
Abstract
This study aimed to explore the association between bone mineral density and physical frailty including nutrition, muscle mass, and oral function. We included participants aged 35–80 years and examined their bone mineral density, serum albumin level, body composition, and variance of hue (VOH) of two-colored gum. We also used the geriatric oral health assessment index (GOHAI). These data were used to calculate the geriatric nutritional risk index (GNRI) and skeletal muscle index (SMI). Multinomial logistic regression was performed to assess the relationship between GNRI, SMI, VOH, GOHAI, and bone mineral density after adjusting for comorbidities, including hypertension, diabetes mellitus, and previous bone fracture. We included 228 participants and classified their bone mineral density as normal, osteopenic, or osteoporotic. Older age (odds ratio (OR) 1.15, 95% confidence interval (CI) [1.08, 1.23]), low GNRI (OR 0.90, 95% CI [0.83, 0.98]), low SMI (OR 0.43, 95% CI [0.27, 0.68]), and high VOH (OR 1.08, 95% CI [1.01, 1.17]) were significantly associated with osteoporosis. Older age (OR 1.08, 95% CI [1.04, 1.11]) and low GNRI (OR 0.93, 95% CI [0.87, 0.99]) were significantly associated with osteopenia. GNRI, SMI, and VOH were significantly associated with osteoporosis among male participants. Although the multinomial logistic regression analysis indicated that GNRI, SMI, VOH, and GOHAI were not significantly associated with osteoporosis or osteopenia among female participants, the demographic distribution showed that older age, low GNRI, and low SMI were significantly associated with bone mineral density decline. Physical frailty, including nutritional decline, muscle mass loss, and poor oral status, is associated with low bone density. This easy-to-use tool can be used to detect osteoporosis early and to prevent osteoporosis and osteoporosis-related fractures.
Similar content being viewed by others

Introduction
Aging-associated decline occurs in biological, physiological, psychological, behavioral, and social processes as individuals age. Osteoporosis is an age-related systemic skeletal disease characterized by bone mass loss and bone microarchitecture deterioration. An imbalance in the rates of bone resorption and formation causes osteoporosis. Furthermore, low bone mineral density can cause osteoporotic fractures, leading to socioeconomic burden, reduced quality of life, post-fracture complications, and a high mortality risk. Notably, it has been positively proven that aging, menopause, comorbidities such as hypertension (HTN) and diabetes mellitus (DM), and health behaviors, such as low physical activity, cigarette smoking, and alcohol consumption, stress, medication use, and air pollution contribute to the risk of osteoporosis1,2,3,4. Poor oral status and low mandibular cortical width are also risk factors for osteoporosis5.
Aging increases the risk of poor health outcomes and can lead to frailty. Frailty is a multidimensional geriatric syndrome that occurs with age and ultimately causes morbidity, hospitalization, disability, and mortality. It represents the loss of harmonic interaction among multiple domains, including the physical, psychological, and social components6. A recent study used frailty as a screening tool to predict osteoporotic fractures7. Among the frailty domains, we focused on physical frailty, including nutritional status and muscle mass. The geriatric nutritional risk index (GNRI), used as an assessment, is a nutrition-related risk index that identifies malnutrition and evaluates suitable timing for nutritional support8. The skeletal muscle index (SMI) assesses skeletal muscle mass.
Masticatory dysfunction results in poor chewing efficiency, difficulty in chewing, inadequate nutrient intake, and poor food digestion and absorption. The two-colored gum test for assessing masticatory performance has previously been validated9,10. Masticatory performance can also be evaluated by the questionnaire. The self-reported geriatric oral health assessment index (GOHAI) focuses on subjective oral health and can be used to evaluate oral health-related quality of life, including physical and psychosocial functions and pain or discomfort11.
As the aging process gradually decreases human physical and mental capacity, early detection of aberrations can help prevent subsequent disease burdens such as osteoporosis and bone fractures. In the present study, we used physical frailty and oral health as indicators to explore their correlation with bone mineral density.
Methods
Participants
Adult participants from communities aged between 35 and 80 years were recruited from Puzi Hospital (Chiayi County, southern Taiwan) between November 01, 2021, and December 31, 2022. Participants with a history of pharyngeal surgery, laryngeal surgery, moderate-to-severe dementia, stroke, cerebral palsy, myasthenia gravis, oral cancer, aspiration pneumonia, moderate-to-severe Parkinson's disease, or Alzheimer's disease were excluded. All participants agreed to participate in the study and signed informed consent forms. This study was approved by the Institutional Review Board of Biomedical Science Research, Academia Sinica (AS-IRB-BM-21047).
Data collection
The research team included a clinical dentist and a trained research nurse. The data included demographic characteristics (age, sex, and self-reported height), electronic medical records, bone mineral density of femoral neck, serum albumin levels, body composition, masticatory ability, and GOHAI scores. Electronic medical records collected from the Taiwan National Health Insurance (NHI) PharmaCloud System included comorbidities such as HTN, DM, and a history of bone fracture. The NHI PharmaCloud System contains real-time inpatient and outpatient medication records for the previous 6 months. A workflow detailing the data collection procedure is provided in the supplement (Fig. S1).
Bone mineral density
Bone mineral density of the femoral neck was evaluated using dual-energy X-ray absorptiometry (DXA; Hologic Discovery Wi, Hologic Inc., Bedford, MA, USA). T scores ≤ − 2.5, between − 2.5 and − 1, and − 1 standard deviation (SD) were classified as osteoporosis, osteopenia, and normal, respectively.
Geriatric nutritional risk index (GNRI)
The GNRI served as an objective indicator to evaluate participants’ nutritional status. This was calculated as follows:
where WLo represents the ideal weight determined by the Lorentz equation:
The albumin value used in the calculation was obtained from the blood test.
Skeletal muscle index (SMI)
The SMI was calculated by dividing the limb skeletal muscle mass (kg) by the square of the height (m2). Limb skeletal muscle mass was measured using a bioelectrical impedance analyzer (Tanita MC-780MA; Tanita Corporation, Japan). The participants held the two handles with their arms separated from the trunk for 1 min to perform the body composition analysis.
Masticatory ability
Masticatory ability was tested using two-colored gum comprising green and dark violet layers produced by Vivident Fruit Swing Karpuz Üzüm Sakız 26 gr (Turkey). We excluded participants aged > 80 years for fear of accidental swallowing while chewing gum. To determine the number of chewing cycles, participants aged 35–49 years chewed a series of two-colored gum samples in five subsequent tests, starting with five cycles followed by 10, 20, 30, and 50 cycles12. The participants rested between tests. The increased difference in variance of hue (VOH) with increasing chewing cycles and 30 chewing cycles can effectively distinguish the mixing abilities. The research nurse instructed the participants to perform 30 chewing cycles. After chewing, the gum samples were returned, placed in transparent plastic bags, and flattened to 1 mm using a plastic plate (Fig. 1A). Both sides of the flattened samples were photographed using a smartphone (HTC Desire 20+). The freely available software ViewGum (Fig. 1B, http://www.dhal.com/viewgum.htm) transformed the images into a hue, saturation, and intensity (HSI) color space. The VOH is considered an indicator of the degree of mixing, with a larger VOH signifying inadequate mixing and thus reduced masticatory ability. For the analysis, VOH was expressed as a percentage.

The processing and image identification of chewed gum samples.
Geriatric oral health assessment index (GOHAI)
The GOHAI measures self-perceived oral health in the last 3 months. The GOHAI comprises 12 items grouped into three dimensions: pain or discomfort, physical function, and psychosocial function. Total scores were calculated by summing each item with the responses using a 5-point Likert scale. Higher scores indicated good oral health. This study used a validated GOHAI questionnaire (Chinese version)13.
Statistical analysis and data mining
Participants were divided into normal, osteopenic, and osteoporotic groups. Age, sex, electronic medical records, GNRI, SMI, masticatory ability, and GOHAI scores were examined and calculated. Kruskal–Wallis and Fisher’s exact tests were used to compare the characteristics of the three different bone mineral density groups. Multinomial logistic regression was used to explore the association between the characteristics and different bone mineral density groups. The regression analyses included all variables of interest. Statistical significance was set at P < 0.05. All analyses were performed using R software (version 4.2.2)14.
Ethics approval and consent to participate
The study was approved by the Institutional Review Board (of Biomedical Science Research, Academia Sinica (AS-IRB-BM-21047). Written informed consent was obtained from all participants. This study was performed in accordance with the Declaration of Helsinki and followed the approved protocol.
Results
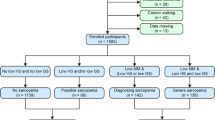
We included 228 participants aged 35–80 years. According to the bone mineral density T score, the number of participants in the normal, osteopenic, and osteoporotic groups was 77, 103, and 48, respectively (Table 1). The average age in the osteoporotic group was the oldest (mean = 71.5 years old, SD = 4.9) and that in the normal group was the youngest (mean = 58.8, SD = 12.6). The proportion of females was high, relatively high, and relatively low in the osteoporotic (81.3%), osteopenic (57.3%), and normal (45.5%) groups, respectively. The proportion of participants with comorbidities, including HTN, DM, and previous bone fractures, was relatively low, ranged from 11.7 to 18.8%, 16.7 to 31.2%, and 0 to 4.9%, respectively. The GNRI and SMI decreased with a reduction of bone mineral density, indicating that poor nutrition and low muscle mass were associated with a reduction of bone mineral density. The VOH value increased with a reduction in bone mineral density, indicating poor masticatory ability associated with a reduction in bone mineral density. Severe osteoporosis is associated with malnutrition, skeletal muscle mass loss, and low masticatory ability. The GOHAI score was not associated with a reduction of bone mineral density. Age, sex, GNRI, and SMI were significantly different among the three groups; however, VOH, GOHAI, and comorbidities, including HTN, DM, and previous bone fractures, did not exhibit significant differences. The trends in age, comorbidities, GNRI, SMI, and VOH were consistent across the total, female, and male participants, indicating a reduction in bone mineral density (Table 2). In particular, the GOHAI score was significantly different among the three groups of bone mineral density among female participants.
Table 3 shows the results of the multinomial logistic regression analysis for GNRI, SMI, VOH, and bone mineral density after adjusting for comorbidities, including HTN, DM, and previous bone fractures. Older age (odds ratio (OR) 1.15, 95% confidence interval (CI) [1.08, 1.23]), low GNRI (OR 0.90, 95% CI [0.83, 0.98]), low SMI (OR 0.43, 95% CI [0.27, 0.68]), and high VOH (OR 1.08, 95% CI [1.01, 1.17]) are significantly associated with osteoporosis (Nagelkerke pseudo R-squared = 0.45). Older age (OR 1.08, 95% CI [1.04, 1.11]) and low GNRI (OR 0.93, 95% CI [0.87, 0.99]) were significantly associated with osteopenia. Among male participants, low GNRI (OR 0.81, 95% CI [0.68, 0.96]), low SMI (OR 0.31, 95% CI [0.10, 0.996]), and high VOH (OR 1.19, 95% CI [1.05, 1.35]) were significantly associated with osteoporosis (Nagelkerke pseudo R-squared = 0.52). Older age (OR 1.07, 95% CI [1.01, 1.13]), low GNRI (OR 0.89, 95% CI [0.80, 0.99]), and high VOH levels (OR 1.10, 95% CI [1.00, 1.21]) were significantly associated with osteopenia. Although the results of the multinomial logistic regression indicated that GNRI, SMI, VOH, and GOHAI were not significantly associated with osteoporosis or osteopenia among female participants, the demographic distribution showed that older age, low GNRI, and low SMI were significantly associated with a decline in bone mineral density. Furthermore, we found that high VOH (OR 0.88, 95% CI [0.80, 0.97]) was negatively associated with increased GNRI among all participants (Table S1), indicating that low masticatory ability is related to poor nutritional status.
Discussion
To our knowledge, this is the first study to combine physical frailty and oral health to predict low bone mineral density, including osteopenia and osteoporosis, allowing for the development of an indicator for the early identification of osteoporosis and further behavioral changes in the early stages.
In our study, age, physical frailty, and oral health were significantly associated with osteoporosis, particularly in males, after adjusting for comorbidities. The related biological mechanisms are discussed below:
The GNRI was calculated using the albumin level, weight, and height. Hypoalbuminemia has been reported to be directly and indirectly linked to nuclear factor-κB (NF-κB). NF-κB decreases osteoblastic activity and increases osteoclast activity15. In addition, a low GNRI is significantly associated with low dietary protein intake16. An animal study reported that protein restriction reduced plasma concentrations of insulin-like growth factor-I (IGF-I)17. IGF-I regulates bone metabolism and adapts bone structure to mechanical loads during growth and development18.
In the biological domain of physical frailty, loss of muscle mass influences physical function and energy metabolism19. Notably, muscle mass increases the mechanical load on bones and directly loads the bone through muscle contractions during physical activity20. A high SMI stimulates and maintains bone mineral density. Similar biological pathways and common risk factors for frailty and osteoporosis were identified7, including age-related factors, low physical activity, weight loss, cognitive decline, sarcopenia, depression, and hormonal imbalances such as testosterone, estrogen, insulin-like growth factor-I (IGF-I), growth hormone (GH), vitamin D, and pro-inflammatory cytokines21,22.
The VOH of the bicolor chewing gum represents the degree of mixing and masticatory ability. Studies have shown that 30 chewing cycles can effectively discriminate masticatory ability9. This test can be performed on individuals with natural dentition as well as on those with complete dentures10. Decline in oral function restricts food intake and the absorption of nutrients, including calcium, vitamin D, magnesium, potassium, vitamin C, vitamin K, several B vitamins, and omega-3 polyunsaturated fatty acids, all related to bone mineral density23. A previous study on 114 patients diagnosed with gastric cancer found that the Eichner index, classified based on occlusal contacts, had a significant positive correlation with the GNRI24. We used VOH to represent the masticatory ability and observed the same trend. Another cross-sectional study involving 100 participants aged > 60 years investigated the relationship between osteoporosis in the mandibular bones and oral health-related quality of life25. In this study, mandibular osteoporosis and GOHAI scores were not significantly correlated. The GOHAI is self-reported, and the total score for each of the 12 items ranges from 0 to 60. The mean GOHAI score in our study was approximately 54 and 55, representing our participants’ self-perception of oral health as relatively healthy. Therefore, no association between the GOHAI and boned mineral density was found. A systematic review highlighted the relationships between oral health and bone mineral density disorders in older adults, reporting that masticatory function is associated with osteoporosis and occlusal force with bone mineral density26. Similarly, we found poor masticatory ability was significantly associated with osteoporosis.
No association between nutrition, SMI, and bone mineral density was observed in the female participants. This may be because our study did not comprehensively consider potential confounders, including estrogen and glucocorticoid levels, which are known to influence bone mineral density. Osteoporosis can arise from either estrogen deficiency or excess glucocorticoids. Estrogen deficiency can lead to an imbalance in bone remodeling, induce osteoclast apoptosis, alter the osteocyte microenvironment, affect the immune system, and cause hypermineralization27. Similarly, excess glucocorticoids can lead to microscopic heterogeneity in bone structure, creating mechanically inhomogeneous regions and potentially weak sites28. Additionally, excess glucocorticoid are associated with osteoblast and osteocyte apoptosis, resulting in decreased bone formation29.
Our results showed that physical frailty, including nutritional decline and muscle mass loss, can be used to detect different levels of bone mineral density, including normal, osteopenic, and osteoporotic. By increasing the awareness of health status and encouraging regular health examinations, medical personnel can use the results of blood tests, body composition analysis, and oral function performance as references to assess the risk of osteoporosis and help prevent osteoporosis-related fractures in the future.
We proposed an integrated approach for screening low bone mineral density; however, the present study had some limitations. First, evaluating the causal relationships in this cross-sectional study was difficult. We need to ensure continuous follow-up of these participants for mechanism-related explanations. Second, serum albumin data and bone mineral density of the femoral neck were collected only once from the participants, leading to deviations in the GNRI and T scores. These values vary over time, and a single time point cannot accurately represent long-term status. Third, some parameters related to bone mineral levels, such as menopausal status and hormone levels, may have been overlooked. Considering menopausal status or hormone levels, the factors we explored, such as GNRI and SMI, may demonstrate the significance of bone mineral density among female participants.
Conclusion
We identified the multidimensional aspects of bone mineral density, including physical frailty and oral health. Using this approach, we can detect low mineral density early in older adults, which can be expanded to prevent osteoporosis and osteoporosis-related fractures.
Data availability
The datasets used during the current study are available from the corresponding author on reasonable request.
References
Lane, N. E. Epidemiology, etiology, and diagnosis of osteoporosis. Am. J. Obstet. Gynecol. 194, S3-11. https://doi.org/10.1016/j.ajog.2005.08.047 (2006).
Feldbrin, Z. & Shargorodsky, M. Bone remodelling markers in hypertensive patients with and without diabetes mellitus: Link between bone and glucose metabolism. Diabetes Metab. Res. Rev. 31, 752–757. https://doi.org/10.1002/dmrr.2668 (2015).
Pouresmaeili, F., Kamalidehghan, B., Kamarehei, M. & Goh, Y. M. A comprehensive overview on osteoporosis and its risk factors. Ther. Clin. Risk Manag. 14, 2029–2049. https://doi.org/10.2147/tcrm.S138000 (2018).
Tang, G. et al. Low BMI, blood calcium and vitamin D, kyphosis time, and outdoor activity time are independent risk factors for osteoporosis in postmenopausal women. Front. Endocrinol. 14, 1154927. https://doi.org/10.3389/fendo.2023.1154927 (2023).
Pisulkar, S., Pisulkar, G., Pakhan, A. D., Godbole, S. & Dahane, T. Mandibular bone mineral density to predict skeletal osteoporosis: A literature review. Int. J. Recent Surg. Med. Sci. 02, 096–101. https://doi.org/10.5005/jp-journals-10053-0021 (2016).
Gobbens, R. J., van Assen, M. A., Luijkx, K. G., Wijnen-Sponselee, M. T. & Schols, J. M. Determinants of frailty. J. Am. Med. Dir. Assoc. 11, 356–364. https://doi.org/10.1016/j.jamda.2009.11.008 (2010).
Li, G. et al. An overview of osteoporosis and frailty in the elderly. BMC Musculoskelet. Disord. 18, 46. https://doi.org/10.1186/s12891-017-1403-x (2017).
Bouillanne, O. et al. Geriatric nutritional risk index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 82, 777–783. https://doi.org/10.1093/ajcn/82.4.777 (2005).
Endo, T. et al. A two-colored chewing gum test for assessing masticatory performance: A preliminary study. Odontology 102, 68–75. https://doi.org/10.1007/s10266-012-0089-7 (2014).
Hama, Y., Kanazawa, M., Minakuchi, S., Uchida, T. & Sasaki, Y. Properties of a color-changeable chewing gum used to evaluate masticatory performance. J. Prosthodont. Res. 58, 102–106. https://doi.org/10.1016/j.jpor.2013.12.005 (2014).
Atchison, K. A. & Dolan, T. A. Development of the geriatric oral health assessment index. J. Dent. Educ. 54, 680–687 (1990).
Weijenberg, R. A. et al. Two-colour chewing gum mixing ability: Digitalisation and spatial heterogeneity analysis. J. Oral Rehabil. 40, 737–743. https://doi.org/10.1111/joor.12090 (2013).
Chou, Y.-C. Validation of the Geriatric Oral Health Assessment Index in Taiwan. Master's degree thesis, Kaohsiung Medical University. https://hdl.handle.net/11296/g23763 (2010).
R: A Language and Environment for Statistical Computing (2022).
Afshinnia, F., Wong, K. K., Sundaram, B., Ackermann, R. J. & Pennathur, S. Hypoalbuminemia and osteoporosis: Reappraisal of a controversy. J. Clin. Endocrinol. Metab. 101, 167–175. https://doi.org/10.1210/jc.2015-3212 (2016).
Kiuchi, A. et al. Association between low dietary protein intake and geriatric nutrition risk index in patients with chronic kidney disease: A retrospective single-center cohort study. Nutrients 8, 662. https://doi.org/10.3390/nu8100662 (2016).
Thissen, J. P., Triest, S., Maes, M., Underwood, L. E. & Ketelslegers, J. M. The decreased plasma concentration of insulin-like growth factor-I in protein-restricted rats is not due to decreased numbers of growth hormone receptors on isolated hepatocytes. J. Endocrinol. 124, 159–165. https://doi.org/10.1677/joe.0.1240159 (1990).
Yakar, S. et al. Serum IGF-1 determines skeletal strength by regulating subperiosteal expansion and trait interactions. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 24, 1481–1492. https://doi.org/10.1359/jbmr.090226 (2009).
Kim, K. M., Jang, H. C. & Lim, S. Differences among skeletal muscle mass indices derived from height-, weight-, and body mass index-adjusted models in assessing sarcopenia. Korean J. Intern. Med. 31, 643–650. https://doi.org/10.3904/kjim.2016.015 (2016).
Taaffe, D. R. et al. Race and sex effects on the association between muscle strength, soft tissue, and bone mineral density in healthy elders: The health, aging, and body composition study. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 16, 1343–1352. https://doi.org/10.1359/jbmr.2001.16.7.1343 (2001).
Rolland, Y. et al. Frailty, osteoporosis and hip fracture: Causes, consequences and therapeutic perspectives. J. Nutr. Health Aging 12, 335–346. https://doi.org/10.1007/bf02982665 (2008).
Soto, M. E. et al. Frailty and the interactions between skeletal muscle, bone, and adipose tissue-impact on cardiovascular disease and possible therapeutic measures. Int. J. Mol. Sci. 24, 4534. https://doi.org/10.3390/ijms24054534 (2023).
Muñoz-Garach, A., García-Fontana, B. & Muñoz-Torres, M. Nutrients and dietary patterns related to osteoporosis. Nutrients 12, 1986. https://doi.org/10.3390/nu12071986 (2020).
Abe, A. et al. Correlation between geriatric nutritional risk index and oral condition in gastric cancer patients. Oral Dis. 29, 836–842. https://doi.org/10.1111/odi.14035 (2023).
Madarina, A., Kusdhany, L. S. & Mahiddin, F. G. Mandibular bone osteoporosis and oral health-related quality of life in the elderly. J. Int. Dent. Med. Res. 10, 423–428 (2017).
Dibello, V. et al. Oral health indicators and bone mineral density disorders in older age: A systematic review. Ageing Res. Rev. 100, 102412. https://doi.org/10.1016/j.arr.2024.102412 (2024).
Zhang, W. et al. Immunoporosis: Role of immune system in the pathophysiology of different types of osteoporosis. Front. Endocrinol. 13, 965258. https://doi.org/10.3389/fendo.2022.965258 (2022).
Xi, L. et al. Investigation of bone matrix composition, architecture and mechanical properties reflect structure–function relationship of cortical bone in glucocorticoid induced osteoporosis. Bone 136, 115334. https://doi.org/10.1016/j.bone.2020.115334 (2020).
Cheng, C. H., Chen, L. R. & Chen, K. H. Osteoporosis due to hormone imbalance: An overview of the effects of estrogen deficiency and glucocorticoid overuse on bone turnover. Int. J. Mol. Sci. 23, 1376. https://doi.org/10.3390/ijms23031376 (2022).
Acknowledgements
We are grateful to Miss Yu-Ping Wang and Mr. Chun-Wei Su for collecting and preprocessing the data.
Funding
This research was supported by a grant from Academia Sinica, Taiwan (Grant Number AS-HLGC-110-01). The funder had no role in the study design, data collection and analysis, decision to publish, or manuscript preparation.
Author information
Authors and Affiliations
Contributions
P.C.C. contributed to conception, design, data collection, data analysis, interpretation and drafted the manuscript. T.C.C. contributed to conception, design, and interpretation, acquired to research resources, and critically revised the manuscript. All the authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chung, PC., Chan, TC. Physical frailty and oral health as risk factors for low bone density in community-dwelling residents. Sci Rep 14, 18131 (2024). https://doi.org/10.1038/s41598-024-68958-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-68958-8
- Springer Nature Limited