concentration during upper gastrointestinal endoscopy in young, middle-aged, and elderly patients. Anesthesiology 93, 662–669 (2000).
Acknowledgements
This manuscript was edited by Wallace Academic Editing. Finally, it is with true pleasure that I acknowledge the contributions of my supervisor, Dr. Antoun Koht of Northwestern University, Finberg School of Medicine, who gave me intellectual discussions about this paper.
Funding
This research was funded by National Taiwan University Hospital, Grant Number: NTUH.107-M3963.
Author information
Authors and Affiliations
Contributions
Study design/IRB: F.F.T., H.P.W. Study conduct/Patient recruitment: F.F.T., C.M.L. Data analysis: F.F.T., J.R.Y. Writing paper: F.F.T., J.R.Y., S.Z.F. Revising paper: F.F.T., S.Z.F.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tsai, FF., Liu, CM., Wang, HP. et al. Deceleration capacity of heart rate variability as a predictor of sedation related hypotension. Sci Rep 11, 10850 (2021). https://doi.org/10.1038/s41598-021-90342-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-90342-z
- Springer Nature Limited