
Abstract
Mineral Trioxide Aggregate (MTA) is the gold standard for vital pulp treatment (VPT), but its superiority over novel calcium silicate-based cements in permanent teeth lacks systematic evidence. This study aimed to compare the efficacy of these materials in VPT through a network meta-analysis. A systematic search was conducted in MEDLINE, EMBASE, Cochrane Library, and Web of Science until January 20, 2024. The inclusion criteria were randomized controlled trials involving VPT with biomaterials and reversible or irreversible pulpitis diagnoses in mature permanent teeth. The primary outcome was the odds ratio (OR) of failure rates with 95% confidence intervals. In the 21 eligible trials, failure rates were significantly higher with calcium-hydroxide than MTA at six (OR 2.26 [1.52-3.36]), 12 (OR 2.53 [1.76-3.62]), and 24 months (OR 2.46 [1.60-3.79]). Failure rates for Totalfill at six (OR 1.19 [0.55-2.58]) and 12 months (OR 1.43 [0.71-2.92]), and Biodentine at six (OR 1.09 [0.66-1.78]), 12 (OR 1.21 [0.74-1.96]), and 24 months (OR 1.47 [0.81-2.68]) were not significantly different from MTA. The results were similar in the direct pulp capping subgroup, whereas, in the partial and full pulpotomy subgroup, there was not enough evidence to achieve significant differences. MTA, Biodentine, and Totalfill are the most efficient materials for VPT. However, calcium-hydroxide-based materials are not recommended in VPT.
Similar content being viewed by others
Introduction
Vital pulp treatment (VPT, alternatively, the vital pulp therapy), such as pulp capping, partial pulpotomy, or full pulpotomy, offers a faster, less invasive, and technically simpler alternative to root canal treatment for the treatment of deep carious lesions and exposed pulp1. VPT could be at least as successful as root canal treatment2,3,4.
VPT aims to preserve pulp vitality and function5; therefore, the innate immune defense mechanism of the pulp is retained6. In contrast, loss of pulp vitality results in impaired receptor function, such as the sensation of biting forces7,8. The pulp tissue in a tooth acts as a shock absorber during biting and chewing9 and by influencing proprioceptive sensation, potentially providing a higher tolerance to mechanical stress and reducing the risk of tooth fracture8,10,11.
A key factor in the success of VPT is the bioactive material applied to the pulp tissue1,12,13. Mineral Trioxide Aggregate (MTA) is the gold standard material for VPT12,13. Its biocompatibility has been demonstrated in vitro14,15, in vivo16,17, and in case report18. The pH of MTA is high during the setting process; therefore, it has an excellent antimicrobial effect19,20. Clinical studies21,22,23 have reported a high success rate of MTA in VPT. However, the clinical application and mixing of MTA are not straightforward, but maintaining a proper mixing ratio of the components affects the physical characteristics of MTA20. In addition, MTA has a long setting time24,25 and needs excess water for the complete setting process20. Although the newer version of MTA has a reduced setting time, Biodentine is still the fastest26. Nevertheless, MTA may cause tooth discoloration27,28,29.
Over the past 10–15 years, several bioactive materials have been developed for VPT to replace MTA. For example, Biodentine has a faster setting time and causes less discoloration on the tooth30. TheraCalLC is a light-curing resin-modified calcium silicate-based material31 with a dentin bridge formation similar to MTA32. However, TheraCalLC has shown higher in vitro cytotoxicity than MTA or Biodentine33. Totalfill is a premixed calcium silicate-based root repair material with an excellent clinical success rate34. The calcium-enriched mixture (CEM) contains calcium oxide (CaO), sulfur trioxide (SO3), phosphorous pentoxide (P2O5), and silicon dioxide (SiO2)35. CEM has good sealing ability and antimicrobial effects36,37.
Some previous pairwise meta-analyses have compared the MTA with the Ca(OH)2. The MTA was found to be superior to Ca(OH)2 in direct pulp capping of permanent teeth after three months38 and at 12 and 24 months39. However, after indirect pulp capping, the difference was not significant at 6 and 12 months40. However, less evidence is available for pulpotomy. A meta-analysis based on cohort studies41 found no significant superiority of CEM or MTA over Ca(OH)2 after full pulpotomy in matured permanent teeth. More recently, a meta-analysis of randomized controlled trials42 found significant superiority of MTA over Ca(OH)2 in direct pulp capping and pulpotomy.
In addition, previous pairwise meta-analyses have compared the MTA with new biomaterials. The efficacy of Biodentin was comparable to that of MTA in direct pulp capping39. Similarly, calcium silicate-based materials were similar to MTA in other VPT modalities43. However, the biomaterials were combined into a single group. Whether the new biomaterials had a distinct effect on the success rate based on the VPT modalities and follow-up period remains to be answered. Therefore, a stratified network meta-analysis is proposed to compare MTA, Ca(OH)2, and different calcium silicate-based materials considering the follow-up period and using only RCTs in matured permanent teeth.
The primary objective of this study was to compare the clinical failure rate of calcium-hydroxide-based and contemporary bioactive materials in VPT of permanent teeth to MTA. The secondary aim was to perform a subgroup analysis based on intervention types by comparing the direct and indirect pulp capping and partial and full pulpotomy. This study aimed to rank these bioactive materials by network meta-analysis44.
Materials and methods
Protocol and registration
This systematic review and meta-analysis were conducted according to the Preferred Reporting Items for Systematic Reviews and Network Meta-Analyses (PRISMA-NMA) guidelines45,46. It was registered in the Prospectively Registered Systematic Reviews (PROSPERO) database (CRD42022375573).
Eligibility criteria
The PICOS framework was used. The clinical question was: Is there a difference in failure rate between different bioactive materials and MTA in the vital pulp treatment of permanent teeth?
The PICOS details were as follows:
P: Mature permanent teeth with vital pulp therapy.
I: Bioactive materials (BiodentineTM, Ca(OH)2, CEM, Calcium Silicate-based Sealer, Calcium silicate-based materials).
C: Mineral Trioxide Aggregate (MTA).
O: Failure rate.
S: Randomized controlled trials.
Inclusion criteria for studies
Randomized controlled trials were included. Studies with preoperative diagnosis, a description of the clinical procedure, and biomaterials. Studies with the initial diagnosis of reversible or irreversible pulpitis or Wolters classification-based pulpitis47. The failure of VPT was defined as having clinical symptoms, pain, sensitivity to cold and percussion tests, and/or signs of periapical inflammation. The number of study participants in each follow-up period is defined. The minimum follow-up period was six months.
Exclusion criteria for studies
The exclusion criteria of studies are the following: case reports, two-armed interventional, cohort, and case-controlled studies, meta-analyses, reviews, animal studies, conference abstracts, non-English written papers, and the study population involved primary dentition, immature permanent teeth, and trauma cases.
Information sources and search strategy
An electronic literature search was conducted using the following databases: MEDLINE (PubMed), EMBASE, Cochrane Library, and Web of Science. A citation chase was performed (https://www.rayyan.ai/). The following search key was used: (vital pulp therapy OR vital-pulp therapy OR direct pulp capping OR direct pulp-capping OR indirect pulp capping OR indirect pulp-capping OR partial pulpotomy OR partial-pulpotomy OR full pulpotomy OR full-pulpotomy OR pulp capping OR pulp-capping) AND (Biodentine OR CEM OR Calcium Silicate Sealer OR Calcium-silicate based materials OR calcium silicate-based material OR calcium hydroxide OR MTA OR pulp capping material* OR calcium silicate OR calcium silicate materials OR biomaterial*) AND (Adult* OR mature tooth OR mature teeth OR permanent teeth OR permanent tooth OR permanent OR mature).
The systematic search was completed on January 20, 2024. All articles were imported into EndNote 20 for duplicate removal. The articles were arranged alphabetically for manual screening. First, automatic duplicate removal was performed in EndNote 20, followed by manual duplicate removal. Then, the database was uploaded to the Rayyan system (https://www.rayyan.ai/).
Selection process
The entire selection process was conducted simultaneously by two independent observers (P.K. and O.V.), with each observer evaluating articles based on their title, abstract, and full text. The first screening involved the titles and the abstracts of the articles. Then, a full-text selection was completed for all studies that met the inclusion criteria or when there was insufficient information in the abstract to make a proper decision. Conflicts were resolved through discussion with the two reviewers. The same two independent researchers reviewed the full texts for quality and inclusion in the network meta-analysis. A third author (K.K.) was also involved in case of disagreement.
Data collection/extraction process
Two independent observers collected data, P.K. and O.V. No automatic tools were used for data extraction. First, the data of some articles that matched the inclusion criteria was extracted into an MS Excel sheet form. The statistician verified the form first. Studies declared that only the percentage of failed and successful cases without absolute numbers were excluded from the meta-analysis.
Data items/Effect measure
The verified MS Excel form was used for data extraction of all included studies, comprising the following information: publication information (author/year), study type, demographics of study participants, pulpal diagnosis, type of vital pulp treatment, materials applied, follow-up times, and numbers lost to follow-up. The primary outcomes were vital pulp treatment failure rates after six months, 12 months, and 24 months. The effect measure was the odds ratio (OR) with 95% confidence intervals48. If the tested material had an odds ratio of higher than one, indicating a higher failure rate for the tested material than for the MTA group.
Some studies49,50,51,52,53 did not calculate the previously lost unsuccessful cases for every follow-up. Therefore, the authors of this study added the number of unsuccessful lost cases to the number of participants at the subsequent follow-up for the meta-analysis to obtain the actual failure rate.
Risk of bias (RoB) assessment
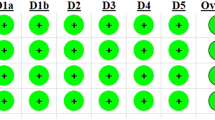
According to the Cochrane Collaboration, the risk of bias in the randomized clinical trials was analyzed by the Risk of Bias 2 tool (https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials). The Risk of Bias 2 tool consists of five domains: randomization process (D1), deviations from intended interventions (D2), missing outcome data (D3), measurement of outcome (D4), selection of reported results (D5). Each domain can have three different results: low risk, some concern, and high risk. The worst domain result will set the overall bias of the particular study.
Synthesis methods
First, pooled analysis was performed separately for data from all treatment modalities (including indirect and direct pulp capping and partial and full pulpotomy) at each follow-up interval (6, 12, and 24 months). In the second step, subgroup analysis was conducted separately for each treatment modality (indirect pulp capping, direct pulp capping, partial pulpotomy, and full pulpotomy) at each follow-up interval, provided a minimum of three eligible studies were available for each subgroup.
A frequentist method was used to perform the network meta-analyses (NMAs). As we assumed considerable between-study heterogeneity due to the nature of medical treatments and conditions, a random-effects model was used to pool effect sizes (ORs) with a 95% confidence interval (95% CI). The reason for using this method for dichotomous data is zero events in the studies. This method handles zero events with correction. The network plot indicates the strength of the comparisons between materials by depicting the number of patients and studies.
The three follow-up periods were analyzed in a stratified manner. Forest plots were used to examine the consistency of the relationship between direct, indirect, and network point estimates. Consistency means that the relative effect of a comparison based on direct evidence does not differ from the one based on indirect evidence54. The evidence plot shows direct and indirect estimation ratios in the network meta-analysis. Funnel plots were constructed for all outcomes, and Egger's tests were performed to assess the small-study effect. P-scores rank treatments, which measure the certainty that one treatment is better than another treatment, and are averaged over all competing treatments. P-score ranges from 0 to 1, with higher values indicating higher ranks. Calculations were performed using the R package (version 4.1.1), Netmeta (version 2.7–0), and Pairwise (version 0.6.0–0). Netmeta could estimate network meta-analysis models within a frequentist framework and derive from graph-theoretical techniques initially developed for electrical networks55.
Certainty assessment
The certainty assessment was evaluated according to CINeMA (Confidence in Network Meta-Analysis). CINeMA includes six domains: within-study bias, reporting bias, indirectness, imprecision, heterogeneity, and incoherence56,57. There are three levels of judgment for each domain (no concerns, some concerns, or major concerns). Domain judgments can be summarized into four confidence levels for each outcome: very low, low, moderate, or high.
CINeMA considers the agreement between the confidence and prediction intervals to assign a score for 'heterogeneity' for each NMA effect (i.e. pair of cements). Prediction intervals provide a range within which the true effect of a new study is likely to lie57. The imprecision and heterogeneity scores were based on an arbitrarily chosen odds ratio of 1.2, which was considered clinically important.
Ethics approval statement and document
No ethical approval was required for this systematic review and network meta-analysis, as all data were published in peer-reviewed journals. Datasets used in this study can be found in the full-text articles included in systematic reviews and network meta-analyis.
Results
Study selection
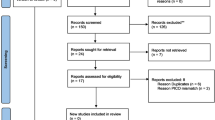
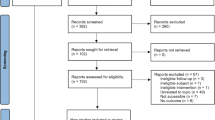
The systematic search revealed 2119 records in MEDLINE (820), EMBASE (741), CENTRAL (306), and Web of Science (252). Automatic and manual removal of duplicates resulted in 1264 articles. After title and abstract selection, 80 eligible articles remained. Cohen's kappa was 0.96 between the two independent observers. After full-text reading, 21 articles were selected4,34,49,50,51,52,53,58,59,60,61,62,63,64,65,66,67,68,69,70,71. Cohen’s kappa of the full-text selection was 0.89 (Fig. 1). The excluded studies and the reason for exclusion are listed in Supplementary Table 1.

Prisma 2020 flow diagram of the screening and selection process.
Study characteristics
Baseline characteristics of the 21 included studies are presented in (Table 1). The number of treated and lost patients and the successful and unsuccessful cases in every follow-up period, funding source, and conflict of interest were recorded. The network plot (Figs. 2A, 3A, 4A, 5A, 6A, 7A,8A, 9A, 10A, 11A) indicates the number of direct comparisons between materials for the 6, 12, and 24 month follow-up periods. The description of the used materials is presented in Supplementary Table 2.

Comparing MTA and investigated bioactive materials at 6 months follow-up—pooled data, including all treatment modalities (A) Network-plot: An orange circle represents every bioactive material; the circle size represents the number of treated patients. The width of the lines and the numbers represent the number of studies where a direct comparison was made. (B) P-score: The p-score represents a ranking between the compared materials. (C) Outcome forest plot: The zero effect is the MTA vs. the other materials. The grey squares represent the odds ratio (OR), and the length of the black lines shows 95% (CI) confidence intervals.

Comparing MTA and investigated bioactive materials at 12 months follow-up—pooled data, including all treatment modalities (A) Network-plot: An orange circle represents every bioactive material; the circle size represents the number of treated patients. The width of the lines and the numbers represent the number of studies where a direct comparison was made. (B) P-score: The p-score represents a ranking between the compared materials. (C) Outcome forest plot: The zero effect is the MTA vs. the other materials. The grey squares represent the odds ratio (OR), and the length of the black lines shows 95% (CI) confidence intervals.

Comparing MTA and investigated bioactive materials at 24 months follow-up—pooled data, including all treatment modalities (A) Network-plot: An orange circle represents every bioactive material; the circle size represents the number of treated patients. The width of the lines and the numbers represent the number of studies where a direct comparison was made. (B) P-score: The p-score represents a ranking between the compared materials. (C) Outcome forest plot: The zero effect is the MTA vs. the other materials. The grey squares represent the odds ratio (OR), and the length of the black lines shows 95% (CI) confidence intervals.

Comparing MTA and investigated bioactive materials at 6 months follow-up—indirect pulp capping (A) Network-plot: An orange circle represents every bioactive material; the circle size represents the number of treated patients. The width of the lines and the numbers represent the number of studies where a direct comparison was made. (B) P-score: The p-score represents a ranking between the compared materials. (C) Outcome forest plot: The zero effect is the MTA vs. the other materials. The grey squares represent the odds ratio (OR), and the length of the black lines shows 95% (CI) confidence intervals.

MTA and investigated bioactive materials at 6 months follow-up—direct pulp capping (A) Network-plot: An orange circle represents every bioactive material; the circle size represents the number of treated patients. The width of the lines and the numbers represent the number of studies where a direct comparison was made. (B) P-score: The p-score represents a ranking between the compared materials. (C) Outcome forest plot: The zero effect is the MTA vs. the other materials. The grey squares represent the odds ratio (OR), and the length of the black lines shows 95% (CI) confidence intervals.

MTA and investigated bioactive materials at 12 months follow-up—direct pulp capping (A) Network-plot: An orange circle represents every bioactive material; the circle size represents the number of treated patients. The width of the lines and the numbers represent the number of studies where a direct comparison was made. (B) P-score: The p-score represents a ranking between the compared materials. (C) Outcome forest plot: The zero effect is the MTA vs. the other materials. The grey squares represent the odds ratio (OR), and the length of the black lines shows 95% (CI) confidence intervals.

MTA and investigated bioactive materials at 24 months follow-up—direct pulp capping (A) Network-plot: An orange circle represents every bioactive material; the circle size represents the number of treated patients. The width of the lines and the numbers represent the number of studies where a direct comparison was made. (B) P-score: The p-score represents a ranking between the compared materials. (C) Outcome forest plot: The zero effect is the MTA vs. the other materials. The grey squares represent the odds ratio (OR), and the length of the black lines shows 95% (CI) confidence intervals.

Comparing MTA and investigated bioactive materials at 12 months follow-up—partial pulpotomy (A) Network-plot: An orange circle represents every bioactive material; the circle size represents the number of treated patients. The width of the lines and the numbers represent the number of studies where a direct comparison was made. (B) P-score: The p-score represents a ranking between the compared materials. (C) Outcome forest plot: The zero effect is the MTA vs. the other materials. The grey squares represent the odds ratio (OR), and the length of the black lines shows 95% (CI) confidence intervals.

Comparing MTA and investigated bioactive materials at 6 months follow-up—full pulpotomy (A) Network-plot: An orange circle represents every bioactive material; the circle size represents the number of treated patients. The width of the lines and the numbers represent the number of studies where a direct comparison was made. (B) P-score: The p-score represents a ranking between the compared materials. (C) Outcome forest plot: The zero effect is the MTA vs. the other materials. The grey squares represent the odds ratio (OR), and the length of the black lines shows 95% (CI) confidence intervals.

Comparing MTA and investigated bioactive materials at 12 months follow-up—full pulpotomy (A) Network-plot: An orange circle represents every bioactive material; the circle size represents the number of treated patients. The width of the lines and the numbers represent the number of studies where a direct comparison was made. (B) P-score: The p-score represents a ranking between the compared materials. (C) Outcome forest plot: The zero effect is the MTA vs. the other materials. The grey squares represent the odds ratio (OR), and the length of the black lines shows 95% (CI) confidence intervals.
Risk of Bias assessment
Five studies showed high risk, twelve had some concern, and four indicated low risk (Supplementary Fig. 1).
Assessment of publication bias
All funnel plots were inverted and symmetric in all follow-up periods and subgroups, indicating no small study effect (Supplementary Figs. 2–11). Egger’s p values also indicate the lack of publication bias in all three follow-ups72,73.
Certainty of evidence
After comparing materials based on pooled data at each follow-up interval, concerns regarding imprecision and heterogeneity prompted a downgrade in the certainty of evidence. The heterogeneity in pooled data at six and 24 month data was more pronounced. It was pronounced at those material comparisons where the number of direct data was small. Similarly, imprecision, heterogeneity, and incoherence warranted downgrading within the direct pulp capping subgroups. The appearance of heterogeneity in the direct pulp capping subgroup at all follow-up periods was pronounced. It was also pronounced in those material comparisons where the number of direct data was few. The main concerns in imprecision and heterogeneity were observed in the indirect pulp capping subgroup. The main concern in the partial and full pulpotomy subgroups was imprecision (see Supplementary Figs. 12–37). Consequently, the certainty of evidence ranged from high to very low across all subgroups.
The outcome of the studies
Pooled data, including all treatment modalities at the six-month follow-up
The total number of patients included in the network analysis was 1932, with 257 failure events. The comparison structure is depicted in the network graph (Fig. 2A). Based on the p-score (Fig. 2B), the materials ranked from lowest to the highest OR as follows: CEM, MTA, Biodentine, TotalFill, TheraCalLC, Ca(OH)2, Ca(OH)2LC.
No significant difference was observed in the OR between CEM, Biodentine, Totalfill, and TheraCalLC groups compared to MTA (Fig. 2C, Supplementary Figs. 38, 48). However, the OR was significantly higher in the Ca(OH)2 and Ca(OH)2LC groups than in the MTA group.
Pooled data, including all treatment modalities at the 12 month follow-up
The total number of patients in the network analysis was 2158, with 333 failure events. The comparison structure is depicted in the network graph (Fig. 3A). Based on the p-score, the materials ranked from lowest to the highest OR as follows: MTA, CEM, Biodentine, TotalFill, TheraCalLC, Ca(OH)2, and Ca(OH)2LC (Fig. 3B).
No significant difference was observed in the OR between CEM, Biodentine, and TotalFill groups compared to MTA (Fig. 3C, Supplementary Figs. 39, 49). However, the OR was significantly higher in the TheraCalLC, Ca(OH)2, and Ca(OH)2LC groups than in the MTA group.
Pooled data, including all treatment modalities at the 24 month follow-up
The total number of patients in the network analysis was 1107, with 257 failure events. The comparison structure is illustrated in the network graph (Fig. 4A). Based on the p-score, the materials ranked from lowest to the highest OR as follows: MTA, Biodentine, TheraCalLC, TotalFill, CEM, Ca(OH)2, and Ca(OH)2LC (Fig. 4B). The probability of MTA's rank gradually increased from six to 24 months.
No significant difference was observed in the OR between Biodentine, TotalFill, and CEM groups compared to MTA (Fig. 4C, Supplementary Figs. 40, 50). However, there was no direct comparison between CEM and the other materials except between CEM and MTA. The OR was significantly higher in TheraCalLC, Ca(OH)2, and Ca(OH)2LC groups than in the MTA group.
Indirect pulp capping at the six-month follow-up
Four studies were included with 239 patients and 17 failure events. The comparison structure is illustrated in the network graph (Fig. 5A). Based on the p-score (Fig. 5B), the materials ranked from lowest to highest OR are Biodentine, MTA, Ca(OH)2. No significant difference was observed in the OR between Biodentine and Ca(OH)2 groups compared to MTA (Fig. 5C, Supplementary Figs. 41, 51).
Direct pulp capping at the six-month follow-up
Seven studies were included with 1243 patients and 182 failure events. The comparison structure is depicted in the network graph (Fig. 6A). Based on the p-score (Fig. 6B), the materials ranked from lowest to highest OR are as follows: CEM, MTA, Biodentine, TheraCalLC, Ca(OH)2, Ca(OH)2LC.
No significant difference was observed in the OR between CEM, Biodentine, and TheraCalLC groups compared to MTA (Fig. 6C, Supplementary Figs. 42, 52). Failure was significantly more likely in Ca(OH)2 and Ca(OH)2LC groups higher than in the MTA group. However, there were just two direct comparisons of CEM with Ca(OH)2 and MTA.
Direct pulp capping at the 12 month follow-up
Six studies were included, with 1122 and 231 failure events. The comparison structure is illustrated in the network graph (Fig. 7A). Based on the p-score, the materials ranked from lowest to the highest OR as follows: CEM, MTA, Biodentine, TheraCalLC, Ca(OH)2, and Ca(OH)2LC (Fig. 7B).
No significant difference in the OR was observed between CEM, Biodentine, and TheraCalLC groups compared to MTA (Fig. 7C, Supplementary Figs. 43, 53). The OR was significantly higher in TheraCalLC, Ca(OH)2, and Ca(OH)2LC groups than in the MTA group.
Direct pulp capping at the 24 month follow-up
Three studies were included with 667 patients and 209 failure events. The comparison structure is shown in the network graph (Fig. 8A). Based on the p-score, the materials ranked from lowest to the highest OR as follows: MTA, Biodentine, TheraCalLC, Ca(OH)2, and Ca(OH)2LC (Fig. 8B).
No significant difference was observed in the OR between Biodentine compared to MTA (Fig. 8C, Supplementary Figs. 44, 54). The OR was significantly higher in TheraCalLC, Ca(OH)2, and Ca(OH)2LC groups than in the MTA group.
Partial pulpotomy at the 12 month follow-up
Three studies were included with 250 patients and 33 failure events. The comparison structure is shown in the network graph (Fig. 9A). Based on the p-score (Fig. 9B), the materials ranked from lowest to the highest OR are as follows: Biodentine, MTA, TotalFill, Ca(OH)2.
No significant difference was observed in the OR between Biodentine, TotalFill, and Ca(OH)2 groups compared to MTA (Fig. 9C, Supplementary Figs. 45, 55).
Full pulpotomy at the six-month follow-up
Three studies were included with 207 patients and 27 failure events. The comparison structure is shown in the network graph (Fig. 10A). Based on the p-score (Fig. 10B), the materials ranked from lowest to highest OR are as follows: Ca(OH)2, TotalFill, MTA, and Biodentine.
No significant difference was observed in the OR between Ca(OH)2, TotalFill, and Biodentine groups compared to MTA (Fig. 10C, Supplementary Figs. 46, 56).
Full pulpotomy at the 12 month follow-up
Four studies were included with 581 patients and 56 failure events. The comparison structure is depicted in the network graph (Fig. 11A). Based on the p-score (Fig. 11B), the materials ranked from lowest to highest OR are as follows: Biodentine, Ca(OH)2, MTA, TotalFill, and CEM. Compared to MTA, the OR was not significantly different between the Biodentine, Ca(OH)2, TotalFill, and CEM groups (Fig. 11C, Supplementary Figs. 47, 57).
Discussion
The current network meta-analysis showed solid statistical evidence for MTA over Ca(OH)2 products, such as Ca(OH)2 and Ca(OH)2LC, with a 2–3 times higher failure rate in VPT over two years. Therefore, the first null hypothesis comparing Ca(OH)2 products, such as Ca(OH)2 and Ca(OH)2LC with MTA, regardless of the treatment modalities, was rejected.
The second hypothesis was partially rejected. The Ca(OH)2 resulted in three times more failure than the MTA in direct pulp capping. No significant difference was observed between MTA and Ca(OH)2 in pulpotomy groups. Nevertheless, only a few studies were eligible and did not compare directly (full pulpotomy at 6 and 12 months), resulting in high confidence intervals. However, it is not rational based on its significant inferiority even in the least severe pulp lesion, including Ca(OH)2 in future pulpotomy randomized clinical trials.
In contrast to our results, most previous studies34,49,62,64 found no significant difference between Ca(OH)2 and MTA at six-month follow-ups. Despite the higher odds ratio for Ca(OH)2 and for Ca(OH)2LC than for MTA, the limited sample size of the individual studies prevented a conclusion from being drawn. However, synthesizing the individual study results by meta-analysis could provide a high level of evidence74,75.
In addition, a recent retrospective cohort study76 has found success rates of 100%, 95%, 95%, 86%, and 89% for direct pulp capping at 1, 5, 10, 20, and 35 years of follow-up with Ca(OH)2 (Dycal, Dentsply), respectively. However, the careful methodology developed by the author might explain these excellent results. In the case of medium/large pulp exposure, the calcium-hydroxide powder was applied to the pulp to control the moisture before Dycal application. It is important to note that the same person performed the treatment and evaluation, indicating a possible bias.
Most randomized clinical trials that compared Ca(OH)2 to MTA49,50,61,62,63,64,67,68,71 included teeth with reversible pulpitis and direct or indirect pulp capping without pulpotomy. The success rates of these studies varied widely, between 58 and 96% at six months, 64 and 92% at 12 months, and 40 and 92% at 24 months. However, the success rates of MTA in the same studies (direct comparison) were more consistent, between 84 and 100% at six months and 83 and 98% at 12 months. At 24 months, the success rates ranged from 85 to 100% after excluding one study61. This study reported a crude failure rate of 13.6%. However, to align with the methodology of other studies in the meta-analysis, the failure rate was recalculated, excluding lost cases. This recalculation yielded an unrealistically low failure rate of 45% with MTA. The involvement of 43 dental practices may have introduced bias, leading to the loss of an exceptionally high number of cases (135 out of 183) during follow-up, thus significantly distorting the reported rates.
No subgroup analysis could be conducted in this meta-analysis for pulpotomy because only one randomized clinical trials34 performed pulpotomy with Ca(OH)2. In that particular study, the odds ratios for Ca(OH)2/MTA were high: 3.23 at six months, 4.09 at 12 months, and 7.15 at 24 months, indicating a clear advantage of MTA over the Ca(OH)2 in pulpotomy after irreversible pulpitis.
In a histological study on animals, Ca(OH)2 induced less dentin bridge formation after direct pulpal application than MTA77. Twelve of the 15 teeth that underwent Ca(OH)2 treatment developed pulp inflammation; only the rest formed dentin bridges without signs of inflammation. It is hypothesized that the inadequate adhesion of calcium-hydroxide-based materials to the tooth structure, their low mechanical strength, and solubility can result in microleakage and dental pulp infection78. Ca(OH)2 forms only a weak mineralized barrier with high permeability. The high dissolvability of Ca(OH)2 disintegrates the material, leaving voids 79. This is a potential way for reinfection and a possible reason for the higher failure rate in VPT79.
Compact hard tissue formation without bacterial invasion is crucial for successful vital pulp treatment, and this depends on the sealing ability of the capping material80. In contrast to Ca(OH)2, bioactive tricalcium silicate-based cements can create an ideal healing environment and form reparative dentin81. They also have a better sealing ability than CaOH2, which is likely one of the main reasons for their success79,80.
The hypothesis that the newer bioactive materials would be as efficient in VPT as MTA was partially rejected as TheraCalLC was inferior to MTA at 12 and 24 months by significant odds ratios of 2.09 and 2.10. TheraCalLC is a resin-modified light-curing calcium silicate-based material. The TheraCalLC was only used for direct pulp capping in the included studies. The material has low solubility, fast setting time, and good sealing ability82. However, no calcium-hydroxide formation was observed during hydration with TheraCalLC83. Calcium-hydroxide is highly effective in stimulating odontoblast activity, directly resulting in mineralization84. Therefore, these specific properties might be attributed to the low performance at 12 and 24 months.
CEM has an antimicrobial effect37 and a good sealing ability36, which are essential for the success of VPT. This meta-analysis comparing CEM to MTA, including all treatment modalities, indicated a non-significant odds ratio of 0.15, 0.97, and 3.32 at six, 12, and 24 months. Similar results were obtained in the direct pulp capping subgroup with reversible pulpitis at both six and 12 month follow-ups in the full pulpotomy subgroup with irreversible pulpitis at 12 months. However, only three randomized clinical trials4,60,67 could be included for comparison between CEM and MTA. Consequently, more studies are necessary to increase the level of evidence for CEM.
The network meta-analysis showed that Totalfill was not inferior to MTA at each follow-up in the pooled subgroups. Three studies were included in the six- and 12-month follow-ups, but only one study in the 24 month follow-ups. The TotalFill demonstrated non-inferiority to MTA in the 12 month partial pulpotomy and six- and 12 month full pulpotomy subgroups. It should be noted that the partial pulpotomy subgroup included one study with TotalFill, while the full pulpotomy subgroups included three studies. Totalfill is a calcium silicate-based repair material with beneficial biological properties58. The manufacturer already premixes TotalFill, so no further preparation is required. TotalFill demonstrates optimal biocompatibility, no cytotoxicity, and has an osteogenic property85. Totalfill does not shrink during setting and is hydrophilic and insoluble in tissue fluids86.
The current meta-analysis showed that the clinical efficacy of Biodentine in VPT is not inferior to MTA in any subgroups of treatment modality, suggesting that it has an excellent alternative. Biodentine shows high cytocompatibility87 and has good antimicrobial potential88. Fast setting time and less discoloring potential are favorable clinical properties30. Biodentine has beneficial regenerative properties that improve dental pulp stem cell proliferation, attachment, and migration89. Furthermore, Biodentine was more effective in promoting mineralization than MTA90.
A recently published meta-analysis compared calcium silicate and hydroxide-based materials to MTA91. However, this study performed a network meta-analysis to compare all materials studied directly and indirectly. Through the network meta-analysis, additional materials could be included, such as TheraCalLC, TotalFill, and Ca(OH)2LC. Consequently, materials could be ranked according to their clinical efficacy. Another distinction was that we excluded immature and trauma cases and focused solely on mature permanent teeth, which is more clinically relevant for dentists treating adult patients. In addition, we included 24-month follow-up periods contrary to the 12 month follow-up in the previous study. Although the authors of the previous meta-analysis noted that additional studies were required to determine success rates accurately, we addressed this issue using a bias elimination calculation method.
Strengths and limitations
An essential strength of the current analysis is that all studies included were randomized controlled trials with large sample sizes. In addition, some original data was reevaluated to derive precise estimates of odds ratios by standardizing the calculation across the studies. A successful subgroup analysis for the direct pulp capping revealed that Ca(OH)2 performs poorly even in the least severe pulp lesions.
However, the present study has limitations due to weak arms for some of the comparisons and subgroups. Specifically, CEM was compared only to MTA and Ca(OH)2 at six and 12 months and only to MTA at 24 months, whereas Totalfill was only compared to MTA and Biodentine and Ca(OH)2. In addition, CEM was used in only three studies, warranting caution in interpreting the results. These weaker comparison arms may impact the accuracy of the findings. However, as the odds ratio of conventional Ca(OH)2 is significantly higher than MTA, it would be unfeasible and ethically questionable to include Ca(OH)2 in a large-scale study comparing new bioactive materials to it.
In the pooled results, heterogeneity was not a severe problem. However, in subgroup analyses, heterogeneity increased, but imprecision was the primary concern. This is because there are few randomized clinical trials with more clinically complicated situations, such as symptomatic cases with a partial or complete pulpotomy. Four studies4,53,58,69 included full pulpotomy, and three studies34,68,70 included partial pulpotomy. In one study60, the extent of the pulpotomy was not defined, and another study did not distinguish between direct pulp capping and full pulpotomy51. The rest of the studies did not apply pulpotomy or did not declare it.
The longest follow-up in the included studies was 24 months, except for one article, Peskersoy et al.64. The limited duration of follow-up for VPT restricts the ability to draw long-term conclusions from the results.
Implications for research
A review of the articles clarified that critical demographic data, such as sex, age, and tooth types, were either not published or lacked stratified results. Given the influence of age in clinical decision-making, it is necessary to conduct studies involving mature permanent teeth, including middle-aged and possibly elderly individuals.
It is also crucial to report the number of cases lost to follow-up and calculate failure rates considering the lost cases.
In conventional asymptomatic pulp capping, MTA has shown promising results. However, neither study directly compared the reversible and irreversible pulpitis; many did not classify the pulpal state, nor did the studies use the Wolters classification47. Further studies with larger sample sizes are needed to establish the best clinical practice for treating irreversible pulpitis, as recommended by Wolters et al.47.
More extended follow-up periods are strongly recommended. Some of the included studies did not report all follow-up periods. It would also be helpful to look at the trends in failure over the whole follow-up period.
Implications for practice
Ca(OH)2 is not recommended for any vital pulp treatment, including pulp capping. However, newer calcium silicate-based materials such as Biodentine and Totalfill, which offer improved treatment properties, can be considered as alternatives to MTA. Based on the results of the present study, it can be concluded that MTA has the best clinical performance in VPT. It is important to emphasize that the handling and setting time of MTA is worse than that of Biodentine. In those clinical situations where setting time is relevant, Biodentine is the preferred material. Newer MTA products may be better at handling tooth discoloration, but they are still inferior to Biodentine. In cases where aesthetics are mandatory (in the anterior region), Biodentine could be a better alternative for VPT. Failure can occur even after six months without symptoms, so long-term monitoring is essential.
Conclusion
The network meta-analysis indicated a high to very low confidence rating that Mineral Trioxide Aggregate and Biodentine are superior materials for vital pulp treatment during 6, 12, and 24 months compared to calcium-hydroxide-based materials. Based on the 2–3 times higher failure rate, the clinical application of Ca(OH)2 and Ca(OH)2LC for VPT can no longer be recommended for direct pulp-capping for pulpotomy. With a moderate to low confidence rating, Biodentine and Totalfill could be a suitable MTA substitute.
Data availability
The data that support the findings of this study are available upon reasonable request from the corresponding author. Relevant reporting guidelines paperwork (see 5.2 Reporting Guidelines below) This protocol for the systematic review was registered in the PROSPERO database (registration number CRD42022375573) and adheres to the Preferred Reporting Items for Systematic Reviews (PRISMA-NMA) guidelines.
References
Bjorndal, L., Simon, S., Tomson, P. L. & Duncan, H. F. Management of deep caries and the exposed pulp. Int. Endod. J. 52, 949–973. https://doi.org/10.1111/iej.13128 (2019).
Asgary, S., Eghbal, M. J., Fazlyab, M., Baghban, A. A. & Ghoddusi, J. Five-year results of vital pulp therapy in permanent molars with irreversible pulpitis: A non-inferiority multicenter randomized clinical trial. Clin. Oral Investig. 19, 335–341. https://doi.org/10.1007/s00784-014-1244-z (2015).
Cushley, S. et al. Pulpotomy for mature carious teeth with symptoms of irreversible pulpitis: A systematic review. J. Dent. 88, 103158. https://doi.org/10.1016/j.jdent.2019.06.005 (2019).
Asgary, S. et al. Outcomes of root canal therapy or full pulpotomy using two endodontic biomaterials in mature permanent teeth: A randomized controlled trial. Clin. Oral Investig. 26, 3287–3297. https://doi.org/10.1007/s00784-021-04310-y (2022).
Leong, D. J. X. & Yap, A. U. Vital pulp therapy in carious pulp-exposed permanent teeth: An umbrella review. Clin. Oral Investig. 25, 6743–6756. https://doi.org/10.1007/s00784-021-03960-2 (2021).
Hahn, C. L. & Liewehr, F. R. Innate immune responses of the dental pulp to caries. J. Endod. 33, 643–651. https://doi.org/10.1016/j.joen.2007.01.001 (2007).
Awawdeh, L., Hemaidat, K. & Al-Omari, W. Higher maximal occlusal bite force in endodontically treated teeth versus vital contralateral counterparts. J. Endod. 43, 871–875. https://doi.org/10.1016/j.joen.2016.12.028 (2017).
Randow, K. & Glantz, P. O. On cantilever loading of vital and non-vital teeth .An experimental clinical study. Acta Odontol. Scand. 44, 271–277. https://doi.org/10.3109/00016358609004733 (1986).
Ou, K. L. et al. Effect of damping properties on fracture resistance of root filled premolar teeth: A dynamic finite element analysis. Int. Endod. J. 42, 694–704. https://doi.org/10.1111/j.1365-2591.2009.01570.x (2009).
Loewenstein, W. R. & Rathkamp, R. A study on the pressoreceptive sensibility of the tooth. J. Dent. Res. 34, 287–294. https://doi.org/10.1177/00220345550340021701 (1955).
Patel, S., Bhuva, B. & Bose, R. Present status and future directions: vertical root fractures in root filled teeth. Int. Endod. J. 55(Suppl 3), 804–826. https://doi.org/10.1111/iej.13737 (2022).
Parirokh, M., Torabinejad, M. & Dummer, P. M. H. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview—part I: Vital pulp therapy. Int. Endod. J. 51, 177–205. https://doi.org/10.1111/iej.12841 (2018).
Duncan, H. & Yamauchi, Y. Pulp exposure management. Clin. Dent. Rev. https://doi.org/10.1007/s41894-019-0043-y (2019).
Pelliccioni, G. A. et al. Evaluation of osteoblast-like cell response to Proroot MTA (mineral trioxide aggregate) cement. J. Mater. Sci. Mater. Med. 15, 167–173. https://doi.org/10.1023/b:jmsm.0000011819.26935.47 (2004).
Ribeiro, D. A., Matsumoto, M. A., Duarte, M. A., Marques, M. E. & Salvadori, D. M. In vitro biocompatibility tests of two commercial types of mineral trioxide aggregate. Braz. Oral Res. 19, 183–187. https://doi.org/10.1590/s1806-83242005000300005 (2005).
da Silva, G. N., Braz, M. G., de Camargo, E. A., Salvadori, D. M. & Ribeiro, D. A. Genotoxicity in primary human peripheral lymphocytes after exposure to regular and white mineral trioxide aggregate. Oral Surg. Oral Med Oral Pathol. Oral Radiol. Endod. 102, e50-54. https://doi.org/10.1016/j.tripleo.2006.02.032 (2006).
Ribeiro, D. A., Matsumoto, M. A., Duarte, M. A., Marques, M. E. & Salvadori, D. M. Ex vivo biocompatibility tests of regular and white forms of mineral trioxide aggregate. Int. Endod. J. 39, 26–30. https://doi.org/10.1111/j.1365-2591.2005.01043.x (2006).
Polyák, M., Komora, P., Szabó, E. V., Lohinai, Z. M. & Vág, J. Application of Hyperpure Chlorine Dioxide for Regenerative Endodontic Treatment of a Root-Canal-Treated Immature Tooth with External Cervical Resorption and Periapical Lesion: A Case Report. Applied Sciences 13, 10400 (2023).
Cavenago, B. C. et al. Influence of powder-to-water ratio on radiopacity, setting time, pH, calcium ion release and a micro-CT volumetric solubility of white mineral trioxide aggregate. Int. Endod. J. 47, 120–126. https://doi.org/10.1111/iej.12120 (2014).
Parirokh, M. & Torabinejad, M. Mineral trioxide aggregate: a comprehensive literature review–Part I: Chemical, physical, and antibacterial properties. J. Endod. 36, 16–27. https://doi.org/10.1016/j.joen.2009.09.006 (2010).
Lin, L. M., Ricucci, D., Saoud, T. M., Sigurdsson, A. & Kahler, B. Vital pulp therapy of mature permanent teeth with irreversible pulpitis from the perspective of pulp biology. Aust Endod J 46, 154–166. https://doi.org/10.1111/aej.12392 (2020).
Ricucci, D., Loghin, S. & Siqueira, J. F. Jr. Correlation between clinical and histologic pulp diagnoses. J. Endod. 40, 1932–1939. https://doi.org/10.1016/j.joen.2014.08.010 (2014).
Ricucci, D., Siqueira, J. F. Jr., Li, Y. & Tay, F. R. Vital pulp therapy: histopathology and histobacteriology-based guidelines to treat teeth with deep caries and pulp exposure. J. Dent. 86, 41–52. https://doi.org/10.1016/j.jdent.2019.05.022 (2019).
Parirokh, M. & Torabinejad, M. Mineral trioxide aggregate: a comprehensive literature review–part III: Clinical applications, drawbacks, and mechanism of action. J. Endod. 36, 400–413. https://doi.org/10.1016/j.joen.2009.09.009 (2010).
Islam, I., Chng, H. K. & Yap, A. U. Comparison of the physical and mechanical properties of MTA and portland cement. J. Endod. 32, 193–197. https://doi.org/10.1016/j.joen.2005.10.043 (2006).
Ravindran, V. & Jeevanandan, G. Comparative evaluation of the physical and antimicrobial properties of mineral trioxide aggregate, biodentine, and a modified fast-setting mineral trioxide aggregate without tricalcium aluminate: An in vitro study. Cureus 15, e42856. https://doi.org/10.7759/cureus.42856 (2023).
Kahler, B. & Rossi-Fedele, G. A review of tooth discoloration after regenerative endodontic therapy. J. Endod. 42, 563–569. https://doi.org/10.1016/j.joen.2015.12.022 (2016).
Nagas, E., Ertan, A., Eymirli, A., Uyanik, O. & Cehreli, Z. C. Tooth discoloration induced by different calcium silicate-based cements: A two-year spectrophotometric and photographic evaluation in vitro. J. Clin. Pediatr. Dent. 45, 112–116. https://doi.org/10.17796/1053-4625-45.2.7 (2021).
Türkoğlu Kayaci, Ş, Solmazgül Yazici, Z. & Arslan, H. Spectrophotometric analysis of coronal tooth discoloration induced by various calcium silicate cements in full pulpotomy of permanent molars: Theracal pt biodentine and proroot MTA. J. Endod. https://doi.org/10.1016/j.joen.2023.11.008 (2023).
Rajasekharan, S., Martens, L. C., Cauwels, R. & Anthonappa, R. P. Biodentine material characteristics and clinical applications: A 3 year literature review and update. Eur. Arch. Paediatr. Dent. 19, 1–22. https://doi.org/10.1007/s40368-018-0328-x (2018).
Arandi, N. Z. & Rabi, T. TheraCal LC: From biochemical and bioactive properties to clinical applications. Int. J. Dent. https://doi.org/10.1155/2018/3484653 (2018).
Zeater, B., Abboud, S. & Hanafi, L. Comparison of the effects of theracal lc and mineral trioxide aggregate on direct pulp capping (DPC) based on histological findings. Cureus 14, e25326. https://doi.org/10.7759/cureus.25326 (2022).
Manaspon, C. et al. Human dental pulp stem cell responses to different dental pulp capping materials. BMC Oral Health 21, 209. https://doi.org/10.1186/s12903-021-01544-w (2021).
Taha, N. A. & Khazali, M. A. Partial pulpotomy in mature permanent teeth with clinical signs indicative of irreversible pulpitis: A randomized clinical trial. J. Endod. 43, 1417–1421. https://doi.org/10.1016/j.joen.2017.03.033 (2017).
Asgary, S. & Ahmadyar, M. Vital pulp therapy using calcium-enriched mixture: An evidence-based review. J. Conserv. Dent. 16, 92–98. https://doi.org/10.4103/0972-0707.108173 (2013).
Asgary, S., Shahabi, S., Jafarzadeh, T., Amini, S. & Kheirieh, S. The properties of a new endodontic material. J. Endod. 34, 990–993. https://doi.org/10.1016/j.joen.2008.05.006 (2008).
Hasan Zarrabi, M., Javidi, M., Naderinasab, M. & Gharechahi, M. Comparative evaluation of antimicrobial activity of three cements: New endodontic cement (NEC), mineral trioxide aggregate (MTA) and Portland. J. Oral Sci. 51, 437–442. https://doi.org/10.2334/josnusd.51.437 (2009).
Schwendicke, F., Brouwer, F., Schwendicke, A. & Paris, S. Different materials for direct pulp capping: Systematic review and meta-analysis and trial sequential analysis. Clin. Oral Investig. 20, 1121–1132. https://doi.org/10.1007/s00784-016-1802-7 (2016).
Cushley, S. et al. Efficacy of direct pulp capping for management of cariously exposed pulps in permanent teeth: A systematic review and meta-analysis. Int. Endod. J. 54, 556–571. https://doi.org/10.1111/iej.13449 (2021).
Kiranmayi, G., Hussainy, N., Lavanya, A. & Swapna, S. Clinical performance of mineral trioxide aggregate versus calcium hydroxide as indirect pulp-capping agents in permanent teeth: A systematic review and meta-analysis. J. Int. Oral Health 11, 235–243. https://doi.org/10.4103/jioh.jioh_122_19 (2019).
Alqaderi, H., Lee, C. T., Borzangy, S. & Pagonis, T. C. Coronal pulpotomy for cariously exposed permanent posterior teeth with closed apices: A systematic review and meta-analysis. J. Dent. 44, 1–7. https://doi.org/10.1016/j.jdent.2015.12.005 (2016).
Fasoulas, A. et al. Comparative efficacy of materials used in patients undergoing pulpotomy or direct pulp capping in carious teeth: A systematic review and meta-analysis. Clin. Exp. Dent. Res. 9, 1129–1148. https://doi.org/10.1002/cre2.767 (2023).
Sabeti, M., Huang, Y., Chung, Y. J. & Azarpazhooh, A. prognosis of vital pulp therapy on permanent dentition: A systematic review and meta-analysis of randomized controlled trials. J. Endod. 47, 1683–1695. https://doi.org/10.1016/j.joen.2021.08.008 (2021).
Watt, J. & Del Giovane, C. Network meta-analysis. Methods Mol. Biol. 2345, 187–201. https://doi.org/10.1007/978-1-0716-1566-9_12 (2022).
Page, M. J. et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 134, 178–189. https://doi.org/10.1016/j.jclinepi.2021.03.001 (2021).
Hutton, B. et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 162, 777–784. https://doi.org/10.7326/M14-2385 (2015).
Wolters, W. J. et al. Minimally invasive endodontics: A new diagnostic system for assessing pulpitis and subsequent treatment needs. Int. Endod. J. 50, 825–829. https://doi.org/10.1111/iej.12793 (2017).
Ranganathan, P., Aggarwal, R. & Pramesh, C. S. Common pitfalls in statistical analysis: Odds versus risk. Perspect. Clin. Res. 6, 222–224. https://doi.org/10.4103/2229-3485.167092 (2015).
Selvendran, K. E., Ahamed, A. S., Krishnamurthy, M., Kumar, V. N. & Raju, V. G. Comparison of three different materials used for indirect pulp capping in permanent molars: An in vivo study. J. Conserv. Dent. 25, 68–71. https://doi.org/10.4103/jcd.jcd_551_21 (2022).
Leye Benoist, F., Gaye Ndiaye, F., Kane, A. W., Benoist, H. M. & Farge, P. Evaluation of mineral trioxide aggregate (MTA) versus calcium hydroxide cement (Dycal((R)) ) in the formation of a dentine bridge: a randomised controlled trial. Int. Dent. J. 62, 33–39. https://doi.org/10.1111/j.1875-595X.2011.00084.x (2012).
Awawdeh, L., Al-Qudah, A., Hamouri, H. & Chakra, R. J. Outcomes of vital pulp therapy using mineral trioxide aggregate or biodentine: A prospective randomized clinical trial. J. Endod. 44, 1603–1609. https://doi.org/10.1016/j.joen.2018.08.004 (2018).
Ahlawat, M. et al. Direct pulp capping with mineral trioxide aggregate and biodentine in cariously exposed molar teeth: 1-year follow-up—An in vivo study. J. Pharm. Bioallied Sci. 14, S983–S985. https://doi.org/10.4103/jpbs.jpbs_837_21 (2022).
Doranala, S. et al. Comparative assessment of titanium-prepared platelet-rich fibrin, EndoSequence root repair material, and calcium hydroxide as pulpotomy agents in permanent teeth with irreversible pulpitis: A randomized controlled trial. J. Conserv. Dent. 24, 606–610. https://doi.org/10.4103/jcd.jcd_264_21 (2021).
Schwarzer, G., Carpenter, J. R. & Rücker, G. Meta-analysis with R (Springer, 2015).
Rucker, G. Network meta-analysis, electrical networks and graph theory. Res. Synth. Methods 3, 312–324. https://doi.org/10.1002/jrsm.1058 (2012).
Nikolakopoulou, A. et al. CINeMA: An approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 17, e1003082. https://doi.org/10.1371/journal.pmed.1003082 (2020).
Papakonstantinou, T., Nikolakopoulou, A., Higgins, J. P. T., Egger, M. & Salanti, G. CINeMA: Software for semiautomated assessment of the confidence in the results of network meta-analysis. Campbell Syst. Rev. 16, e1080. https://doi.org/10.1002/cl2.1080 (2020).
Taha, N. A., Al-Rawash, M. H. & Imran, Z. A. Outcome of full pulpotomy in mature permanent molars using 3 calcium silicate-based materials: A parallel, double blind, randomized controlled trial. Int. Endod. J. 55, 416–429. https://doi.org/10.1111/iej.13707 (2022).
Mente, J. et al. Mineral trioxide aggregate or calcium hydroxide direct pulp capping: An analysis of the clinical treatment outcome. J. Endod. 36, 806–813. https://doi.org/10.1016/j.joen.2010.02.024 (2010).
Asgary, S. & Eghbal, M. J. Treatment outcomes of pulpotomy in permanent molars with irreversible pulpitis using biomaterials: A multi-center randomized controlled trial. Acta Odontol. Scand. 71, 130–136. https://doi.org/10.3109/00016357.2011.654251 (2013).
Hilton, T. J., Ferracane, J. L., Mancl, L., Northwest Practice-based Research Collaborative in Evidence-based. Comparison of CaOH with MTA for direct pulp capping: A PBRN randomized clinical trial. J. Dent. Res. 92, 16S-22S. https://doi.org/10.1177/0022034513484336 (2013).
Koc Vural, U., Kiremitci, A. & Gokalp, S. Randomized clinical trial to evaluate mta indirect pulp capping in deep caries lesions after 24 months. Oper. Dent. 42, 470–477. https://doi.org/10.2341/16-110-C (2017).
Suhag, K., Duhan, J., Tewari, S. & Sangwan, P. Success of direct pulp capping using mineral trioxide aggregate and calcium hydroxide in mature permanent molars with pulps exposed during carious tissue removal: 1 year follow-up. J. Endod. 45, 840–847. https://doi.org/10.1016/j.joen.2019.02.025 (2019).
Peskersoy, C., Lukarcanin, J. & Turkun, M. Efficacy of different calcium silicate materials as pulp-capping agents: Randomized clinical trial. J Dent Sci 16, 723–731. https://doi.org/10.1016/j.jds.2020.08.016 (2021).
Iyer, J. V. et al. Comparative evaluation of different direct pulp capping agents in carious tooth: An in vivo study. J Conserv Dent 24, 283–287. https://doi.org/10.4103/jcd.jcd_71_21 (2021).
Kaul, S. et al. Comparative analysis of biodentine, calcium hydroxide, and 2% chlorhexidine with resin-modified glass ionomer cement as indirect pulp capping materials in young permanent molars. J. Contemp. Dent. Pract. 22, 511–516. https://doi.org/10.5005/jp-journals-10024-3084 (2021).
Parameswaran, M., Vanaja Madanan, K., Kumar Maroli, R. & Raghunathan, D. Efficacy of calcium enriched mixture cement, mineral trioxide aggregate and calcium hydroxide used as direct pulp capping agents in deep carious lesions—A Randomised Clinical Trial. Eur. Endod. J. 8, 253–261. https://doi.org/10.14744/eej.2023.83007 (2023).
Singh, D. V. V., Taneja, S. & Fatima, S. Comparative evaluation of treatment outcome of partial pulpotomy using different agents in permanent teeth-a randomized controlled trial. Clin. Oral Investig. 27, 5171–5180. https://doi.org/10.1007/s00784-023-05136-6 (2023).
Singla, R. et al. Comparative assessment of the outcome of complete pulpotomy using mineral trioxide aggregate and Biodentine in mature permanent mandibular molars with symptomatic irreversible pulpitis: A randomized clinical trial with 18 months of follow-up. J Conserv Dent Endod 26, 402–408. https://doi.org/10.4103/jcd.jcd_170_23 (2023).
Tzanetakis, G. N., Koletsi, D. & Georgopoulou, M. Treatment outcome of partial pulpotomy using two different calcium silicate materials in mature permanent teeth with symptoms of irreversible pulpitis: A randomized clinical trial. Int. Endod. J. 56, 1178–1196. https://doi.org/10.1111/iej.13955 (2023).
Rao, M. et al. Comparative assessment of clinical outcomes in vital pulp therapy with bioactivemta:An invivo study. J. Pharm. Negat. Results 13, 2256–2261. https://doi.org/10.47750/pnr.2022.13.S07.310 (2022).
Egger, M., Davey Smith, G., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 315, 629–634. https://doi.org/10.1136/bmj.315.7109.629 (1997).
Lin, L. & Chu, H. Quantifying publication bias in meta-analysis. Biometrics 74, 785–794. https://doi.org/10.1111/biom.12817 (2018).
Hegyi, P. et al. Academia europaea position paper on translational medicine: The cycle model for translating scientific results into community benefits. J. Clin. Med. https://doi.org/10.3390/jcm9051532 (2020).
Hegyi, P., Eross, B., Izbeki, F., Parniczky, A. & Szentesi, A. Accelerating the translational medicine cycle: the Academia Europaea pilot. Nat. Med. 27, 1317–1319. https://doi.org/10.1038/s41591-021-01458-8 (2021).
Ricucci, D., Rocas, I. N., Alves, F. R. F., Cabello, P. H. & Siqueira, J. F. Jr. Outcome of direct pulp capping using calcium hydroxide: A Long-term retrospective study. J. Endod. 49, 45–54. https://doi.org/10.1016/j.joen.2022.11.005 (2023).
Faraco, I. M. Jr. & Holland, R. Response of the pulp of dogs to capping with mineral trioxide aggregate or a calcium hydroxide cement. Dent. Traumatol. 17, 163–166. https://doi.org/10.1034/j.1600-9657.2001.170405.x (2001).
Taira, Y., Shinkai, K., Suzuki, M., Kato, C. & Katoh, Y. Direct pulp capping effect with experimentally developed adhesive resin systems containing reparative dentin-promoting agents on rat pulp: mixed amounts of additives and their effect on wound healing. Odontology 99, 135–147. https://doi.org/10.1007/s10266-011-0006-5 (2011).
Kumar, N. et al. Biomimetic approaches in clinical endodontics. Biomimetics (Basel) https://doi.org/10.3390/biomimetics7040229 (2022).
Yoon, J. H. et al. Hard tissue formation after direct pulp capping with osteostatin and MTA in vivo. Restor Dent Endod https://doi.org/10.5395/rde.2021.46.e17 (2021).
Camilleri, J., Sorrentino, F. & Damidot, D. Investigation of the hydration and bioactivity of radiopacified tricalcium silicate cement biodentine and MTA angelus. Dent. Mater. 29, 580–593. https://doi.org/10.1016/j.dental.2013.03.007 (2013).
Gandolfi, M. G., Siboni, F. & Prati, C. Chemical-physical properties of TheraCal, a novel light-curable MTA-like material for pulp capping. Int. Endod. J. 45, 571–579. https://doi.org/10.1111/j.1365-2591.2012.02013.x (2012).
Camilleri, J. Hydration characteristics of Biodentine and Theracal used as pulp capping materials. Dent. Mater. 30, 709–715. https://doi.org/10.1016/j.dental.2014.03.012 (2014).
Camilleri, J., Laurent, P. & About, I. Hydration of Biodentine, Theracal LC, and a prototype tricalcium silicate-based dentin replacement material after pulp capping in entire tooth cultures. J. Endod. 40, 1846–1854. https://doi.org/10.1016/j.joen.2014.06.018 (2014).
Papadopoulou, C., Georgopoulou, M., Karoussis, I., Kyriakidou, K. & Papadopoulos, T. In vitro evaluation of biocompatibility and cytotoxicity of total fill bioceramic root repair material putty for endodontic use. Br. J. Med. Health Res. https://doi.org/10.46624/bjmhr.2020.v7.i2.003 (2020).
Debelian, G. & Trope, M. The use of premixed bioceramic materials in endodontics. Giornale Italiano di Endodonzia https://doi.org/10.1016/j.gien.2016.09.001 (2016).
Poggio, C. et al. Cytocompatibility and antibacterial properties of capping materials. Sci. World J. 2014, 181945. https://doi.org/10.1155/2014/181945 (2014).
Koutroulis, A., Kuehne, S. A., Cooper, P. R. & Camilleri, J. The role of calcium ion release on biocompatibility and antimicrobial properties of hydraulic cements. Sci. Rep. 9, 19019. https://doi.org/10.1038/s41598-019-55288-3 (2019).
Luo, Z. et al. Effect of Biodentine on the proliferation, migration and adhesion of human dental pulp stem cells. J. Dent. 42, 490–497. https://doi.org/10.1016/j.jdent.2013.12.011 (2014).
Rodrigues, E. M. et al. An assessment of the overexpression of BMP-2 in transfected human osteoblast cells stimulated by mineral trioxide aggregate and Biodentine. Int. Endod. J. 50(Suppl 2), e9–e18. https://doi.org/10.1111/iej.12745 (2017).
Silva, E. et al. Success rate of permanent teeth pulpotomy using bioactive materials: A systematic review and meta-analysis of randomized clinical trials. Int. Endod. J. https://doi.org/10.1111/iej.13939 (2023).
Acknowledgements
The author would like to thank Gergely Agócs for his contribution to the synthesis methods.
Funding
Open access funding provided by Semmelweis University.
Author information
Authors and Affiliations
Contributions
P.K.: Conceptualization, Investigation, Data Curation, Writing Original Draft, Visualization O.V.: Investigation, Data Curation, Writing Review Editing N.G.: Formal analysis, Writing Original Draft, Visualization P.H.: Methodology, Writing Review Editing, Supervision K.K.: Methodology, Writing Review Editing, Project administration A.G.: Investigation, Writing Review Editing G.V.: Methodology, Writing Review Editing, Supervision B.K.: Conceptualization, Methodology, Writing Original Draft, Supervision J.V.: Conceptualization, Methodology, Writing Original Draft, Supervision.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Komora, P., Vámos, O., Gede, N. et al. Comparison of bioactive material failure rates in vital pulp treatment of permanent matured teeth – a systematic review and network meta-analysis. Sci Rep 14, 18421 (2024). https://doi.org/10.1038/s41598-024-69367-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-69367-7
- Springer Nature Limited