
Abstract
The term “geriatric giants” refers to the chronic disabilities of senescence leading to adverse health outcomes. This study aimed to investigate the prevalence and predictors of geriatric giants in Southern Iran. The participants were selected from Bushehr city using a multistage cluster random sampling method. Demographic data were collected through interviews. Frailty, incontinence, immobility, depression, cognitive impairment, and malnutrition were measured by questionnaires and instruments. Finally, data from 2392 participants were analyzed. The prevalence of fecal incontinence was less than 1% among all participants and similar in men and women. In contrast, compared with men, women had higher prevalence of urinary incontinence (36.44% vs. 17.65%), depression (39.05% vs. 12.89%), anorexia and malnutrition (2.35% vs. 0.82%), immobility (8.00% vs. 2.5%), frailty (16.84 vs. 7.34), and pre-frailty (54.19 vs. 38.63%). The prevalence of dependence and cognitive impairment was also higher in women and considerably increased with the age of participants. In total, 12.07% of subjects were frail, and 46.76% were pre-frail. The prevalence of frailty exponentially increased in older age, ranging from 4.18% among those aged 60–64 years to 57.35% in those aged ≥ 80 years. Considering 95% confidence interval (CI), multivariate logistic regression revealed that low physical activity [odds ratio (OR) 31.73 (18.44–54.60)], cancer (OR 3.28 (1.27–8.44)), depression [OR 2.42 (1.97–2.98)], age [OR 1.11 (1.08–1.14)], waist circumference [OR 1.03 (1.01–1.06)], BMI [OR 1.07 (1.01–1.14)], MNA score [OR 0.85 (0.79–0.92)], polypharmacy [OR 2.26 (1.30–3.95)] and male gender [OR 0.63 (0.42–0.93)] were independently associated with frailty. White blood cell count (WBC), smoking, marital status, and number of comorbidities were not independently associated with frailty. Low physical activity was the strongest predictor of frailty, which may need more attention in geriatric care. Frailty, its predictors, and other components of geriatric giants were considerably more common among women and older ages.
Similar content being viewed by others


Introduction
Life expectancy has markedly increased over the past decades mainly due to reduced mortality during early and middle life in the first half of the twentieth century and improved survival after 65 years of age in the second half of the twentieth century1,2. The prevalence of major chronic diseases generally increases with age and aging is accompanied by higher odds of several health conditions, particularly geriatric giants3,4. In 1965, Bernard Isaacs defined geriatric giants as “immobility, instability, incontinence, and impaired intellect/memory”. The definition was then modified by experts in the field. Different components of geriatric giants can interact with each other and one component can contribute to the incidence of the other known as the geriatric cascade, which propels old subjects from robustness to disability5. As they are assumed the natural consequence of senescence by patients, their caregivers, and even physicians, the giants of geriatrics often do not receive enough attention until they impose a significant burden on patients and the healthcare system5,6. Although there is not a unanimous definition, we considered frailty, immobility, instability, incontinence, cognitive impairment, anorexia, functional status, depression, and polypharmacy as geriatric giants in this study.
A recent report from Turkey with 2816 participants indicated that the prevalence of polypharmacy, urinary incontinence, depression, dementia, falls, sarcopenia, frailty, and malnutrition was as high as 54.5%, 47.6%, 35.1%, 21.6%, 33.6%, 31.7%, 28.3%, and 9.6%, respectively7. Another study from Turkey indicated that 90.3% of patients with Lewy body dementia and 54.9% of patients with Alzheimer's disease had ≥ 3 components of geriatric giants, reminding the effect of one component on the presence of other components8. Moreover, the presence of a pre-existing condition such as anemia was shown to increase the odds of geriatric giants9.
Frailty is the result of deficit accumulation in several body systems, which itself increases vulnerability to external stressors10. Not all old patients, but many of them, particularly those visiting health centers, experience frailty. Based on the definition of frailty and the characteristics of the target population, the prevalence of frailty and pre-frailty in most studies widely varies across different studies mainly from 5.9 to 17.4% and from 26.8 to 62.8%, respectively11. However, a study from the north of Iran with 2010 participants reported that the prevalence of frailty and pre-frailty was 33.4% and 43.5%, respectively12. In addition, a meta-analysis of 9 studies from the Middle East reported that the prevalence of pre-frailty and frailty was as high as 39% and 35%, respectively13. A study from France has estimated that pre-frailty and frailty caused 750 € and a 1500 € increment in ambulatory health expenditures for each individual just in 201214. Clinical identification of frailty is necessary for promoting the adaptation of health care services to the needs. Recently, the prevalence of frailty has become a major index for evaluating the health status of the elderly population. On the other hand, healthcare policies have been modified to allocate more resources for preventing frailty or educating and rehabilitating those with frailty15,16. Herein, an interdisciplinary effort has been made in recent years to recognize frailty as a medical condition that needs early screening, advanced knowledge, and sufficient management10,16.
Having a thorough knowledge of the extent of the problem and its predictors is the main prerequisite for policy-making. Herein, in this community-based study, we measured the prevalence of geriatric giants and frailty in Southern Iran and simultaneously identified the associated factors. Identification of the prevalence of geriatric giants and frailty in Iran can better reflect the current status of geriatric health in this region. Particularly, a deeper insight into the associated factors of geriatric giants and frailty may help design better preventive and screening plans to promote geriatric health. Using a multistage cluster random sampling method, we included participants from the second wave of the Bushehr Elderly Health Program (BEHP)17.
Results
Data were obtained from 2392 participants. Among them, 51.37% were female. The mean age of the participants was 70.13 years. The prevalence of obesity was 23.39% (95% CI 23.70–27.16) (Table 1).
The WHO age-standardized prevalence of frailty was 12.07% (95% CI 10.89–13.36%) and the prevalence of pre-frailty was 46.76% (95% CI 44.72–48.81%) based on Fried frailty phenotype. The WHO age-standardized prevalence of frailty was 14.20% (95% CI 12.83–15.70%) and the prevalence of pre-frailty was 64.75% (95% CI 62.76–66.69%) based on frailty index. The prevalence of frailty increased with age. For instance, based on Fried frailty phenotype, the prevalence of frailty was 4.18% among those with 60–64 years of age and reached 57.35% among those ≥ 85 years of age. Based on frailty index, the prevalence of frailty was 7.59% among those with 60–64 years of age and reached 55.17% among those ≥ 85 years of age. Furthermore, the prevalence of frailty in females was more than twice of that in males based on the Fried frailty phenotype (16.84% vs. 7.34%, respectively) (Table 2). The prevalence of frailty in females was more than three times of that in males based on the frailty index (21.09% vs. 6.88%, respectively). The prevalence of frailty and pre-frailty in different age and sex groups based on frailty index has been summarized in Supp Table 1. The most common characteristic of all frail participants was low walking speed (34.16%), and the least common feature was weight loss (6.15%) (Supp Table 2).
Using the χ2 test, we measured the effect of monthly income or wealth quantile on frailty. Our data showed that monthly income and wealth quantile could not significantly change the prevalence of frailty (Table 3). After adjusting for several factors, multivariate logistic regression revealed that low physical activity [OR 31.73 (18.44–54.60)], cancer [OR 3.28 (1.27–8.44)], depression [OR 2.42 (1.97–2.98)], age [OR 1.11 (1.08–1.14)], waist circumference [OR 1.03 (1.01–1.06)], BMI [OR 1.07 (1.01–1.14)], MNA score [OR 0.85 (0.79–0.92)], polypharmacy [OR 2.26 (1.30–3.95)] and male gender [OR 0.63 (0.42–0.93)] were independently associated with frailty. WBC, smoking, marital status, and number of comorbidities were not independently associated with frailty (Table 4).
Only 70.99% (95% CI 69.18–72.24%) of participants were independent based on Katz activities of daily living (ADL). The independence ratio in Katz ADL was markedly higher in males than in females (81.02% vs. 61.62%). However, dependency in ≥ 4 domains was found in less than 1% of participants (Table 5). Instrumental activities of daily living (IADL) showed a lower prevalence of independence (40.83%, 95% CI 38.87–40.81). The prevalence of dependence increased with the age of participants, and no woman ≥ 85 years old was independent (Supp Table 3).
Among all participants, 27.40% (95% CI 25.68–29.20) had urinary incontinence. The prevalence of urinary incontinence in women was more than twice that in men (36.44% vs. 17.65%). In addition, the prevalence of urinary incontinence among women increased with age from 31% in those with 60–64 years of age to 45% in those ≥ 85 years of age. However, the prevalence of fecal incontinence was less than 1% among all participants, which was similar in both sexes (Supp Table 4).
WHO age-standardized prevalence of immobility was 5.32% in all participants. The prevalence of immobility was three-time higher in women than in men, and it increased with age (Table 6).
WHO age-standardized prevalence of mild depression, moderate depression, and severe depression was 16.48%, 5.61%, and 4.17%, respectively. The prevalence of depression was not statistically significant in males but it was prominent in females. There was a considerable difference between males and females regarding depression. This difference was notable in severe depression and it was several times more prevalent in females than males (Supp Table 5).
As mentioned, the cognitive function was assessed using the Mini-cog tool. WHO age-standardized prevalence of cognitive dysfunction was 53.74% (95% CI 51.70–55.77%) in all participants. The prevalence of cognitive impairment increased with age. Cognitive impairment was more common in females and this difference was more prominent in younger participants than in older participants (Supp Table 4).
Mild malnutrition was assessed using the Mini Nutritional Assessment (MNA). Only 1.62% of subjects had mild malnutrition and this problem was nearly three times more common in females than in males (2.35% vs. 0.82%). There was not a linear relationship between mild malnutrition and age, but the highest prevalence of mild malnutrition was observed in participants ≥ 85 years of age (5.88%) (Supp upp Table 4).
In addition, we measured the co-incidence of 4 components of geriatric giants including frailty, sarcopenia, cognitive impairment, and anorexia. Among all participants in this study, 725 (31.14%) participants had none of these components, 978 (42.01%) participants had one of these components, 482 (20.70%) participants had two of these components, 126 (5.41%) participants had three of these components, and 17 (0.73%) participants had four of these components (Fig. 1). Multinomial logistic regression also indicated that male gender, MNA score, and BMI were negatively associated with the presence or coexistence of frailty, sarcopenia, cognitive impairment, and anorexia of aging, whereas age, waist circumference, and low physical activity were positively associated with the presence or coexistence of frailty, sarcopenia, cognitive impairment, and anorexia of aging. In particular, low physical activity showed the greatest relative risk ratios (RRRs) for the co-existence of geriatric giants. Moreover, cancer, smoking, alcohol consumption, WBC count, marital status, and polypharmacy were not significantly associated with the coexistence of frailty, sarcopenia, cognitive impairment, and anorexia of aging (Table 7).

Venn diagram depicting the coexistence of frailty, sarcopenia, cognitive impairment, and anorexia of aging.
Discussion
In this study, we found that the prevalence of frailty and pre-frailty was 12.07% and 46.76% in Southern Iran, respectively. Frailty, cognitive impairment, dependence, urinary incontinence, immobility, depression, anorexia, and malnutrition were considerably more common in older ages and among women. Low physical activity, cancer, female gender, malnutrition, depression, age, waist circumference, and BMI were positively and independently associated with frailty. Among them, low physical activity was the strongest predictor of frailty in this study.
As mentioned previously, each component of geriatric giants is associated with other components5. For instance, data from 5474 individuals ≥ 70 years of age revealed that urinary incontinence in older age is significantly and positively associated with falls18. Reciprocally, falling was associated with urinary incontinence and physical limitation18. Consistently, we have shown that malnutrition/anorexia, depression, and low physical activity are associated with frailty. Thus, preventing or treating one component of geriatric giants may improve the others.
The Longitudinal Ageing Study in India (LASI) with 31,464 participants reported that among patients aged ≥ 60, late-life depression and cognitive impairment had an overall prevalence of 0.7% and 13.7%, respectively19. Furthermore, late-life depression was 74% and 69% more common among those who had difficulty with ADL and IADL19. Moreover, the study reported that cognitive impairment was more frequent among depressed individuals19. These findings may partly warrant the higher prevalence of cognitive impairment among females in our study. As depression was more common among women in all ranges of age, cognitive impairment followed the same pattern. In particular, the prevalence of cognitive impairment was markedly higher in women aged 60–74 years, compared with men of the same age. In addition to a higher prevalence of depression, low physical activity may lead to a higher prevalence of cognitive impairment among women. A recent study has shown that moderate-intensity physical activity can substantially improve cognitive function and quality of life in those with mild cognitive impairment20.
A systematic review of 23 articles indicated that isolated fecal incontinence was found in 3.5% (interquartile range 2.8%) of older people who resided in care homes21. Besides, cognitive impairment, urinary incontinence, advanced age, limited functional capacity, reduced mobility, and diarrhea were correlated with fecal incontinence in this study21. Fecal incontinence was less common in our study as our participants had better health conditions.
The prevalence of frailty is expected to grow in the aging population22. Frailty is associated with a marked decline in daily functioning and significantly increased susceptibility to stressors, falls, hospitalization, and mortality22. Previous studies have shown that frailty is positively correlated with disability-adjusted life years (DALY); therefore, frail patients constitute a substantial proportion of the global burden of disease23. Although many studies unveiled the indispensable importance of frailty, still there is little progress in its management22,24. In particular, having better knowledge about the risk factors of frailty can help to modify healthcare services and prevent frailty or its complications through early intervention22. With the increase in life expectancy in the coming decades, years spent with frailty will gradually increase, which is anticipated to substantially escalate health care expenses24.
Similar to our findings, a meta-analysis including 81,258 subjects revealed that the pooled prevalence of pre-frailty and frailty were 43% and 10%, respectively11. In addition, the pooled prevalence of frailty was 8% based on the Fried frailty phenotype11. Consistent with our findings, the prevalence of frailty exponentially increased with age in this meta-analysis11. After adjusting for other factors among 484 participants, Gobbens et al.25 reported that medium income, an unhealthy lifestyle, and multimorbidity can predict frailty. They also reported that age was only associated with physical frailty, history of life events was only associated with psychological frailty, and female gender was only associated with social frailty25. A study with 1867 participants aged ≥ 65 years indicated that only age and education were associated with frailty26. A recent study from China with 14,314 participants reported that older age, being a professional or technician before 60 years of age, poor economic condition, and poor oral hygiene are risk factors for frailty, while eating rice as a staple food, regular exercise, having a spouse as the first person to share thoughts with, doing an annual physical examination, and not needing a caregiver during illness are protective factors against frailty27. Furthermore, the meta-analysis of 14 studies uncovered that increasing age, female gender, activities of daily living disability, and having three or more chronic diseases are positively associated with frailty11. We showed that low physical activity, cancer, female gender, malnutrition, depression, age, waist circumference, polypharmacy, and BMI were positively and independently associated with frailty. However, WBC, smoking, and marital status were not independently associated with frailty in this study.
Low physical activity can be both a risk factor and an outcome of frailty28. Frail patients become physically limited and rely on their caregivers and family members for their daily functioning29. Even, it has been observed that frail patients have specific patterns of walking29. On the other hand, physical dependence and the absence of physical activity make individuals frail28. On the contrary, maintaining a minimum level of physical activity, particularly aerobic exercise, may prevent or postpone frailty in older age28. Herein, a study including 780 patients unveiled that age, malnutrition, functional dependence, and severe knee osteoarthritis can enhance the risk of frailty28. Among the risk factors, severe knee osteoarthritis, which utterly restricts physical activity, was associated with an 18-time higher risk of frailty. However, mild and moderate osteoarthritis that allow a sufficient level of physical activity for daily functioning were not associated with frailty28.
A systematic review of 20 studies with 2916 patients revealed that frailty and pre-frailty are frequently observed among cancer patients (median prevalence of 42% and 43%, respectively)30. In addition, frailty predicts higher rates of mortality and treatment-associated complications in cancer patients30.
Senescence is associated with altered biological processes and metabolism, ineffective immune response, and impaired or weak response to stressors, which may interfere with normal homeostasis31,32,33. Consistently, it has been unfolded that abnormal immune response, deregulation of cellular metabolism, and impaired metabolism of macromolecules are involved in the pathogenesis of frailty34. Similar o frailty, aging is accompanied by several chronic diseases and comorbidities resulting in decreased functional reserve35. Thus, a deeper insight into the biology of aging may improve the prevention, screening, and treatment of frailty31.
Similar to our study, previous studies showed that being female can significantly elevate the risk of frailty, which may be due to physiologic differences in metabolism, muscle mass, body composition, mental status, physical strength, and life expectancy36,37. Furthermore, it has been observed that frail women have longer survival than both frail and non-frail men37. Interestingly, by stratifying participants into different groups of BMI, Hubbard et al. unveiled that participants with a BMI of 25–29.9 are at the lowest risk of frailty, but a BMI of higher or lower than this range is associated with a greater risk of frailty38. In particular, those with a BMI of less than 20 were at the greatest risk of frailty38. Likewise, a meta-analysis by Yuan et al. indicated that both being underweight or obese was associated with an increased risk of frailty39. Consistently, our findings indicated that both high BMI and malnutrition are independently associated with frailty.
There are some limitations to this study. First, the prevalence of frailty, pre-frailty, and other components of geriatric giants cannot be applied to other regions, as none of the previous or future studies can do the same because the prevalence is specific to each region and its population. However, the associations found in this study can be validated by other studies in different regions and populations. Second, due to the cross-sectional nature of this study, it cannot support causality and future prospective studies are needed to measure the presence of causality in the observed relationship. Third, large studies with participants from different regions are needed to better reflect the prevalence of geriatric giants in Iran and the Middle East.
With all shortcomings, compared with previous studies12,40,41, this study has some strengths. First, the greater sample size and better sampling method in this study can help better reflect the prevalence of geriatric giants in the study region. Second, most studies from Iran focused on frailty, but this study is the first study that measured different components of geriatric giants in the Iranian population. Third, this study comprehensively assessed the associations between geriatric giants or frailty and different variables, which can provide new ideas for future studies and improve the screening and prevention of frailty.
Conclusion
Our findings showed that the prevalence of frailty and pre-frailty was 12.07% and 46.76% in a sample from the Iranian population. We found that the prevalence of frailty exponentially increases in older ages. Frailty and other giants of geriatrics such as cognitive impairment, dependence, urinary incontinence, immobility, depression, anorexia, and malnutrition were markedly more common in women than in men. Low physical activity, cancer, female gender, malnutrition, depression, age, waist circumference, polypharmacy, and BMI were positively and independently associated with frailty. Among them, low physical activity was the strongest predictor of frailty. Our findings provide a deeper insight into the prevention of frailty and can be useful for the design of future interventional studies.
Methods
Participants
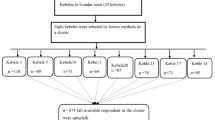
We used data from the second wave of the Bushehr Elderly Health Program (BEHP). Participants were urban residents from Bushehr in the south of Iran. They were included using a multistage cluster random sampling method. The detail of the first and second wave of this study was published elsewhere17. In the first wave, 3000 older adults (age > 60 years) who lived in a community in Bushehr were enrolled. The participants were chosen from 75 separate neighborhoods defined by the local municipality. The number of participants selected from each neighborhood was proportional to the number of households registered in the last census. In the second wave, 2480 subjects from the first wave were enrolled again. They were invited to a health center, and their health status was evaluated. Data on demographic characteristics, lifestyle factors, general health, medical history, and mental and functional status were collected through a questionnaire. Assessment of anthropometric indices, performance-based tests, muscle strength tests, blood pressure evaluation, and body composition measurements were performed. Because of incomplete data, finally, 2392 subjects were included for analysis. The reason for incomplete data was death or insufficient compliance of patients for completing the assessments.
Data collection
The phenotype of frailty was defined according to the Fried phenotype. Unintentional weight loss ≥ 4.5 kg during the past year was asked. Exhaustion was defined as positive answers to two questions of the Center for Epidemiological Studies Depression (CES-D). Slowness was defined based on sex and height. Handgrip strength and physical activity were determined using the lowest quintile of mean handgrip measures after three times of measurements in each hand. Low physical activity was defined as the lowest metabolic equivalent during 1 week based on WHO physical activity questionnaire. The presence of one or two of the aforementioned criteria was defined as pre-frailty and the presence of more than two criteria was defined as frailty42.
Demographic data were also collected during the interview. Anthropometric data such as weight, height, and waist circumference were measured based on NHANCE-3 guidelines. Body mass index (BMI) was calculated by dividing weight (kg) by squared height (meter). Overnight fasting blood samples were collected and fasting blood sugar, Hb A1C, and complete blood count (CBC) were measured using automatic standardized devices. Diabetes mellitus and hypertension were defined according to ADA 2018 and JNC-8 criteria.
Urinary and fecal incontinence was defined as the incidence of any episode of incontinence during the last 6 months. Mobility and instability were evaluated by asking the participants and their partners about their ability to move. In addition, timed up and go test and short physical performance battery (SPPB) scores were assessed43. The incidence and number of falls during the last year were recorded. Anorexia in the past 3 months was evaluated by the Mini Nutritional Assessment (MNA) questionnaire44. Furthermore, information regarding drug history and significant weight loss (≥ 4.5 kg) during the last year was also collected. Taking more than five drugs per day was considered polypharmacy.
Katz ADL instrument was utilized for assessing independence in basic daily activities, including bathing, feeding, urinary and fecal continence, dressing, toileting, and transferring45. Lawton instrumental activity of daily living was used for assessing intermediate daily function. This instrument has eight domains. A score of eight shows independence in all areas and a score of zero shows complete dependence.
Mood was measured using patient health questionnaire 9 (PHQ-9)46. This questionnaire has nine items and each item is a Likert-type question with a score from zero to three. The maximum score is 27 showing the worst mood and zero showing the best mood. The validity and reliability of this tool were approved in the Iranian population47.
Cognitive function was assessed using two instruments; the Mini-Cog score and the category fluency test. Mini-Cog had two stages48. In the first stage, the ability to recall three words was evaluated. Remembering all words was considered normal cognition and recalling none of them was considered impaired cognition. Participants who recalled one or two words, entered the second stage, a clock drawing test. Those who correctly drew the clock were considered cognitively intact; otherwise, the subjects were considered cognitively impaired. Furthermore, the category fluency test was used for naming animals. Subjects were categorized into impaired cognition and normal cognition groups based on the number of years they spent in school. Participants with impaired cognition in at least one test were categorized into the impaired cognition group.
We also measured the frailty index comprising 35 items. These items were needing assistance with bathing, dressing, getting in and out of a chair, walking around the house, eating, grooming, using toilet, going up and down stairs, shopping, housework, meal preparation, taking medication, managing finances, experiencing weight loss of more than 4.5 kg in the last year, walking outside, feeling that everything is an effort, feeling depressed or lonely, having trouble getting going, high blood pressure, heart attack, congestive heart failure, stroke, cancer, diabetes, arthritis, chronic lung disease, chronic kidney disease, gait speed, BMI, grip strength, cognitive impairment (Mini-Cog), seizures, urinary incontinence, and bowel incontinence.
The frailty index did not include peak flow, shoulder strength, and timed normal pace due to the lack of clear cut-points in the original article49.
Recorded procedures were used to transform categorical, ordinal, and interval variables into a common scale ranging from 0 to 1. In this mapping, 0 represents the absence of a deficit, while 1 represents the full presence of the deficit. Individual deficit scores were combined to create an index, where a score of 0 indicated the absence of deficits and a score of 1 indicated the presence of all 40 deficits49. Although we report the prevalence of frailty based on two measures, frailty index and Fried frailty phenotype, the latter was used for constructing regression models and interpreting the associations between frailty and other variables.
All questionnaires used in this study were previously translated into Persian language and validated in Iran17.
Ethics approval
The Ethics Committee of Tehran University of Medical Sciences and Bushehr University of Medical Sciences approved the protocol of this study (IR.TUMS.EMRI.REC.1394.0036). Written informed consent was obtained before participation. The protocol of this study followed the Ethics standards defined by the 2013 version of the Declaration of Helsinki. This study has been reported following the STROBE Statement.
Statistical analysis
The prevalence of variables was calculated as a survey analysis with the weighting of the Iranian population census 2016. For comparing our findings with those from other countries, the data were age-standardized based on the World Health Organization (WHO) population 2000–2025.
Quantitative variables are expressed as mean (SD). The prevalence of pre-frailty, frailty, and other components of geriatric giants was assessed in males and females and across different ranges of age. We also used the Chi-square (χ2) test to assess the effect of monthly income or wealth quantile on the prevalence of frailty.
A binary logistic regression model was used to identify the independent factors associated with frailty. The following variables were adjusted in the binary logistic regression model: age, gender, physical activity, cancer, MNA score, PHQ-9 score, waist circumference, BMI, WBC, smoking, marital status, number of comorbidities, and polypharmacy. The presence of the following comorbidities was assessed to calculate the number of comorbidities: hypertension, diabetes, hypo- and hyperthyroidism, chronic kidney disease, rheumatoid arthritis, osteoarthritis, Alzheimer’s disease, liver disease, lung disease, epilepsy, and Parkinson’s. We also used multinomial logistic regression model to investigate the associations between the number of geriatric giants and age, sex, low physical activity, cancer, MNA score, PHQ-9 score, waist circumference, BMI, and smoking.
In addition, we measured the co-incidence of 4 components of geriatric giants, including frailty, sarcopenia, cognitive impairment, and anorexia. Moreover, a multinomial logistic regression model was developed to assess the effect of different variables on the co-existence of frailty, sarcopenia, cognitive impairment, and anorexia. Age, sex, physical activity, cancer, MNA score, PHQ-9 score, waist circumference, BMI, smoking, WBC count, alcohol consumption, marital status, and the number of drugs were entered into this analysis as independent variables.
Stata package version 12 (StataCorp Texas, USA) was utilized for analysis. P values < 0.05 were considered statistically significant.
Data availability
Data analyzed for this article will be provided by the corresponding authors upon a reasonable request.
References
Oeppen, J. & Vaupel, J. W. Demography. Broken limits to life expectancy. Science 296, 1029–1031. https://doi.org/10.1126/science.1069675 (2002).
Christensen, K., Doblhammer, G., Rau, R. & Vaupel, J. W. Ageing populations: The challenges ahead. Lancet 374, 1196–1208. https://doi.org/10.1016/s0140-6736(09)61460-4 (2009).
Clegg, A., Young, J., Iliffe, S., Rikkert, M. O. & Rockwood, K. Frailty in elderly people. Lancet 381, 752–762. https://doi.org/10.1016/s0140-6736(12)62167-9 (2013).
Dwolatzky, T. Hazzard’s geriatric medicine and gerontology. Jama 302, 1813–1813 (2009).
Bartoszek, A., Niedorys, B. & Szalast, K. Geriatric giants among the elderly. J. Educ. Health Sport 9, 367–374 (2019).
Romero-Ortuno, R., Stuck, A. E. & Masud, T. The giants of education in geriatric medicine and gerontology. Age Ageing https://doi.org/10.1093/ageing/afac004 (2022).
Bulut, E. A., Soysal, P. & Isik, A. T. Frequency and coincidence of geriatric syndromes according to age groups: single-center experience in Turkey between 2013 and 2017. Clin. Interv. Aging 13, 1899–1905 (2018).
Soysal, P. & Tan, S. G. The prevalence and co-incidence of geriatric syndromes in older patients with early-stage Alzheimer’s disease and dementia with Lewy bodies. Aging Clin. Exp. Res. 33, 2599–2603 (2021).
Kara, O., Smith, L., Tan, S. G. & Soysal, P. The clinical implications and importance of anemia in older women. Acta Clin. Belg. 77, 558–564 (2022).
Rolfson, D. B., Heckman, G. A., Bagshaw, S. M., Robertson, D. & Hirdes, J. P. Implementing frailty measures in the canadian healthcare system. J. Frailty Aging 7, 208–216. https://doi.org/10.14283/jfa.2018.29 (2018).
He, B. et al. Prevalence and risk factors for frailty among community-dwelling older people in china: A systematic review and meta-analysis. J. Nutr. Health Aging 23, 442–450. https://doi.org/10.1007/s12603-019-1179-9 (2019).
Boura, F. T., Hosseini, S. R., Mouodi, S., Ghadimi, R. & Bijani, A. Frailty syndrome in older adults and related sociodemographic factors in the north of Iran: A population-based study. Iran. Red Crescent Med. J. 23, e259 (2021).
Alqahtani, B. A. et al. Healthcare. p 108 (MDPI)
Sirven, N. & Rapp, T. The cost of frailty in France. Euro. J Health Econ. HEPAC Health Econ. Prev. Care 18, 243–253. https://doi.org/10.1007/s10198-016-0772-7 (2017).
Holroyd-Leduc, J. et al. Giving voice to older adults living with frailty and their family caregivers: engagement of older adults living with frailty in research, health care decision making, and in health policy. Res. Involv. Engagem. 2, 23. https://doi.org/10.1186/s40900-016-0038-7 (2016).
Gwyther, H. et al. Understanding frailty: a qualitative study of European healthcare policy-makers’ approaches to frailty screening and management. BMJ open 8, e018653. https://doi.org/10.1136/bmjopen-2017-018653 (2018).
Shafiee, G. et al. Bushehr elderly health (BEH) programme: Study protocol and design of musculoskeletal system and cognitive function (stage II). BMJ Open 7, e013606 (2017).
Foley, A. L. et al. Association between the geriatric giants of urinary incontinence and falls in older people using data from the Leicestershire MRC Incontinence Study. Age Ageing 41, 35–40. https://doi.org/10.1093/ageing/afr125 (2012).
Muhammad, T. & Meher, T. Association of late-life depression with cognitive impairment: Evidence from a cross-sectional study among older adults in India. BMC Geriatr. 21, 364. https://doi.org/10.1186/s12877-021-02314-7 (2021).
Song, D. & Yu, D. S. F. Effects of a moderate-intensity aerobic exercise programme on the cognitive function and quality of life of community-dwelling elderly people with mild cognitive impairment: A randomised controlled trial. Int. J. Nurs. Stud. 93, 97–105. https://doi.org/10.1016/j.ijnurstu.2019.02.019 (2019).
Musa, M. K. et al. The prevalence, incidence, and correlates of fecal incontinence among older people residing in care homes: A systematic review. J. Am. Med. Dir. Assoc. 20, 956-962.e958. https://doi.org/10.1016/j.jamda.2019.03.033 (2019).
Hoogendijk, E. O. et al. Frailty: Implications for clinical practice and public health. Lancet 394, 1365–1375. https://doi.org/10.1016/s0140-6736(19)31786-6 (2019).
O’Donovan, M. R., Sezgin, D., Liew, A. & O’Caoimh, R. Burden of disease, disability-adjusted life years and frailty prevalence. QJM Mon. J. Assoc. Phys. 112, 261–267. https://doi.org/10.1093/qjmed/hcy291 (2019).
Kasajima, M. et al. Projecting prevalence of frailty and dementia and the economic cost of care in Japan from 2016 to 2043: A microsimulation modelling study. Lancet. Public Health 7, e458–e468. https://doi.org/10.1016/s2468-2667(22)00044-5 (2022).
Gobbens, R. J., van Assen, M. A., Luijkx, K. G., Wijnen-Sponselee, M. T. & Schols, J. M. Determinants of frailty. J. Am. Med. Dir. Assoc. 11, 356–364 (2010).
Ntanasi, E. et al. Prevalence and risk factors of frailty in a community-dwelling population: The HELIAD study. J. Aging Health 32, 14–24. https://doi.org/10.1177/0898264318801735 (2020).
Li, S. et al. Frailty risk prediction model among older adults: A Chinese nation-wide cross-sectional study. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph19148410 (2022).
Wanaratna, K., Muangpaisan, W., Kuptniratsaikul, V., Chalermsri, C. & Nuttamonwarakul, A. Prevalence and factors associated with frailty and cognitive frailty among community-dwelling elderly with knee osteoarthritis. J. Commun. Health 44, 587–595. https://doi.org/10.1007/s10900-018-00614-5 (2019).
Pradeep Kumar, D. et al. Sensor-based characterization of daily walking: a new paradigm in pre-frailty/frailty assessment. BMC Geriatr. 20, 164. https://doi.org/10.1186/s12877-020-01572-1 (2020).
Handforth, C. et al. The prevalence and outcomes of frailty in older cancer patients: A systematic review. Ann. Oncol. Off. J. Euro. Soc. Med. Oncol. 26, 1091–1101. https://doi.org/10.1093/annonc/mdu540 (2015).
Fedarko, N. S. The biology of aging and frailty. Clin. Geriatr. Med. 27, 27–37. https://doi.org/10.1016/j.cger.2010.08.006 (2011).
Müller, L., Di Benedetto, S. & Pawelec, G. The immune system and its dysregulation with aging. Subcell. Biochem. 91, 21–43. https://doi.org/10.1007/978-981-13-3681-2_2 (2019).
Srivastava, S. Emerging insights into the metabolic alterations in aging using metabolomics. Metabolites https://doi.org/10.3390/metabo9120301 (2019).
Zhang, Y., Chatzistamou, I. & Kiaris, H. Identification of frailty-associated genes by coordination analysis of gene expression. Aging 12, 4222–4229. https://doi.org/10.18632/aging.102875 (2020).
Thillainadesan, J., Scott, I. A. & Le Couteur, D. G. Frailty, a multisystem ageing syndrome. Age Ageing 49, 758–763. https://doi.org/10.1093/ageing/afaa112 (2020).
Davis, M. R. et al. Gender differences in the prevalence of frailty in heart failure: A systematic review and meta-analysis. Int. J. Cardiol. 333, 133–140. https://doi.org/10.1016/j.ijcard.2021.02.062 (2021).
Corbi, G. et al. Inter-relationships between gender, frailty and 10-year survival in older italian adults: An observational longitudinal study. Sci Rep 9, 18416. https://doi.org/10.1038/s41598-019-54897-2 (2019).
Hubbard, R. E., Lang, I. A., Llewellyn, D. J. & Rockwood, K. Frailty, body mass index, and abdominal obesity in older people. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 65, 377–381. https://doi.org/10.1093/gerona/glp186 (2010).
Yuan, L., Chang, M. & Wang, J. Abdominal obesity, body mass index and the risk of frailty in community-dwelling older adults: A systematic review and meta-analysis. Age Ageing 50, 1118–1128. https://doi.org/10.1093/ageing/afab039 (2021).
Delbari, A., Zanjari, N., Momtaz, Y. A., Rahim, F. & Saeidimehr, S. Prevalence of frailty and associated socio-demographic factors among community-dwelling older people in southwestern Iran: A cross-sectional study. J. Diabetes Metab. Disord. 20, 601–610 (2021).
Shohani, M., Mohammadi, I., Seidkhani, H. & Mohamadnejad, S. The prevalence of frailty and its associated factors among Iranian hospitalized older adults. Nurs. Midwifery Stud. 11, 215 (2022).
Fried, L. P. et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 56, M146–M157 (2001).
Hassankhani, H., Asghari Jafarabadi, M., Darvishpur Kakhki, A., Malek, M. & Scott, J. Reliability and validity of the Persian version of the falls efficacy scale—international. J. Am. Geriatr. Soc. 63, 596–598 (2015).
Mahdavi, A. M., Mahdavi, R., Lotfipour, M., Jafarabadi, M. A. & Faramarzi, E. Evaluation of the Iranian mini nutritional assessment short-form in community-dwelling elderly. Health Promot. Perspect 5, 98 (2015).
Taheri Tanjani, P. & Azadbakht, M. Psychometric properties of the Persian version of the activities of daily living scale and instrumental activities of daily living scale in elderly. J. Mazandaran Univ. Med. Sci. 25, 103–112 (2016).
Farrahi, H. et al. Psychometric properties of the Persian version of patient health questionnaire-9. Iran. J. Psychiatry Clin. Psychol. 27, 248–263 (2021).
Dadfar, M., Kalibatseva, Z. & Lester, D. Reliability and validity of the Farsi version of the patient health questionnaire-9 (PHQ-9) with Iranian psychiatric outpatients. Trends Psychiatry Psychother. 40, 144–151 (2018).
Rezaei, M., Rashedi, V., Lotfi, G., Shirinbayan, P. & Foroughan, M. Psychometric properties of the Persian adaptation of mini-cog test in Iranian older adults. Int J Aging Hum Dev 86, 266–280 (2018).
Searle, S. D., Mitnitski, A., Gahbauer, E. A., Gill, T. M. & Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. 8, 1–10 (2008).
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
S.Z.B. (writing the draft, editing the draft), M.A. (writing the draft, editing the draft), H.F. (data collection), A.Y. (editing the draft), S.M. (data collection), S.M.A. (data curation), S.S. (editing the draft), F.S. (data analysis, conceptualization), A.O. (conceptualization), N.F. (data collection), I.N. (data collection), B.L. (data curation), G.S. (data curation), and R.H. (data collection). This study has been reported after obtaining patients’ informed consent.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Badrkhahan, S.Z., Ala, M., Fakhrzadeh, H. et al. The prevalence and predictors of geriatric giants in community-dwelling older adults: a cross-sectional study from the Middle East. Sci Rep 13, 12401 (2023). https://doi.org/10.1038/s41598-023-39614-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-39614-4
- Springer Nature Limited
This article is cited by
-
Prevalence of cognitive frailty and its associated factors in a population of Iranian older adults
Aging Clinical and Experimental Research (2024)