
Abstract
Managed colonies of the European honey bee, Apis mellifera, have faced considerable losses in recent years. A widespread contributing factor is a microsporidian pathogen, Nosema ceranae, which occurs worldwide, is increasingly resistant to antibiotic treatment, and can alter the host’s immune response and nutritional uptake. These obligate gut pathogens share their environment with a natural honey bee microbiome whose composition can affect pathogen resistance. We tested the effect of N. ceranae infection on this microbiome by feeding 5 day-old adult bees that had natural, fully developed microbiomes with live N. ceranae spores (40,000 per bee) or a sham inoculation, sterile 2.0 M sucrose solution. We caged and reared these bees in a controlled lab environment and tracked their mortality over 12 d, after which we dissected them, measured their infection levels (gut spore counts), and analyzed their microbiomes. Bees fed live spores had two-fold higher mortality by 12 d and 36.5-fold more spores per bee than controls. There were also strong colony effects on infection levels, and 9% of spore-inoculated bees had no spore counts at all (defined as fed-spores-but-not-infected). Nosema ceranae infection had significant but subtle effects on the gut microbiomes of experimentally infected bees, bees with different infection levels, and fed-spores-but-not-infected vs. bees with gut spores. Specific bacteria, including Gilliamella ASVs, were positively associated with infection, indicating that multiple strains of core gut microbes either facilitate or resist N. ceranae infection. Future studies on the interactions between bacterial, pathogen, and host genotypes would be illuminating.
Similar content being viewed by others

Introduction
Animal pollination services play a significant role in global food crop production, contributing about 35% of the total production1,2. About 75% of the world's food crops are at least partially dependent on insect pollination 3, with wild insects, including native bee species, making meaningful contributions4. However, commercial honey bees, such as the European honey bee A. mellifera, are crucial for the successful pollination of many crops. The estimated yearly value of commercial A. mellifera colonies as pollinators is between $12.3 and $16.4 billion in the U.S. alone5. The demand for commercial European honey bees as pollinators has increased as the proportion of pollinator-dependent crops in agriculture has tripled over the past 50 years6. Colony losses have also been observed globally to a degree that is not normal, pointing to poor overall health7. Contributing factors include migratory beekeeping, poor nutrition, infestations with Varroa destructor, and pathogens such as Nosema ceranae, which have received particular attention8,9. Interactions between these factors, such as pesticide exposure increasing susceptibility to Varroa destructor and N. ceranae, have proven problematic8, 10.
One particular pathogen, N. ceranae, has infected between 46–63% of honey bees sampled in different studies conducted around the world11,12,13,14. A new genus name was proposed for this pathogen, Vairimorpha ceranae 15, but we will use the name, N. ceranae, based upon more recent literature (Bartolome et al., 2024). This microsporidian originated from the Asian honey bee (Apis cerana) and has since been found to infect other honey bee species, including Apis mellifera, Apis florea, and Apis dorsata16. Within A. mellifera, the invasive N. ceranae has surpassed the endemic pathogen, Nosema apis, in terms of distribution and infectivity 17,18,19. In France, some colonies have been found to contain eight times more N. ceranae than N. apis20, likely due to commercial trade in infected A. mellifera colonies21. Our research therefore focused on N. ceranae.
Nosema ceranae infection has multiple effects including suppressed immune response, digestive tissue degeneration, and premature mortality22,23,24. Infection can also modify pheromones essential for normal worker behavior, reduce brood rearing, and induce earlier foraging activity 24,25,26. These effects reduce colony fitness27, and N. ceranae can thus significantly decrease the survival of colonies in poor health, particularly in conjunction with other factors such as insecticide exposure10,28,29. In general, many of N. ceranae’s effects seem to manifest in the bee gut. Infected bees exhibit modified behaviors such as increased sucrose consumption and lower tendencies to share food30. Infected midgut cells also have a reduced ability to absorb nutrients23. Because N. ceranae exclusively infects the bee gut, it should have a strong effect on the gut microbiome31,32,33.
Globally, the microbiome of western honey bees has the same nine bacterial types34,35. This microbiome is colonized and matures approximately 5 d after adult emergence36. These microbes contain genes that are involved in host immune response, metabolism, growth, and development35,37,38. Honey bee specific microbes and N. ceranae co-occur abundantly in the midgut and hindgut 36,39. Researchers are increasingly focused on these interactions. Pollen patties inoculated with honey bee gut bacterium, Parasaccharibacter apium, lowered Nosema levels in workers that were challenged with Nosema40. Inoculation with Bifidobacterium and Lactobacillus strains isolated from the bee gut also reduced N. ceranae infection levels41. However, some studies have shown that an imbalance of microbiota composition (dysbiosis), induced via bacterial inoculation, can increase mortality and susceptibility to parasites such as Nosema 35,42,43,44,45. Understanding how N. ceranae infection alters the gut microbiome therefore has implications for developing treatments to combat the effects of infection and dysbiosis.
Feeding workers the same dose of live N. ceranae spores can lead to markedly different infection outcomes, with some bees having no spores at all in their gut while others can have infections exceeding one million gut spores32,46,47. Studies have identified significant variation based on colony identity, suggesting either that genetic background, the microbiome, or multiple factors may be involved32,47. We hypothesized that the gut microbiome may play an important factor in the ability of individual bees to resist N. ceranae infection. We, therefore, conducted a screening experiment in which we fed recently emerged honey bees with the same dose of live N. ceranae spores, divided the resulting bees into different groups based on their level of subsequent infection as measured by midgut spore counts, and analyzed their microbiomes. We note that changes in microbiome composition may reflect the outcome of infection, not initial conditions that helped bees resist infection. It is not possible to sample the microbiome of a living bee before and after infection. However, the information obtained after infection is still informative because we know relatively little about the association between N. ceranae infection and the bee microbiome.
Materials and Methods
Study site and colonies
We conducted our experiment on 15 Apis mellifera ligustica colonies at the Biology Field Station (32°53′07.9″N 117°13′55.1″W) apiary at the University of California San Diego. All colonies were healthy, based on standard inspection techniques48. Before being used for our experiments, we randomly sampled foragers (bees with pollen on their legs) returning to the colonies and dissected out 10 bees per colony to check for potential N. ceranae infections. None of the bees sampled had any gut spores.
General methods
Collection of recently emerged bees
To obtain recently emerged bees, we first took out a frame from one of the colonies and located a large patch of capped worker brood. Using a brush, we carefully removed all the adult worker bees from the area and then used a corner of a hive tool to gently lift the caps off the worker broods to reveal the developing pupae. We selected pupae with deep purple eyes, which indicate they are close to eclosion. Then, we placed a sterile wire cage (5 × 7.5x2.5 cm) around the pupae and carefully pushed it into the wax to keep all sides even and tight. After putting the frame back in its original slot in the colony, we checked the cage every 24 h for adult emergence. Once the bees had emerged, they remained inside their colonies, confined within their wire cages and we waited 5 days to collect them, as honey bee workers need to develop their characteristic microbiome through food exchange and grooming with adult workers. After 5 days, we removed the frame, brushed off any other bees, and placed two sterile plastic cages (11.5 × 11.5x9 cm) on a table, facing upward with their sliding doors open. Holding the frame over the plastic cages with the wire cage closest to the opening, we removed the wire cage from the frame and quickly brushed the bees into the plastic cages. Then, we closed the cages with the sliding door.
Spore preparation and counting
We prepared fresh N. ceranae spores which consisted of standard extraction and purification of spores at room temperature from heavily infected bees less than 12 h before they were fed to bees46. We followed the standard procedure for measuring infection levels, using a hemocytometer to count the number of spores per bee49. We used PCR analysis to confirm that the spores were N. ceranae (see methods of46).
Feeding recently emerged bees with Nosema ceranae
After obtaining the bees, we divided them into two groups: a control group (each bee received a 5 µl dose of sterile 2.0 M sucrose solution) and an experimental group (each bee received 40,000 spores in 5 µl of sterile 2.0 M sucrose solution, chosen because it effectively infects bees,46). To feed the bees, we placed them in individual, sterile vials and inserted a micropipette tip filled with the appropriate treatment into the vial lid. We positioned the vials in a tray beneath LED lights (SMD 3528, 240 lumens/m) to encourage feeding32. If the bees did not consume all of the solution within 30–60 min, we manually fed them the remaining solution to ensure that each bee received the same dose. After they finished feeding, we placed 25 bees in each cage, with all bees in the same cage receiving the same treatment. To keep the bees alive during the experiment, we placed a 5 ml syringe filled with approximately 3 ml of 2.0 M sterile sucrose solution in each plastic cage and returned the cages to the incubator.
Gut dissection and Nosema ceranae extraction
We maintained the bees in the cages inside a dark incubator set to the standard conditions of 34 °C and 70% relative humidity for caged adult worker bees50. Every 2 days, we monitored the bees, refilled their sucrose solution, recorded any mortality, and removed any dead bees.
After 12 days, chosen because the spores should fully mature by then (Fries et al., 2013), we placed all surviving bees in individual microcentrifuge tubes on ice for 10–15 min and then dissected them. For each bee, we swiftly removed the midgut and rectum, as the midgut is the main location of N. ceranae39 and the rectum holds the majority of the gut microbiome36. We placed the gut and rectum into a microcentrifuge tube containing 100 µl of bee gut extraction buffer, which was chilled and homogenized using a Kontes motorized pestle for 30 s. Each liter of bee gut extraction buffer, with a pH of 7.4, contained 1.45 mM NaCl, 0.02 g Peptone, and 500 µl Tween 20. The buffer was sterilized through autoclaving. We then transferred 30 µl of the homogenized gut solution to a separate microcentrifuge tube for microbiome analysis and preserved a part of the sample for future culturing by transferring another 30 µl of the original gut solution to a third tube with 30 µl of 30% reagent grade glycerol, which was then vortexed. To avoid contamination, for each bee, we used a different set of dissection tools, a different pestle, and a different microcentrifuge tube. Before use, all tools and pestles were thoroughly sanitized by washing with lab detergent, rinsed with 100% ethanol, rinsed multiple times with deionized water, and then autoclaved. All pipette tips were discarded after one use. All samples were kept on ice at all times and were stored at − 70 °C to prevent microbiome degradation.
Characterizing microbiota composition
The gut samples (midgut and hindgut) of bees from 10 randomly selected colonies (out of the 16 that we used) were collected and transferred to sterile 96-well sample extraction plates from the DNeasy extraction kit provided by Qiagen (Valencia, CA). To extract DNA, 50 μL of a mixture of 0.1 mm glass beads and two sterile 3.2 mm steel beads were added to each well. The samples were lysed by adding 180 μL of buffer ATL (Qiagen, Valencia, CA) to each well, then subjected to bead beating using a Tissue Lyser (Qiagen, Valencia, CA) for six minutes at 30 Hz. Twenty μL of proteinase K was added to each sample and incubated overnight at 56 °C. The extraction was completed following the protocol recommended by the DNeasy Blood and Tissue kit (Qiagen, Valencia, CA).
To determine the composition of the microbiota, we utilized established protocols to conduct 16S rRNA gene analysis. For the PCR reactions, we used the 799F (CMGGGTATCTAATCCKGTT) and 1115R (AGGGTTGCGCTCGTTG) primers that target the V5 and V6 regions of the 16S rRNA gene and excluded plastid regions32,51,52. The sequencing construct was built using a dual barcoding approach with two primer sets53,54. The PCR reactions were cleaned using the PureLink Pro PCR Clean-Up Kit (ThermoFisher Scientific, Waltham, MA), then each sample was normalized to an equal molarity using SequalPrep normalization plates (ThermoFisher Scientific, Waltham, MA) and finally, the reactions were pooled and sequenced with a 2 × 300 bp paired-end run using V3 reagents on the Illumina MiSeq platform.
Statistics and bioinformatic analyses
To determine the effects of treatment on spore levels, we used Analysis of Variance (ANOVA) with log-transformed spore counts (after inspecting model residuals) as our response variable and used colony identity, treatment, and the interaction colony x treatment as fixed effects. Cage name was a random effect nested within colony. Colony identity was a fixed effect because we explicitly wished to test the hypothesis that colonies varied. Although these data are counts, the measurement per bee ranged from 0 to over 41 million in increments of 5000 and therefore closely approximated a continuous variable suitable for ANOVA. We used JMP Pro v14.3.0.
To test if the proportion of surviving bees and treatment affected the mean spore count per bee in a cage, we used a Mixed Model (REML algorithm), calculated the proportion of surviving bees (number of living bees at the end of a trial/number of bees at the beginning of the trial), and tested if the proportion of surviving bees, treatment, and their interaction explained variation in the log-transformed average spore counts per bee. In this analysis, each cage was an individual data point, and colony was a random variable. We used JMP Pro v14.3.0.
To determine the effects of treatment (control bees that were not fed spores vs. experimental bees that were fed spores) upon survival, we first used a simple Kaplan–Meier survival model without colony, and then ran a Proportional Hazards Survival model with censoring and colony, treatment, and the interaction colony x treatment as fixed effects. We report model results as Effect Likelihood Ratio tests (L-R chi-square tests). We used JMP Pro v14.3.0 and reported a mean ± 1 standard error. To test the effects of treatment and average mortality per cage after 12 days on the log-transformed average spore counts per surviving bee per cage, we ran a Mixed Model (REML algorithm) with colony as a random effect and the interaction of average mortality per cage x treatment. When interactions were not significant, we eliminated them and reported the results of the reduced model.
To look at the influences of treatment on the microbiome, we processed the 16S rRNA gene data using QIIME2 version 2017–1149. We evaluated the quality scores of the DNA sequence and removed low-quality regions and chimeras, using the default parameters of DADA251. We then assigned taxonomy to each amplicon sequence variant (ASV) through two methods: (1) by training the Silva database (v. 12852) with our primer set in QIIME2 and using the sklearn classifier53 and (2) using NCBI’s 16S rRNA database to conduct local BLAST searches and pull out the taxonomy of the top hit, the top hit’s accession number, and the percent identity of the query to the top hit.
The statistical analyses were conducted with R version 4.03. We removed 18 contaminants that were present in our blanks with the R-package decontam (ver 1.10.0), using a conservative threshold of 0.5. We also filtered out mitochondria or chloroplasts in QIIME2. To normalize the number of sequences per library, we ran alpha-rarefaction in QIIME2 and selected 2500 reads per sample to retain most samples while still capturing the majority of the diversity of the samples (Fig. S1). This rarified feature table was then analyzed further with the R vegan package (ver 2.5–7).
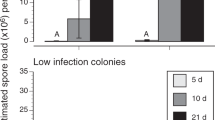
We measured alpha and beta diversity to look at differences between (1) uninfected bees versus infected bees and (2) the level of infections divided into four factor levels based on quartiles of the spore load data in bees whose microbiomes we analyzed: control bees that were never fed spores and had zero spores (control bees), bees with spore counts below the median spore count value (low spore count bees), bees with spore count ranging from the median to the 75th quartile (moderate spore count bees), and bees with spores above the 75th quartile (high spore count bees). We based our quartile levels on bees whose microbiomes we analyzed (Table S1) because the main purpose of creating different infection levels was to understand our microbiome results in greater detail. However, for consistency, we applied these same quartiles to the infection data for all bees (Table S1, Fig. 1).

Spore counts and survival in control bees (fed no spores in sucrose solution) and experimental bees (fed spores in sucrose solution) after 12 days are shown. (A) N. ceranae infection levels were classified into four groups: fed-spores-but-not-infected bees with no spore counts and low, moderate, and high spore count bees (low=spore counts<median, moderate=median to 75th quartile, high=>75th quartile, see Table S1). (B) Survival plot showing that experimental bees had lower survival than control bees (see Results, P < 0.0001). (C) There is no relationship between mean mortality per cage and mean spores per bee per cage. However, experimental bees had significantly higher spore counts than control bees (spline lines and 95% confidence intervals shown as shaded areas).
We also compared (3) bees that were given the sham treatment (control bees fed only pure sucrose without spores) and bees that were fed spores but subsequently had no gut spores (fed-spores-but-not-infected bees). To evaluate beta diversity, we created Bray–Curtis dissimilarities matrices and performed nonmetric multidimensional scaling using metamds in vegan. We used vegan betadisp to test for homogeneity of multivariate dispersions and treated colony identity as a block. The results were visualized with ordiellipse, where the ellipses represent 95% confidence intervals.
To look at alpha diversity we ran two linear mixed-effect models using the lme4 package in R (ver. 1.1.27.1) and one linear model. The response variable for all three models was the number of ASVs in the bees and the predictor variable was the treatments described above. For our analyses of (1) control versus treatment and (2) levels of infection, we used colony and cage numbers as random effects and ran linear mixed effects models. We could not use random effects in our (3) resistance model because it violated model assumptions, so we ran a simple linear model. Model assumptions were tested with the DHARMa package in R (ver 0.4.3). To determine the statistical significance of the two linear mixed effects models, we conducted Type II Wald chi-square tests. We used ancom in QIIME2 to test for ASVs that were differentially abundant between the microbiomes of the treatment groups. We used vegan’s betadisper function to compare dispersion between groups. Lastly, we used the phyloseq package in R for bacterial profiling/plotting the relative abundance of bacterial taxa.
Results
Effects of treatment on survival and spore counts
The outcome of being fed live spores varied among the bees, depending on their colony background (Fig. 1A). The highest spore count, 12 days after bees were fed live spores, was 41,400,000. Out of the 506 control bees that were not fed any spores, only 8% had any spores (22,024 ± 20,063 spores/bee in bees with any spores). Out of the 497 bees that were fed live N. ceranae spores, only 9% were not infected (0 spore counts, defined as “fed-spores-but-not-infected”).
Our model accounted for 83% of the variance in spore count. There were significant differences between the treatment groups (control bees that were not fed spores vs. experimental bees that were fed spores: F1,37 = 464.18, P < 0.0001) and colonies (F15,38 = 2.20, P = 0.026), and no significant treatment x colony interaction (although this interaction was close to significant, F15,23 = 2.06, P = 0.06). Cage was also a significant effect (Wald P value = 0.0001) and accounted for 30% of model variance.
Out of the 15 colonies, 42.9% of bees fed N. ceranae spores died prior to day 12, while only 22.5% of control bees died in the same time frame. In the simple survival model that only tested the effects of treatment on survival, bees fed spores had significantly lower survival than bees fed sucrose only (L-R Chi-square = 46.24, 1 df, P < 0.0001, Fig. 1B). However, in the Proportional Hazards model that included colony identity as a factor, survival depended upon colony background. This model showed no significant differences in treatment (L-R Chi-square = 2.90 × 10–6, 1 df, P = 0.9986), because survival strongly depended on source colony (L-R Chi-square = 122.54, 14 df, P < 0.0001), as shown by the significant interaction between colony and treatment (L-R Chi-square = 31.90, 14 df, P = 0.004). For seven colonies, the mortality rate was significantly higher in the experimental bees compared to the control bees (L-R Chi-square ≥ 4.13, 1 df, P ≤ 0.04), while in the remaining eight colonies, there were no significant differences in mortality between the two treatments (L-R Chi-square ≤ 3.50, 1 df, P ≥ 0.06). In the eight colonies where feeding bees spores significantly reduced their survival, the experimental survival proportion at day 12 was 0.45 ± 0.03 (mean ± 1 SE). In contrast, in the seven colonies where survival was not significantly reduced, the experimental survival proportion at day 12 was 0.64 ± 0.02.
We also tested if average survival per cage and treatment could predict the average spore count per bee per cage. Our model accounted for 76% of the variance in spore counts. Treatment significantly predicted the average spore count per bee per cage (F1,33 = 149.80, P < 0.0001), and there was a significant effect of survival (F1,10 = 5.80, P = 0.038, Fig. 1C). The interaction between average survival and treatment (F1,35 = 2.93, P = 0.10) was not significant. Colony (a random effect) accounted for < 1% of the variance in this model. Essentially, control bees had almost no spores, and experimental bees were highly infected such that cages in which a higher proportion of bees survived during the 12-day trial had a higher average spore count.
Effects of spore treatment on microbiome composition
The beta diversity between the microbiomes of treatment and control bees was significantly different (F1,228 = 4.43, P < 0.001, R2 = 0.019). The overall beta dispersion between treatment and control bees was not significant (F 1,228 = 6.27, P = 0.13). However, beta dispersion of the microbiome was significantly different between the different infection groups (F3,142 = 3.61, P = 0.048). Pairwise comparisons of beta dispersion for the different groups revealed a significant difference between the fed-spores-but-not-infected bees and the high spore count bees (P = 0.05) and significant differences between the median spore count bees and fed-spores-but-not-infected vs. median spore count bees (P = 0.002) and low vs. median spore count bees (P = 0.028, Fig. 2).

Microbial community compositions are shown. (A) Control bees were fed no spores, only the sucrose solution, and experimental bees were each fed 40,000 spores in sucrose solution. (B) N. ceranae infection levels were classified into four groups: fed-spores-but-not-infected bees with no spore counts and low, moderate, and high spore count bees (based upon quartiles, see Table S1). (C) Both control and fed-spores-but-not-infected bees had no spore counts, but beta diversity (P = 0.002) and beta dispersion (P = 0.001) were significantly different between these two groups of bees. The ellipses show 95% confidence intervals per group.
Concerning infection levels, beta diversity was significantly different between the infection groups (F3,142 = l 0.99, P = 0.03, R2 = 0.04). In pairwise comparisons, all of the groups differed significantly from each other except between the low spore count and fed-spores-but-not-infected bees (no infection) and between moderate spore count and high spore count bees. There were no significant differences in alpha diversity between the different infection level groups (Χ 23 = 3.29, N = 97,155, P = 0.07). Three uncultured gamma proteobacteria (Gilliamella) ASVs and one unknown bacteria ASV had statistically significant differential abundance between the infection levels (and most abundant in the high infection group, Table S1). A pairwise BLAST search revealed that the Gilliamella ASV that was significantly more abundant in high spore count bees differed from the two Gilliamella ASVs that positively correlated with infection in our previous work32.
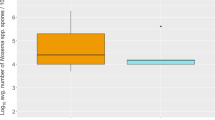
Feeding bees live spores significantly affected alpha diversity as compared to uninfected control bees (Χ 21 = 4.97, N = 176, P = 0.026, Fig. 3). There were statistically significant differences in the abundance of five uncultured Lactobacillus (a higher abundance in the treatment for three out of the five Lactobacillus) and one Bombella (higher abundance in the control) (Table S1).

Alpha diversity is shown. There were significant differences in alpha diversity between the control bees (bees not fed spores) and the experimental bees (bees that were fed live spores, Χ 21 = 4.97, N = 176, P = 0.026).
Finally, with respect to resistance, beta diversity was significantly different between fed-spores-but-not-infected and control bees (F1,139 = 2.95, P < 0.001, R2 = 0.02). Beta dispersion was significantly different between control and fed-spores-but-not-infected bees (F1,126 = 13.58, P = 0.001). However, there were no significant differences in alpha diversity between control and fed-spores-but-not-infected bees (Χ 2 1 = 0.0484, N = 100, P = 0.826). Two uncultured Lactobacillus sp. ASVs were statistically significantly differentially abundant between control and fed-spores-but-not-infected bees (one was more abundant in fed-spores-but-not-infected bees while the other was more abundant in control, Table S1). Besides the few taxa mentioned, there were no significant differences in the relative abundance of bacteria between groups. We also plotted the relative abundance of the top ten bacterial species and genera by control (uninfected bees), bees fed-spores-but-not-infected, low infection, medium infection, and high infection levels in Fig. S2.
Discussion
We aimed to determine the impact of feeding live spores on the survival and infection levels of bees in a controlled laboratory setting. Our prior N. ceranae experiment involved returning bees fed spores back to their colonies. However, this treatment resulted in low levels of infection among the control bees, likely due to the interaction of infected and control bees32. To overcome this limitation, we isolated the control and experimental bees in separate cages in this experiment.
Feeding live N. ceranae spores to bees led to a significant increase in gut spore levels and a decrease in bee survival, as anticipated. Notably, infection levels varied significantly among different colonies, suggesting that factors such as the colony's genetic background, microbiome composition, or a combination of both, play a role in their resistance or susceptibility to N. ceranae. Bees exhibited subtle differences in their microbiome compositions that depended upon whether they were infected or sham inoculated, had different infection levels, or displayed resistance or susceptibility to infection. These shifts manifested as subtle changes in community composition (Beta-diversity as tested with PerMANOVA) but not differences in how variable communities were by treatment (Beta-dispersion). Alpha diversity (the number of bacterial taxa, in this case ASVs, per sample) also varied by treatment, but not in the presence or absence of core bacteria. Our findings therefore suggest that shifts in the abundance of core honey bee bacteria, rather than the presence or absence of specific bacteria, are associated with resistance to and the susceptibility of bees to different levels of infection with N. ceranae.
Multiple studies have shown that N. ceranae infection has a harmful effect on A. mellifera, so it is not surprising that infection reduces worker lifespan. Our bees fed with N. ceranae spores had a mortality rate of 43% after 12 days post-inoculation (dpi), which was significantly higher than the control bees' mortality rate of 23%. These results are similar to those reported in other studies, such as Goblirsch et al.55 and Milbrath et al.47.
Our treatment method for bees differed from previous studies in several ways, which may explain some of the differences in results. For example, our bees were only fed with a sterile sucrose solution, while some other studies provided their caged bees with non-sterile pollen and dietary supplements. We also caged our bees on comb in the colony for the first 5 days post-eclosion to allow them to obtain the colony microbiome.
We found that the bees fed with live spores were significantly more infected than control bees. On average, bees that were fed 40,000 live spores had infection levels of 7.7 million spores per bee at 12 dpi, with 91.5% of them being infected (defined as having at least one spore by microscopic analysis). This is in line with previous studies that showed that older bees, especially foragers, are the most susceptible and highly infected by N. ceranae.
Overall, there is considerable variation in infection levels among different experiments, which may be due to differences in N. ceranae purification and feeding techniques, bee age, and colony background56,57. Our study recorded the highest infection level to be 41.4 million spores per bee, which is comparable to levels found in other studies56,57. Further research is necessary to fully understand the mechanisms behind N. ceranae resistance and susceptibility in bees.
Nosema ceranae infection had a significant but subtle effect on honey bee gut microbiome composition. Bees that were either experimentally infected or sham inoculated showed subtle differences in the composition of their microbiomes. Similarly, bees that were fed-spores-but-not-infected or were fed spores and became infected also had some differences in their microbiomes. These results reflect differences in the abundances of ‘core’ honey bee bacteria instead of differences in presence or absence of specific bacteria. For example, a Lactobacillus apis ASV was at greater abundance in infected bees compared to control bees, while a L. bombicola ASV and two Snodgrasella ASVs were at lower abundance in infected bees. Previous work has shown that Lactobacillus spp. can mitigate Nosema infection either when administered alone58 or in conjunction with Bifidobacterium (Baffoni et al., 2015). Likewise, Snodgrasella, inhibits Nosema infection via host-immune priming and subsequent disruption of the pathogen’s redox system59. However, as noted by Raymann and Moran35, whether these correlations are driven by infection or are drivers of infection remains to be seen. While other factors account for the majority of microbiome variation, our finding that N. ceranae infection has subtle effects on honey bee gut microbiome composition is consistent with our previous study32, as well as the work of others33,60,61,62.
As in our previous research32, we found two Gilliamella ASVs that were positively associated with N. ceranae infection. However, these Gilliamella ASVs differed between our two studies. This result suggests that several or even many Gilliamella strains may either facilitate or be involved in resistance to N. ceranae infection, while other strains appear to not be affected or involved. Exploring strain-level interactions between gut microbes, gut pathogens, and hosts could be a rich future research direction.
Several other studies have demonstrated a positive correlation between certain microbiome bacteria and bee diseases. Schwarz et al.44 found that the presence of Gilliamella apicola increased in bees affected by the parasite, L. passim. Furthermore, stressed bees that were treated with S. alvi and L. passim had the largest amount of G. apicola. An analysis of bee colonies diagnosed with Colony Collapse Disorder (CCD), a rapid decline of honey bee colonies, displayed a consistent pattern of heightened Gammaproteobacteria (including G. apicola and Frischella perrara)44. Rubanov et al.32, showed that two specific sequence variants of Gilliamella, a core gut symbiont previously linked to gut dysbiosis, were significantly more prevalent in bees from colonies with high levels of N. ceranae as compared to those with low levels. However, Ye et al.63 discovered that the relative abundance of Gilliamella spp. was significantly reduced in bees infected with American foulbrood (AFB, caused by Paenibacillus larvae) or chalkbrood (caused by Ascosphaera apis). Additionally, Erban et al.64 found that Citrobacter freundii and Hafnia alvei were more abundant in association with AFB. Zhang et al.33 showed that Bifidobacterium spp. significantly increased with N. ceranae infection. Although the specific causes and mechanisms of this association are still unknown, these results suggest that indigenous Bifidobacterium spp. in honey bee hindguts may have no preventative effects on N. ceranae disease.
There is evidence that some bacteria can be associated with the ability of bees to resist disease. Erban et al.64 found that the bacteria Enterococcus faecalis, Klebsiella oxytoca, Spiroplasma melliferum, and Morganella morganii were more abundant in colonies that were either outside the zone in which AFB is found or within the AFB zone but asymptomatic. Daisley et al.65 reported that the use of probiotic lactobacilli improved colony resistance to AFB. Laboratory experiments with honey bee larvae showed that Lactobacillus plantarum Lp39, Lactobacillus rhamnosus GR-1, and Lactobacillus kunkeei BR-1 could reduce pathogen loads, increase expression of key immune genes, and improve survival during P. larvae infection. Borges et al.66 showed that feeding bees Enterococcus faecium reduced N. ceranae spore numbers without affecting bee mortality. Ye et al.63 showed that healthy larvae were significantly enriched in the bacterial genera Lactobacillus and Stenotrophomonas, as well as the fungal genera Alternaria and Aspergillus. The authors suggest that this enrichment of microorganisms may protect larvae from potential infections. In contrast, the relative abundance of Gilliamella spp. was significantly reduced in infected foraging bees. Finally, some bacteria have shown no impact on bee disease levels. Floyd et al.67 found no effect of Parasacharribacter apium strain C6 (now Bombella apis68) on European foulbrood (EFB), contrary to prior findings. Stephan et al.69found no effect of lactic acid bacteria dietary supplementation against AFB disease.
Some studies indicate that a more diverse microbiome may not necessarily be beneficial for honey bees. Zhang et al.70 found that bees fed a prebiotic had slightly higher pathogen counts but also lower mortality rates. Analysis of the bee microbiota suggested that infected bees had a similar composition to those with a longer lifespan, and the prebiotic seemed to enhance these similarities. Erban et al.64 showed that bees infected with AFB had microbiomes with higher alpha diversity than control bees. Napflin and Schmid-Hempel71 found that, in Bombus terrestris, higher microbiota OTU diversity was associated with lower resistance to Crithidia bombi. Parasite infection success can depend on microbiota composition, but the key alterations are elusive. The microbiota-host interaction before parasite exposure, rather than the exposure to the parasite itself, may be key.
In contrast, other studies suggest that having a diverse microbiome is beneficial. Mockler et al.72 found that high microbiome diversity was associated with lower levels of Crithidia infection in Bombus impatiens, while Harris et al.73 found that the complete community of gut bacteria is necessary to protect against the bacterial pathogen Paenibacillius larvae. It is important to consider that these results may vary depending on the species of bee, the pathogen in question, and the methods used to study the relationship between the microbiome and bee health. For example, Nosema is restricted to adult gut tissues, whereas other diseases affect immature stages and may have more systemic effects on the microbial community external to the gut. Finally, Li et al.62 inoculated bees with N. ceranae and fed them an antibiotic that eliminated their microbiomes. Eliminating the microbiome harmed bee immune functioning and made bees more susceptible to N. ceranae infection. Further research is clearly needed to fully understand the microbiome's role in honeybees' health.
Our findings therefore support the growing body of literature that highlights the correlation between specific microbiome bacteria and honey bee diseases. Interestingly, our results emphasize the changes in the abundance of core honey bee bacteria rather than the presence or absence of specific bacteria may be important for honey bee health.
Finally, we should consider that the microbiome may vary seasonally. Rouze et al.74 showed that exposure to the parasite N. ceranae and fipronil treatment can alter the abundance of certain bacterial species in the bee gut, potentially negatively impacting bee health. Almeida et al.75 found that the strongest determinant of honeybee microbiome composition was time, with clustering of the microbiome by time point observed across all apiaries. The study also found a correlation between the forager bee microbiome and hive health, as measured by the number of larvae, bees, and honey production. These findings highlight the importance of considering seasonal variation and the potential impact of environmental factors, such as forage availability, when studying the honey bee microbiome.
Data availability
The datasets generated and/or analyzed during the current study are available in the Zenodo.com repository, at this DOI:https://doi.org/10.5281/zenodo.10795522.
References
Lonsdorf, E. et al. Crop pollination services. In Natural capital: theory and practice of mapping ecosystem services (eds Karieva, P. et al.) 168–187 (Oxford University Press, 2011).
Winfree, R., Gross, B. J. & Kremen, C. Valuing pollination services to agriculture. Ecol. Econ. 71, 80–88. https://doi.org/10.1016/j.ecolecon.2011.08.001 (2011).
Garibaldi, L. A. et al. Wild pollinators enhance fruit set of crops regardless of honey bee abundance. Science 339, 1608–1611. https://doi.org/10.1126/science.1230200 (2013).
Ollerton, J. et al. Overplaying the role of honey bees as pollinators: A comment on Aebi and Neumann (2011). Trends Ecol. Evolu. 27, 141–142. https://doi.org/10.1016/j.tree.2011.12.001 (2012).
Losey, J. E. & Vaughan, M. The economic value of ecological services provided by insects. BioScience 56, 311–323. https://doi.org/10.1641/0006-3568(2006)56[311:TEVOES]2.0.CO;2 (2006).
Aizen, M. A. & Harder, L. D. The global stock of domesticated honey bees is growing slower than agricultural demand for pollination. Curr. Biol. 19, 915–918. https://doi.org/10.1016/j.cub.2009.03.071 (2009).
Potts, S. G. et al. Global pollinator declines: Trends, impacts and drivers. Trends Ecol. Evolu. 25, 345–353. https://doi.org/10.1016/j.tree.2010.01.007 (2010).
Goulson, D., Nicholls, E., Botías, C. & Rotheray, E. L. Bee declines driven by combined stress from parasites, pesticides, and lack of flowers. Science 347, 1255957–1255957. https://doi.org/10.1126/science.1255957 (2015).
Rennich, K., Pettis, J., vanEngelsdorp, D., Bozarth, R., Eversole, H., Roccasecca, K., Smith, M., Stitzinger, J., Andree, M., Snyder, R. et al. National honey bee pests and diseases survey report, pp. 1–17: USDA Animal and Plant Health Inspection Service. http://www.step-project.net/NPDOCS/2011_National_Survey_Report.pdf. (2012).
Pettis, J. S., vanEngelsdorp, D., Johnson, J. & Dively, G. Pesticide exposure in honey bees results in increased levels of the gut pathogen Nosema. Naturwissenschaften 99, 153–158. https://doi.org/10.1007/s00114-011-0881-1 (2012).
Ansari, M. J., Al-Ghamdi, A., Nuru, A., Khan, K. A. & Alattal, Y. Geographical distribution and molecular detection of Nosema ceranae from indigenous honey bees of Saudi Arabia. Saudi J. Biol. Sci. 24, 983–991. https://doi.org/10.1016/j.sjbs.2017.01.054 (2017).
Imani Baran, A., Kalami, H., Mazaheri, J. & Hamidian, G. Nosema ceranae was the only detected microsporidian species from Iranian honey bee colonies: A molecular and phylogenetic study. Parasitol. Res. 121, 355–366. https://doi.org/10.1007/s00436-021-07381-8 (2022).
Ostroverkhova, N. V., Konusova, O. L., Kucher, A. N., Kireeva, T. N. & Rosseykina, S. A. Prevalence of the Microsporidian Nosema spp. in Honey Bee Populations (Apis mellifera) in Some Ecological Regions of North Asia. Vet. Sci. 7, 111. https://doi.org/10.3390/vetsci7030111 (2020).
Papini, R. et al. Prevalence of the microsporidian Nosema ceranae in honeybee (Apis mellifera) apiaries in Central Italy. Saudi J. Biol. Sci. 24, 979–982. https://doi.org/10.1016/j.sjbs.2017.01.010 (2017).
Tokarev, Y. S. et al. A formal redefinition of the genera Nosema and Vairimorpha (Microsporidia: Nosematidae) and reassignment of species based on molecular phylogenetics. J. Invertebr. Pathol. 169, 107279. https://doi.org/10.1016/j.jip.2019.107279 (2020).
Chaimanee, V. et al. Susceptibility of four different honey bee species to Nosema ceranae. Veterinary Parasitol. 193, 260–265. https://doi.org/10.1016/j.vetpar.2012.12.004 (2012).
Charbonneau, L. R., Hillier, N. K., Rogers, R. E. L., Williams, G. R. & Shutler, D. Effects of Nosema apis, N. ceranae, and coinfections on honey bee (Apis mellifera) learning and memory. Sci. Rep. 6, 1–7. https://doi.org/10.1038/srep22626 (2016).
Martín-Hernández, R. et al. Microsporidia infecting Apis mellifera: coexistence or competition. Is Nosema ceranae replacing Nosema apis?. Environ. Microbiol. 14, 2127–2138. https://doi.org/10.1111/j.1462-2920.2011.02645.x (2011).
Wang, Q. et al. Nosema ceranae, the most common microsporidium infecting Apis mellifera in the main beekeeping regions of China since at least 2005. J. Apicult. Res. 58, 562–566. https://doi.org/10.1080/00218839.2019.1632148 (2019).
Chauzat, M. et al. Presence of Nosema ceranae in French honey bee colonies. J. Apicult. Res. 46, 127. https://doi.org/10.1080/00218839.2007.11101380 (2007).
Klee, J. et al. Widespread dispersal of the microsporidian Nosema ceranae, an emergent pathogen of the western honey bee, Apis mellifera. J. Invertebr. Pathol. 96, 1–10. https://doi.org/10.1016/j.jip.2007.02.014 (2007).
Dussaubat, C. et al. Gut pathology and responses to the microsporidium Nosema ceranae in the honey bee Apis mellifera. PLoS One 7, e37017. https://doi.org/10.1371/journal.pone.0037017 (2012).
Martín-Hernández, R. et al. Comparison of the energetic stress associated with experimental Nosema ceranae and Nosema apis infection of honeybees (Apis mellifera). Parasitol. Res. 109, 605–612. https://doi.org/10.1007/s00436-011-2292-9 (2011).
Paris, L., El Alaoui, H., Delbac, F. & Diogon, M. Effects of the gut parasite Nosema ceranae on honey bee physiology and behavior. Curr. Opin. Insect. Sci. 26, 149–154. https://doi.org/10.1016/j.cois.2018.02.017 (2018).
Botías, C., Martín-Hernández, R., Barrios, L., Meana, A. & Higes, M. Nosema spp. infection and its negative effects on honey bees (Apis mellifera iberiensis) at the colony level. Veterinary Res. 44, 25. https://doi.org/10.1186/1297-9716-44-25 (2013).
Kralj, J. & Fuchs, S. Nosema sp. influences flight behavior of infected honey bee (Apis mellifera) foragers. Apidologie 41, 21–28. https://doi.org/10.1051/apido/2009046 (2009).
Higes, M. et al. How natural infection by Nosema ceranae causes honeybee colony collapse. Environ. Microbiol. 10, 2659–2669. https://doi.org/10.1111/j.1462-2920.2008.01687.x (2008).
Aufauvre, J. et al. Parasite-insecticide interactions: A case study of Nosema ceranae and fipronil synergy on honeybee. Sci. Rep. 2, 1–7. https://doi.org/10.1038/srep00326 (2012).
Wu, J. Y., Smart, M. D., Anelli, C. M. & Sheppard, W. S. Honey bees (Apis mellifera) reared in brood combs containing high levels of pesticide residues exhibit increased susceptibility to Nosema (Microsporidia) infection. J. Invertebr. Pathol. 109, 326–329. https://doi.org/10.1016/j.jip.2012.01.005 (2012).
Naug, D. & Gibbs, A. Behavioral changes mediated by hunger in honeybees infected with Nosema ceranae. Apidologie 40, 595–599. https://doi.org/10.1051/apido/2009039 (2009).
Paris, L. et al. Honeybee gut microbiota dysbiosis in pesticide/parasite co-exposures is mainly induced by Nosema ceranae. J. Invertebr. Pathol. 172, 107348. https://doi.org/10.1016/j.jip.2020.107348 (2020).
Rubanov, A., Russell, K. A., Rothman, J. A., Nieh, J. C. & McFrederick, Q. S. Intensity of Nosema infection is associated with specific honey bee gut bacteria and weakly associated with gut microbiome structure. Sci. Rep. 9, 3820. https://doi.org/10.1038/s41598-019-40347-6 (2019).
Zhang, Y. et al. Nosema ceranae infection enhances Bifidobacterium spp. abundances in the honey bee hindgut. Apidologie 50, 353–362. https://doi.org/10.1007/s13592-019-00644-5 (2019).
Kwong, W. K. & Moran, N. A. Gut microbial communities of social bees. Nat. Rev. Microbiol. 14, 374–384. https://doi.org/10.1038/nrmicro.2016.43 (2016).
Raymann, K. & Moran, N. A. The role of the gut microbiome in health and disease of adult honey bee workers. Curr. Opin. Insect Sci. 26, 97–104. https://doi.org/10.1016/j.cois.2018.02.012 (2018).
Martinson, V. G., Moy, J. & Moran, N. A. Establishment of characteristic gut bacteria during development of the honeybee worker. Appl. Environ. Microbiol. 78, 2830–2840. https://doi.org/10.1128/AEM.07810-11 (2012).
Engel, P., Martinson, V. G. & Moran, N. A. Functional diversity within the simple gut microbiota of the honey bee. Proceedings of the National Academy of Sciences of the United States of America 109, 11002-11007. (2012). https://doi.org/10.1073/pnas.1202970109
Kwong, W. K., Mancenido, A. L. & Moran, N. A. Immune system stimulation by the native gut microbiota of honey bees. Royal Soc. Open Sci. 4, 170003–170009. https://doi.org/10.1098/rsos.170003 (2017).
Bourgeois, A. L., Beaman, L. D., Holloway, B. & Rinderer, T. E. External and internal detection of Nosema ceranae on honey bees using real-time PCR. J. Inverteb. Pathol. 109, 1–3. https://doi.org/10.1016/j.jip.2012.01.002 (2012).
Corby-Harris, V. et al. Parasaccharibacter apium, gen. nov., sp. nov., Improves Honey Bee (Hymenoptera: Apidae) Resistance to Nosema. Ecotoxicology 109, 537–543. https://doi.org/10.1093/jee/tow012 (2016).
Baffoni, L. et al. Effect of dietary supplementation of Bifidobacterium and Lactobacillus strains in Apis mellifera L. against Nosema ceranae. Benef. Microbes 7, 1–8. https://doi.org/10.3920/BM2015.0085 (2016).
Maes, P. W., Rodrigues, A. P., Oliver, R., Mott, B. M. & Anderson, K. E. Diet related gut bacterial dysbiosis correlates with impaired development, increased mortality and Nosema disease in the honey bee (Apis mellifera). Molecular Ecol. https://doi.org/10.1111/mec.13862 (2016).
Petersen, C. & Round, J. L. Defining dysbiosis and its influence on host immunity and disease. Cell Microbiol. 16, 1024–1033. https://doi.org/10.1111/cmi.12308 (2014).
Schwarz, R. S., Moran, N. A. & Evans, J. D. Early gut colonizers shape parasite susceptibility and microbiota composition in honey bee workers. Proceedings of the National Academy of Sciences of the United States of America 113, 9345-9350. (2016). https://doi.org/10.1073/pnas.1606631113
Sommer, F. & Backhed, F. The gut microbiota–masters of host development and physiology. Nat. Rev. Microbiol. 11, 227–238. https://doi.org/10.1038/nrmicro2974 (2013).
Eiri, D. M., Suwannapong, G., Endler, M. & Nieh, J. C. Nosema ceranae can infect honey bee larvae and reduces subsequent adult longevity. PLoS One 10, e0126330-e126417. https://doi.org/10.1371/journal.pone.0126330 (2015).
Milbrath, M. O. et al. Comparative virulence and competition between Nosema apis and Nosema ceranae in honey bees (Apis mellifera). J. Invertebr. Pathol. 125, 9–15. https://doi.org/10.1016/j.jip.2014.12.006 (2015).
Dietemann, V., Ellis, J. D. & Neumann, P. The COLOSS BEEBOOK volume I: standard methods for Apis mellifera research. https://boris.unibe.ch/55024/. (2013).
Cantwell, G. E. Standard methods for counting Nosema spores. Am. Bee J. 110, 222–223 (1970).
Williams, G. R. et al. Standard methods for maintaining adult Apis mellifera in cages under in vitro laboratory conditions. J. Apicult. Res. 52, 1–35. https://doi.org/10.3896/IBRA.1.52.1.04 (2013).
Graystock, P., Rehan, S. M. & McFrederick, Q. S. Hunting for healthy microbiomes: determining the core microbiomes of Ceratina, Megalopta, and Apis bees and how they associate with microbes in bee collected pollen. Conserv. Genet. 18, 701–711. https://doi.org/10.1007/s10592-017-0937-7 (2017).
Rothman, J. A., Carroll, M. J., Meikle, W. G., Anderson, K. E. & McFrederick, Q. S. Longitudinal effects of supplemental forage on the honey bee (Apis mellifera) Microbiota and Inter- and Intra-Colony Variability. Microb. Ecol. 76, 814–824. https://doi.org/10.1007/s00248-018-1151-y (2018).
Kembel, S. W., O'Connor, T. K., Arnold, H. K., Hubbell, S. P., Wright, S. J. & Green, J. L. Relationships between phyllosphere bacterial communities and plant functional traits in a neotropical forest. Proceedings of the National Academy of Sciences of the United States of America 111, 13715-13720. (2014). https://doi.org/10.1073/pnas.1216057111
McFrederick, Q. S. & Rehan, S. M. Characterization of pollen and bacterial community composition in brood provisions of a small carpenter bee. Molecular Ecol. 25, 2302–2311. https://doi.org/10.1111/mec.13608 (2016).
Goblirsch, M., Huang, Z. Y. & Spivak, M. S. Physiological and behavioral changes in honey bees (Apis mellifera) induced by Nosema ceranae infection. PLoS One 8, e58165. https://doi.org/10.1371/journal.pone.0058165 (2013).
Forsgren, E. & Fries, I. Comparative virulence of Nosema ceranae and Nosema apis in individual European honey bees. Veterinary Parasitol. 170, 212–217. https://doi.org/10.1016/j.vetpar.2010.02.010 (2010).
Huang, W.-F., Solter, L., Aronstein, K. & Huang, Z. Infectivity and virulence of Nosema ceranae and Nosema apis in commercially available North American honey bees. J. Inverteb. Pathol. 124, 107–113. https://doi.org/10.1016/j.jip.2014.10.006 (2015).
Arredondo, D. et al. Lactobacillus kunkeei strains decreased the infection by honey bee pathogens Paenibacillus larvae and Nosema ceranae. Benef. Microbes 9, 279–290. https://doi.org/10.3920/BM2017.0075 (2018).
Lang, H. et al. Engineered symbiotic bacteria interfering Nosema redox system inhibit microsporidia parasitism in honeybees. Nat. Commun. 14, 2778. https://doi.org/10.1038/s41467-023-38498-2 (2023).
Hubert, J. et al. Changes in the bacteriome of honey bees associated with the parasite Varroa destructor, and pathogens Nosema and Lotmaria passim. Microbial Ecol. 73, 1–14. https://doi.org/10.1007/s00248-016-0869-7 (2016).
Jabal-Uriel, C., Alba, C., Higes, M., Rodriguez, J. M. & Martin-Hernandez, R. Effect of Nosema ceranae infection and season on the gut bacteriome composition of the European honeybee (Apis mellifera). Sci. Rep. 12, 9326. https://doi.org/10.1038/s41598-022-13337-4 (2022).
Li, J. H. et al. New evidence showing that the destruction of gut bacteria by antibiotic treatment could increase the honey bee’s vulnerability to Nosema infection. PLoS One 12, e0187505. https://doi.org/10.1371/journal.pone.0187505 (2017).
Ye, M. H. et al. Microbiota dysbiosis in honeybee (Apis mellifera L.) larvae infected with brood diseases and foraging bees exposed to agrochemicals. R. Soc. Open Sci. 8, 201805. https://doi.org/10.1098/rsos.201805 (2021).
Erban, T. et al. Honeybee (Apis mellifera)-associated bacterial community affected by American foulbrood: Detection of Paenibacillus larvae via microbiome analysis. Sci. Rep. 7, 5084. https://doi.org/10.1038/s41598-017-05076-8 (2017).
Daisley, B. A. et al. Novel probiotic approach to counter Paenibacillus larvae infection in honey bees. ISME J. https://doi.org/10.1038/s41396-019-0541-6 (2019).
Borges, D., Guzman-Novoa, E. & Goodwin, P. H. Effects of prebiotics and probiotics on honey bees (Apis mellifera) infected with the microsporidian parasite Nosema ceranae. Microorganisms 9, 481. https://doi.org/10.3390/microorganisms9030481 (2021).
Floyd, A. S. et al. Microbial ecology of european foul brood disease in the honey bee (Apis mellifera): Towards a microbiome understanding of disease susceptibility. Insects https://doi.org/10.3390/insects11090555 (2020).
Smith, E. A. et al. Reclassification of seven honey bee symbiont strains as Bombella apis. bioRxiv https://doi.org/10.1099/ijsem.0.004950 (2020).
Stephan, J. G. et al. Honeybee-specific lactic acid bacterium supplements have no effect on american foulbrood-infected honeybee colonies. Appl. Environ. Microbiol. 85, 283–314. https://doi.org/10.1128/AEM.00606-19 (2019).
Zhang, Y. et al. Nosema (Nosema) ceranae infection alters honey bee microbiota composition and sustains the survival of adult honey bees. Biology (Basel) https://doi.org/10.3390/biology10090905 (2021).
Napflin, K. & Schmid-Hempel, P. High gut microbiota diversity provides lower resistance against infection by an intestinal parasite in bumblebees. Am. Nat. 192, 131–141. https://doi.org/10.1086/698013 (2018).
Mockler, B. K., Kwong, W. K., Moran, N. A. & Koch, H. Microbiome structure influences infection by the parasite Crithidia bombi in bumble bees. Appl. Environ. Microbiol. 84, e02335-e2417. https://doi.org/10.1128/AEM.02335-17 (2018).
Harris, E. V., de Roode, J. C. & Gerardo, N. M. Diet-microbiome-disease: Investigating diet’s influence on infectious disease resistance through alteration of the gut microbiome. PLoS Pathog. 15, e1007891. https://doi.org/10.1371/journal.ppat.1007891 (2019).
Rouze, R., Mone, A., Delbac, F., Belzunces, L. & Blot, N. The honeybee gut microbiota is altered after chronic exposure to different families of insecticides and infection by Nosema ceranae. Microbes Environ. 34, 226–233. https://doi.org/10.1264/jsme2.ME18169 (2019).
Almeida, E. L. et al. Geographical and seasonal analysis of the honeybee microbiome. Microb. Ecol. https://doi.org/10.1007/s00248-022-01986-x (2022).
Acknowledgements
We would like to thank the anonymous reviewers, the editor, and Josh Kohn, and David Holway, whose comments improved our manuscript. We are grateful for the assistance of Yvonna Nguyen, Kaylx Su, Divya Kirani, and Aria Loduca.
Author information
Authors and Affiliations
Contributions
E.L. conducted the infection experiment. J.M. analyzed the bee microbiomes. E.L., J.M., Q.M., and J.C.N. analyzed the data and wrote the paper. Q.M. and J.C.N. provided key materials and funding support. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lau, E., Maccaro, J., McFrederick, Q.S. et al. Exploring the interactions between Nosema ceranae infection and the honey bee gut microbiome. Sci Rep 14, 20037 (2024). https://doi.org/10.1038/s41598-024-67796-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-67796-y
- Springer Nature Limited