
Abstract
Lung isolation usually refers to the isolation of the operative from the non-operative lung without isolating the non-operative lobe(s) of the operative lung. We aimed to evaluate whether protecting the non-operative lobe of the operative lung using a double-bronchial blocker (DBB) with continuous positive airway pressure (CPAP) could reduce the incidence of postoperative pneumonia. Eighty patients were randomly divided into two groups (n = 40 each): the DBB with CPAP (Group DBB) and routine bronchial blocker (Group BB) groups. In Group DBB, a 7-Fr BB was placed in the middle bronchus of the right lung for right lung surgery and in the inferior lobar bronchus of the left lung for left lung surgery. Further, a 9-Fr BB was placed in the main bronchus of the operative lung. In Group BB, routine BB placement was performed on the main bronchus on the surgical side. The primary endpoint was the postoperative pneumonia incidence. Compared with Group BB, Group DBB had a significantly lower postoperative pneumonia incidence in the operative (27.5% vs 5%, P = 0.013) and non-operative lung (40% vs 15%) on postoperative day 1. Compared with routine BB use for thoracoscopic lobectomy, using the DBB technique to isolate the operative lobe from the non-operative lobe(s) of the operative lung and providing CPAP to the non-operative lobe(s) through a BB can reduce the incidence of postoperative pneumonia in the operative and non-operative lungs.
Similar content being viewed by others


Background
Double-lumen tubes (DLT) and bronchial blockers (BB) are the most commonly used airway tools in thoracic surgery1. They allow isolation of the operative lung from the non-operative lung, which prevents contamination of the non-operative lung by pollutants, such as blood and sputum2. However, in thoracoscopic lobectomy, these two options only protect the non-operative lung from contamination and do not protect the non-operative lobe(s) of the operative lung. Recent case reports have explored the protection of non-operative lobe(s) of the operative lung using solutions such as a DLT + BB or the double-bronchial blocker (DBB) technique3,4,5. These plans are feasible and can provide lung protection for nonsurgical lung lobes. However, given the small sample sizes of these previous reports, the feasibility and efficacy of using DLT + BB or DBB techniques in thoracoscopic lobectomy still need to be determined. Compared with using DLT, using BB showed more infiltrate especially at the surgery side based on the chest X-ray6. Therefore, we hypothesised that a DBB used with continuous positive airway pressure (CPAP) technology might protect the non-operative lobe(s) of the operative lung during thoracoscopic lobectomy.
This randomised controlled trial aimed to compare the effects of DBB with CPAP technology and those of routine BB on the non-operative lobe(s) of the operative lung and the incidence of postoperative pneumonia in both the operative and non-operative lung after thoracoscopic lobectomy.
Methods
Ethics
This study was approved by the Medical Ethics Committee of the Fourth Hospital of Hebei Medical University on 20 September 2021 (ID:2021116) and was registered before patient enrolment in the Chinese Clinical Trial Registry (http://www.chictr.org.cn; registration number: ChiCTR2100052086; Principal investigator: Jianfeng Fu; Date of registration: 16 October 2021). The trial was conducted from 1 November 2021 to 28 February 2022. Written informed consent was obtained from all patients before the trial. The first author of this article was responsible for recruiting participants among patients scheduled for video-assisted thoracoscopic lobectomy at our hospital. The manuscript was written in accordance with the CONSORT statement. The authors declare that all experiments on human subjects were conducted in accordance with the Declaration of Helsinki and that all procedures were carried out with the adequate understanding and written consent of the subjects.
Participants
We recruited patients with lung cancer who were scheduled to undergo thoracoscopic lobectomy at the Fourth Hospital of Hebei Medical University. The inclusion criteria were as follows: (1) ASA grade I–II; (2) age 18–65 years, with a body mass index of 18.5–25 kg/m2; (3) no obvious abnormalities in pulmonary function, unlimited or obstructive ventilatory dysfunction, and FEV1/FVC > 70%; (4) no obvious abnormalities in cardiac function, no cardiovascular disease, and ejection fraction > 50%; (5) no preoperative anaemia or other haematological diseases and no history of radiotherapy or chemotherapy; and (6) voluntary study participation with provision of written informed consent. The exclusion criteria were as follows: (1) history of bronchial asthma and airway hyperreactivity; (2) pulmonary infection, bronchopleural fistula, emphysema, or pulmonary vesicles; and (3) presence of a tumour in the airway affecting the placement of bronchial blockers.
Using a computer-generated randomisation table, patients were randomly divided into two groups: the DBB with CPAP group (Group DBB; n = 40) and the routine BB group (Group BB; n = 40). The anaesthesiologists and surgeons, but not the postoperative follow-up team, were informed of the group allocation.
Anaesthesia
After the patient entered the operative room, the nurse established upper limb venous access; conducted electrocardiography, pulse oximetry, non-invasive blood pressure measurement, and bispectral index monitoring; and performed radial artery puncture and catheterisation under local anaesthesia for invasive monitoring of arterial blood pressure. Anaesthesia was induced with sufentanil 0.2–0.4 μg/kg, cis-atracurium 0.2 mg/kg, and etomidate 0.2–0.3 mg/kg. After the eyelid reflex disappeared, mask-assisted ventilation was provided for 3 min.
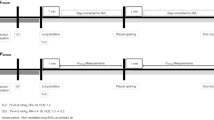
The airway management protocol for patients in Group DBB was as follows. First, we inserted a 7-Fr BB through the mouth under direct vision. Next, we inserted a #8.0 tube 2–3 cm below the glottis. The position of the BB was adjusted using a fibre-optic bronchoscope (for right lung surgery, we placed the 7-Fr BB in the middle bronchus of the right lung; for left lung surgery, we put the 7-Fr BB in the inferior lobar bronchus of the left lung. We then fixed the tube and 7-Fr BB. Subsequently, a 9-Fr BB was put through the tube in the main bronchus of the operative lung) (Fig. 1). When starting single-lung ventilation, we provided 5 cm H2O CPAP to the nonsurgical lung lobe on the surgical side through the suction hole of the BB. This was maintained until the restoration of bilateral pulmonary ventilation.

Position of the BB, (a): for right lung surgery, 7-Fr BB was placed in the middle bronchus of the right lung while the 9-Fr BB was placed through the tube in the right main bronchus; (b): for left lung surgery, 7-Fr BB was placed in the inferior lobar bronchus of the left lung while the 9-Fr BB was placed through the tube in the left main bronchus; (c, d): for left lung surgery, position of 7-Fr BB and 9-Fr BB in the patient's trachea.
The airway management protocol for the Group BB was as follows. First, an #8.0 tube was inserted through the mouth and placed 2–3 cm below the glottis. Next, a 9-Fr BB was put into the tube. A fibre-optic bronchoscope was used to confirm that the BB was in a good position and placed appropriately in the main bronchus of the operative lung. During one-lung ventilation, the BB suction port was connected to the atmosphere.
The anaesthesia maintenance and recovery methods were the same for all patients. We added 0.05 mg/kg cis-atracurium every half hour. The pressure-control ventilation mode was based on the ideal body weight, and dual-lateral ventilation was performed before the thoracic cavity was connected to the atmosphere. The respiratory parameters were as follows: tidal volume, 8–10 mL/kg; respiratory rate, 12–14 bpm; inspiration–expiration ratio, 1:2; inhaled oxygen concentration, 100%; and partial pressure of end-tidal carbon dioxide (PetCO2) maintained at 35–45 mm Hg. A fibre-optic bronchoscope was inserted with the patient lying on their side. When the pleura was opened, lung collapse was induced using a disconnection technique7,8. After manual recruitment of the non-operative lungs, one-lung ventilation was maintained. During one-lung ventilation, the respiratory parameters were as follows: tidal volume, 6–8 mL/kg; respiratory rate, 13–15 bpm; inspiration–expiration ratio, 1:2; inhaled oxygen concentration, 100%; PetCO2 maintained at 35–45 mm Hg. After surgery, the BB was removed, and the sputum was thoroughly suctioned. After spontaneous breathing was restored, the tracheal tube was removed, and the patient was returned to the ward after attaining a Steward score of 6.
Outcomes
The primary outcome was the incidence of postoperative pneumonia in the operative and non-operative lungs on the first day after surgery. Three of the following five characteristics were pneumonia9: chest radiograph with infiltrate, fever > 38 °C, leucocytosis, antibiotic treatment, and positive sputum culture. Secondary outcomes included the duration of surgery, the incidence of hypoxaemia, BB displacement rate, surgeon satisfaction, white blood cell count (WBC), neutrophil count (N), neutrophil percentage (N%), C-reactive protein (CRP) level, length of hospital stay (LOS), and total hospital costs.
Based on the criteria above, the respiratory physician in the postoperative follow-up team determined whether the patient developed pneumonia. Hypoxaemia was considered to have occurred when oxygen saturation was < 90%. Intraoperatively, if a sudden increase in airway pressure occurred and ventilation could not be maintained, or if the operative lung suddenly inflated, we considered that BB displacement had occurred; accordingly, a bronchoscope was used to reposition the BB. Such occurrences were recorded.
Surgeon satisfaction with respect to the operating space was evaluated by the surgeon after the operation (Level I: large operating space, uneventful surgery; Level II: sufficient operating space to allow surgery completion; Level III: small operating space impeding surgery completion without adjustment).
Statistical analysis
The incidence of pulmonary complications after thoracic surgery is high10, ranging from 10.7 to 50%9,11,12,13. Therefore, we assumed that the incidence of pneumonia in Group BB would be 45%. In a pilot study, the incidence of pneumonia in a DBB-treated group was approximately 15%. The formula for comparing the rates between two independent samples was as follows:
Accordingly, 35 participants were required in each group (power: 0.8; type I error: 0.05; \({u}_{\alpha }\) = 1.96; \({u}_{\beta }\) = 0.842). To address exclusion and loss, we increased the number of patients in each group and eventually targeted 40 patients per group.
Fisher's exact test was used for between-group comparisons of the incidence of postoperative pneumonia, expressed as a percentage. The t-test was used for between-group comparisons of the duration of surgery, WBC count, N count, N%, CRP, LOS, and total hospitalisation costs, with the results being expressed as mean ± standard deviation. Chi-square tests were used for between-group comparisons of the incidence of hypoxaemia, the BB displacement rate, and surgeon satisfaction. Statistical significance was set at p < 0.05. All analyses were performed using IBM SPSS Statistics 23.0 for Windows (IBM Corporation, Armonk, NY, USA).
Results
Between November 2021 and February 2022, 80 patients were randomly and equally assigned to the two groups (Fig. 2). All the patients completed the trial. Table 1 presents the demographic characteristics of patients in each group.

CONSORT diagram of the study participants.
Compared with Group BB, Group DBB had a significantly lower incidence of postoperative pneumonia in the operative lung (P = 0.013; Table 2) and non-operative lung (P = 0.023; Table 2).
There were no significant between-group differences in the duration of surgery, the incidence of hypoxaemia, BB displacement rate, and surgeon satisfaction (P > 0.05; Table 3). Further, no significant between-group differences existed in the WBC count, N, N%, and CRP levels on the first day after surgery (P > 0.05, Table 3). Moreover, there were no significant between-group differences in hospitalisation time or total hospitalisation costs (P > 0.05, Table 3).
Discussion
Postoperative pneumonia is a common complication of thoracoscopic lobectomy and can affect patient prognosis9. Our findings showed that the incidence of operative lung pneumonia in group BB was 5.5 times higher than in Group DBB. In contrast, the incidence of non-operative lung pneumonia in Group BB was 2.67 times higher than in Group DBB. These findings indicate that the use of a DBB significantly reduced the incidence of postoperative pneumonia, which could affect patient prognoses.
The two most commonly used airway tools for lung isolation are DLT and BB14, which are designed to prevent contamination of the non-operative lung by tumours or secretions from the operative lung15. However, these two airway tools cannot isolate the operative lobes from the non-operative lobes of the operative lung. In this study, we used the DBB technique to isolate not only the operative lung from the non-operative lung but also the operative lobe(s) from the non-operative lobe(s) of the operative lung, which prevented contamination of the non-operative lobe(s) by the operative lobe(s) of the operative lung. This may explain the low incidence of operative lung pneumonia in Group DBB. We provided the non-operative lobes of the operative lungs with 5 cm H2O CPAP through the BB suction hole. Studies have confirmed that 5 cm H2O CPAP does not affect the surgical field of view16 and that this can reduce the local immune response in the non-operative lobe(s) of the operative lungs17. This may be another reason for the relatively lower incidence of operative lung pneumonia in Group DBB.
During one-lung ventilation, hypoxic pulmonary vasoconstriction (HPV) causes blood flow to shift from the operative lung to the non-operative lung16,18, which increases blood flow in the non-operative lung by 49–56%17. High perfusion in the non-operative lung is directly related to lung injury19. A previous study confirmed that, during one-lung ventilation, there was a higher incidence of alveolar and interstitial oedema, haemorrhage, neutrophil infiltration, and microatelectasis in the non-operative lung than in the operative lung19. Similar conclusions have been drawn from different animal models. Broccard et al. suggested that the intensity of lung perfusion contributes to ventilator-induced lung injury20. A study on acute lung injury after lobectomy found that density increased more in the non-operated lung than in the operated lung, suggesting a truly asymmetric form of acute respiratory distress syndrome21. This explains the higher incidence of pneumonia in the non-operative lung than in the operative lung in both groups. In this study, we administered 5 cm H2O CPAP to the non-operative lobe(s) of the operative lung in Group DBB, which weakened HPV, attenuating the increase in operative lung vascular resistance and diminishing the transfer of blood flow from the operative lung to the non-operative lung17,18. This may be another reason for the lower incidence of non-operative lung pneumonia in Group DBB than in Group BB.
A high displacement rate and interruption of surgery have been reported as disadvantages of BB22. We observed no significant between-group difference in the BB displacement rate, consistent with previous reports22,23,24. The BB displacement rate is related to the placement position; because the right main bronchus is shorter, the BB displacement rate in right lung surgery is higher than that in left lung surgery25. In Group DBB, one BB was placed deep in the inferior lobar bronchus of the left lung or middle lobar bronchus of the right lung, which made it less likely to shift. There were no cases of hypoxaemia; further, there were no significant between-group differences in surgeon satisfaction, indicating that the minor expansion of the non-operative lung lobe did not affect the execution of the surgery, and it did not cause hypoxaemia because of BB displacement.
Numerous factors affect patient prognosis and LOS, such as patient age and the extent of surgical resection10. In this study, we used randomisation to allocate patients to groups, with no significant between-group differences in age or surgical lung tissue. We reduced the incidence of postoperative pneumonia in patients who underwent DBB through the indicated intervention. Although the LOS in this group was 0.5 d shorter than that in Group BB, this difference did not reach statistical significance. The sample size of this trial was estimated based on the incidence of postoperative pneumonia; therefore, the sample size may have been too small to identify significant differences in LOS. Future tests with larger sample sizes are required.
To ensure the stability of CPAP, we used a device that could continuously adjust the pressure and monitor CPAP in real-time using a pressure sensor to ensure that the pressure applied was the pressure that was set for the experiment. In Group DBB, one patient experienced inflation of the non-operative lobe(s) of the operative lung because of CPAP pressure of 5 cm H2O, which affected the surgeon's ability to operate. The surgery could be performed smoothly after adjusting the CPAP pressure to 4 cm H2O. Currently, most research on CPAP is conducted using a DLT; moreover, it has been concluded that a CPAP of 5 cm H2O can improve oxygenation26,27. Few studies have investigated the optimal CPAP administered by BB, with only a few case reports using a pressure of 5 cm H2O28,29; therefore, we used a CPAP of 5 cm H2O in this study.
Limitations
This study had some limitations. First, it was a single-centre study. To ensure consistency among the study participants, the participants selected for this study underwent lobectomy and did not undergo procedures such as pneumonectomy. Therefore, it remains unclear whether DBB reduces the incidence of pneumonia in patients undergoing other surgical procedures. Second, the sample size was estimated based on the incidence of pneumonia in patients, which was relatively small. Finally, the anaesthesiologists and surgeons could not be blinded. Because the surgeon can see the location of the blue cuff of the BB under the thoracoscope, it was easy for the surgeon to know the patient's group allocation. Additionally, two BBs were used in our study, increasing the patient burden. Using an improved BB to achieve the effects of the DBB technique in subsequent studies may be more beneficial to patients.
Conclusions
In conclusion, the current study showed that, for thoracoscopic lobectomy, using the DBB technique to isolate the operative from the non-operative lobe(s) of the operative lung and providing CPAP to the non-operative lobe(s) through the BB can reduce the incidence of postoperative pneumonia in both lungs. This does not increase the rate of BB displacement or complicate the execution of the surgery and holds benefits for patient prognosis. Further larger-scale studies on this topic should investigate the extent of the benefits this approach has for patients.
Abbreviations
- DBB:
-
Double-bronchial blocker
- CPAP:
-
Continuous positive airway pressure
- BB:
-
Bronchial blocker
- DLT:
-
Double-lumen tubes
- WBC:
-
White blood cell count
- N:
-
Neutrophil count
- N%:
-
Neutrophil percentage
- CRP:
-
C-reactive protein
- LOS:
-
Length of hospital stay
- PetCO2 :
-
Pressure of end-tidal carbon dioxide
- HPV:
-
Hypoxic pulmonary vasoconstriction
References
Cohen, E. Back to blockers?: The continued search for the ideal endobronchial blocker. Anesthesiology https://doi.org/10.1097/ALN.0b013e3182839981 (2013).
Kumar, N. et al. Left-sided double-lumen tube vs EZ-blocker for one-lung ventilation in thoracic surgery: A systematic review and meta-analysis. Semin. Cardiothorac. Vasc. Anesth. https://doi.org/10.1177/10892532231184781 (2023).
Gil, M. G. et al. A new strategy in lung/lobe isolation in patients with a lung abscess or a previous lung resection using double lumen tubes combined with bronchial blockers. Ann. Card. Anaesth. 25(3), 343–345. https://doi.org/10.4103/aca.ACA_16_21 (2023).
Sumitani, M. et al. Selective lobar bronchial blockade using a double-lumen endotracheal tube and bronchial blocker. Gen. Thorac. Cardiovasc. Surg. 55(5), 225–227. https://doi.org/10.1007/s11748-007-0108-8 (2007).
Amar, D. et al. A novel method of one-lung isolation using a double endobronchial blocker technique. Anesthesiology 95(6), 1528–1530. https://doi.org/10.1097/00000542-200112000-00039 (2001).
Yang, L. et al. A comparison between bronchial blockers and double-lumen tubes for patients undergoing lung resection: A propensity score-matched cohort study. Int. J. Med. Sci. 19(11), 1706–1714. https://doi.org/10.7150/ijms.75835 (2022).
Bussières, J. S. et al. Bronchial blocker versus left double-lumen endotracheal tube in video-assisted thoracoscopic surgery: A randomized-controlled trial examining time and quality of lung deflation. Can. J. Anesth./J. Can. Anesth. 63(7), 818–827. https://doi.org/10.1007/s12630-016-0657-3 (2016).
Young Yoo, J. et al. Disconnection technique with a bronchial blocker for improving lung deflation: A comparison with a double-lumen tube and bronchial blocker without disconnection. J. Cardiothorac. Vasc. Anesth. 28(4), 904–907. https://doi.org/10.1053/j.jvca.2013.07.019 (2014).
Van Haren, R. M. et al. Enhanced recovery decreases pulmonary and cardiac complications after thoracotomy for lung cancer. Ann. Thorac. Surg. 106(1), 272–279.https://doi.org/10.1016/j.athoracsur.2018.01.088 (2018).
Shang, K., Jin, L., Zhang, G., Li, X. & Yu, H. Risk factors for pulmonary complications after thoracoscopic lung resection and the prediction value. Chin. J. Anesthesiol. 42(07), 823–826.https://doi.org/10.3760/cma.j.cn131073.20220401.00707 (2022).
Li, X. F. et al. Comparative effect of propofol and volatile anesthetics on postoperative pulmonary complications after lung resection surgery: A randomized clinical trial. Anesth. Analg. 133(4), 949–957.https://doi.org/10.1213/ANE.000-0000000005334 (2021).
Inderpal, S. et al. Lobectomy in octogenarians: Real world outcomes for robotic-assisted, video-assisted thoracoscopic, and open approaches. J. Thorac. Dis. 11(6), 2420–2430. https://doi.org/10.21037/jtd.2019.05.52 (2019).
Colquhoun, D. A. et al. A lower tidal volume regimen during one-lung ventilation for lung resection surgery is not associated with reduced postoperative pulmonary complications. Anesthesiology 134(4), 562–576. https://doi.org/10.1097/ALN.0000000000003729 (2021).
Cheng, Q. et al. The disconnection technique with the use of a bronchial blocker for improving nonventilated lung collapse in video-assisted thoracoscopic surgery. J. Thorac. Dis. 12(3), 876–882. https://doi.org/10.21037/jtd.2019.12.75 (2020).
Licker, M. et al. Isolation of the lung: Double-lumen tubes and endobronchial blockers. Trends Anaesth. Crit. Care https://doi.org/10.1016/j.tacc.2014.04.003 (2014).
Sentürk, M. et al. A comparison of the effects of 50 % oxygen combined with CPAP to the non-ventilated lung vs. 100 % oxygen on oxygenation during one-lung ventilation. Anasthesiologie Intensivmedizin Notfallmedizin Schmerztherapie Ains 39(6), 360. https://doi.org/10.1055/s-2004-814506 (2004).
Verhage, R. J. et al. Reduced local immune response with continuous positive airway pressure during one-lung ventilation for oesophagectomy. BJA: Br. J. Anaesth. 112, 920 (2014).
Tojo, K., Goto, T. & Kurahashi, K. Protective effects of continuous positive airway pressure on a nonventilated lung during one-lung ventilation: A prospective laboratory study in rats. Eur. J. Anaesthesiol. 33(10), 776. https://doi.org/10.1097/EJA.0000000000000460 (2016).
Kozian, A. et al. One-lung ventilation induces hyperperfusion and alveolar damage in the ventilated lung: An experimental study. Br. J. Anaesth. 4, 549–559. https://doi.org/10.1093/bja/aen021 (2008).
Broccard, A. F., Hotchkiss, J. R. & Kuwayama, N. Consequences of vascular flow on long injury induced by mechanical ventilation. Am. J. Respir. Crit. Care Med. 157(6), 1935–1942 (1998).
Padley, S. P. et al. Asymmetric ARDS following pulmonary resection: CT findings initial observations. Radiology 223, 468 (2002).
Langiano, N. et al. Airway management in anesthesia for thoracic surgery: A “real life” observational study. J. Thorac. Dis. 11(8), 3257–3269.https://doi.org/10.21037/jtd.2019.08.57 (2019).
Templeton, T. W. et al. A prospective comparison of intraluminal and extraluminal placement of the 9-french arndt bronchial blocker in adult thoracic surgery patients. J. Cardiothorac. Vasc. Anesth.https://doi.org/10.1053/j.jvca.2017.02.188 (2017).
Lu, Y. et al. Bronchial blocker versus left double-lumen endotracheal tube for one-lung ventilation in right video-assisted thoracoscopic surgery. J. Cardiothorac. Vasc. Anesth. 32(1), 297–301. https://doi.org/10.1053/j.jvca.2017.07.026 (2018).
Xie, Y. H. et al. The application of endobronchial blocker in video-assisted thoracoscopy surgery. Int. J. Anesthesiol. Resusc. 34(6), 3. https://doi.org/10.3760/cma.j.issn.1673-4378.2013.06.005 (2013).
Long, S. et al. Effect of the VivaSight double-lumen tube on the incidence of hypoxaemia during one-lung ventilation in patients undergoing thoracoscopic surgery: A study protocol for a prospective randomised controlled trial. BMJ Open 13(4), e068071. https://doi.org/10.1136/bmjopen-2022-068071 (2023).
L’Acqua, C. et al. CPAP effects on oxygen delivery in one-lung ventilation during minimally invasive surgical ablation for atrial fibrillation in the supine position. J. Cardiothorac. Vasc. Anesth. 34(11), 2931–2936. https://doi.org/10.1053/j.jvca.2020.03.064 (2020).
Muelleck, J. R., Maracaja, L. & Templeton, T. W. Selective lobar blockade with a bronchial blocker in combination with a double lumen tube to manage refractory hypoxemia: A case report. Cureus 14(7), e26638. https://doi.org/10.7759/cureus.26638 (2022).
Zhou, C. et al. Continuous positive airway pressure for treating hypoxemia due to pulmonary vein injury: A case report. World J. Clin. Cases https://doi.org/10.12998/wjcc.v11.i8.1830 (2023).
Funding
The authors received no funding for this study.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study's conception and design. Chao Zhou and Hongbo Guo wrote the manuscript; Shan Song and Xinxin Cui followed up on the patient after surgery and diagnosed pneumonia. Xuelian Zhao and Huaqin Liu provided revision suggestions; Huanshuang Pei and Shasha Zhang contributed to the redaction of this manuscript and proofreading; Jianfeng Fu contributed to the manuscript finalising. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhou, C., Song, S., Fu, J. et al. Protecting the non-operative lobe/s of the operative lung can reduce the pneumonia incidence after thoracoscopic lobectomy: a randomised controlled trial. Sci Rep 14, 9442 (2024). https://doi.org/10.1038/s41598-024-60114-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-60114-6
- Springer Nature Limited