
Abstract
Plyometric training (PT) is an effective training method for improving physical fitness among trained individuals; however, its impact on health-related physical fitness in untrained participants remains ambiguous. Therefore, this meta-analysis aimed to evaluate the effects of PT on health-related physical fitness among untrained participants. Six electronic databases (PubMed, CINAHL Plus, MEDLINE Complete, Web of Science Core Collection, SCOPUS, and SPORTDiscus) were systematically searched until March 2024. We included controlled trials that examined the effects of PT on health-related physical fitness indices in untrained participants. Twenty-one studies were eligible, including a total of 1263 participants. Our analyses revealed small to moderate effects of PT on body mass index, muscular strength, cardiorespiratory fitness, and flexibility (ES = 0.27–0.61; all p > 0.05). However, no significant effects were detected for body fat percentage and lean mass (ES = 0.21–0.41; all p > 0.05). In conclusion, the findings suggest that PT may be potentially effective in improving health-related physical fitness indices (i.e., body mass index, muscular strength, cardiorespiratory fitness, and flexibility) in untrained participants. However, the results should be interpreted cautiously due to data limitations in some fitness variables.
Similar content being viewed by others


Introduction
Physical fitness is characterized by the capacity to engage in daily activities with energy and alertness, without excessive fatigue, while still enjoying leisure pursuits and responding effectively to unexpected emergencies1. Health-related physical fitness pertains to the specific aspects of physical fitness closely linked to overall health and well-being2. The level of health-related physical fitness is a predictive factor for cardiovascular and metabolic diseases, as well as the overall risk of mortality across one’s lifespan3,4. The components of health-related physical fitness include body composition, muscular strength, muscular endurance, flexibility, and cardiorespiratory fitness5. Numerous studies have consistently demonstrated that adequate health-related fitness is linked to a reduced risk of disease and an improved quality of life. For example, insufficient cardiorespiratory fitness has been correlated with an increased incidence of hypertension6, cardiovascular diseases7, and mental health disorders such as depression8. Likewise, sub-optimal body composition (e.g., low muscle mass and high adipose tissue levels) is associated with significant chronic ailments, such as cancers, type 2 diabetes, and mortality9.
Plyometric training (PT) is a highly favored training approach frequently recommended by researchers as an effective method for enhancing various aspects of physical performance10,11,12,13. Conceptually, PT is characterized by the utilization of the stretch–shortening cycle (SSC), which occurs during the transition from a swift eccentric muscle contraction (deceleration phase) to a quick concentric muscle contraction (acceleration phase)14. SSC movements take advantage of the elastic properties of connective tissue and muscle fibers, enabling muscles to store elastic energy during the deceleration phase and release it during the acceleration phase to augment muscular force and power production15,16. Moreover, PT induces numerous favorable adaptations in musculoskeletal and neural systems, muscle function and performance of healthy individuals17. In this sense, by enhancing the SSC and related neuro-mechanical mechanisms, PT can potentially improve human performance.
In the literature, many systematic reviews and meta-analyses have demonstrated that PT enhances physical fitness. For example, PT has proven beneficial in improving the physical fitness of athletes across a diverse range of sports, including team sports18, water sports19, racket sports20, and combat sports21. Moreover, several meta-analyses have confirmed that PT can improve physical fitness in both healthy young individuals and adults22,23,24,25. A meta-analysis by de Villarreal et al.26 emphasized that PT significantly increases strength performance. Similarly, Ramirez-Campillo et al.27 identified PT as an effective and safe form of exercise for enhancing body composition. However, these research efforts have mainly focused on athletic groups or a mix of trained and untrained subjects. The impact of PT may differ significantly depending on various characteristics of the subjects, such as their level of training, age, gender, or familiarity with plyometric exercises26. Consequently, the effectiveness and feasibility of PT in enhancing overall health-related physical fitness among untrained individuals remain underexplored, with a notable lack of comprehensive reviews on this topic.
Historically, plyometric exercises have typically demanded a significant degree of neuromuscular control and a substantial level of strength, often indicated by requirements such as a back squat of at least 150% of one’s body mass28. This has generated uncertainty among practitioners regarding the safety and feasibility of plyometric exercises for untrained individuals. These concerns arise from the fact that untrained populations typically lack the fundamental neuromuscular control and strength levels traditionally considered prerequisites for athletes before engaging in high-intensity PT29. On the contrary, some experts argue that basic competency in bodyweight movements should suffice before gradually introducing simple plyometric exercises into a training regimen30. In line with this viewpoint, PT has been successfully integrated into the routines of very elderly individuals over the age of 7531 and young children under ten years of age32,33, with no reported injuries or adverse events.
Despite a growing number of experimental trials investigating the impact of PT on untrained individuals, the effects on health-related physical fitness seem inconsistent. For example, while some researchers34,35 have documented improvements in cardiorespiratory fitness after PT, others have found no such improvements36,37. Moreover, some studies38,39 have identified positive effects of PT on body composition, such as reductions in body fat percentage, while other studies37,40 have reported no positive impact. Hence, it is urgent for investigators to find an appropriate way to address the existing conflicting results. Conducting a systematic review and meta-analysis, which involves systematically collecting and screening relevant studies and rigorously assessing the quality of the included research, represents the highest level of evidence in evidence-based practice41. Currently, no systematic review or meta-analysis has been published regarding the effect of PT interventions on overall health-related physical fitness in untrained populations. Therefore, the primary objective of this systematic review and meta-analysis was to identify and rigorously assess the existing research findings derived from collected data and to pool the results of publications in a meta-analysis. By doing so, we intend to provide a well-informed conclusion regarding the impact of PT on health-related physical fitness in untrained participants.
Materials and methods
The present review is reported following the updated PRISMA statement42, and the review protocol has been registered in the PROSPERO (identifier CRD42023473050).
Search strategy
We conducted a comprehensive literature search by accessing six electronic databases: PubMed, CINAHL Plus, MEDLINE Complete, Web of Science Core Collection, SCOPUS, and SPORTDiscus, from their inception to March 20, 2024. Specific combinations of terms were tailored for each of these databases: (“plyometric training” OR “ballistic training” OR “jump training” OR “plyometric exercise*” OR “power training” OR “stretch–shortening cycle”) AND (“physical fitness” OR “body composition” OR “body weight status” OR “body mass” OR BMI OR “body fat” OR “cardiorespiratory fitness” OR “cardiorespiratory endurance” OR “muscular fitness” OR “musculoskeletal fitness” OR “muscular strength” OR “muscular endurance” OR “flexibility”). Moreover, a thorough manual search was conducted on both Google Scholar and the reference lists of all selected papers to ensure that no relevant publications were missed. The search string for each database can be found in Supplementary Material Appendix 1.
Selection criteria
The inclusion criteria following the PICOS framework43 were applied as follows: (a) untrained participants who did not engage in any systematic training or competitive sport, without restrictions on sex and age; (b) a PT intervention lasting more than two weeks, including lower body exercises (e.g., jumping, hopping, skipping) and/or upper body exercises (e.g., medicine ball exercises, push-ups) utilizing the SSC. Studies that incorporated combined training (e.g., PT and balance training) were included in the analysis when the control group underwent the same training regimen, except the PT component; (c) a control group; (d) at least one measure of health-related physical fitness parameters; (e) randomized controlled or non-randomized controlled design.
Studies were excluded if they (a) involved injured individuals (e.g., ankle sprain); (b) had interventions lasting shorter than two weeks; (c) did not provide adequate results (e.g., mean and standard deviation); (d) tested the effects of PT without a control group; (e) training interventions that do not include PT or training interventions where PT programs make up less than 50% of the total training load when combined with other training methods (e.g., heavy resistance training), and (f) were conducted in languages other than English. Because of translation difficulties and most of the literature on PT is in English44, only English language studies were included.
Risk of bias in individual studies and certainty of evidence
The risk of bias in each selected randomized controlled trial (RCTs) was evaluated using the updated Cochrane risk of bias assessment for randomized trials (RoB-2)45. For non-randomized controlled trials (non-RCTs), the Risk Of Bias In Non-randomized Research of Interventions (ROBINS-I) tool was employed46. The certainty of evidence was analyzed and summarized following the guidelines outlined in the GRADE handbook47. Two research team members independently (ND, KGS) evaluated the risk of bias for each selected trial.
Data extraction
The data items were common metrics of health-related physical fitness, including (a) body composition (e.g., body mass index (BMI), body fat percentage, and lean mass), (b) muscular strength (e.g., handgrip), (c) muscular endurance (e.g., sit-ups), (d) cardiorespiratory fitness (e.g., maximal oxygen uptake (VO2max)), and (e) flexibility (e.g., sit and reach). Apart from the mentioned data elements, descriptive characteristics of the PT interventions (e.g., length, frequency) and the participants (e.g., sex, age) were extracted, and adverse effects were recorded. To conduct the meta-analysis, we chose original articles that provided data suitable for calculation and utilized consistent outcome measures.
Statistical analyses
When at least three trials provided sufficient data to calculate the effect size (ES), a meta-analysis was conducted19,48. Mean and standard deviation data from pre- and post-intervention measures were used to compute ESs for performance outcomes in both the PT and control groups (i.e., Hedges’ g). The data were standardized using the post-intervention standard deviation values, and a random-effects model was employed to account for variances across trials that could potentially affect the effects of PT49,50. The values of ES were accompanied by 95% confidence intervals (CIs), and the calculated ES values were interpreted using the following scale: ES < 0.2 was considered trivial, 0.2–0.6 was classified as small, > 0.6–1.2 was considered moderate, > 1.2–2.0 was categorized as large, > 2.0–4.0 was considered very large, and ES > 4.0 was considered extremely large51. In trials involving multiple intervention groups, the sample size of the control group was split proportionately so that all subjects could be compared52. In cases where authors did not submit adequate data (in graphics or were missing), we attempted to contact the corresponding authors. If the authors did not reply to our requests or could not supply the relevant data, the investigation’s findings were dropped from the study. However, if data were presented in a figure but no numerical data was included in the tables or supplementary material, we utilized the Graph Digitizer software (Digitizelt, Germany) to extract the relevant data from the graphs or figures53. We evaluated study heterogeneity using I2 statistics. Values below 25% indicated low heterogeneity, 25–75% suggested moderate heterogeneity, and above 75% reflected high heterogeneity54. The extended Egger’s test was employed to assess the publication bias risk in the studies55. When bias was detected, the trim and fill method was utilized. Stratification of the meta-analyses was performed for each of these factors, and a threshold of p < 0.05 was utilized as the significance level to determine statistical significance. The Comprehensive Meta-Analysis software (Version 3.0; Biostat, Englewood, NJ, USA) was used for all analyses. In addition, if it was not feasible to statistically pool the data, the findings were presented in a narrative format.
Results
Study selection
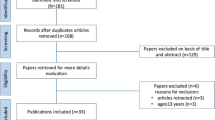
As shown in Fig. 1, the databases yielded a total of 3993 documents, with an additional 18 publications obtained via references and Google Scholar. After manually removing duplicates, there were 2221 unique records remaining. These records’ titles and abstracts were evaluated, yielding 511 publications acceptable for full-text examination. Following a careful evaluation of all the texts, 490 documents were removed, leaving 21 studies that met all of the criteria set for the systematic review and meta-analysis.

PRISMA flow diagram.
Risk of bias in individual studies and certainty of evidence
RoB-2 assessments were conducted on 17 RCTs34,35,37,38,39,40,56,57,58,59,60,61,62,63,64,65,66, while ROBINS-I assessments were employed for four non-RCTs36,67,68,69. Out of these trials, 12 exhibited an overall moderate risk of bias or some concerns35,37,40,56,57,58,59,60,64,66,67,69, seven noted a high (or serious) risk of bias34,38,39,61,62,63,68, and only two showed a low risk of bias36,65, as illustrated in Figs. 2 and 3. Figure 2 presents the results of the RoB-2 assessments. Among these RCTs, only three reported their randomization sequence generation method, which involved either stratified block randomization or online randomization software (www.randomizer.org)61,63,65. In contrast, the remaining eleven articles did not comprehensively describe their randomized procedures. In six RCTs, a high risk of bias was identified due to missing data, which was linked to a dropout rate exceeding 15%34,38,39,61,62,63. A visual depiction of the findings of ROBINS-I evaluations is shown in Fig. 3. A non-RCT study identified a moderate risk of bias due to an approximately 10% dropout rate and concerns regarding the selection of reported outcomes69. Another study68 revealed a high risk of bias because of a 25% dropout rate. Additionally, one trial had a moderate risk of bias in selecting study participants67.

RoB-2 assessments. Created using Robvis tool.

ROBINS-I assessments. Created using Robvis tool.
Table 1 shows the GRADE analysis results. The GRADE analyses found very low to moderate levels of certainty in the evidence supporting the outcomes.
Study characteristics
Table 2 provides a detailed overview of the participants’ characteristics and PT programs employed in the included studies. Supplementary Material Appendix 2 contains the data used in the meta-analyses. Publications were released between 2000 and 2023. The included studies involved a collective participation of 1263 subjects, comprising 417 females and 846 males. The sample sizes within the study groups ranged from 15 to 220 subjects, with participants’ ages spanning from 7 to 69.5 years. The majority of studies exclusively recruited either males (n = 11)36,37,38,40,56,60,62,63,65,66,69 or females (n = 7)34,39,58,61,64,67,68, while other three studies included both female and male participants35,57,59. Nine studies provided information on the effects of PT interventions on body composition34,37,38,39,40,61,62,67,68, 15 on muscular strength36,37,38,39,57,58,59,60,61,62,63,64,66,67,69, six on cardiorespiratory fitness34,35,36,37,57,65, five on flexibility36,37,56,57,64, and one on muscular endurance69. The length of PT intervention varied from 4 to 36 weeks, with most trials opting for a 12-week intervention period (n = 8). The planned training sessions ranged from 12 to 108, with weekly training sessions set at either two or three. The duration of each session varied from 15 to 90 min.
Synthesis of the results
Body composition
Five studies assessed BMI, involving six experimental groups and five control groups (pooled n = 369). The results indicated a small effect of PT on BMI (ES = 0.46; 95% CI − 0.09 to 1.01; p = 0.099). A high heterogeneity (I2 = 91.83%) was observed, and the Egger’s test indicated p = 0.920. After we removed one study62 from the analysis, we found a significant moderate effect in favor of PT while heterogeneity decreased (ES = 0.53; 95% CI 0.03–1.04; p < 0.039, I2 = 73.91%; Fig. 4).

Forest plot and effect sizes for plyometric training (PT) compared with controls for body mass index. EG experimental group.
Regarding body fat percentage, data from eight studies were analyzed, including nine experimental groups and eight control groups (pooled n = 341). The results indicated a small effect of PT on body fat percentage (ES = 0.41; 95% CI − 0.02 to 0.84; p = 0.064; Fig. 5). A moderate heterogeneity (I2 = 71.38%) was observed, and the Egger’s test indicated p = 0.005. Since publication bias for body fat percentage was detected, we applied the trim and fill method; however, the ES remained unchanged.

Forest plot and effect sizes for plyometric training (PT) compared with controls for body fat percentage. EG experimental group.
Regarding lean mass, data from five studies were analyzed, including five experimental groups and five control groups (pooled n = 149). The results indicated a small effect of PT on lean mass (ES = 0.21; 95% CI − 0.07 to 0.49; p = 0.143; Fig. 6). A low heterogeneity (I2 = 0.00%) was observed, and the Egger’s test indicated p = 0.951.

Forest plot and effect sizes for plyometric training (PT) compared with controls for lean mass.
Muscular strength
Fifteen studies assessed muscular strength, involving seventeen experimental groups and fifteen control groups (pooled n = 865). The results indicated a moderate effect of PT on muscular strength (ES = 0.61; 95% CI 0.40–0.82; p < 0.001; Fig. 7). A moderate heterogeneity (I2 = 47.08%) was observed, and the Egger’s test indicated p = 0.669.

Forest plot and effect sizes for plyometric training (PT) compared with controls for muscular strength. EG experimental group.
Cardiorespiratory fitness
Six studies assessed cardiorespiratory fitness, involving ten experimental groups and seven control groups (pooled n = 493). The results indicated a moderate effect of PT on cardiorespiratory fitness (ES = 0.61; 95% CI 0.31–0.92; p < 0.001; Fig. 8). A moderate heterogeneity (I2 = 59.28%) was observed, and the Egger’s test indicated p = 0.016. After the trim and fill method, the adjusted values indicated a point estimate of ES = 0.44 (95% CI 0.14–0.73).

Forest plot and effect sizes for plyometric training (PT) compared with controls for cardiorespiratory fitness. EG experimental group.
Flexibility
Five studies assessed flexibility, involving five experimental groups and five control groups (pooled n = 276). The results indicated a moderate effect of PT on flexibility (ES = 0.54; 95% CI 0.05–1.04; p = 0.032). A high heterogeneity (I2 = 76.19%) was observed, and the Egger’s test indicated p = 0.274. After we removed one study64 from the analysis, although the significant effect of PT remained (ES = 0.27; 95% CI 0.03–0.51; p < 0.001; Fig. 9), the heterogeneity was reduced to 0.00%.

Forest plot and effect sizes for plyometric training (PT) compared with controls for flexibility.
Muscular endurance
Due to the limited availability of studies, muscular endurance could not be included in the meta-analysis. Thus, the certainty of the evidence was automatically rated as very low. A study assessed the effect of PT on muscular endurance among 220 male high school students. The results revealed that the muscular endurance of adolescents significantly improved after 12 weeks of PT69.
Adverse effects
In a study conducted by Van Roie et al.63, which focused on older men aged 68–80 years, out of the 14 participants who initially joined the PT group, three individuals (one in week 5 and two in week 6) discontinued their participation due to various issues. One participant dropped out due to knee pain, while the other two experienced gastrocnemius muscle strain during forward or sideways step-up exercises. Four participants reported knee pain and five experienced mild muscle soreness. Notably, only three participants in the PT group did not report any side effects over the 12 weeks. In three other studies37,39,58, a few participants were excluded due to health issues, but the authors emphasized that these health issues were unrelated to the PT program. In addition, Villada et al.68 reported no injuries during the training period, except for subjective fatigue and muscle aches during the first weeks of participation. Beyond these instances, no other studies included in this review documented any cases of soreness, fatigue, injuries, pain, or adverse effects caused by PT intervention.
Discussion
This meta-analysis examined peer-reviewed research on the effects of PT vs. controls on health-related physical fitness outcomes in untrained individuals. These analyses indicate that PT can significantly improve MBI, muscular strength, cardiorespiratory fitness, and flexibility compared to control conditions. However, the effects of PT on body fat percentage and lean mass were not statistically significant. In addition, based on the available data, it cannot be determined whether PT can enhance muscular endurance. According to the GRADE assessment, the level of evidence for the evaluated outcomes ranged from very low to moderate.
The effect of PT on body composition
Enhancing lean body mass and decreasing the percentage of body fat are advantageous health outcomes in addressing the increasing prevalence of obesity70. In the present review, body composition was evaluated using BMI, body fat percentage, and lean mass. The included studies measured the body composition parameters using skinfold calipers37,68 and bioelectrical impedance analysis34,62. Bioelectrical impedance analysis has gained popularity due to its affordability, portability, and ease of use71. However, some researchers have noted that bioelectrical impedance analysis might overestimate the body fat percentage in lean and athletic individuals, while it might underestimate this percentage in those who are heavier and have a higher body fat percentage72. Our meta-analysis revealed that PT positively affects BMI in untrained individuals; however, it does not show significant benefits in reducing body fat percentage or improving lean body mass. It seems that changes in body composition are the main elements that restore energy balance via increased energy expenditure73. The observed improvement in BMI can be attributed to the increased energy expenditure and muscle mass gains associated with PT74,75. However, the absence of alterations in body composition parameters (i.e., body fat percentage and lean body mass) aligns with findings from a prior meta-analysis investigating the impact of lower extremity PT on body composition27. Moreover, several studies focusing on athletes found no substantial changes in body composition. For example, Campo et al.76 determined that a 12-week PT program had no significant effects on body fat in female soccer players. Similarly, in the case of Aloui et al.77, no substantial changes in body fat percentage were observed following an eight-week PT regimen for handball players.
Some researchers have pointed out that the age range plays a significant role in developmental changes, where substantial increases in weight and height may lead to negligible changes in body composition78. Vetrovsky et al.24 propose that PT may not be the primary exercise choice if the goal is to effect changes in body composition. Still, it could be integrated into a periodized program to yield additional functional adaptations that may not be achieved through other types of exercise interventions. It is worth noting that a study by Racil et al.34 discovered that PT, when added to high-intensity interval training in overweight/obese females, led to a more substantial decrease in body fat in comparison to high-intensity interval training alone. Furthermore, several studies suggest combining exercise training with dietary adjustments leads to decreased body fat and increased lean mass79,80,81. Additionally, some investigators have claimed that aerobic exercise is the preferred method for reducing body fat and body mass. Concurrently, they recommend adopting a training program incorporating plyometric exercises to enhance lean body mass82,83. In this regard, researchers are encouraged to delve deeper into the dose-response relationships concerning PT variables, such as exercise type, intensity, and volume, or their combination with other strategies. This exploration is expected to improve our understanding of the relationship between PT and body composition measures, potentially enhancing the health benefits for untrained populations.
The effect of PT on muscular strength
Muscular strength is the capacity to exert force under specified biomechanical conditions84. This physical attribute is essential, as it influences proficiency in executing various tasks, whether in sports or daily life85. The evaluation of muscular strength across different studies incorporated various measurement methods, including leg press, knee extension, handgrip strength, and push-ups. These tests evaluated strength in distinct muscle groups, which may explain the moderate level of heterogeneity observed in the analysis. Our findings indicate that positive effects on the muscular strength of untrained participants were observed after PT. These results align with the conclusions drawn from previous meta-analyses9,26. Strength increases resulting from PT are based on the physiological principle that stretching a muscle before contraction leads to greater force generation26. In short, PT-induced enhancements in muscular strength can be attributed to several neuromuscular adaptations, including (a) improved neural activation of agonist muscles, (b) modifications in single-fiber mechanics, (c) changes in muscle size and structure, and (d) alterations in muscle-tendon mechanical stiffness14,16,86. Furthermore, the gains in muscular strength following PT can also be attributed to muscle hypertrophy87. Additionally, increased body weight and height naturally occurring with age could be connected to improvements in muscular strength88,89. Given that most of the research in our review assessed muscular strength in children and adolescents, the results presented here can be considered a typical and expected response to training.
According to a systematic review, it appears that PT may positively impact muscular strength in older adults, although perhaps not to the same magnitude as resistance training24. In addition, resistance training is a popular method used to improve muscular strength85,90. In our analysis, research conducted by Van Roie et al.63 investigated the impact of PT compared to regular walking and reported favorable results. Besides, they observed similar improvements in muscular strength after 6 weeks of PT compared to conventional resistance exercises in older individuals. Nevertheless, older people who participate in PT may be at risk of injury (e.g., knee pain)63. There is a need for additional studies to determine the optimal training parameters (e.g., volume, intensity, frequency, and specific exercises) to enhance muscular strength gains and reduce injury risks among older individuals. Another study conducted by Faigenbaum et al.56 demonstrated that incorporating plyometric exercises into a resistance training program proved to be more effective than resistance training alone in enhancing muscular strength. Collectively, our findings suggest that PT could serve as a viable approach for improving muscular strength in untrained populations.
The effect of PT on cardiorespiratory fitness
Cardiorespiratory fitness is commonly acknowledged as essential in preventing heart disease91,92. Improving cardiorespiratory fitness is strongly associated with overall health enhancements93. Findings from research conducted by Azmi et al.94 suggest that maintaining elevated levels of cardiorespiratory fitness in childhood is linked to maintaining a healthy BMI and reducing cardiometabolic risks in adolescence and adulthood. VO2max is widely accepted as the gold standard for assessing cardiorespiratory fitness95 and reflects the maximum rate of oxygen consumption and the physiological processes behind it96. Data on cardiovascular fitness, quantified through VO2max, were available in four of the included studies34,35,36,37. Our meta-analysis identified positive effects of PT on cardiorespiratory fitness. Among the six studies included, two34,37 examined changes in cardiorespiratory fitness among overweight or obese individuals. Racil et al.34 found that 12 weeks of PT coupled with high-intensity intermittent training significantly improved cardiorespiratory fitness in obese female adolescents. Conversely, Nobre et al.37 observed no significant effects of 12 weeks of PT on cardiorespiratory fitness in obese boys. Another study65 demonstrated that a nine-week PT program improved cardiorespiratory fitness in adult males, while Almeida et al.36 reported that a 12-week PT program did not lead to enhanced cardiorespiratory fitness in children. Interestingly, a previous study reported that the training surface can influence the outcomes of PT97. However, one study included in this review, involving plyometric exercises on different surfaces (sand and firm surfaces), suggested that the type of surface did not significantly affect the cardiorespiratory fitness changes induced by the training35.
In the athletic literature, Mazurek et al.10 conducted a study involving young handball players and noted a significant increase in cardiorespiratory fitness after 5 weeks of PT. Similarly, Lum et al.94 recruited endurance runners and observed a significant improvement in cardiorespiratory fitness following 6 weeks of PT. Ramirez-Campillo et al.98 compared the performance of young soccer players before and after an 8-week PT intervention and identified noticeable enhancements in cardiorespiratory fitness. Notably, it appears that PT yields significant changes in cardiorespiratory fitness among both athletic and non-athletic populations. The enhancement of cardiorespiratory fitness could be attributed to the heightened energetic cost associated with performing PT99. Moreover, aerobic training may improve markers of cardiorespiratory fitness (e.g., blood volume, cardiac output) through its beneficial effects on central adaptations. Furthermore, improved cardiorespiratory fitness might result from an increase in mitochondrial content, an activation of adenosine monophosphate-activated protein kinase, and an elevated maximal activity of citrate synthase100,101,102. Overall, the findings from our review supported the notion that PT can effectively enhance cardiorespiratory fitness among untrained individuals.
The effect of PT on flexibility
Flexibility enables a joint to move easily through its entire range of motion and also encompasses a muscular component related to muscle length5. This attribute of flexibility plays a role in injury prevention, posture enhancement, alleviating back pain, and reducing muscle soreness103. Five studies evaluated flexibility using the sit-and-reach tests, which are likely the most widely utilized methods for assessing hamstring and lower back flexibility104. Our findings indicate that PT improves flexibility performance in untrained participants. The improvements in flexibility within the PT group can be attributed to increased excitability of neuromuscular receptors in muscles, tendons, joints, and ligaments16. Specifically, the improved flexibility might be explained by the potential reductions in stiffness within the muscle–tendon complex and similar alterations in the elastic properties of the surrounding joint structures86,105. Moreover, PT can induce changes in the elastic properties of both muscle and connective tissues through motor unit recruitment and the frequency of neural firing. This, in turn, potentiates the reflex arc and leads to increased neuromuscular adaptation17. Furthermore, it reduces the Golgi tendon organs’ responsiveness to excessive tensile loads within the muscles, enabling enhanced stretching of the muscular elastic components16.
These findings align with some studies that have observed statistically significant improvements in flexibility among athletes. De Villarreal et al.106 reported that a 7-week period of PT resulted in increased flexibility among high-school basketball players. Similarly, da Silva et al.107 confirmed the beneficial impact of a 4-week PT regimen on improving flexibility in female Futsal athletes. Furthermore, it is also plausible that participants who frequently engaged in static or dynamic stretching before plyometric exercises may have experienced a beneficial impact on flexibility. Stretching routines increase muscle temperature, activate the nervous system, improve intramuscular coordination, and enhance muscle elasticity108. Overall, the improvement of flexibility in untrained participants after PT is an important finding, because a deficit in this health-related fitness component has been linked to muscle and joint injuries in the lower extremities.
The effect of PT on muscular endurance
Greater muscular endurance can lower the risk of falling and related injuries109,110. However, only one study69 in the current review examined the impact of 12 weeks of PT on muscular endurance in adolescents and reported significant enhancements in this aspect of fitness. This trial69 measured muscular endurance using the sit-up test, which is a safe, cost-effective, and applicable method for evaluating core muscular endurance in both females and males111. As far as our knowledge extends, very limited information is available on this finding, making further elaboration and discussion somewhat challenging. Consequently, we can speculate that PT may enhance the properties of the SSC within the muscles, resulting in improved musculotendinous and neural unit performance, ultimately facilitating maximal force generation in the shortest time14. Such improvements could be associated with enhancements in muscular endurance. However, due to the scarcity of studies addressing this point, further research is imperative before conclusive recommendations can be made.
Limitations
There are a few limitations worth noting in this review. Firstly, due to the scarcity of research for each programming parameter, we did not conduct subgroup analyses on PT variables (e.g., frequency, length, and total sessions) for physical fitness performance measures. Moreover, apart from studies on muscular strength (n = 15), only a small number of studies included in the meta-analysis assess the effects of PT on other fitness indices (n = 5–8). Secondly, none of the studies examined potential confounding factors that could influence the relationship between physical exercise and outcomes (i.e., health-related physical fitness), such as sleep behaviors and dietary habits. Thirdly, according to the GRADE evaluation, the level of certainty in the reported fitness outcomes ranged from very low to moderate, weakening the confidence of these estimates. Finally, the growth and maturation of young participants may affect the overall training effects112. Nevertheless, 11 studies included in this review recruited children or adolescents without providing information about their biological maturity. Despite the limitations mentioned above, our review offers a novel and noteworthy value to the current body of knowledge, shedding light on the efficacy of PT in enhancing health-related physical fitness in untrained populations.
Practical applications
The findings of this study hold practical significance for physical education teachers and practitioners. Firstly, the analysis demonstrates that PT effectively enhances BMI, muscular strength, cardiorespiratory fitness, and flexibility in untrained participants. However, due to limited data, specific training variables for optimizing these aspects of physical fitness cannot be confidently recommended. Generally, the most important considerations when developing PT programs for BMI, muscular strength cardiorespiratory fitness, and flexibility were that effective programs included two to three sessions per week for a minimum of 4 weeks. Secondly, researchers are encouraged to undertake well-designed studies investigating the effects of PT on muscular endurance. The additional studies are crucial to validate further and reinforce the conclusions drawn in this analysis. Thirdly, the utilization of PT is a cost-effective alternative compared to other training strategies, as it requires no or little equipment. Typically, PT involves engaging in drills that utilize the participant’s body weight as a load113. This makes it a convenient and accessible training approach for untrained participants, allowing them to incorporate it into their daily routines easily.
Conclusion
This meta-analysis revealed that PT may be potentially effective in improving health-related physical fitness indices (i.e., body mass index, muscular strength, cardiorespiratory fitness, and flexibility) in untrained participants. However, its effects on body fat percentage and lean muscle mass were not significant. Caution is warranted when interpreting these findings because of data limitations in some fitness variables. Future research should focus on conducting more high-quality studies on PT interventions for health-related physical fitness in untrained populations to provide more reliable evidence for practical applications in this field.
Data availability
Data is provided within the manuscript or Supplementary Information files.
Abbreviations
- PT:
-
Plyometric training
- SSC:
-
Stretch–shortening cycle
- RCTs:
-
Randomized controlled trial studies
- Non-RCTs:
-
Non-randomized controlled trials
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- PROSPERO:
-
International prospective register of systematic reviews
- ROB-2:
-
Risk of bias
- ROBINS-I:
-
In non-randomized research of interventions
- GRADE:
-
Grading of referrals, assessment, develop, and evaluations
- CI:
-
Confidence interval
- ES:
-
Effect size
References
Kariyawasam, A., Ariyasinghe, A., Rajaratnam, A. & Subasinghe, P. Comparative study on skill and health related physical fitness characteristics between national basketball and football players in Sri Lanka. BMC. Res. Notes 12, 1–5. https://doi.org/10.1186/s13104-019-4434-6 (2019).
Cirone, D., Berbrier, D. E., Gibbs, J. C. & Usselman, C. W. Health-related physical fitness in women with polycystic ovary syndrome versus controls: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 309, 1–20. https://doi.org/10.1007/s00404-023-07004-w (2023).
Blair, S. N., Cheng, Y. & Holder, J. S. Is physical activity or physical fitness more important in defining health benefits? Sci. Sport Exerc. 33, S379–S399. https://doi.org/10.1097/00005768-200106001-00007 (2001).
Tomkinson, G. R. et al. European normative values for physical fitness in children and adolescents aged 9–17 years: Results from 2 779 165 Eurofit performances representing 30 countries. Br. J. Sports Med. 52, 1445–1456. https://doi.org/10.1136/bjsports-2017-098253 (2017).
American College of Sports Medicine. Acsm’s Health-Related Physical Fitness Assessment Manual 5th edn. (Lippincott Williams & Wilkins, 2013).
Al-Mallah, M. H., Sakr, S. & Al-Qunaibet, A. Cardiorespiratory fitness and cardiovascular disease prevention: An update. Curr. Atheroscler. Rep. 20, 1–9. https://doi.org/10.1007/s11883-018-0711-4 (2018).
Ezzatvar, Y. et al. Cardiorespiratory fitness measured with cardiopulmonary exercise testing and mortality in patients with cardiovascular disease: A systematic review and meta-analysis. J. Sport Health Sci. 10, 609–619. https://doi.org/10.1016/j.jshs.2021.06.004 (2021).
Kandola, A., Ashdown-Franks, G., Stubbs, B., Osborn, D. P. J. & Hayes, J. F. The association between cardiorespiratory fitness and the incidence of common mental health disorders: A systematic review and meta-analysis. J. Affect. Disord. 257, 748–757. https://doi.org/10.1016/j.jad.2019.07.088 (2019).
Ramirez-Campillo, R. et al. The effects of plyometric jump training on physical fitness attributes in basketball players: A meta-analysis. J. Sport Health Sci. 11, 656–670. https://doi.org/10.1016/j.jshs.2020.12.005 (2021).
Mazurek, K. et al. Effects of short-term plyometric training on physical performance in male handball players. J. Hum. Kinet. 63, 137–148. https://doi.org/10.2478/hukin-2018-0014 (2018).
Moran, J. et al. Effects of vertically and horizontally orientated plyometric training on physical performance: A meta-analytical comparison. Sports Med. 51, 65–79. https://doi.org/10.1007/s40279-020-01340-6 (2021).
Deng, N. et al. Effects of plyometric training on skill and physical performance in healthy tennis players: A systematic review and meta-analysis. Front. Physiol. 13, 3158–3169. https://doi.org/10.3389/fphys.2022.1024418 (2022).
Kons, R. L. et al. Effects of plyometric training on physical performance: An umbrella review. Sports Med.-Open 9, 4. https://doi.org/10.1186/s40798-022-00550-8 (2023).
Sole, C. J., Bellon, C. R. & Beckham, G. K. Plyometric training. In Advanced Strength and Conditioning: An Evidence-Based Approach (eds Turner, A. & Comfort, P.) 307–327 (Routledge, 2022).
Morio, C. et al. Time course of neuro-mechanical changes underlying stretch–shortening cycle during intermittent exhaustive rebound exercise. Eur. J. Appl. Physiol. 111, 2295–2305. https://doi.org/10.1007/s00421-011-1859-6 (2011).
Davies, G., Riemann, B. L. & Manske, R. Current concepts of plyometric exercise. Int. J. Sports Phys. Ther. 10, 760–786 (2015).
Markovic, G. & Mikulic, P. Neuro-musculoskeletal and performance adaptations to lower-extremity plyometric training. Sports Med. 40, 859–895. https://doi.org/10.2165/11318370-000000000-00000 (2010).
Slimani, M., Chamari, K., Miarka, B., Del Vecchio, F. B. & Chéour, F. Effects of plyometric training on physical fitness in team sport athletes: A systematic review. J. Hum. Kinet. 53, 231. https://doi.org/10.1515/hukin-2016-0026 (2016).
Ramirez-Campillo, R. et al. Effects of plyometric jump training on measures of physical fitness and sport-specific performance of water sports athletes: A systematic review with meta-analysis. Sports Med.-Open 8(1), 108. https://doi.org/10.1186/s40798-022-00502-2 (2022).
Deng, N., Soh, K. G., Abdullah, B. & Huang, D. Effects of plyometric training on measures of physical fitness in racket sport athletes: A systematic review and meta-analysis. PeerJ 11, e16638. https://doi.org/10.7717/peerj.16638 (2023).
Ojeda-Aravena, A. et al. A systematic review with meta-analysis on the effects of plyometric-jump training on the physical fitness of combat sport athletes. Sports 11(2), 33. https://doi.org/10.3390/sports11020033 (2023).
Oxfeldt, M., Overgaard, K., Hvid, L. G. & Dalgas, U. Effects of plyometric training on jumping, sprint performance, and lower body muscle strength in healthy adults: A systematic review and meta-analyses. Scand. J. Med. Sci. Sports 29(10), 1453–1465. https://doi.org/10.1111/sms.13487 (2019).
Moran, J., Clark, C. C., Ramirez-Campillo, R., Davies, M. J. & Drury, B. A meta-analysis of plyometric training in female youth: Its efficacy and shortcomings in the literature. J. Strength Cond. Res. 33(7), 1996–2008. https://doi.org/10.1519/JSC.0000000000002768 (2019).
Vetrovsky, T., Steffl, M., Stastny, P. & Tufano, J. J. The efficacy and safety of lower-limb plyometric training in older adults: A systematic review. Sports Med. 49, 113–131. https://doi.org/10.1007/s40279-018-1018-x (2019).
Garcia-Carrillo, E. et al. Effects of upper-body plyometric training on physical fitness in healthy youth and young adult participants: A systematic review with meta-analysis. Sports Med.-Open 9(1), 93. https://doi.org/10.1186/s40798-023-00631-2 (2023).
De Villarreal, E. S., Requena, B. & Newton, R. U. Does plyometric training improve strength performance? A meta-analysis. J. Sci. Med. Sport 13(5), 513–522. https://doi.org/10.1016/j.jsams.2009.08.005 (2010).
Ramirez-Campillo, R. et al. Body composition adaptations to lower-body plyometric training: A systematic review and meta-analysis. Biol. Sport 39, 273–287. https://doi.org/10.5114/BIOLSPORT.2022.104916 (2022).
Bompa, O. T. & Buzzichelli, C. Periodization of Strength Training for Sports 4th edn. (Human Kinetics, 2013).
Goodwin, J. E. & Jeffreys, I. Plyometric training: Theory and practice. In Strength and Conditioning for Sports Performance (eds Goodwin, J. E. & Jeffreys, I.) 346–382 (Routledge, 2016).
Potach, D. H. & Chu, D. A. Program design and technique for plyometric training. In Essentials of Strength Training and Conditioning 4th edn (eds Haff, G. G. & Triplett, N. T.) 471–520 (Human Kinetics, 2015).
Cakar, E. et al. Jumping combined exercise programs reduce fall risk and improve balance and life quality of elderly people who live in a long-term care facility. Eur. J. Phys. Rehabil. Med. 46, 59–67 (2010).
Johnson, B. A., Salzberg, C. L. & Stevenson, D. A. A systematic review: Plyometric training programs for young children. J. Strength Cond. Res. 25, 2623–2633. https://doi.org/10.1519/JSC.0b013e318204caa0 (2011).
Sortwell, A., Newton, M., Marinho, D. A., Ferraz, R. & Perlman, D. The effects of an eight week plyometric-based program on motor performance skills and muscular power in 7–8-year-old primary school students. Int. J. Kinesiol. Sports Sci. 9, 1–12. https://doi.org/10.7575/aiac.ijkss.v.9n.4p.1 (2021).
Racil, G. et al. Plyometric exercise combined with high-intensity interval training improves metabolic abnormalities in young obese females more so than interval training alone. Appl. Physiol. Nutr. Metab. 41, 103–109. https://doi.org/10.1139/apnm-2015-0384 (2015).
Marzouki, H. et al. Effects of surface-type plyometric training on physical fitness in schoolchildren of both sexes: A randomized controlled intervention. Biology 11, 1035. https://doi.org/10.3390/biology11071035 (2022).
Almeida, M. B. D. et al. Plyometric training increases gross motor coordination and associated components of physical fitness in children. Eur. J. Sport Sci. 21, 1263–1272. https://doi.org/10.1080/17461391.2020.1838620 (2021).
Nobre, G. G. et al. Twelve weeks of plyometric training improves motor performance of 7- to 9-year-old boys who were overweight/obese: A randomized controlled intervention. J. Strength Cond. Res. 31, 2091–2099. https://doi.org/10.1519/JSC.0000000000001684 (2017).
Ingle, L., Sleap, M. & Tolfrey, K. The effect of a complex training and detraining programme on selected strength and power variables in early pubertal boys. J. Sports Sci. 24, 987–997. https://doi.org/10.1080/02640410500457117 (2006).
Marín-Cascales, E., Rubio-Arias, J. A., Romero-Arenas, S. & Alcaraz, P. E. Effect of 12 weeks of whole-body vibration versus multi-component training in post-menopausal women. Rejuvenat. Res. 18, 508–516. https://doi.org/10.1089/rej.2015.1681 (2015).
Ozen, S. V. Reproductive hormones and cortisol responses to plyometric training in males. Biol. Sport 29, 193–197. https://doi.org/10.5604/20831862.1003442 (2012).
Gopalakrishnan, S. & Ganeshkumar, P. Systematic reviews and meta-analysis: Understanding the best evidence in primary healthcare. J. Fam. Med. Prim. Care 2(1), 9–14. https://doi.org/10.4103/2249-4863.109934 (2013).
Page, M. J. et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 88, 105906. https://doi.org/10.1016/j.ijsu.2021.105906 (2021).
Amir-Behghadami, M. & Janati, A. Population, intervention, comparison, outcomes and study (PICOS) design as a framework to formulate eligibility criteria in systematic reviews. Emerg. Med. J. 1, 1. https://doi.org/10.1136/emermed-2020-209567 (2020).
Ramirez-Campillo, R. et al. Methodological characteristics and future directions for plyometric jump training research: A scoping review. Sports Med. 48, 1059–1081. https://doi.org/10.1007/s40279-018-0870-z (2018).
Flemyng, E. et al. Using risk of bias 2 to assess results from randomised controlled trials: Guidance from Cochrane. BMJ Evid.-Based Med. 28, 260–266. https://doi.org/10.1136/bmjebm-2022-112102 (2023).
Sterne, J. A. et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355, i4919. https://doi.org/10.1136/bmj.i4919 (2016).
Schünemann, H. J. et al. GRADE guidelines: 21 part 1. Study design, risk of bias, and indirectness in rating the certainty across a body of evidence for test accuracy. J. Clin. Epidemiol. 122, 129–141. https://doi.org/10.1016/j.jclinepi.2019.12.020 (2022).
Ramirez-Campillo, R. et al. Effects of plyometric jump training on the reactive strength index in healthy individuals across the lifespan: A systematic review with meta-analysis. Sports Med. 53, 1029–1053. https://doi.org/10.1007/s40279-023-01825-0 (2023).
Deeks, J. J., Higgins, J. P. & Altman, D. G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions (eds Higgins, J. P. & Green, S.) 243–296 (The Cochrane Collaboration, 2008).
Kontopantelis, E., Springate, D. A. & Reeves, D. A re-analysis of the Cochrane Library data: The dangers of unobserved heterogeneity in meta-analyses. PLoS ONE 8, e69930. https://doi.org/10.1371/journal.pone.0069930 (2013).
Hopkins, W. G., Marshall, S. W., Batterham, A. M. & Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 41, 3–13. https://doi.org/10.1249/MSS.0b013e31818cb278 (2009).
Higgins, J. P., Deeks, J. J. & Altman, D. G. Special topics in statistics. In Cochrane Handbook for Systematic Reviews of Interventions (eds Higgins, J. P. & Green, S.) 481–529 (The Cochrane Collaboration, 2008).
Drevon, D., Fursa, S. R. & Malcolm, A. L. Intercoder reliability and validity of WebPlotDigitizer in extracting graphed data. Behav. Modif. 41, 323–339. https://doi.org/10.1177/0145445516673998 (2016).
Higgins, J. P. & Thompson, S. G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 21, 1539–1558. https://doi.org/10.1002/sim.1186 (2002).
Egger, M., Davey Smith, G., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 315, 629–634. https://doi.org/10.1136/bmj.315.7109.629 (1997).
Faigenbaum, A. D. et al. Effects of a short-term plyometric and resistance training program on fitness performance in boys age 12 to 15 years. J. Sports Sci. Med. 6, 519–525 (2007).
Faigenbaum, A. D. et al. “Plyo play”: A novel program of short bouts of moderate and high. Phys. Educ. Winter 66(1), 37 (2009).
Tsang, K. & DiPasquale, A. Improving the Q: H strength ratio in women using plyometric exercises. J. Strength Cond. Res. 25, 2740–2745. https://doi.org/10.1519/JSC.0b013e31820d9e95 (2011).
Park, J., Cho, K. & Lee, W. Effect of jumping exercise on muscle strength and balance of elderly people: A randomized controlled trial. J. Phys. Ther. Sci. 24, 1345–1348. https://doi.org/10.1589/jpts.24.1345 (2012).
Chaouachi, A., Othman, A. B., Hammami, R., Drinkwater, E. J. & Behm, D. G. The combination of plyometric and balance training improves sprint and shuttle run performances more often than plyometric-only training with children. J. Strength Cond. Res. 28, 401–412. https://doi.org/10.1519/JSC.0b013e3182987059 (2014).
Marín-Cascales, E., Alcaraz, P. E. & Rubio-Arias, J. A. Effects of 24 weeks of whole body vibration versus multicomponent training on muscle strength and body composition in postmenopausal women: A randomized controlled trial. Rejuvenat. Res. 20, 193–201. https://doi.org/10.1089/rej.2016.1877 (2017).
Qi, F. et al. Effects of combined training on physical fitness and anthropometric measures among boys aged 8 to 12 years in the physical education setting. Sustainability 11(5), 51219. https://doi.org/10.3390/su11051219 (2019).
van Roie, E. et al. An age-adapted plyometric exercise program improves dynamic strength, jump performance and functional capacity in older men either similarly or more than traditional resistance training. PLoS ONE 15, 1–22. https://doi.org/10.1371/journal.pone.0237921 (2020).
Radwan, N. L., Mahmoud, W. S., Mohamed, R. A. & Ibrahim, M. M. Effect of adding plyometric training to physical education sessions on specific biomechanical parameters in primary school girls. J. Musculoskel. Neuronal Interact. 21, 237–246 (2021).
Singh, G. et al. Effects of sand-based plyometric-jump training in combination with endurance running on outdoor or treadmill surface on physical fitness in young adult males. J. Sports Sci. Med. 21(2), 277–286. https://doi.org/10.52082/jssm.2022.277 (2022).
Bulqini, A., Widodo, A., Muhammad, H. N., Putera, S. H. P. & Sholikhah, A. M. A. Plyometric hurdle jump training using beach sand media increases power and muscle strength in young adult males. Phys. Educ. Theory Methodol. 23, 531–536. https://doi.org/10.17309/tmfv.2023.4.06 (2023).
Witzke, K. A. & Snow, C. M. Effects of plyometric jump training on bone mass in adolescent girls. Med. Sci. Sports Exerc. 32, 1051–1057. https://doi.org/10.1097/00005768-200006000-00003 (2000).
Villada, J. F. R., León Ariza, H. H., Jiménez, A. S. & Sepúlveda, C. M. Alterations in body composition, capillary glucose and functionality during explosive strength training in older women. Int. J. Disabil. Hum. Dev. 15, 251–259. https://doi.org/10.1515/ijdhd-2015-0011 (2016).
Thaqi, A., Berisha, M. & Hoxha, S. The effect of plyometric training on the power-related factors of children aged 16 years-old. Prog. Nutr. 22, e2020004. https://doi.org/10.2751/pn.v22i2-S.10441 (2020).
Willoughby, D., Hewlings, S. & Kalman, D. Body composition changes in weight loss: Strategies and supplementation for maintaining lean body mass, a brief review. Nutrients 10, 1876. https://doi.org/10.3390/nu10121876 (2018).
Shim, A., Cross, P., Norman, S. & Hauer, P. Assessing various body composition measurements as an appropriate tool for estimating body fat in National Collegiate Athletic Association Division I female collegiate athletes. Am. J. Sports Sci. Med. 2(1), 1–5. https://doi.org/10.12691/ajssm-2-1-1 (2014).
Merrigan, J. et al. Reliability and validity of contemporary bioelectrical impedance analysis devices for body composition assessment. J. Exerc. Nutr. 5(4), 103133. https://doi.org/10.53520/jen2022.103133 (2022).
Fonseca, D. C. et al. Body weight control and energy expenditure. Clin. Nutr. Exp. 20, 55–59. https://doi.org/10.1016/j.yclnex.2018.04.001 (2018).
Barillas, S. R. et al. Repeated plyometric exercise attenuates blood glucose in healthy adults. Int. J. Exerc. Sci. 10(7), 1076 (2017).
Monti, E. et al. The time-course of changes in muscle mass, architecture and power during 6 weeks of plyometric training. Front. Physiol. 11, 567299. https://doi.org/10.3389/fphys.2020.00946 (2020).
Campo, S. S. et al. Effects of lower-limb plyometric training on body composition, explosive strength, and kicking speed in female soccer players. J. Strength Cond. Res. 23, 1714–1722. https://doi.org/10.1519/JSC.0b013e3181b3f537 (2009).
Aloui, G. et al. Effects of elastic band plyometric training on physical performance of team handball players. Appl. Sci. 11, 1309. https://doi.org/10.3390/app11031309 (2021).
Oliveira, A., Monteiro, A., Jacome, C., Afreixo, V. & Marques, A. Effects of group sports on health-related physical fitness of overweight youth: A systematic review and meta-analysis. Scand. J. Med. Sci. Sports 27, 604–611. https://doi.org/10.1111/sms.12784 (2017).
Miller, T., Mull, S., Aragon, A. A., Krieger, J. & Schoenfeld, B. J. Resistance training combined with diet decreases body fat while preserving lean mass independent of resting metabolic rate: A randomized trial. Int. J. Sport Nutr. Exerc. Metab. 28(1), 46–54. https://doi.org/10.1123/ijsnem.2017-0221 (2018).
Benito, P. J. et al. Strength plus endurance training and individualized diet reduce fat mass in overweight subjects: A randomized clinical trial. Int. J. Environ. Res. Public Health 17(7), 2596. https://doi.org/10.3390/ijerph17072596 (2020).
Kotarsky, C. J. et al. Time-restricted eating and concurrent exercise training reduces fat mass and increases lean mass in overweight and obese adults. Physiol. Rep. 9(10), e14868. https://doi.org/10.14814/phy2.14868 (2021).
Willis, L. H. et al. Effects of aerobic and/or resistance training on body mass and fat mass in overweight or obese adults. J. Appl. Physiol. 113(12), 1831–1837. https://doi.org/10.1152/japplphysiol.01370.2011 (2012).
Collins, H., Fawkner, S., Booth, J. N. & Duncan, A. The effect of resistance training interventions on weight status in youth: A meta-analysis. Sports Med. Open 4, 41. https://doi.org/10.1186/s40798-018-0154-z (2018).
Carroll, T. J., Riek, S. & Carson, R. G. Neural adaptations to resistance training: Implications for movement control. Sports Med. 31, 829–840. https://doi.org/10.2165/00007256-200131120-00001 (2001).
Grgic, J. et al. Effect of resistance training frequency on gains in muscular strength: A systematic review and meta-analysis. Sports Med. 48, 1207–1220. https://doi.org/10.1007/s40279-018-0872-x (2018).
Turner, A. N. & Jeffreys, I. The stretch-shortening cycle: Proposed mechanisms and methods for enhancement. Strength Cond. J. 32, 87–99. https://doi.org/10.1519/SSC.0b013e3181e928f9 (2010).
Grgic, J., Schoenfeld, B. J. & Mikulic, P. Effects of plyometric vs resistance training on skeletal muscle hypertrophy: A review. J. Sport Health Sci. 10, 530–536. https://doi.org/10.1016/j.jshs.2020.06.010 (2020).
De Ste Croix, M. B., Deighan, M. A. & Armstrong, N. Assessment and interpretation of isokinetic muscular strength during growth and maturation. Sports Med. 33, 727–743. https://doi.org/10.2165/00007256-200333100-00002 (2003).
Radnor, J. M., Oliver, J. L., Waugh, C. M., Myer, G. D. & Lloyd, R. S. The influence of maturity status on muscle architecture in school-aged boys. Pediatr. Exerc. Sci. 32, 89–96. https://doi.org/10.1123/pes.2019-0201 (2020).
Peterson, M. D., Rhea, M. R., Sen, A. & Gordon, P. M. Resistance exercise for muscular strength in older adults: A meta-analysis. Ageing Res. Rev. 9(3), 226–237 (2010).
Myers, J., Kokkinos, P. & Nyelin, E. Physical activity, cardiorespiratory fitness, and the metabolic syndrome. Nutrients 11, 1652. https://doi.org/10.3390/nu11071652 (2019).
Lindgren, M. & Börjesson, M. The importance of physical activity and cardiorespiratory fitness for patients with heart failure. Diabetes Res. Clin. Pract. 176, 108833. https://doi.org/10.1016/j.diabres.2021.108833 (2021).
Azmi, N. A., Zaki, N. T. A., Kong, M. C., Ab Rahman, N. N. A. & Zanudin, A. Correlation of physical activity level with physical fitness and respiratory function amongst undergraduates. Trends Sci. 18, 24. https://doi.org/10.48048/tis.2021.24 (2021).
Lum, D., Barbosa, T. M., Aziz, A. R. & Balasekaran, G. Effects of isometric strength and plyometric training on running performance: A randomized controlled study. Res. Q. Exerc. Sport 94, 263–271. https://doi.org/10.1080/02701367.2021.1969330 (2023).
Ross, R. et al. Importance of assessing cardiorespiratory fitness in clinical practice: A case for fitness as a clinical vital sign: A scientific statement from the American Heart Association. Circulation 134, e653–e699. https://doi.org/10.1161/CIR.0000000000000461 (2016).
Green, S. & Askew, C. VO2peak is an acceptable estimate of cardiorespiratory fitness but not VO2max. J. Appl. Physiol. 125(1), 229–232. https://doi.org/10.1152/japplphysiol.00850.2017 (2018).
Buga, S. & Gencer, Y. G. The effect of plyometric training performed on different surfaces on some performance parameters. Prog. Nutr. 24, e2022072. https://doi.org/10.23751/pn.v24iS1.13014 (2022).
Ramirez-Campillo, R. et al. Effect of unilateral, bilateral, and combined plyometric training on explosive and endurance performance of young soccer players. J. Strength Cond. Res. 29, 1317–1328. https://doi.org/10.1519/JSC.0000000000000762 (2015).
Berryman, N., Maurel, D. & Bosquet, L. Effect of plyometric vs dynamic weight training on the energy cost of running. J. Strength Cond. Res. 24(7), 1818–1825. https://doi.org/10.1519/JSC.0b013e3181def1f5 (2010).
Gibala, M. J., Gillen, J. B. & Percival, M. E. Physiological and health-related adaptations to low-volume interval training: Influences of nutrition and sex. Sports Med. 44, 127–137. https://doi.org/10.1007/s40279-014-0259-6 (2014).
Gidlund, E. K. Exercise and the mitochondria. In Cardiorespiratory Fitness in Cardiometabolic Diseases (eds Kokkinos, P. & Narayan, P.) (Springer, 2019).
Lin, X. et al. Effects of exercise training on cardiorespiratory fitness and biomarkers of cardiometabolic health: A systematic review and meta-analysis of randomized controlled trials. J. Am. Heart Assoc. 4(7), e002014. https://doi.org/10.1161/JAHA.115.002014 (2015).
Thompson, D. L. Fitness focus copy-and-share: Flexibility. ACSMs Health Fit J. 12, 5. https://doi.org/10.1249/FIT.0b013e318184516b (2008).
Ayala, F., de Baranda, P. S., Croix, M. D. S. & Santonja, F. Criterion-related validity of four clinical tests used to measure hamstring flexibility in professional futsal players. Phys. Ther. Sport 12(4), 175–181. https://doi.org/10.1016/j.ptsp.2011.02.005 (2011).
Ramírez-delaCruz, M., Bravo-Sánchez, A., Esteban-García, P., Jiménez, F. & Abián-Vicén, J. Effects of plyometric training on lower body muscle architecture, tendon structure, stiffness and physical performance: A systematic review and meta-analysis. Sports Med.-Open 8, 40. https://doi.org/10.1186/s40798-022-00431-0 (2022).
de Villarreal, E. S., Molina, J. G., de Castro-Maqueda, G. & Gutiérrez-Manzanedo, J. V. Effects of plyometric, strength and change of direction training on high-school basketball player’s physical fitness. J. Hum. Kinet. 78, 175–186. https://doi.org/10.2478/hukin-2021-0036 (2021).
da Silva, N. V. F. et al. Effects of short-term plyometric training on physical fitness parameters in female futsal athletes. J. Phys. Ther. Sci. 29, 783–788. https://doi.org/10.1589/jpts.29.783 (2017).
Deng, N. et al. Effects of combined upper and lower limb plyometric training interventions on physical fitness in athletes: A systematic review with meta-analysis. Int. J. Environ. Res. Public Health 20, 482. https://doi.org/10.3390/ijerph20010482 (2023).
Kell, R. T., Bell, G. & Quinney, A. Musculoskeletal fitness, health outcomes and quality of life. Sports Med. 31, 863–873. https://doi.org/10.2165/00007256-200131120-00003 (2001).
Ambegaonkar, J. P., Caswell, S. V., Winchester, J. B., Caswell, A. A. & Andre, M. J. Upper-body muscular endurance in female university-level modern dancers: A pilot study. J. Dance Med. Sci. 16, 3–7. https://doi.org/10.1177/1089313X1201600101 (2012).
Bianco, A. et al. The sit up test to exhaustion as a test for muscular endurance evaluation. Springerplus 4, 309. https://doi.org/10.1186/s40064-015-1023-6 (2015).
Ford, P. et al. Participant development in sport and physical activity: The impact of biological maturation. Eur. J. Sport Sci. 12, 515–526. https://doi.org/10.1080/17461391.2011.577241 (2012).
Ramirez-Campillo, R. et al. Effects of plyometric jump training on vertical jump height of volleyball players: A systematic review with meta-analysis of randomized-controlled trial. J. Sports Sci. Med. 19, 489–499. https://doi.org/10.25932/publishup-52589 (2020).
Author information
Authors and Affiliations
Contributions
N.D. wrote the first draft of the manuscript. N.D., D.H., and K.G.S. collected data. N.D., D.H., F.X. and K.G.S analyzed and interpreted the data. K.G.S., B.B.A., M.B., and D.Z revised the original manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Deng, N., Soh, K.G., Abdullah, B.B. et al. Effects of plyometric training on health-related physical fitness in untrained participants: a systematic review and meta-analysis. Sci Rep 14, 11272 (2024). https://doi.org/10.1038/s41598-024-61905-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-61905-7
- Springer Nature Limited