
Abstract
Coronary heart disease (CHD) risk is influenced by socioeconomic status-related parameters, particularly occupation. We investigated occupational gaps in CHD risk and how the introduction of remote work moderated the observed occupational differences in CHD risk during the coronavirus disease 2019 pandemic in Japan. Data from a web-based, nationwide cohort study, comprising 17,640 workers (aged 20–65 years) with baseline data from December 2020, were analyzed. Participants were grouped by occupation as upper-level nonmanual workers (managers/professionals) and others (reference group). The primary outcome was CHD (angina pectoris/myocardial infarction) onset retrospectively confirmed at the 1-year follow-up survey. Upper-level nonmanual workers exhibited a higher CHD incidence than others (2.3% vs. 1.7%). This association was pronounced in the younger (20–49 years) population, with a significant CHD risk (adjusted risk ratio = 1.88). Upper-level nonmanual workers exhibited nearly 15% higher remote work prevalence, with a significant remote work-related CHD risk (adjusted risk ratio = 1.92). The mediating effects of remote work explained an overall disparity of 32% among the younger population. Occupational gaps in CHD incidence in Japan differ from those in Western countries, where upper-level nonmanual workers have lower cardiovascular risk. In Japan, remote work can mediate CHD risk in the younger population of upper-level nonmanual workers.
Similar content being viewed by others



Introduction
Coronary heart disease (CHD) is a leading cause of morbidity and mortality worldwide, with significant emphasis on the fundamental influence of socioeconomic status (SES)-related parameters, particularly occupation, on CHD risk1,2. Numerous studies have extensively documented contemporary, universal occupational gaps in CHD risk3,4, highlighting an “inverse” pattern: individuals in higher occupational classes, such as those holding upper-level nonmanual jobs, including managerial and professional positions, tend to experience lower cardiovascular risk than do their counterparts in lower occupational strata5,6. Occupational factors, such as job-related stress and sedentary work, and established behavioral risks, such as smoking and elevated serum cholesterol levels, have been identified as mediators of occupational CHD risk4,7,8.
However, occupational disparities in CHD risk have remained understudied in Japan, and some previous studies have reported associations deviating from those observed in Western countries6,9,10,11. Prior nationwide studies in Japan have shown a “positive” pattern, where individuals in higher occupational classes exhibited an increased CHD risk11. These findings challenge conventional knowledge, highlighting that occupational gaps in CHD risk may be diverse even in developed countries with high-quality medical care accessible to all through universal health coverage.
Furthermore, the prominence of remote work, particularly during the coronavirus disease 2019 (COVID-19) pandemic, has been a focus area in terms of occupational health12. Recent studies have revealed the psychological distress associated with remote work13,14,15. However, the impact of this trend on occupational CHD disparities remains unexplored. As Japan confronted the challenges of the pandemic, remote work became a pivotal aspect of employment practices (> 60% of companies adopted remote work)13. Nonetheless, the extent to which remote work, a hallmark of the COVID-19 era, may influence these risks remains uninvestigated.
Therefore, this study aimed to examine occupational gaps in CHD risk in Japan to elucidate how the emergence of remote work, a novel working style in Japan, mediated the observed occupational disparities in CHD risk during the COVID-19 pandemic. Here, we show for the first time that the benefits to cardiovascular health experienced by upper-level nonmanual workers may not always be universally applicable in remote work.
Results
Table 1 displays the baseline characteristics and outcomes of the study cohort. The incidence of CHD was higher among CHD among upper-level nonmanual workers than among their counterparts in other-occupation categories (2.3% vs. 1.7%). This disparity in CHD incidence was particularly pronounced in the younger population (3.1% vs. 1.3%), whereas no significant difference was observed in the older population. Upper-level nonmanual workers exhibited nearly 15% and 10% higher prevalence for remote work and smoking, respectively, than did the other-occupation groups. Additionally, among 4536 current smokers, the proportion of those who had increased their smoking habits at baseline was higher among remote workers than among non-remote workers (15.2% vs. 9.7%; Table 2). Meanwhile, the prevalence of long working hours did not differ between non-remote and remote workers: 1142/13728 (8.3%) versus 339/3912 (8.7%, P = 0.49), respectively.
The relative risks (RRs) for CHD incidence associated with occupation are presented in Fig. 1 (see full results for other variables in Supplemental Table S1). While the RR of upper-level nonmanual workers did not reach statistical significance in the overall and older populations, it demonstrated a significant increase in the younger population (Model 1: RR = 2.19, 95% CI 1.40–3.42). After adjusting for remote work in Model 2, the RR was attenuated but remained significant (RR = 1.96, 95% CI 1.24–3.08). Finally, in Model 3, with full adjustments for behavioral, clinical, mental, and occupational risks, the RR was significant (RR = 1.88, 95% CI 1.18–3.00). The remote work RR for CHD incidence was not elevated in the older population; however, it was significantly elevated in the overall and younger populations (RR = 1.49, 95% CI 1.19–1.86 and RR = 1.92, 95% CI 1.37–2.68, respectively; Fig. 1). The RR of hypertension was elevated while that of long working hours was not significant (Supplemental Table S1).

Relative risks and 95% confidence intervals for coronary heart disease incidence Relative risks were estimated using two-level multilevel Poisson regression with robust variance. Participants (Level 1) were nested within 47 prefectures (Level 2), and a random intercept was employed for prefectures. Adjustments were made for basic confounding variables of sex, age, educational attainment, and household income in Model 1. In Model 2, covariates simultaneously included upper-level nonmanual workers and remote workers. In Model 3, further adjustments were made for the following potential mediating variables: behavioral factors (smoking, heavy drinking, and physical activity), clinical factors (body mass index, hypertension, and diabetes), psychological distress, and long working hours. Abbreviations: RR, Relative risk; CI, confidence interval.
Lastly, in the mediation analysis of the association between occupation and CHD incidence among the younger population (for all and older populations, see Supplemental Table S2), the mediating effects of remote work explained an overall proportion of 32% (Table 3). Sex-specific analyses showed similar patterns, while the impact was most pronounced in younger men (Table 4).
Discussion
In this study, we examined occupational gaps in CHD risk in Japan to elucidate how the emergence of remote work mediated the observed occupational disparities in CHD risk during the COVID-19 pandemic. Contrary to the SES gap in CHD observed in many developed countries, where higher occupational classes typically exhibit lower CHD risks, the present study confirmed that individuals in higher occupational classes in Japan tended to face higher CHD risks during the COVID-19 pandemic. Individuals in higher occupational groups faced nearly double the risk of CHD incidence among younger men. This aligns with the results of previous studies conducted in this country6,9,10,11. Interestingly and unexpectedly, this study also made a novel observation that remote work appears to play a role in “increasing” cardiovascular risk. Thus, it emerges as a significant mediator for occupation-related CHD incidence in Japan, accounting for approximately one-third of the mediating effects.
These deviations from the contemporary SES pattern may partly be attributed to behavioral risk factors, notably smoking, associated with remote-site workplaces, including the home, which is physically outside of the original workplace. In Japan, considerable efforts have been invested in promoting smoking cessation as part of occupational health practices. However, this study revealed that the prevalence of current smoking is possibly higher in upper-level nonmanual workers than in other-occupation groups. When these upper-level nonmanual workers engage in remote work, often from their homes, the smoking regulations and policies of their original workplace no longer apply. Consequently, quitting smoking becomes more challenging16, and it is conceivable that the quantity of smoking may even increase under these circumstances, as observed among current smokers in the present study.
In some instances, remote work has been reported to increase workers’ productivity and be associated with better mental health17. However, current occupational health research has focused on the fact that social support from coworkers tends to decrease among remote workers, resulting in occupational distress13,14,15,18. During the present study period, when remote work had rapidly spread in its early stage in Japan, younger managers and professionals may have faced increased workloads without adequate social support, given that remote work was a new working style that was not experienced previously. Therefore, the subsequent job stress may have contributed to an increased CHD risk among this specific population. In addition, a higher prevalence of longtime working among upper-level nonmanual workers may have influenced CHD in relation to job stress in this study.
This study has some limitations. First, despite being conducted in a cohort design, CHD onset was retrospectively self-reported at the 1-year follow-up point, which was not enough to sufficiently observe CHD onset. Consequently, detailed clinical diagnoses and information were unavailable for analysis. Selection bias was inevitably introduced in this Internet cohort study, as respondents self-selected for participation; thus, the generalizability was partly limited. However, the follow-up rate of almost 70% was fair. Second, the regression analyses comprehensively considered numerous multi-dimensional variables, including behavioral, clinical, mental, and occupational factors. However, the intensity of smoking and the impact of heated tobacco products, which are new tobacco products that have gained popularity during the study period19 could not be assessed owing to a lack of information. Unadjusted confounding variables may have also been present. Nevertheless, the study’s strength lies in its findings that shed light on remote work in combination with occupational class, which has become a “new normal” among younger generations but presents disadvantages in terms of cardiovascular health. These novel findings may help elucidate the underlying mechanisms of occupational disparities in CHD related to remote work in future studies.
In conclusion, this study reveals that the current occupational disparities in CHD incidence in Japan follow a pattern different from that in Western countries. Among the younger population, remote work appears to mediate coronary risk for upper-level nonmanual workers. These findings highlight the complex interplay of occupational factors in CHD risk and call for further investigation into the impact of remote work on cardiovascular health within different demographics.
Methods
Study design and setting
This nationwide, web-based cohort study followed 17,640 participants over the course of 1 year. Data were extracted from the Collaborative Online Research on the Novel-coronavirus and Work (CORoNaWork) Project, an extensive online cohort survey of Japanese workers enrolled in December 2020 during the country’s “third wave” of COVID-19 infections20. Details of the baseline survey and follow-up protocol have been described20,21,22. In brief, the study cohort encompassed individuals who were workers aged 20–65 years at baseline. They were selected via a systematic sampling strategy that considered factors such as sex, occupation, and regional residence within Japan. This study was performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the University of Occupational and Environmental Health, Japan (no. R2-079). Informed consent was obtained.
From an initial recruitment pool of 33,087 participants, 6051 participants who provided invalid responses were excluded, retaining 27,036 eligible participants for the baseline analysis of the CORoNaWork Project (Wave 1). Subsequently, in this cohort study, 18,560 participants were respondents to a 1-year follow-up survey in December 2021 (response rate, 68.6%; Wave 2). Among these, 920 participants with a medical history of CHD at baseline were excluded (see profiles in Supplemental Table S3), yielding the analytical cohort of 17,640 working individuals aged 20–65 years who had never experienced CHD at the baseline.
Primary outcome: CHD onset
The primary outcome was CHD onset, which was retrospectively confirmed at Wave 2. The question about CHD incidence in the Wave 2 survey was phrased as follows: “Are you presently undergoing outpatient care or treatment for angina pectoris or myocardial infarction?” Participants responded with one of the following options: “I have never had this illness,” “I am currently undergoing outpatient care or treatment,” “I was previously receiving outpatient care or treatment, but I am currently on self-interruption,” “I was advised to undergo tests or treatment, but I have not visited a medical institution,” or “I am currently cured or in remission (no longer requiring treatment).”
The absence of CHD during the follow-up period was defined as a response of “I have never had this illness.” Meanwhile, the other four responses indicated incident CHD during the study period. The exact date of CHD onset was not available in this study.
Occupational class
For occupational class, participants were grouped into upper-level nonmanual workers (n = 1886, 10.7%, comprising managers and/or professionals) and others (n = 15,754, 89.3%), according to previous studies6,11. In general, regarding socioeconomic disparities in mortality, upper-level nonmanual workers, including individuals with the highest occupational class, tend to have the best advantages in economic (income, security, and advancement prospects) and occupational dimensions (authority and autonomy)6,11.
Remote work and other covariates
Remote work was considered a primary mediating variable that may influence changes in occupational CHD risk. Participants were categorized as engaged in remote work if they reported working from home at least once per month during the baseline assessment.
When examining the association between occupational class and CHD risk, the following fundamental confounding variables were considered: sex, age, educational attainment (≤ 12 years [high school] or ≥ 13 years [college or university]), and household income (< 2 million JPY [approximately 20,000 USD] or ≥ 2 million JPY). Additionally, to further consider potential mediators, various covariates of behavioral factors (smoking, habitual drinking [> 1 day/week], and physical activity [either a ≥ 30 min light sweating exercise more than once per week or a ≥ 1 h walking or equivalent activities more than once per week]), clinical factors (body mass index, hypertension, and diabetes), psychological distress (Kessler 6 scores > 10), and long working hours (> 55 h weekly) were included23.
Statistical analysis
Risk ratios (RRs) and 95% confidence intervals (CIs) were estimated for CHD incidence among upper-level nonmanual workers. The other-occupation group served as the reference group. A two-level multilevel Poisson regression with robust variance, where participants (Level 1) were nested within 47 prefectures (Level 2), was employed, and a random intercept for prefectures was applied24. Owing to the lack of precise timing information for CHD onset in the study, incidence rate ratios could not be estimated. In the multivariable regression analysis, adjustments were made for basic confounding variables of sex, age, educational attainment, and household income (Model 1). In Model 2, a primary mediating variable of remote work was added. Finally, all potential mediating variables were accounted for in Model 3. Moreover, in Models 2 and 3, the estimated RRs of remote work were acknowledged as explanation factors for CHD incidence related to remote work. In a subgroup analysis, stratified analyses were conducted by age groups: (i) a younger population aged 20–49 years and (ii) an older population aged 50–65 years. Sex-specific analyses were also performed.
Furthermore, a causal mediation analysis (Fig. 2) using a four-way decomposition method was performed to estimate the proportion of occupational disparities in CHD risk in upper-level nonmanual workers explained by remote work25. The exposure (upper-level nonmanual worker), mediator (remote work), confounders (sex, age, educational attainment, and household income), and outcome (CHD incidence) were defined24,25,26,27. Statistical significance was set at 0.05, and all P-values were two-sided. Data were analyzed using STATA/MP17 (StataCorp LLC, College Station, TX, USA).
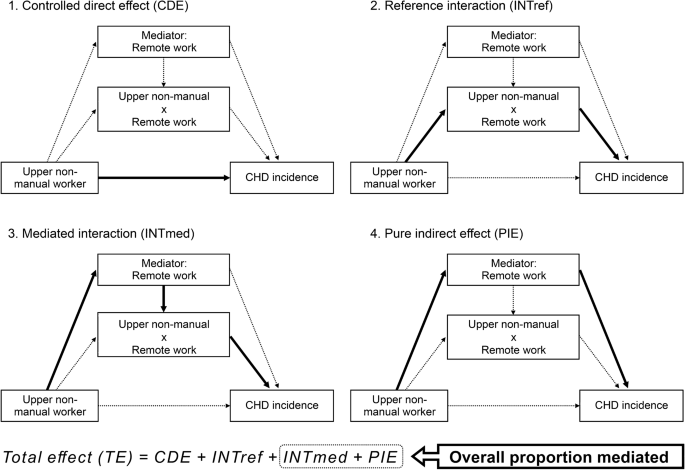
Causal diagram representing the four-way decomposition of the association between upper-level nonmanual workers, remote work, and coronary heart disease incidence. The exposure (upper-level nonmanual worker), mediator (remote work), confounders (sex, age, educational attainment, and household income), and outcome (coronary heart disease [CHD] incidence) were defined. Logistic regression models were fitted with a four-way decomposition for the outcome (as a function of the exposure, the mediator, exposure-mediator interaction, and confounders) and the mediator (as a function of the exposure and confounders). The total effect (TE) of the exposure, in the presence of the mediator with which the exposure may interact, on the outcome is decomposed into four components due to just mediation (pure indirect effect, PIE), just interaction (reference interaction, INTref), both mediation and interaction (mediated interaction, INTmed), and neither mediation nor interaction (controlled direct effect, CDE): i.e., TE = CDE + INTref + INTmed + PIE. The overall proportion of the total effect explained by the mediating effect (“total indirect effect”) was estimated using these four components, as follows: (INTmed + PIE)/TE.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Stringhini, S. et al. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: A multicohort study and meta-analysis of 1·7 million men and women. Lancet 389, 1229–1237 (2017).
Avendano, M. et al. Socioeconomic status and ischaemic heart disease mortality in 10 Western European populations during the 1990s. Heart 92, 461–467 (2006).
Marmot, M. G. et al. Health inequalities among British civil servants: The Whitehall II study. Lancet 337, 1387–1393 (1991).
Kivimäki, M. et al. Job strain as a risk factor for coronary heart disease: A collaborative meta-analysis of individual participant data. Lancet 380, 1491–1497 (2012).
Erikson, R., Goldthorpe, J. H. & Portocarero, L. Intergenerational class mobility and the convergence thesis: England, France and Sweden. Br. J. Sociol. 61, 185–219 (2010).
Tanaka, H. et al. Mortality inequalities by occupational class among men in Japan, South Korea and eight European countries: A national register-based study, 1990–2015. J. Epidemiol. Community Health 73, 750–758 (2019).
Iso, H. et al. Perceived mental stress and mortality from cardiovascular disease among Japanese men and women: The Japan collaborative cohort study for evaluation of cancer risk sponsored by Monbusho (JACC Study). Circulation 106, 1229–1236 (2002).
Chandola, T. et al. Work stress and coronary heart disease: What are the mechanisms?. Eur. Heart J. 29, 640–648 (2008).
Wada, K. et al. Trends in cause specific mortality across occupations in Japanese men of working age during period of economic stagnation, 1980–2005: Retrospective cohort study. BMJ 344, e1191 (2012).
Fukai, K. et al. A case control study of occupation and cardiovascular disease risk in Japanese men and women. Sci. Rep. 11, 23983 (2021).
Zaitsu, M. et al. Occupational class and risk of cardiovascular disease incidence in Japan: Nationwide, multicenter, hospital-based case-control study. J. Am. Heart Assoc. 8, e011350 (2019).
Yoshikawa, Y. & Kawachi, I. Association of socioeconomic characteristics with disparities in COVID-19 outcomes in Japan. JAMA Netw. Open 4, e2117060 (2021).
Otsuka, S. et al. A cross-sectional study of the mismatch between telecommuting preference and frequency associated with psychological distress among Japanese workers in the COVID-19 pandemic. J. Occup. Environ. Med. 63, e636–e640 (2021).
Miyake, F. et al. Job stress and loneliness among desk workers during the COVID-19 pandemic in Japan: Focus on remote working. Environ. Health Prev. Med. 27, 33 (2022).
Ikegami, K. et al. Job stress and work from home during the COVID-19 pandemic among Japanese workers: A prospective cohort study. Health Psychol. Behav. Med. 11, 2163248 (2023).
Yamamoto, T., Abbas, H., Kanai, M., Yokoyama, T. & Tabuchi, T. Factors associated with smoking behaviour changes during the COVID-19 pandemic in Japan: A 6-month follow-up study. Tob. Control (2022).
Awada, M., Lucas, G., Becerik-Gerber, B. & Roll, S. Working from home during the COVID-19 pandemic: Impact on office worker productivity and work experience. Work 69, 1171–1189 (2021).
Tejero, L. M. S., Seva, R. R. & Fadrilan-Camacho, V. F. F. Factors associated with work-life balance and productivity before and during work from home. J. Occup. Environ. Med. 63, 1065–1072 (2021).
Myagmar-Ochir, E. et al. Occupational difference in use of heated tobacco products: A cross-sectional analysis of retail workers in Japan. BMJ Open 11, e049395 (2021).
Fujino, Y. et al. Protocol for a nationwide Internet-based health survey of workers during the COVID-19 pandemic in 2020. J. UOEH 43, 217–225 (2021).
Anan, T. et al. Association between COVID-19 infection rates by region and implementation of non-pharmaceutical interventions: A cross-sectional study in Japan. J. Public Health 45, 229–236 (2023).
Mori, T. et al. Workplace infection control measures and perceived organizational support during the COVID-19 pandemic in Japan: A prospective cohort study. J. Occup. Environ. Med. 64, e769–e773 (2022).
Kivimäki, M. et al. Long working hours and risk of coronary heart disease and stroke: A systematic review and meta-analysis of published and unpublished data for 603,838 individuals. Lancet 386, 1739–1746 (2015).
Zaitsu, M. et al. Maternal heated tobacco product use during pregnancy and allergy in offspring. Allergy 78, 1104–1112 (2023).
Vanderweele, T. J. A unification of mediation and interaction: A 4-way decomposition. Epidemiology 25, 749–761 (2014).
Discacciati, A., Bellavia, A., Lee, J. J., Mazumdar, M. & Valeri, L. Med4way: a Stata command to investigate mediating and interactive mechanisms using the four-way effect decomposition. Int. J. Epidemiol. 48, 15–20 (2018).
Zaitsu, M. et al. Occupational disparities in survival from common cancers in Japan: Analysis of Kanagawa cancer registry. Cancer Epidemiol. 77, 102115 (2022).
Acknowledgements
The current members of the CORoNaWork Project, in alphabetical order, are as follows: Dr. Akira Ogami, Dr. Ayako Hino, Dr. Hajime Ando, Dr. Hisashi Eguchi, Dr. Keiji Muramatsu, Dr. Koji Mori, Dr. Kosuke Mafune, Dr. Makoto Okawara, Dr. Mami Kuwamura, Dr. Mayumi Tsuji, Dr. Ryutaro Matsugaki, Dr. Seiichiro Tateishi, Dr. Shinya Matsuda, Dr. Tomohiro Ishimaru, Dr. Tomohisa Nagata, Dr. Yoshihisa Fujino (present chairperson of the study group), and Dr. Yu Igarashi. All members are affiliated with the University of Occupational and Environmental Health, Japan. This work was supported and partly funded by research grants from the University of Occupational and Environmental Health, Japan (no grant number); the Japanese Ministry of Health, Labour and Welfare (H30-josei-ippan-002, H30-roudou-ippan-007, 19JA1004, 20JA1006, 210301-1, 20HB1004, 23EA1003, 23FA1004, 23JA1003, and 23JA1004); the Japan Society for the Promotion of Science (JSPS KAKENHI JP22K17401); UOEH Grant-in-Aid for Collaborative Research between the Institute of Industrial Ecological Sciences and the University Hospital (2022-1); Anshin Zaidan (no grant number); the Collabo-Health Study Group (no grant number); and Hitachi Systems, Ltd. (no grant number) and scholarship donations from Chugai Pharmaceutical Co., Ltd. (no grant number). The funders were not involved in the study design, collection, analysis, or interpretation of data, the writing of this paper, or the decision to submit the paper for publication.
Author information
Authors and Affiliations
Contributions
Y.F. supervised the study. All the authors designed the research protocol, developed the questionnaire, and created the dataset. M.Z. developed the methodology and M.Z. and T.I. analyzed the data. M.Z., T.I., and S.T. wrote the first draft of the manuscript. All authors revised and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zaitsu, M., Ishimaru, T., Tsushima, S. et al. Incidence of coronary heart disease among remote workers: a nationwide web-based cohort study. Sci Rep 14, 8415 (2024). https://doi.org/10.1038/s41598-024-59000-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-59000-y
- Springer Nature Limited