
Abstract
The aims of the present study were to profile the antimicrobial susceptibility patterns of a diverse range of Nocardia species isolated in Japan, and to determine the ability of matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) for species/complex identification. Identification of 153 clinical isolates was performed by full-length 16S rRNA gene sequencing as a reference method to evaluate the usefulness of MALDI-TOF MS identification. Antimicrobial susceptibility testing (AST) for 14 antibiotics was performed using the broth microdilution method against 146 of the isolates. Among the total 153 clinical isolates, Nocardia farcinica complex (25%) was the most common species, followed by Nocardia cyriacigeorgica (18%), Nocardia brasiliensis (9%), Nocardia nova (8%), and Nocardia otitidiscaviarum (7%). Among 150 isolates identified to the species/complex level by 16S rRNA gene sequencing, MALDI-TOF MS with the use of a supplemental Nocardia library (JMLD library ver.ML01) correctly identified 97.3% (n = 146) to the species/complex level and 1.3% (n = 2) to the genus level. Among the 146 Nocardia isolates that underwent AST, the susceptibilities were 100% to linezolid, 96% to amikacin, 94% to trimethoprim-sulfamethoxazole, and 76% to imipenem. None of the trimethoprim-sulfamethoxazole-resistant isolates carried either plasmid-mediated sulfonamide-resistant genes (sul1, sul2) or trimethoprim-resistant genes (dfrA).
Similar content being viewed by others


Introduction
Nocardia species are ubiquitous environmental organisms that can cause local or disseminated infection in humans. The lung is the most common primary site of infection, and central nervous system infection is often encountered through hematogenous dissemination from a pulmonary focus, particularly in immunocompromised hosts1. Prompt diagnosis and appropriate treatment of nocardiosis are required, because it is a fatal infection2. Trimethoprim-sulfamethoxazole (TMP-SMX) is the first-line agent for initial therapy for nocardiosis3, thus accurate determination of the susceptibility to TMP-SMX in clinical isolates is crucial. Conville et al. reported that the standard broth microdilution method for TMP-SMX may cause false resistance because of difficulties in end-point interpretation, and they recommend performing a confirmation test via sulfisoxazole disk diffusion testing4. Unfortunately we are unable to purchase sulfisoxazole disks in Japan; therefore there is no reliable data concerning Nocardia isolates resistant to TMP-SMX in Japan. On the other hands, identification of clinical isolates to the species/complex level is important, because Nocardia species differ in clinical spectrum and susceptibility patterns5,6,7. Gene sequencing such as 16S rRNA gene is currently used for the identification of Nocardia species; however, recently, matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS)-based identification has been identified as a rapid, easy and reliable method8,9.
The aims of the present study were to profile the antimicrobial susceptibility patterns of a diverse range of Nocardia species isolated from clinical specimens in Japan, and to determine the utility of MALDI-TOF MS for the routine identification of Nocardia species.
Materials and methods
Bacterial isolates and identification
A total of 153 clinical isolates of Nocardia species recovered from patients in 25 microbiology laboratories in Japan were studied. The isolates were cultured from respiratory tract specimens (n = 90), skin and soft tissue (n = 14), blood (n = 5), deep abscess (n = 6), pleural effusion (n = 1), ascitic fluid (n = 1), synovial fluid (n = 1), others (n = 5) and unknown (n = 30). Identification of Nocardia species was based on Gram stain, colonial morphology and molecular technique. All isolates were identified by full-length 16S rRNA gene sequencing, for which the universal primers 8UA (5′-AGAGTTTGATCMTGGCTCAG-3′) and 1485B (5′-ACGGGCGGTGTGTRC-3′) were used, as described previously10. We performed sequencing analysis using a GenBank BLAST search and EzBioCloud (https://www.ezbiocloud.net/identify/result?id=5ef99cb3c39ad461094e9aa3). Previously established criteria for identification of Nocardia isolates to the species or complex level were followed11,12.
MALDI-TOF MS identification
All Nocardia species isolates were analyzed using a Microflex LT bench top mass spectrometer (Bruker Daltonics, Germany). MALDI Biotyper 3.1 software (Bruker Daltonics, MALDI Biotyper reference library version 8.0.0.0) was applied with the use of a supplemental Nocardia library (JMLD library ver.ML01, containing 114 Main Spectras for 46 Nocardia species) provided by BCKK MALDINOMICS (Beckman Coulter Japan, Tokyo, Japan). The isolates were cultivated on 5% sheep blood agar plates at 35℃, and tested at 18 and 48 h, an early stage of growth8. Samples were prepared as previously described (on-plate extraction)8. Protein extraction was also performed using the formic acid/ethanol method according to the Bruker Daltonics’ protocol for any isolate failed to be identified by on-plate extraction. A spectral score of ≥ 2.00 was considered identification to the species level, a score of 1.700–1.999 indicated identification at the genus level, and a score of < 1.70 was considered unreliable identification.
Complex level identification was performed on some Nocardia species according to Conville’s criteria11.
Nocardia asteroides ATCC 23206, Nocardia brasiliensis ATCC 23238, Nocardia farcinica ATCC 23157, and Nocardia otitidiscaviarum ATCC 23240 were used as the quality control strains.
Antimicrobial susceptibility testing (AST)
AST was performed using the broth microdilution method with frozen panels (Eiken Chemical, Tokyo, Japan), according to the Clinical and Laboratory Standards Institute (CLSI) M24-A2 guidelines13 against 146 clinical isolates. In brief, a heavy organism suspension was prepared in a small volume of sterile saline with 7–10 3-mm glass beads and was vortexed vigorously. Clumps were allowed to settle for 15 min, and the supernatant was adjusted to a 0.5 McFarland standard using a calibrated nephelometer. For frozen panel inoculation, the adjusted 0.5 McFarland suspension was diluted 30-fold with sterile saline and 10 µl of the diluted solution was dispensed into each well of the panel. The panels were incubated at 35℃ for 72 h until moderate growth was observed in the growth control wells. For TMP-SMX, the MICs were determined as the wells corresponding to 80% inhibition of growth compared to the controls. The MICs were determined for TMP-SMX, amikacin, tobramycin, ceftriaxone, imipenem, minocycline, linezolid, ciprofloxacin, moxifloxacin, clarithromycin, cefotaxime (100 isolates only), meropenem (100 isolates only), tigecycline (100 isolates only), and arbekacin (100 isolates only), and interpreted as recommended by CLSI. Staphylococcus aureus ATCC 29213, Pseudomonas aeruginosa ATCC 27853 and Enterococcus faecalis ATCC 29212 were used as the quality control strains.
For confirmation of TMP-SMX resistance, disk diffusion testing with a 250-μg sulfisoxazole disk (Hardy Diagnostics, CA, USA)4 was performed in all 21 TMP-SMX-resistant isolates determined by AST (MIC ≥ 4/76 μg/ml). Moreovere, re-analysis of the broth microdilution method using panels with different lots and inoculum colony count were also performed. For this analysis, Nocardia nova ATCC BAA-2227 and Escherichia coli ATCC 25922 were used as the quality control strains.
Detection of plasmid-mediated TMP-SMX-resistant genes
The plasmid-mediated sulfonamide-resistant genes (sul1, sul2)14 and trimethoprim-resistant gene (dfrA)15 were detected by PCR in 21 TMP-SMX-resistant isolates, determined by AST (MIC ≥ 4/76 μg/ml) (see Table S1 for the primer sequence and Figure S1 for a gel electrophoresis image of positive controls in the supplemental material).
The present study was conducted in accordance with the ethical guidelines of the Ministry of Health, Labor and Welfare of Japan. No ethical committee approvals or informed consent were needed for this study.
Conference presentation
A part of this study was presented at the 27th European Congress of Clinical Microbiology and Infectious Diseases, 22 to 25 April 2017, Vienna, Austria [abstr. #316].
Results
Identification of clinical isolates by full-length 16S rRNA gene sequencing
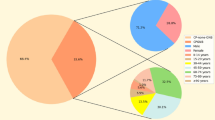
Among the 153 clinical isolates, 150 were identified to the species/complex level, including 24 different species/complexes, and the remaining three isolates were identified to the genus level (Table 1). Nocardia farcinica complex (n = 39; 25%) was the most common species, followed by Nocardia cyriacigeorgica (n = 27; 18%), Nocardia brasiliensis (n = 14; 9%), Nocardia nova (n = 12; 8%), Nocardia otitidiscaviarum (n = 11; 7%), Nocardia elegans (n = 10; 7%), Nocardia beijingensis (n = 7; 5%), N. nova complex (n = 4), Nocardia abscessus (n = 4), Nocardia asiatica (n = 4), Nocardia wallacei (n = 3), Nocardia sp. (n = 3), Nocardia transvalensis complex (n = 3), N. abscessus complex (n = 2), Nocardia thailandica (n = 2), and one each of Nocardia aobensis, Nocardia arthritidis, Nocardia asteroides, Nocardia takedensis, Nocardia pseudobrasiliensis, Nocardia yamanashiensis, Nocardia mexicana, and Nocardia vinacea.
N. cyriacigeorgica was the most frequently isolated Nocardia species from the respiratory tract (28%; 25/90), followed by N. farcinica complex (21%; 19/90). N. brasiliensis was isolated in one-half (50%; 7/14) of the skin and soft tissue samples. Figure 1 shows the alignment of 1405 bases of the 16SrRNA gene of all clinical isolates of Nocardia with those of closely related species obtained using the neighbor-joining method16,17 with MEGA X software18.

16S rRNA sequence-based phylogenetic tree of clinical isolates of Nocardia with those of closely related species. The evolutionary history was inferred using the Neighbor-Joining method16. The optimal tree is shown. The tree is drawn to scale, with branch lengths in the same units as those of the evolutionary distances used to infer the phylogenetic tree. The evolutionary distances were computed using the Maximum Composite Likelihood method17 and are in the units of the number of base substitutions per site. The proportion of sites where at least 1 unambiguous base is present in at least 1 sequence for each descendent clade is shown next to each internal node in the tree. This analysis involved 59 nucleotide sequences. Codon positions included were 1st + 2nd + 3rd + Noncoding. All ambiguous positions were removed for each sequence pair (pairwise deletion option). There were a total of 1405 positions in the final dataset. Evolutionary analyses were conducted in MEGA X18. a The read length of N75 strain was 1023 bp with a good quality sequence.
MALDI-TOF MS identification
Among the 150 isolates that had identified to the species/complex level by 16S rRNA gene sequencing, MALDI-TOF MS correctly identified 97.3% (146/150) to the species/complex level and 1.3% (2/150) to the genus level (Table 1). One isolate, which was identified as N. transvalensis complex by 16S rRNA gene sequencing, was misidentified as N. brasiliensis, with a score ≥ 2.00. In addition, there was one isolate that could not be identified, with a score of < 1.70. All three isolates identified to the genus level by 16S rRNA gene sequencing were identified as Nocardia testacea, with scores of ≥ 2.00.
Antimicrobial susceptibility testing
The MIC range, MIC50, MIC90 and susceptibility for the seven most frequently isolated Nocardia species/complexes are shown in Table 2. The antibiograms of the uncommon Nocardia species are listed in Table 3.
Overall, linezolid was the most active drug across all species, with no in vitro resistance. Among the 146 Nocardia isolates that underwent AST, 96% were susceptible to amikacin; 86% were susceptible to TMP-SMX; and 76% were susceptible to imipenem. In contrast, about 80% of the Nocardia isolates were not susceptible to clarithromycin, minocycline or ciprofloxacin. Six amikacin-resistant isolates were N. transvalensis complex. The results of disk diffusion testing with a 250-μg sulfisoxazole disk and re-analysis of the broth microdilution method against 21 TMP-SMX-resistant isolates are shown in Table 4. Of these 21 isolates, five were interpreted as being TMP-SMX-resistant, and 12 were susceptible, while four were not interpretable. Finally, 94% (137/146) of the Nocardia isolates were determined to be susceptible to TMP-SMX. The isolates that were not susceptible to TMP-SMX (including isolates not interpretable) were found among N. otitidiscaviarum (27%; 3/11), N. farcinica complex (8%; 3/37), N. cyriacigeorgica (4%; 1/27), N. thailandica (1/2) and N. mexicana (1/1).
Susceptibility varied according to Nocardia species. Among the frequently isolated species, nonsusceptibility to imipenem was high in N. otitidiscaviarum (100%) and N. brasiliensis (86%), while that was low in N. nova complex (0%), N. cyriacigeorgica (4%) and N. farcinica complex (5%). More than 80% susceptibility to ceftriaxone was shown in N. abscessus complex (89%), N. cyriacigeorgica (85%) and N. transvalensis complex (83%). N. nova complex showed a good susceptibility to clarithromycin, although its resistance rate in other frequently isolated species was high. Susceptibility to fluoroquinolones including moxifloxacin was low among all the Nocardia species except N. transvalensis complex and N. brasiliensis.
For the 100 Nocardia isolates, the MIC50 and MIC90 values of tigecycline were 8 and > 16 μg/ml, respectively. These values for N. brasiliensis and N. otitidiscaviarum, 1 and 2 μg/ml, respectively, were lower than those for the other frequently isolated Nocardia species. The MIC50 and MIC90 values of minocycline for those 100 Nocardia isolates were 4 and 4 μg/ml, respectively.
The cumulative percentages of the 100 Nocardia isolates inhibited by each concentration of arbekacin, amikacin and tobramycin are shown in Fig. 2. The MIC50 and MIC90 values of arbekacin, amikacin and tobramycin were 0.25 and 1, 1 and 4, and 4 and 128 μg/ml, respectively. Arbekacin showed low MIC values (4–16 μg/ml) even against N. transvalensis complex, which included high-level amikacin-resistant isolates (> 256 μg/ml).

MIC distributions of arbekacin, amikacin and tobramycin against 100 Nocardia isolates.
Detection of plasmid-mediated TMP-SMX-resistant genes
None of the five TMP-SMX-resistant isolates or the remaining 16 isolates (TMP-SMX ≥ 4/76 μg/ml) carried either plasmid-mediated sulfonamide-resistant genes (sul1, sul2) or trimethoprim-resistant gene (dfrA).
Discussion
There is limited information about the distribution and antimicrobial susceptibility of various Nocardia species in Japan. In the present study, N. farcinica complex (25%) was the most common species, followed by N. cyriacigeorgica (18%), N. brasiliensis (9%), N. nova (8%), and N. otitidiscaviarum (7%), according to full-length 16S rRNA gene sequence identification. When using the complex criteria for MALDI-TOF MS identification11, N. farcinica complex (25%) remained the most predominant, but the next most dominant species were N. cyriacigeorgica and N. nova complex (18.3% each), followed by the N. abscessus complex (12%), and N. brasiliensis (9%). These epidemiological data, taken together with the antimicrobial susceptibility profiles of different species/complexes, may contribute to accurate empirical treatment decisions.
The current study demonstrates that MALDI-TOF MS is useful for rapidly and accurately providing species/complex identification of Nocardia species. The direct spotting and standard bacterial extraction methods developed for MALDI-TOF MS are suboptimal for Nocardia species, due to the hardness and composition of the cell wall7. Previous studies have stressed the need for enhanced sample preparation methods to sufficiently identify Nocardia species9,19,20,21. Khot et al. reported that the age of Nocardia cultures plays an important role in the success of MALDI-TOF MS identification, and recommended to use a colony at an early stage of growth8. Their method correctly identified 82.8% (72/87) to the species/complex level and 11.5% (10/87) to the genus level if the cut-off for species-level identification was lowered from a score of ≥ 2.00 to ≥ 1.90. The results of the current study indicate that our method is more reliable than Khot’s method, despite the strict threshold value for species-level identification being used. The point of the method used in the present study was to use a colony at an early stage of growth (18–48 h cultivation), and to use a considerably augmented reference spectrum database created with well-characterized strains cultured in the same condition (18–48 h cultivation).
Our results indicate that TMP-SMX still has a good activity against Nocardia species isolated in Japan. TMP-SMX-resistant isolates were found among N. otitidiscaviarum, N. cyriacigeorgica and N. mexicana. The mechanism of resistance to TMP-SMX is being studied mainly in clinically important bacteria such as Escherichia coli and Salmonella species. It has been reported that acquisition of plasmid-mediated resistance genes (sul and dfr) and chromosomal gene mutations in the dhps and dhfr genes coding for the target enzymes dihydropteroate synthase (DHPS) and dihydrofolate reductase (DHFR), respectively, is the major resistance mechanisms22,23,24 in such bacteria. To the best of our knowledge, the mechanism of TMP-SMX resistance in Nocardia species has not yet been clarified, although a recent study reported that the acquisition of plasmid-mediated resistance genes is involved in high resistance as in general bacteria. Valdezate et al. investigated 76 high-level TMP-SMX-resistant Nocardia isolates (≥ 32/608 μg/ml) isolated in Spain between 2007 and 2013, and found that these isolates possessed either one or multiple plasmid-mediated sulfonamide- and/or trimethoprim-resistant genes (sul1, 93.4%; sul2, 78.9%; and dfrA, 14.7%)25. In the present study, we could not find such a strain in the five TMP-SMX-resistant isolates. The MICs of these TMP-SMX-resistant isolates ranged from 4/76 to 8/152 μg/ml, and there were no high-level TMP-SMX-resistant Nocardia isolates. These results suggest that low level resistance around the MIC breakpoints may occur with different resistant mechanisms. Mehta et al. conducted an in vitro experimental evolution study to adapt susceptible clinical isolates of N. cyriacigeorgica and N. nova to the treatment of choice, TMP-SMX. They found that chromosomal gene mutations were seen within genes encoding DHFR, DHPS and a homolog (folp2) of the gene encoding DHPS in experimental de novo resistant strains26. While their study did not include sequence data of clinically TMP-SMX-resistant Nocardia strains, they suggested that chromosomal gene mutations may be implicated in low-level TMP-SMX resistance identical to that of other bacterial species, such as E. coli27.
On the other hand, it is known that TMP-SMX therapy is strongly associated with the emergence of thymidine-dependent small colony variants (SCVs) in Staphylococcus species28. Underlying mutations have been identified for thymidine-dependent SCVs in S. aureus, and mutations of the thyA gene have been shown to be responsible for the SCV phenotype29. The SCVs have also been found in some clinically important bacteria such as Stenotrophomonas maltophilia, P. aeruginosa, E. coli, Salmonella species, and Enterococcus species30,31. The SCV phenotype is characterized by small colony size, slow growth on agar media compared to wild-type isolates, and the inability to generate in vitro susceptibility results under standard conditions, as defined by CLSI30. Unfortunately, to date there have been no reports on SCVs in Nocardia species. Mehta et al. reported that a point mutation was observed at 16 bp upstream of thyA, which is an operon with the DHFR gene (folA), in experimental de novo TMP-SMX-resistant Nocardia strains, although they did not investigate the relationship between the mutation and SCV phenotype26. Nocardia infections are not uncommon in immunosuppressed patients receiving TMP-SMX for prophylaxis1,32; therefore, the existence of SCVs in Nocardia species cannot be denied. Further, TMP-SMX is frequently used not only for prophylaxis, but also for long-term treatment over 6 months1, so it is necessary to elucidate the resistance mechanisms, including chromosomal gene mutations and SCVs, and to develop an accurate detection method for TMP-SMX-resistant strains.
Tigecycline is the first in a new class of antimicrobials, a member of the glycylcyclines, and is an analogue of minocycline with additional properties that negate most mechanisms, mediating resistance to tetracyclines33. In vitro testing has revealed that tigecycline is active against Gram-positive cocci, including Enterococcus species, S. aureus and Streptococcus pneumoniae, and many species of multi-drug-resistant Gram-negative bacteria33. Lai et al. investigated 151 clinical isolates of Nocardia species, and reported that tigecycline had a low MIC90 (1 μg/ml), and that MIC values were ≤ 8 μg/ml against all of the tested isolates, suggesting the potential clinical application of tigecycline for the treatment of nocardiosis34. In the present study, tigecycline had a low MIC distribution only for N. brasiliensis, N. otitidiscaviarum and some clinically unusual Nocardia species. Some researchers have reported that N. farcinica complex, N. nova complex and N. transvalensis complex isolates were less susceptible to tigecycline than N. abscessus, N. brasiliensis, or N. otitidiscaviarum35,36. Further studies are needed to demonstrate the clinical role of tigecycline in the management of nocardiosis.
To our knowledge, the present study is the first to have evaluated the activity of arbekacin against a diverse range of Nocardia species. Arbekacin is a broad-spectrum aminoglycoside licensed for systemic use in Japan and Korea, where it is usually used to treat methicillin-resistant S. aureus infections37,38,39. Matsumoto et al. reported that arbekacin is stable against aminoglycoside-inactivating enzymes such as (3′) aminoglycoside-phosphotransferase, (4′) aminoglycoside-adenyltransferase (AAD), or AAD (2″) and has a weak affinity for (6′-IV) aminoglycoside-acetyltransferase40,41. Therefore, arbekacin has antimicrobial activity against Gram-positive and -negative pathogens, including strains resistant to gentamicin, tobramycin, and amikacin40,42. In this study, arbekacin was four-fold more active than amikacin, and showed low MIC values even against N. transvalensis complex, which is reported to be resistant to all aminoglycosides43. These results indicate that arbekacin has a good potential to be a concomitant antibiotic for empirical therapy or therapy for serious nocardiosis infections.
In conclusion, the current study demonstrated that MALDI-TOF MS is a quick, easy and reliable method for the species/complex identification of Nocardia species. Accurate identification by MALDI-TOF MS and antimicrobial susceptibility profiles together can help earlier implementation of appropriate antimicrobial treatment and improvement of patient prognosis.
References
Wilson, J. W. Nocardiosis; Updates and clinical overview. Mayo Clin. Proc. 87, 403–407 (2012).
Hemmerabach-Miller, M., Stout, J. E., Woodworth, M. H., Cox, G. M. & Saullo, J. L. Nocardia infections in the transplanted host. Transpl. Infect. Dis. 20, e12902 (2018).
Margalit, I. et al. How do I manage nocardiosis?. Clin. Microbiol. Infect. 27, 550–558 (2021).
Conville, P. S. et al. Multisite reproducibility of the broth microdilution method for susceptibility testing of Nocardia species. J. Clin. Microbiol. 50, 1270–1280 (2012).
Brown-Elliott, B. A., Brown, J. M., Conville, P. S. & Wallace, R. J. Jr. Clinical and laboratory features of the Nocardia spp. based on current molecular taxonomy. Clin. Microbiol. Rev. 19, 259–282 (2006).
Conville, P. S., Brown-Elliott, B. A. & Witebsky, F. G. Nocardia, Rhodococcus, Gordonia, Actinomadura, Streptomyces, and other aerobic actinomycetes. In Mannual of clinical microbiology (eds Carroll, K. C. et al.) 525–557 (American Society for Microbiology, 2019).
Blosser, S. J. et al. Multicenter matrix-assisted laser desorption ionization-time of flight mass spectrometry study for identification of clinically relevant Nocardia spp. J. Clin. Microbiol. 54, 1251–1258 (2016).
Khot, P. D., Bird, B. A., Durrant, R. J. & Fisher, M. A. Identification of Nocardia species by matrix-assisted laser desorption ionization-time of flight mass spectrometry. J. Clin. Microbiol. 53, 3366–3369 (2015).
Segawa, S. et al. Identification of Nocardia species using matrix-assisted laser desorption/ionization-time-of-flight mass spectrometry. Clin. Proteomics. 12, 6 (2015).
Nakamura, I., Omori, N., Umeda, A., Ohkusu, K. & Matsumoto, T. First case report of fatal sepsis due to Campylobacter upsaliensis. J. Clin. Microbiol. 53, 713–715 (2015).
Conville, P. S., Brown-Elliott, B. A., Smith, T. & Zelazny, A. M. The complexities of Nocardia taxonomy and identification. J. Clin. Microbiol. 56, 1–10 (2018).
Clinical and Laboratory Standards Institute. Interpretive criteria for identification of bacteria and fungi by DNA target sequencing; approved guideline. In Clinical and Laboratory Standards Institute document MM18-A (Clinical and Laboratory Standards Institute, 2008)
Clinical and Laboratory Standards Institute. Susceptibility testing of mycobacteria, nocardiae, and other aerobic actinomycetes; approved standard, 2nd ed. In Clinical and Laboratory Standards Institute document M24-A2 (Clinical and Laboratory Standards Institute, 2011)
Kozak, G. K., Boerlin, P., Janecko, N., Reid-Smith, R. J. & Jardine, C. Antimicrobial resistance in Escherichia coli isolates from swine and wild small mammals in the proximity of swine farms and in natural environments in Ontario, Canada. Appl. Environ. Microbiol. 75, 559–566 (2009).
Argudin, M. A. et al. Virulence and resistance determinants of German Staphylococcus aureus ST398 isolates from nonhuman sources. Appl. Environ. Microbiol. 77, 3052–3060 (2011).
Saitou, N. & Nei, M. The neighbor-joining method: A new method for reconstructing phylogenetic trees. Mol. Biol. Evol. 4, 406–425 (1987).
Tamura, K., Nei, M. & Kumar, S. Prospects for inferring very large phylogenies by using the neighbor-joining method. Proceedings of the National Academy of Sciences (USA) 101, 11030–11035 (2004).
Kumar, S., Stecher, G., Li, M., Knyaz, C. & Tamura, K. MEGA X: Molecular evolutionary genetics analysis across computing platforms. Mol. Biol. Evol. 35, 1547–1549 (2018).
Hsueh, P. R. et al. Bruker Biotyper matrix-assisted laser desorption ionization-time of flight mass spectrometry system for identification of Nocardia, Rhodococcus, Kocuria, Gordonia, Tsukamurella, and Listeria species. J. Clin. Microbiol. 52, 2371–2379 (2014).
Verroken, A. et al. Evaluation of matrix-assisted laser desorption ionization-time of flight mass spectrometry for identification of Nocardia species. J. Clin. Microbiol. 48, 4015–4021 (2010).
Toyokawa, M. et al. Reliable and reproducible method for rapid identification of Nocardia species by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. Rinsho Biseibutshu Jinsoku Shindan Kenkyukai Shi 24, 1–8 (2013).
Huovinen, P., Sundstrőm, L., Swedberg, G. & Skőld, O. Trimethoprim and sulfonamide resistance. Antimicrob. Agents Chemother. 39, 279–289 (1995).
Perreten, V. & Boerlin, P. A new sulfonamide resistance gene (sul3) in Escherichia coli is widespread in the pig population of Switzerland. Antimicrob. Agents Chemother. 47, 1169–1172 (2003).
Antunes, P., Machado, J., Sousa, J. C. & Peixe, L. Dissemination of sulfonamide resistance genes (sul1, sul2, and sul3) in Portuguese Salmonella enterica strains and relation with integrons. Antimicrob. Agents Chemother. 49, 836–839 (2005).
Valdezate, S. et al. Resistance gene pool to co-trimoxazole in non-susceptible Nocardia strains. Front. Microbiol. 6, 376 (2015).
Mehta, H. et al. Pathogenic Nocardia cyriacigeorgica and Nocardia nova evolve to resist trimethoprim-sulfamethoxazole by both expected and unexpected pathways. Antimocrob. Agents Chemother. 62, e00364-e418 (2018).
Mehta, H. H. & Shamoo, Y. Pathogenic Nocardia: A diverse genus of emerging pathogens or just poorly recognized?. PLoS Pathog. 16, e1008280 (2020).
Kahl, B. C., Becker, K. & Lőffler, B. Clinical significance and pathogenesis of Staphylococcal small colony variants in persistent infections. Clin. Microbiol. Rev. 29, 401–427 (2016).
Chatterjee, I. et al. In vitro mutations of thymidylate synthase (encoded by thyA) are responsible for thymidine dependency in clinical small-colony variants of Staphylococcus aureus. J. Bacteriol. 190, 834–842 (2008).
Anderson, S. W., Stapp, J. R., Burns, J. L. & Qin, X. Characterization of small-colony variant Stenotrophomonas maltophilia isolated from the sputum specimens of five patients with cystic fibrosis. J. Clin. Microbiol. 45, 529–535 (2007).
Johnes, B. E., Purdy, K. J., Tucker, N. P. & Maddocks, S. E. Phenotypic and genotypic characteristics of small colony variants and their role in chronic infection. Microbiol. Insight 8, 15–23 (2015).
Coussement, J. et al. Nocardia infection in solid organ transplant recipients: a multicenter European case-control study. Clin. Infect. Dis. 63, 338–345 (2016).
Pankey, G. A. Tigecycline. J. Antimicrob. Chemother. 56, 470–480 (2005).
Lai, C. C. et al. Multicenter study in Taiwan of the in vitro activities of nemonoxacin, tigectcline, doripenem, and other antimicrobial agents against clinical isolates of various Nocardia species. Antimicrob. Agents Chemother. 55, 2081–2091 (2011).
Schlaberg, R., Fisher, M. A. & Hanson, K. E. Susceptibility profiles of Nocardia isolates based on current taxonomy. Antimicrob. Agents Chemother. 58, 795–800 (2014).
Lebeaux, D. et al. Antibiotic susceptibility testing and species identification of Nocardia isolates: a retrospective analysis of data from a French expert laboratory, 2010–2015. Clin. Microbiol. Infect. 25, 489–495 (2019).
Watanabe, T. et al. Antibacterial activities of arbekacin, a new aminoglycoside antibiotic, against methicillin-cephem-resistant Staphylococcus aureus. Jpn. J. Antibiot. 40, 349–356 (1987) (in Japanese).
Matsumoto, T. et al. Clinical efficacy and safety of arbekacin sulfate in patients with MRSA sepsis or pneumonia: A multi-institutional study. J. Infect. Chemother. 19, 128–137 (2013).
Hwang, J. H. et al. The efficacy and safety of arbekacin and vancomycin for the treatment in skin and tissue MRSA infection: preliminary study. Infect. Chemother. 45, 62–68 (2013).
Matsumoto, T. Arbekacin: another novel agent for treating infections due to methicillin-resistant Staphylococcus aureus and multidrug-resistant Gram-negative pathogens. Clin. Pharmacol. 6, 139–148 (2014).
Matsumoto, T. & Yamamoto, H. The enzymatic mechanisms of resistant to aminoglycoside antibiotics in methicillin-cephem-resistant Staphylococcus aureus. Jpn. J. Antibiot. 41, 523–529 (1988) ( in Japanese).
Sader, H. S., Rhomberg, P. R., Farrell, D. J. & Jones, R. N. Arbekacin activity against contemporary clinical bacteria isolated from patients hospitalized with pneumonia. Antimicrob. Agents Chemother. 59, 3263–3270 (2015).
Conville, P. S., Brown, J. M., Steigerwalt, A. G., Brown-Elliott, B. A. & Witebsky, F. G. Nocardia wallacei sp. Nov. and Nocardia blacklockiae sp. Nov., human pathogens and members of the “Nocardia transvalensis complex”. J. Clin. Microbiol. 46, 1178–1184 (2008).
Acknowledgements
The authors thank microbiology laboratories, which provided the clinical isolates.
Funding
This work was supported by grants from the Kurozumi Medical Foundation and Charitable Trust Laboratory Medicine Research Foundation of Japan.
Author information
Authors and Affiliations
Contributions
M.T., N.O. and A.U. designed research; M.T., D.T., K.O. and K.S. conducted review and editing; M.T., M.I., D.T., M.H., Y.T. and H.S. provided the laboratory tests, data analysis, and resources; and M.T. and K.S. wrote the paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Toyokawa, M., Ohana, N., Ueda, A. et al. Identification and antimicrobial susceptibility profiles of Nocardia species clinically isolated in Japan. Sci Rep 11, 16742 (2021). https://doi.org/10.1038/s41598-021-95870-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-95870-2
- Springer Nature Limited
This article is cited by
-
Clinical characteristics and drug resistance of Nocardia in Henan, China, 2017–2023
Annals of Clinical Microbiology and Antimicrobials (2024)
-
In vitro activity of tedizolid against 43 species of Nocardia species
Scientific Reports (2024)
-
A multi-centre retrospective study of Nocardia speciation and antimicrobial susceptibility in Queensland, Australia
European Journal of Clinical Microbiology & Infectious Diseases (2023)
-
MLSA phylogeny and antimicrobial susceptibility of clinical Nocardia isolates: a multicenter retrospective study in China
BMC Microbiology (2021)