
Abstract
Hand, foot, and mouth disease (HFMD) is a prevalent acute infectious disease caused by enteroviruses, presenting substantial public health challenges in Shanghai, especially among children. The dynamic nature of HFMD’s etiology necessitates an ongoing evaluation of its epidemiological and virological trends to inform effective control strategies. This study aims to investigate the epidemiological patterns and viral evolution of HFMD in Fengxian District, Shanghai, China, with a focus on shifts in predominant viral strains over a 14-year period. We conducted a retrospective analysis of HFMD cases reported to the National Notifiable Disease Reporting System in Fengxian District from January 1, 2009 to December 31, 2022. Epidemiological trends, strain prevalence, and demographic impacts were assessed. A total of 27,272 HFMD cases were documented during the study period, with incidence showing pronounced seasonal fluctuations—peaking in spring and summer and a lesser peak in autumn. The disease incidence demonstrated significant positive correlations with several meteorological variables: daily average temperature (r = 0.30, P < 0.05), relative humidity (r = 0.20, P < 0.05), wind speed (r = 0.17, P < 0.05), and precipitation (r = 0.17, P < 0.05). Geographically, Nanqiao Town, Fengcheng Town, and Xidu Subdistrict reported the highest incidence rates. The demographic analysis revealed a male-to-female ratio of 1.60:1, predominantly affecting children aged 1–3 years. Prior to 2017, Enterovirus 71 (EV71) and Coxsackievirus A16 (CoxA16) were the primary detected strains; post-2017, Coxsackievirus A6 (CoxA6) emerged as the dominant strain. Statistical analysis confirmed significant year-to-year variations in virus detection rates, with decreasing trends for EV71 and other enteroviruses and an increasing trend for CoxA6. The findings indicate a distinct seasonal incidence of HFMD in Fengxian District. This study underscores the need for targeted public health education, enhanced surveillance, and proactive measures in childcare facilities to mitigate disease spread during peak seasons. Moreover, the evolving viral landscape warrants accelerated efforts in vaccine development against new strains to reduce HFMD incidence.
Similar content being viewed by others


Introduction
Hand, foot, and mouth disease (HFMD) is a highly contagious viral infection predominantly affecting children under the age of 51. Caused by enteroviruses, HFMD is characterized by its rapid transmissibility among young children and its potential to trigger widespread outbreaks. Despite its global prevalence, HFMD remains without specific therapeutic interventions, thus imposing significant social and economic burdens at both national and regional levels2. Historically, HFMD first gained attention in Asia, with Singapore reporting cases in 1970, followed by notable outbreaks in Shanghai in 1972 and 1981, and a substantial epidemic in Shandong in 2000. Meanwhile, Japan, one of the nations with the highest recorded instances of large-scale outbreaks, noted its inaugural case in 1960, followed by recurrent outbreaks in 1969–1970, 1973, and 19783, along with a significant outbreak in 19824. Malaysia grappled with multiple outbreaks and epidemics in 19975,6, and Vietnam witnessed outbreaks in 20057. Early detection and alert systems for HFMD outbreaks are pivotal, as they facilitate the allocation and distribution of healthcare resources, expedite the implementation of effective measures, and proactively mitigate the extent of outbreaks, thereby curtailing its incidence and associated mortality and ultimately ameliorating its impact on pediatric health8.
During epidemic periods, asymptomatic carriers are the principal sources of HFMD transmission9, whereas during outbreaks, symptomatic HFMD patients become the primary transmitters10,11. Thus, both symptomatic and asymptomatic individuals play pivotal roles in the propagation and spread of the disease12,13. The transmission pathways of HFMD are complex, significantly contributing to the difficulty of controlling outbreaks. In Fengxian District, the incidence rates of HFMD from 2016 to 2018 were 290.77, 100.55, and 293.86 per 100,000 population, respectively. Initially, EV71 was the predominant pathogen. However, in recent years, there has been a notable increase in the incidence of CoxA6 and CoxA16, which have now surpassed EV71 as the leading pathogens. This shift indicates a significant change in the pathogen composition within this region.
Internationally, HFMD has been extensively documented across continents, with Europe and the Americas also experiencing outbreaks 14,15. Bulgaria and Hungary witnessed outbreaks of Enterovirus 71 (EV71)-associated HFMD in 1975 and 197816,17, respectively. The Netherlands reported two outbreaks primarily attributed to EV71 in 1986 and 2007. During the 1994 outbreak in the United Kingdom, Coxsackievirus A16 (CoxA16) emerged as the primary pathogen18. These global occurrences demonstrate the ubiquity and persistence of HFMD as a public health challenge.
Over the past two decades, China has witnessed a significant escalation in the severity of HFMD outbreaks. In 2000, an epidemic in Zhaoyuan City, Shandong Province, resulted in three fatalities19. The following year, Beijing experienced an outbreak with a recorded incidence rate of 6.65%20. In 2003, Xintai City, Shandong Province, reported 1,359 cases and nine fatalities21. In response to the increasing threat, on May 2, 2008, the National Health and Family Planning Commission of the People's Republic of China classified HFMD as a Class B notifiable infectious disease under the Law of the People's Republic of China on Prevention and Control of Infectious Diseases22. The following years saw dramatic increases in cases and fatalities: in 2009, there were 1,155,525 reported cases with 353 deaths; by 2010, the figures climbed to 1,795,336 cases with 888 deaths23. The period from 2013 to 2015 was particularly severe, with 6,724,998 HFMD reported nationwide, resulting in 325 fatalities and a mortality rate of 4.83 per 100,00024. These outbreaks not only affected public health but also imposed a substantial economic burden. From 2013 to 2015, the economic burden of HFMD-related deaths in China amounted to 148.59 million CNY, 318.97 million CNY, and 85.10 million CNY, respectively. Wang et al. estimated that the annual economic burden of HFMD for a population of 142 million was 7.66 million USD25.
Despite extensive research on HFMD, detailed analyses focusing on the evolution of viral strains and their epidemiological impact in specific regions remain scarce. This study aims to fill this gap by providing a comprehensive examination of the epidemiological and etiological characteristics of HFMD in this area over a 14-year period.
Materials and methods
Data sources
Located in the southern part of Shanghai, China, Fengxian District is distinguished by its subtropical monsoon climate and a population of 1.12 million. The district hosts 12 hospitals and employs 8,910 medical professionals, rendering it an ideal area for the investigation of HFMD due to its diverse climatic and demographic attributes. The data for this study encompassed records of HFMD cases collected from twelve medical institutions within the district, extending from January 1, 2009 to December 31, 2022. These records were sourced from the National Notifiable Disease Reporting System, adhering to the HFMD diagnostic guidelines as delineated in the International Classification of Diseases, Tenth Revision (ICD-10), specifically under disease code B08-401. The collected data included basic demographic information such as gender and age of the patients. The standard map of Fengxian District was obtained from the Institute of Geographic Sciences and Natural Resources Research, the Chinese Academy of Sciences (https://www.resdc.cn/). Concurrent meteorological data for Fengxian District were collected from the China Meteorological Data Network (http://data.cma.cn/) , which included daily average temperature (°C), relative humidity (%), wind speed (m/s), and precipitation (mm). Additionally, the annual population statistics critical for calculating incidence rates were obtained from the Fengxian District Statistical Yearbook. All methods in this study were performed in accordance with relevant guidelines and regulations. Given the retrospective nature of this study, the Medical Ethics Committee of Shanghai Fengxian District Central Hospital has granted an exemption from the requirement for patient informed consent.
Etiology
In our study, the etiological analysis was systematically conducted by collecting diagnosed cases of HFMD within Fengxian District from January 1, 2009, to December 31, 2022. Specimens, including nasopharyngeal swabs, rectal swabs, and fecal samples, were collected following a standardized protocol, established by designated sentinel surveillance hospitals across Fengxian District. The specimens underwent polymerase chain reaction (PCR) testing at the Fengxian District Center for Disease Control and Prevention. Epidemiological patterns, including temporal trends and spatial distribution of HFMD cases, were examined in conjunction with demographic data of the affected population. This integrated analysis aimed to elucidate the interaction between pathogen evolution and population dynamics over the study period. Furthermore, we applied Spearman's rank correlation analysis to investigate the relationships between various meteorological variables and HFMD incidence.
Statistical analysis
Data organization and preliminary analysis were conducted using Microsoft Excel 2019. Spatial distributions and cluster analyses of HFMD incidence were performed using ArcGIS 10.8, enabling detailed mapping and identification of epidemiological patterns across Fengxian District. Statistical analysis was conducted using SPSS 25.0 software. Correlation analyses between HFMD incidence and meteorological variables—namely temperature, relative humidity, wind speed, and precipitation—were conducted using R statistical software. The chi-squared (χ2) test was applied to evaluate the significance of variations among categorical variables, with a significance threshold set at α = 0.05.
Results
Epidemiological overview
Between 2009 and 2022, Fengxian District reported a total of 27,272 cases of HFMD. The average annual incidence rate over this period was 184.08 per 100,000 population. The year 2014 marked the apex of incidence at 320.47 per 100,000, whereas 2022 recorded the nadir at 17.92 per 100,000. Notably, the incidence rates exhibited distinct cyclical variations, with significant fluctuations characterized by alternating peak and trough years. Statistical analysis confirmed a significant periodic pattern in the incidence rates, with decreases noted during odd-numbered years and increases during even-numbered years (χ2trend = 3301.03, P < 0.001) (Fig. 1).

HFMD incidence rates in Fengxian District between 2009 and 2022.
To further elucidate these fluctuations, we calculated the annual growth rates and growth speeds. The year 2014 witnessed the most substantial year-over-year increase in HFMD incidence, surging by 170.33 per 100,000, which cumulatively represented a growth of 96.72 per 100,000 from the preceding year. This year also exhibited the highest growth speed, with a fixed base index of 2.13. In contrast, the year 2021 saw a resurgence, with an increase of 372.22 per 100,000 compared with the previous year, achieving a growth speed of 113.44%. The most significant declines occurred in 2022 and 2020, with reductions of 82.25% and 73.55%, respectively. Throughout the study period, the average month-over-month growth rate was 24.75% (Table 1).
Temporal distribution of HFMD cases
The analysis of HFMD cases in Fengxian District on a monthly basis revealed a pronounced seasonally cyclic pattern of incidence. Starting in March, the number of cases began to increase, reaching its zenith in June before gradually declining throughout July. In the second half of the year, there was a resurgence in cases, with smaller peaks from September to December (Fig. 2).

Monthly incidence rates of HFMD in Fengxian District between 2009 and 2022.
Spatial distribution of HFMD cases
This study presented a comparative analysis of the spatial distribution of HFMD incidences across different urban areas within Fengxian District from 2009 to 2022. Given the lack of comprehensive demographic data for each urban area, our investigation primarily focused on the comparative analysis of reported HFMD case counts. Throughout the district, including all 12 towns, neighborhoods, and tourist regions, HFMD cases were documented. Notably, the highest incidences were recorded in Nanqiao Town, Fengcheng Town, and Xidu Subdistrict, with reported cases numbering 6,611, 5,353, and 3,148, respectively (Fig. 3).

Spatial distribution of HFMD cases in Fengxian District between 2009 and 2022. Note: Drawing approval number: Shanghai S (2022) No. 42.
Demographic characteristics of HFMD cases
Between 2009 and 2022, Fengxian District reported a total of 27,272 cases of HFMD. An analysis of gender distribution revealed a significant discrepancy: males accounted for 61.47% (n = 16,764)s, whereas females represented 38.53% (n = 10,508), culminating in a male-to-female ratio of 1.60:1. The χ2 test unveiled significant differences in the average incidence rates between genders (χ2 = 1045.62, P < 0.001), with males exhibiting a higher incidence rate of 218.96 per 100,000, compared with 146.87 per 100,000 for females.
Age-wise, the distribution of HFMD cases predominantly targeted children aged five and below, who comprised 91.53% (n = 24,961) of the total cases. Within this group, children aged three and below were particularly susceptible, representing 71.87% (n = 19,600) of the total cases. Detailed incidence rate analyses revealed the highest susceptibility in the 1-year-old group, with an average incidence rate of 5,817.73 per 100,000, followed by the 2-year-old group at 4,096.64 per 100,000 and the 3-year-old group at 4,000.54 per 100,000. The incidence rates continued to decrease with increasing age:2688.09 per 100,000 in the 4-year-old group and 1,880.45 per 100,000 in the 0-year-old group.
The incidence of HFMD and its relationship with meteorological factors
From 2009 to 2022, the daily incidence of HFMD in Fengxian District oscillated between zero and a peak of 799 cases. Concurrent meteorological data documented daily average temperatures spanning from 1.14 °C to 30.87 °C. Relative humidity varied from 62.66% to 91.65%, with wind speeds ranging from 1.83 m/s to 4.06 m/s. Daily precipitation levels were observed between 0.18 mm and 15.6 mm (Table 2).
As displayed in Table 3 and Fig. 4, the results of the Spearman's rank correlation analysis revealed significant positive correlations between the daily incidence of HFMD in Fengxian District and meteorological variables, including daily average temperature (r = 0.30, P < 0.05), relative humidity (r = 0.20, P < 0.05), wind speed (r = 0.17, P < 0.05), and precipitation (r = 0.17, P < 0.05).

Correlation analysis between the daily incidence of HFMD and meteorological variables in Fengxian District from 2009 to 2022.
Pathogen monitoring
Overview
From 2009 to 2022, our study collected 1472 clinical samples from HFMD cases in Fengxian District, of which 1316 samples (89.40%) tested positive for viral strains. The most prevalent strain was CoxA16, detected in 34.65% of positive cases, followed by CoxA6 and EV71, each accounting for 19.83% of positive cases.
Temporal dynamics of pathogen composition
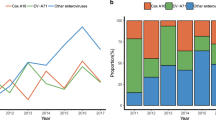
The dominance among HFMD pathogens shifted over the study period. Prior to 2016, EV71 and CoxA16 were the most common strains. However, post-2016, CoxA6 cases increased significantly, overtaking EV71 in prevalence (Fig. 5). This shift resulted in statistically significant differences in the total positive detection rates over the years (χ2 = 18.55, P < 0.001), with EV71 showing a declining trend (χ2 trend = 176.32, P < 0.001) while CoxA6 showing an increasing trend (χ2 trend = 339.03, P < 0.001). Conversely, other enteroviruses demonstrated a declining trend (χ2 trend = 78.00, P < 0.001).

Pathogen composition of HFMD in Fengxian District between 2009 and 2022.
Seasonal analysis revealed that during spring and summer, EV71 and CoxA16 remained prevalent, whereas autumn and winter saw a rise in CoxA6 dominance (Fig. 6).

Pathogen composition of HFMD in Fengxian District by month between 2009 and 2022.
Gender-stratified positivity rates of HFMD virus strains
Among the 1472 cases, 897 were males and 575 were females, with positivity rates of 90.08% and 88.35%, respectively. The distribution of virus strains among males and females was similar, with CoxA6 (31.44% in males vs. 30.26 in females), CoxA16 (25.08% in males vs. 24.17% in females), and EV71 (17.95% in males vs. 17.39% in females) being the most common, showing no statistically significant gender differences (χ2 = 0.299, P > 0.05).
Age-stratified positivity rates of HFMD virus strains
Positivity rates varied across six age groups from one to six years, with corresponding positivity rates of 83.60%, 89.29%, 88.19%, 97.64%, 87.36%, and 90.00%, respectively. Statistically significant differences in positivity rates were observed among different age groups for EV71 (χ2 = 13.60, P < 0.05), CoxA10 (χ2 = 24.73, P < 0.01), and other enteroviruses (χ2 = 13.77, P < 0.05). However, the overall positivity rate (χ2 = 7.27, P > 0.05), CoxA16 positivity rate (χ2 = 7.99, P > 0.05), and CoxA6 positivity rate (χ2 = 5.02, P > 0.05) did not show significant differences.
Discussion
From 2009 to 2022, Fengxian District reported a total of 27,272 HFMD cases, demonstrating an undulating incidence rate. This rate precipitously diminished in 2019–2020, experienced a resurgence in 2021, and descended to its nadir in 2022. This cyclic recurrence, with odd-numbered years exhibiting decreased incidence and even-numbered years showing an upward trend, mirrors analogous patterns in most regions of China26. The period from 2019 to 2022 saw a notable decline in HFMD cases, primarily due to the stringent COVID-19 containment measures that limited social interactions among susceptible populations. In 2021, as COVID-19 restrictions eased and population mobility increased, HFMD cases briefly surged. However, in 2022, the reimplementation of strict COVID-19 protocols in Shanghai, including home isolation policies for schools and childcare facilities, drastically reduced HFMD transmission, resulting in the lowest incidence rates on record. HFMD in Fengxian District incidence also displayed pronounced seasonal dynamics, with the highest rates typically occurring during the warmer months of spring and summer, followed by a secondary, milder peak in the autumn27,28. Previous studies, both in China and internationally, have demonstrated the significance of temperature and humidity as critical risk factors for HFMD29,30,31,32,33,34,35,36. This seasonal pattern in Fengxian District can be attributed to the subtropical maritime climate of the district, near Hangzhou Bay, which supports the survival and spread of HFMD pathogens37,38,39. Additionally, the peak periods coincided with increased outdoor activities among children, increasing their risk of exposure to infection sources. In contrast, the incidence dropped in July, during the school summer vacation, when most children have fewer social contacts. The rise in cases in September correlated with the start of the school year, when children return to more crowded indoor environments, facilitating the virus's spread. Furthermore, the lax implementation of home isolation measures for patients inadvertently bolstered community activities during isolation, thereby amplifying pathogen dissemination. As such, it is imperative to implement targeted preventive and control measures before the primary transmission seasons in March and the commencement of the school year in September.
From 2009 to 2022, reports of HFMD were consistent across all towns, neighborhoods, and tourist areas within Fengxian District. The highest incidences were notably in Nanqiao Town, Fengcheng Town, and Xidu Subdistrict. Nanqiao Town and Fengcheng Town, which are major urban centers located respectively in the eastern and western parts of the district, boast high population densities and a large number of schools and kindergartens. These factors contributed to the heightened HFMD case numbers in these areas. Xidu Subdistrict, positioned at the urban-suburban boundary in Fengxian District, has undergone significant urban revitalization and has seen a substantial influx of migrants. The frequent population mobility in this area further escalates the risk of HFMD transmission.
In terms of gender distribution, HFMD cases were disproportionately higher among males, with a male-to-female ratio of 1.60:1. This disparity was statistically significant and can be attributed to the typically higher levels of physical activity and outdoor engagement among boys, which increases their exposure to HFMD pathogens. Additionally, research suggests that males may exhibit lower vigilance and diminished adherence to hygiene practices compared with females, potentially elevating their susceptibility to infection40,41.
HFMD primarily affected children under five years of age, who accounted for 91.53% of the total reported cases in Fengxian District from 2009 to 2022. Within this demographic, the 1–3-year cohort exhibited the highest susceptibility, with the highest average incidence rates observed in the one-year-old age group. This heightened vulnerability in infants can be attributed to their frequent physical contact with caregivers, often grandparents or other family members, a practice necessitated by parental employment commitments. This close interaction, coupled with potentially suboptimal adherence to infection control practices, highlights an urgent need for focused educational initiatives targeting caregivers42,43. As children age, a notable decline in HFMD incidence is observed, particularly in those over five years. This reduction can be attributed to physiological enhancements in immune function, including age-associated increases in specific antibody production and overall immune competency. Concurrently, the adoption of personal hygiene behaviors further fortifies this age group against HFMD44.
The analysis revealed that a significant proportion of HFMD cases occurred among scattered children—those not enrolled in formal childcare facilities—and preschoolers, accounting for 94.54% of all cases in this district. Scattered children typically receive care within familial or community contexts, which may not rigorously implement structured infection prevention protocols, underscoring the need for community-based management strategies. Moreover, managing HFMD risk in childcare facilities is essential, given the heightened risk of transmission in such densely populated settings. Effective control measures include the implementation of stringent hygiene regulations, regular health inspections, and caregiver training programs focused on infection prevention.
Between 2009 and 2022, we identified 1,472 clinical samples from HFMD cases in Fengxian District, identifying 1,316 positive strains (a positivity rate of 89.40%). The study revealed that CoxA6 and CoxA16 were the most prevalent strains, aligning with patterns witnessed across other regions in China45,46,47,48. Given the unpredictable nature of HFMD pathogens and their capricious virulence, vigilant surveillance and broadened pathogen monitoring are necessary to preemptively identify emerging trends and shifts in pathogen dominance that could lead to localized or widespread outbreaks49. From 2009 to 2016, EV71 and CoxA16 were the dominant strains, and the introduction of the inactivated EV71 vaccine in 2016 marked a significant milestone in controlling HFMD50,51. This initiative led to a marked reduction in EV71 cases, particularly after its intensification post-2017, coinciding with a noticeable rise in CoxA6 infections. This evolution in pathogen composition within Fengxian District mirrors broader trends observed in various other regions across China, underlining the importance of expanding pathogen monitoring efforts. Continuous tracking of emerging strains and adjustments in the pathogen spectrum are pivotal in forestalling the emergence of new dominant strains capable of causing localized or epidemic outbreaks.
Our findings provide important insights into the epidemiological dynamics of HFMD in Fengxian District, with implications for local public health interventions. The shift in dominant viral strains highlights the need for ongoing surveillance and adaptation of prevention strategies. By offering a comprehensive framework that can be applied to similar epidemiological studies in other regions, this study informs future public health policies and intervention strategies for HFMD management.
However, this study has some limitations. These include potential underreporting of cases due to variability in symptom severity and disparities in healthcare access across different regions. Our classification of pathogens was restricted to five types of enteroviruses: EV71, CoxA16, CoxA6, CoxA10, and others. Recognizing these limitations, we plan to incorporate genetic sequencing in future studies to enhance the specificity and breadth of our pathogen analysis.
Conclusion
In summary, children aged 0–5 years. Especially those not enrolled in formal childcare facilities (scattered children) and those in kindergartens, are the key groups of HFMD prevention and control. Strengthening health education for caregivers and educators is essential. Robust etiological surveillance is also critical. It enables the monitoring of HFMD trends and the timely implementation of targeted public health interventions. In addition, the considerable role of other enteroviruses in HFMD cases necessitates expanded research efforts. Further typing and research are needed to better understand these pathogens' characteristics and develop effective countermeasures.
Data availability
The data for this study comprised records of HFMD cases reported by twelve medical institutions at various levels within Fengxian District, Shanghai, China, spanning from January 1, 2009 to December 31, 2022. The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://116.236.221.23/por/service.csp?showsvc=1&autoOpen=1&rnd=eagjejoanfm. The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Wang, Y. et al. Epidemiological and clinical characteristics of severe hand-foot-and-mouth disease (HFMD) among children: a 6-year population-based study. BMC Public Health https://doi.org/10.1186/s12889-020-08961-6 (2020).
Ping, H., Huifen, F., Bin, W. & Jing, Z. Application of time series analysis and model construction in the prediction of hand-foot-mouth disease. J. Practical Med. 34(9), 1554–1556 (2018).
A SV, Y CC, P CK, W N, E LA. An outbreak of hand, foot, and mouth disease in Singapore. Annals of the Academy of Medicine, Singapore. 3(32):381–7. (2003).
Chan, K. P. et al. Epidemic Hand, Foot and Mouth Disease Caused by Human Enterovirus 71. Singapore. Emerg Infect Dis. https://doi.org/10.3201/eid1301.020112 (2003).
G CL, D PU, S LM, G OF, R ZS, P AJ, et al. Deaths of children during an outbreak of hand, foot, and mouth disease in sarawak, malaysia. Clin. Infect. Dis. 3(31):678–83. (2000).
Cardosa, M. J., Krishnan, S., Tio, P. H., Perera, D. & Wong, S. C. Isolation of subgenus B adenovirus during a fatal outbreak of enterovirus 71-associated hand, foot, and mouth disease in Sibu Sarawak. Lancet 22, 44. https://doi.org/10.1016/S0140-6736(98)11032-2 (1999).
Van Tu P, Thao NTT, Perera D, Truong KH, Tien NTK, Thuong TC, et al. Epidemiologic and Virologic Investigation of Hand, Foot, and Mouth Disease, Southern Vietnam, 2005. Emerg. Infect. Dis. [Journal Article; Research Support, Non-U.S. Gov't]. 2007–11–1;13(11):1733–41. (2007).
Yan, L. Study on geographical epidemiology of hand, foot and mouth disease and EV71 gene subtype in Changchun area (Jilin University, 2015).
Mirand, A. et al. Outbreak of hand, foot and mouth disease/herpangina associated with coxsackievirus A6 and A10 infections in 2010, France: A large citywide, prospective observational study. Clin. Microbiol. Infect. 5(18), E110–E118 (2012).
Huang, J. R. The application effect of health education on parents of children with hand-foot-mouth disease. Fertility Health 29(12), 88–90 (2023).
Guo, Y. L. Advances in epidemiology and etiology of hand-foot-mouth disease. Chin. J. Med. Dev. 33(10), 201–203 (2020).
Li, X. J. et al. Case-control Study on Risk Factors of Infection of HFMD Among Children in Chengdu. J. Prevent. Med. Inform. 31(8), 616–619 (2015).
Yang, A. R. Epidemiological characteristics of Hand, foot and mouth disease and intrafamilial infection in Yunnan (Kunming Medical University, 2017).
Kennett ML, Birch CJ, Lewis FA, Yung AP, Locarnini SA, Gust ID. Enterovirus type 71 infection in Melbourne. B World Health Organ. 1974–1–1;51(6):609–15. (1974).
Deibel, R., Gross, L. L. & Collins, D. N. Isolation of a new enterovirus (38506). Proc. Soc. Exp. Biol. Med. https://doi.org/10.3181/00379727-148-38506 (1975).
Melnick, J. L. Enterovirus Type 71 Infections: A Varied Clinical Pattern Sometimes Mimicking Paralytic Poliomyelitis. Rev. Infect. Dis. https://doi.org/10.1093/clinids/6.Supplement_2.S387 (1984).
Kapusinszky, B., Szomor, K. N., Farkas, A., Takacs, M. & Berencsi, G. Detection of non-polio enteroviruses in Hungary 2000–2008 and molecular epidemiology of enterovirus 71, coxsackievirus A16, and echovirus 30. Virus Genes https://doi.org/10.1007/s11262-009-0440-4 (2010).
Bendig JW, Fleming DM. Epidemiological, virological, and clinical features of an epidemic of hand, foot, and mouth disease in England and Wales. Communicable disease report. CDR review. 1996–1–1;6(6):R81. (1996).
Xu, Y. N., Yang, P., Gao, L. Y., Chen, H. J. & Li, W. L. Clinical epidemiological characteristics of hand-foot-mouth disease in children in Zhaoyuan City in the past 10 years. Med. Inform. 24(6), 3427–3428 (2011).
Gao, G. H., Li, W. J. & Xing, W. D. Investigation report of an outbreak of hand, foot and mouth disease in kindergarten. Dis. Surv. 11, 37–38 (2001).
Xu, A. F., Gao, J., Chen, G. & Wang, M. C. Advances in etiology and epidemiology of hand, foot and mouth disease. Chinese J. Health Lab. Technol. 221(1), 252 (2011).
Prevention CCFD. Guidelines for Prevention and Control of Hand, Foot and Mouth Disease (2009 edition); (2009).
Zhan, H. J. & Ke, C. W. Current prevalence and molecular epidemiology of hand-foot-mouth disease in the world. South China J. Prev. Med. 37(5), 34–38 (2011).
Epidemic situation of notifiable infectious diseases in China. Gazette of the National Health Commission of the People's Republic of China. (2017).
YM Zheng, J Yang. Estimation of socio-economic burden of death from HFMD in China from 2013 to 2015. Disease Surveillance. 2017 2017–6–30;32(06):516–20.
Wei J, Wu R, Xing D, Shu J, Hu S, Qin J. Epidemiological characteristics and spatial epidemiology of hand-foot-mouth disease in Hunan Province, China, from 2008 to 2019. Zhongguo dang dai er ke za zhi. 2021–1–1;23(11):1141–8. (2021).
PLOS OS, The POS. Correction: The surveillance of the epidemiological and serotype characteristics of hand, foot, mouth disease in Neijiang city, China, 2010–2017: A retrospective study. PLoS One. 2019–1–1;14(7):e0219726. (2019).
Chen, M. J. Prediction of epidemic trend of hand-foot-mouth pathogens based on time series analysis (Southeast University, 2020).
Cao, Z. D., Ceng, D. J., Wang, Q. Y., Zheng, X. L. & Wang, F. Y. Epidemic regularity and transmission mechanism of hand, foot and mouth disease in Beijing in 2008. Chin. Sci. Bull. 55(9), 764–772 (2010).
D Song, Y Pan. Epidemic characteristics of hand, foot and mouth disease in Hebei District, Tianjin from 2009 to 2017. Journal of Community Medicine. 2019–3–14;17(05):247–50. (2019).
LH Duan, H Xian, JZ Yang, LY Wei. Epidemiological characteristics of hand, foot and mouth disease in Mianzhu City from 2009 to 2018. Occupational Health and Damage. 2019–8–28;34(04):214–9. (2019).
C Yuan-xing, Y Wei-peng, Y Wan-dong, Z Ya-xiu, Z Xiao-ping, W Guang-hua. Epidemiological characteristics of hand, foot and mouth disease in Zhangye city from 2009 to 2018. Endemic Diseases Bulletin(china). 34(5):68–70, 76. (2019).
B He, YM Sun, CY Qiu. Epidemiological and etiological characteristics of hand-foot-mouth disease in preschool children in Haidian District, Beijing from 2009 to 2019. Chinese Journal of Frontier Health and Quarantine. 2022–4–25;45(02):151–4. (2022).
Urashima M, Shindo N, Okabe N. Seasonal models of herpangina and hand-foot-mouth disease to simulate annual fluctuations in urban warming in Tokyo. JPN J INFECT DIS. 2003–1–1;56(2):48–53. (2003).
Onozuka, D. & Hashizume, M. The influence of temperature and humidity on the incidence of hand, foot, and mouth disease in Japan. Sci. Total Environ. https://doi.org/10.1016/j.scitotenv.2011.09.055 (2011).
Xiao, G. X. et al. Analysis of generalized estimation equation of influencing factors of hand, foot and mouth disease in China. Chin. J. Public Health 28(9), 1225–1227 (2012).
Qi, G. et al. Forecast and early warning of hand, foot, and mouth disease based on meteorological factors: Evidence from a multicity study of 11 meteorological geographical divisions in China’s mainland. Environ. Res. 192, 110301 (2021).
Debian, Z. Meteorological Factors and HFMD Response Analysis. Meteorol. Environ. Sci. 34(z1), 135–137 (2011).
Yi-ling, X. U. & Dong, L. I. Relationship between Climatic Factors and HFMD in Zhangdian District of Zibo. J. Trop Med.US. 10(10), 1237–1239 (2010).
Zhou, X. Epidemiological characteristics and time series analysis of hand, foot and mouth disease in Wuzhou City from 2014 to 2018 (Guangxi Medical University, 2019).
Wang Z, Liu T, Li J, Gu Q. Risk factors of hand, foot, and mouth disease caused by Coxsackievirus A6 in children under 6 years of age in Tianjin, China: a case-control study. JPN J INFECT DIS. [Journal Article]. 2021 2021–9–22;74(5):437–42.
Yu QL, Liu YY, Zhao WN, Su T, Xie Y, Zhang WW, et al. Epidemiological and pathogenic characteristics of cases with severe and fatal hand, foot, and mouth disease caused by other enterovirus in Hebei province, 2013–2017. Zhōnghuá liúxíngbìng zázhì. 2020 2020–1–1;41(7):1054–7.
Cui JZ, Nie TR, Ren MR, Liu FF, Li Y, Wang LP, et al. Epidemiological characteristics of fatal cases of hand, foot, and mouth disease in children under 5 years old in China, 2008–2018. Zhōnghuá liúxíngbìng zázhì. 2020–1–1;41(7):1041–6. (2020).
Li, R. & Xiang, S. J. Summary of time series analysis and research in China. Stat. Educ. 7, 6–8 (2006).
Li-na, J. et al. Epidemiological characteristics and temporal-spatial clustering of hand, foot and mouth disease in Guangxi from 2008 to 2015. Chin. J. Dis. Control. Prev. 21(4), 340–344 (2017).
Shao-yi, H., Lin-guang, H., Li, H. & Yan-she, Q. Epidemiological and etiological characteristics among children under 5 years age suffered from HFMD from 2011 to 2017 in Hechi City. Progress Microbiol. Immunol. 46(6), 61–66 (2018).
Wanwan, Z., Weien, C., Zhongfu, L., Jun, Y. & Yihong, X. Epidemiological and etiological characteristics of hand foot and mouth disease in Liuzhou, Guangxi, 2014–2018. Dis. Surv. 37(5), 603–608 (2022).
Meng, Z. et al. Characteristics of high incidence of hand, foot and mouth disease and related factors in autumn of 2017 in Guangdong. Dis. Surv. 33(1), 37–41 (2018).
YW Wang. Prediction of epidemic characteristics and incidence trend of hand, foot and mouth disease (HFMD) in Guilin from 2010 to 2018: Guangxi Medical University; 2019.
Head, J. R. et al. Early Evidence of Inactivated Enterovirus 71 Vaccine Impact Against Hand, Foot, and Mouth Disease in a Major Center of Ongoing Transmission in China, 2011–2018: A Longitudinal Surveillance Study. Clin. Infect. Dis. https://doi.org/10.1093/cid/ciz1188 (2020).
Xin, Y. E. et al. Awareness of enterovirus 71 and willingness of self-paid Enterorirus type 71 inactivated vaccine immunization in guardians of children aged ≤ 3 years in Guangzhou. Dis. Surv. 32(3), 252–257 (2017).
Acknowledgements
We express our sincere gratitude to all participants.
Funding
This work was supported by Fengxian District Science and Technology Development Fund [Grant No. 20201425].
Author information
Authors and Affiliations
Contributions
Xiaodan Hu: Conceptualization, Data Curation, Software, Formal analysis, Writing—Original Draft. Weiyi Zhang: Conceptualization, Data Curation, Software, Formal analysis, supervision. Ting Yuan: Resources, Methodology, Writing—Review & Editing. Jie Wang: Etiological detection, Data Curation. Lixin Tao: Etiological detection. The authors read and approved the final manuscript. All authors have approved the manuscript for submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hu, X., Zhang, W., Yuan, T. et al. Evolving pathogen trends and spatial–temporal dynamics of hand, foot, and mouth disease in Fengxian District, Shanghai (2009–2022). Sci Rep 14, 20398 (2024). https://doi.org/10.1038/s41598-024-71389-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-71389-0
- Springer Nature Limited