
Abstract
Our aim was to investigate the clinical and pathologic characteristics of the epidermal growth factor receptor (EGFR) exon 18 mutations in East Asian lung adenocarcinomas patients. A total of 1,201 lung adenocarcinomas were analyzed for mutation in EGFR. Clinical and pathologic characteristics of patients with EGFR exon 18 mutations were compared with those who harbored classic activating mutations (exon 19 deletions and the L858R point mutation). The mutations in EGFR exon 18 were observed in 2.8% of 1,201 lung adenocarcinomas and 4.6% of patients with EGFR mutations. Patients with a single EGFR exon of 18 mutations had a worse overall survival than those harboring the complex EGFR exon of 18 mutations (p = 0.002) or those with classic activating mutations (p = 0.014). Four of five patients with EGFR exon 18 mutations showed objective response to the EGFR-TKI therapies after disease recurrence. Our results demonstrated that single EGFR exon 18 mutations may be an indicator of poor prognosis compared with complex EGFR exon 18 mutations or classic mutations. Furthermore, the results of the current study will be helpful for decision-making in the treatment of patients with EGFR exon 18 mutations.
Similar content being viewed by others


Introduction
Lung cancer is the leading cause of cancer-related death worldwide and non–small cell lung cancer (NSCLC) is the most common type of this disease1,2. With comprehensive understanding of the genetic alteration of lung cancer, many onco-targeted drugs had been developed and great achievements have been attained in patients with advanced disease3,4,5,6,7,8.
Patients with activating EGFR mutations are identified in ~20% of lung adenocarcinomas in Western countries9 and 40~60% of lung adenocarcinomas in East Asia10,11,12. These mutations mainly consist of in-frame deletions in exon 19 (~50%) and the L858R point mutation in exon 21 (~40%)9 and they are associated with a favorable response to the EGFR tyrosine kinase inhibitors (EGFR-TKI), such as gefitinib and erlotinib5,13. Exon 19 and 21 are located in the intracellular kinase domain of EGFR, which also includes exons 18 and 204.
Both point mutations in exon 18 and insertion mutations in exon 20 are relatively infrequent, respectively, at 3% and 5% of the EGFR mutations14,15. With more than 1.6 million cases of lung cancer diagnosed and 1.3 million deaths per year16, even small subgroups of NSCLC contribute to significant morbidity and mortality. Insertions in exon 20 of EGFR have been reported to be associated with resistance to EGFR-TKI and poor prognosis in NSCLC patients17,18,19,20. Single point mutations in exon 18 mainly consist of E709X and G719X mutations. Those mutations have been identified in several previous studies with limited sample sizes11,21,22,23. However, other complex EGFR mutations that included not only single point mutations in exon 18 but also other genetic alterations in the EGFR kinase domain were not well characterized. In addition, the relationship between the complex mutations and sensitivity to EGFR-TKI therapy has not been completely elucidated.
In this study, we retrospectively investigated the frequency, molecular spectrum and clinicopathologic characteristics of patients with EGFR exon 18 mutations in a large cohort of patients with lung adenocarcinomas. We also analyzed lung cancer patients with single or complex EGFR exon 18 mutations and their correlation to treatment outcome with EGFR-TKI.
Results
A total of 1,201 patients with lung adenocarcinomas were screened for EGFR mutation status. Of those, 737 (61.4%) patients were found to harbor mutations in EGFR. Among the patients who harbored EGFR mutations, we detected 34 (4.6% of 737) patients with mutations in the EGFR exon 18,661 (89.7%) cases with classic activating mutations (exon 19 deletions and L858R point mutation) and 42 patients harbored other rare mutations.
Of the 34 patients with EGFR exon 18 mutations, 27 (79.4%) were women and 29 (85.3%) were never-smokers. The amino acid sequence of the EGFR exon 18 mutations included 23 different variants and only 4 of 23 variants occurred more than once. Seventeen (50.0%) variants involved the G719 locus, 7 (20.6%) variants involved the E709 locus and 4 (11.8%) involved both G719 and E709, with 6 (17.6%) others. The predominant pathological subtype included 16 (47.1%) with acinar tumors, 8 (23.5%) with papillary tumors, 4 (11.8%) with solid tumors, 4 (11.8%) with lepidic tumors and 2 (5.9%) with minimally invasive adenocarcinoma (MIA) (Table 1).
The clinicopathologic characteristics for each individual patient who carried mutations in the EGFR exon 18 are shown in Table 1. No significant differences were identified between the patients carrying a mutation in exon 18 and those with activating mutations regarding age, smoking status, stage, tumor size and differentiation (Table 2).
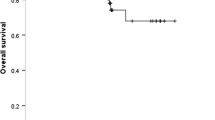
A total of 33 patients with EGFR exon 18 mutations and 489 patients with classic activating mutations diagnosed from October 2007 to March 2011 were included for survival analysis. The median follow-up duration of these patients was 33 months (range: 1–78 months). There were no significant differences in RFS (p = 0.652, Fig. 1A) and OS (p = 0.984, Fig. 1B) between patients with EGFR exon 18 mutations and patients with classic activating mutations. We further divided patients with exon 18 mutations into two subgroups: patients with single EGFR exon 18 mutations and those with complex EGFR exon 18 mutations (EGFR exon 18 mutations + other EGFR mutations). In univariate analysis, although there were no significant differences in RFS between those two subgroups (log-rank p = 0.246, Fig. 1C) and between single EGFR exon 18 mutations and classic mutations (log-rank p = 0.310, Fig. 1C), the OS of patients with single EGFR exon 18 mutations was much worse than those with complex EGFR exon 18 mutations (log-rank p = 0.002, Fig. 1D) or those with classic mutations (log-rank p = 0.014, Fig. 1D). Gender (p = 0.003), smoking history (p < 0.001), tumor size (p < 0.001), stage (p < 0.001) and differentiation (p < 0.001) were significantly associated with RFS. Smoking history (p = 0.017), tumor size (p < 0.001), stage (p < 0.001) and differentiation (p < 0.001) were significantly correlated with a worse OS (Supplementary Table S1). In multivariate analysis incorporating mutation status, gender, age, smoking history, tumor size (≤3 vs. >3 cm), stage (I vs. II–IV), differentiation (well/moderate vs. poor), smoking history (hazard ratio = 2.184, 95% confidence interval: 1.393–3.422, p = 0.001), tumor size (hazard ratio = 1.397, 95% confidence interval: 1.057–1.845, p = 0.019), stage (hazard ratio = 4.763, 95% confidence interval: 3.485–6.510, p < 0.001) and differentiation (hazard ratio = 1.608, 95% confidence interval: 1.199–2.156, p = 0.002) were the independent predictor of RFS and single exon 18 mutations (hazard ratio = 2.239, 95% confidence interval: 1.005–4.989, p = 0.049), tumor size (hazard ratio = 1.917, 95% confidence interval: 1.247–2.947, p = 0.003), stage (hazard ratio = 5.644, 95% confidence interval: 3.064–10.396, p < 0.001) and differentiation (hazard ratio = 2.036, 95% confidence interval: 1.310–3.165, p = 0.002) were the independent predictor of OS (Supplementary Table S2).

Recurrence-free survival (RFS) and overall survival (OS) of cancers with EGFR exon 18 mutations.
Kaplan–Meier survival curves for RFS (A) and OS (B) analyses between classic activating mutations and exon 18 mutations. Kaplan–Meier survival curves for RFS (C) and OS (D) analyses among single exon 18 mutations (indicated as ‘exon 18 only’), complex exon 18 mutations (indicated as ‘exon 18 + X’) and classic mutations. The log-rank test is used.
Nine patients received platinum-based combination chemotherapies and one patient received fluorouracil. Of these, two patients received neoadjuvant chemotherapies before surgery and eight received chemotherapies after disease recurrence. Of the two patients who received neoadjuvant chemotherapies, according to Response Evaluation Criteria in Solid Tumors (RECIST), one had a RECIST stable disease and the other had a RECIST partial response. Of the eight patients receiving chemotherapy, one had a RECIST partial response, two had RECIST stable disease, four had RECIST progressive disease and one was of unknown status because of loss to follow-up (Table 1). The only one patient receiving radiotherapy after disease recurred had a RECIST stable disease (Table 1).
After the disease relapsed, five patients with EGFR exon 18 mutations received EGFR-TKI therapies, including 2 treated with erlotinib and 3 with gifitinib as first-, second- or third-line therapy. According to RECIST, four patients had a RECIST partial response. The times to progression for these patients were 65.0, 14.8+ 20.7+ and 37.5+ months, respectively and the overall survival after taking the TKIs were 68+, 14.8+, 29.4+ and 37.5+ months, respectively (Table 3). One patient had a RECIST stable disease and both the RFS and OS were 24.2+ months (Table 3).
Discussion
The management of lung adenocarcinomas has been transformed by the identification of targetable oncogenic drivers that confer sensitivity to specific tyrosine kinase inhibitors. Activating mutations in the EGFR gene, such as a deletion on exon 19 and a point mutation in exon 21, identifies a distinct subset of lung cancers that are uniquely sensitive to EGFR-TKIs. In the current study, we demonstrated that exon 18 mutations represent an additional target that is sensitive to EGFR-TKI therapy, regardless of less common than classic EGFR mutations.
In the current study, five patients who harbored EGFR exon 18 mutations had a favorable RFS after receiving the TKI therapies. The response rates (4/5) and RFS of our cohort were greater than those reported by other groups21,22,24,25,26. This may be due to the ethnicity and small sample size of our cohort. In addition, one patient harbored double point mutations (G719S+L861Q) and obtained an amazing RFS of 65 months, which causes us to explore the potential effect of TKI therapies on different EGFR mutations. We also found that two patients benefited from TKI therapies after failure to ameliorate the tumor progression by chemotherapies. Furthermore, therapy for one patient failed to ameliorate the tumor progression by radiotherapy and to obtain similar improvement. Taken together, our results suggest that TKI therapies should be considered as a prior choice for advanced lung adenocarcinoma patients with EGFR mutations in exon 18.
Although some previous reports showed the discordance of EGFR mutation between primary and metastatic tumors27,28, further studies with large sample sizes and studies utilizing the high throughput technology of whole exome sequencing demonstrated that driver events, such as EGFR and BRAF mutations, were highly consistent between primary and metastatic tumors. Given that the samples were obtained mainly by aspiration biopsy and FFPE tissues29,30, the quality and quantity might not be enough to obtain an accurate EGFR mutation status.
Survival analysis results showed that there were no significant differences in RFS and OS between EGFR mutations in exon 18 and classic activating mutations. A comparison of the Kaplan-Meier curves suggested that the OS of patients with single exon 18 mutations was shorter than those with complex exon 18 mutations or patients with classic EGFR mutations. However, there were no significant differences in RFS between patients with single exon 18 mutations and those with complex exon 18 mutations or classic mutations. Our results indicate that single EGFR exon 18 mutations may be an indicator of poor prognosis compared with classic activating mutations or complex exon 18 mutations. Further investigations are required to address these differences.
To our knowledge, this report is the first comprehensive study of clinicopathologic features of EGFR exon 18 mutations in a large cohort of patients with lung adenocarcinoma. We showed that EGFR mutations in exon 18 were present in 2.8% of lung adenocarcinomas and 4.6% of EGFR mutations, which were similar to the prevalence of EGFR exon 20 insertion mutations in East Asians as we previously reported31. A limited number of cases with EGFR exon 18 mutations had been reported by previous studies22,25. It is therefore difficult to draw conclusions as to their true prevalence, molecular spectrum and clinicopathologic features. We found 23 kinds of variants of EGFR exon 18 mutations in the current study. Of all exon 18 mutations, G719X mutations in EGFR exon 18 were the most common variant and E709X mutations were the second most common, which was similar to a previous report22. We also showed that patients harboring EGFR exon 18 mutation had clinicopathologic characteristics very similar to those with classic EGFR activating mutations, which were characterized as being more frequent in females and never smokers10,32.
There are several limitations of this study. First, the finding that patients with single exon 18 mutations had a significantly worse OS than those with complex exon 18 mutations was based on a small number of patients, which needs to be validated in a larger series of patients. Second, we conducted cDNA-PCR sequencing as the major experimental method to identify mutations. Results obtained by analyzing corresponding data involving those from the negative EGFR mutations group might change if more sensitive methods, such as the amplification refractory mutation system (ARMS), are used.
In conclusion, our data demonstrated that EGFR exon 18 mutations occurred in 2.8% of patients with NSCLCs and 4.6% of patients with EGFR mutations. Single EGFR exon 18 mutations may be an indicator of poor prognosis compared with classic activating mutations. Given that 4 of 5 patients with EGFR mutations in exon 18 had an objective response to the TKIs therapies and a RFS of 65.0, 14.8+, 20.7+ and 37.5+ months in our cohort, we suggest that advanced patients with those mutations should have TKIs as prior therapy.
Methods
Patients and Samples
From October 2007 to January 2013, we consecutively collected lung tumors resected at the Department of Thoracic Surgery, Fudan University Shanghai Cancer Center, Shanghai, China. Inclusion criteria for this study were as follows: (1) patients underwent complete resection with curative intent and (2) specimens were pathologically confirmed as lung adenocarcinomas with a minimum of 50% of tumor cells and sufficient tissue for comprehensive mutational analyses.
Pathologic slides were reviewed by two certified pathologists (Xuxia Shen and Yuan Li) to classify histologic subtypes of lung adenocarcinomas according to the IASLC/ATS/ERS multidisciplinary classification system33. The following clinicopathologic parameters for each patient were also collected: gender, age at diagnosis, smoking history, systemic treatment of advanced lung cancers and pathologic TNM stage in line with the seventh edition of the lung cancer staging system34. Recurrence-free survival (RFS) and overall survival (OS) of patients diagnosed from October 2007 to March 2011 (because of relatively insufficient follow-up duration) were recorded based on a follow-up clinic visit or a telephone call.
Mutational Analysis
After frozen tumor specimens were dissected in TRIzol reagent (Invitrogen, Carlsbad, CA), DNA and RNA were extracted as per standard protocol and the RNA was reverse transcribed into cDNA by a RevertAid First Strand cDNA Synthesis Kit (Fermentas, EU). EGFR (exons 18–21) were amplified by PCR routinely using cDNA. Direct dideoxynucleotide sequencing was then performed to analyze the amplified products. The EGFR (exons 18–21) amplified products obtained by PCR using DNA for sequencing were used to confirm the uncommon EGFR mutations. Primers and PCR condition are listed in the supplementary Table 3.
Statistical Analysis
Pearson’s χ2 test or Fisher’s exact test was used to investigate the correlations between two categorical variables. The association between one categorical variable and one continuous variable was assessed using the independent sample t-test. The RFS and OS distribution was analyzed using the Kaplan–Meier method and log-rank tests were employed for comparisons of RFS or OS between two categories in univariate analysis. Multivariate survival analysis was conducted using the Cox proportional hazards regression (forward likelihood ratio model) to identify independent prognostic factors. Statistical analyses were performed using SPSS (Statistical Package for the Social Sciences) 16.0 software (SPSS Inc., Chicago, IL). All tests were two-tailed. Statistical significance was set at p < 0.05.
Ethics Statement
This study was conducted in line with the Helsinki Declaration and approved by the Institutional Review Board of the Fudan University Shanghai Cancer Center. Written informed consent was obtained from each patient to allow their biological samples to be genetically analyzed. The experimental protocol of this study was performed strictly in accordance with the guidelines.
Additional Information
How to cite this article: Cheng, C. et al. EGFR Exon 18 Mutations in East Asian Patients with Lung Adenocarcinomas: A Comprehensive Investigation of Prevalence, Clinicopathologic Characteristics and Prognosis. Sci. Rep. 5, 13959; doi: 10.1038/srep13959 (2015).
References
Parkin, D. M. Global cancer statistics in the year 2000. The lancet oncology 2, 533–543 (2001).
Spiro, S. G. & Silvestri, G. A. One hundred years of lung cancer. Am J Resp Crit Care 172, 523–529 (2005).
Kwak, E. L. et al. Anaplastic lymphoma kinase inhibition in non–small-cell lung cancer. N Engl J Med 363, 1693–1703 (2010).
Lynch, T. J. et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non–small-cell lung cancer to gefitinib. N Engl J Med 350, 2129–2139 (2004).
Paez, J. G. et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science 304, 1497–1500 (2004).
Soda, M. et al. Identification of the transforming EML4–ALK fusion gene in non-small-cell lung cancer. Nature 448, 561–566 (2007).
Cappuzzo, F., Bemis, L. & Varella-Garcia, M. HER2 mutation and response to trastuzumab therapy in non–small-cell lung cancer. N Engl J Med 354, 2619–2621 (2006).
Davies, H. et al. Mutations of the BRAF gene in human cancer. Nature 417, 949–954 (2002).
Dogan, S. et al. Molecular epidemiology of EGFR and KRAS mutations in 3,026 lung adenocarcinomas: higher susceptibility of women to smoking-related KRAS-mutant cancers. Clin Cancer Res 18, 6169–6177 (2012).
Sun, Y. et al. Lung adenocarcinoma from East Asian never-smokers is a disease largely defined by targetable oncogenic mutant kinases. J Clin Oncol 28, 4616–4620 (2010).
Wu, J. Y. et al. Effectiveness of tyrosine kinase inhibitors on “uncommon” epidermal growth factor receptor mutations of unknown clinical significance in non-small cell lung cancer. Clin Cancer Res 17, 3812–3821 (2011).
Wu, Y.-L. et al. Intercalated combination of chemotherapy and erlotinib for patients with advanced stage non-small-cell lung cancer (FASTACT-2): a randomised, double-blind trial. Lancet Oncol 14, 777–786 (2013).
Mok, T. S. et al. Gefitinib or carboplatin–paclitaxel in pulmonary adenocarcinoma. N Engl J Med 361, 947–957 (2009).
Pao, W. & Chmielecki, J. Rational, biologically based treatment of EGFR-mutant non-small-cell lung cancer. Nat Rev Cancer 10, 760–774 (2010).
Mitsudomi, T., Kosaka, T. & Yatabe, Y. Biological and clinical implications of EGFR mutations in lung cancer. Int J Clin Oncol 11, 190–198 (2006).
Jemal, A. et al. Global cancer statistics. CA-Cancer J Clin 61, 69–90 (2011).
Oxnard, G. R. et al. Natural history and molecular characteristics of lung cancers harboring EGFR exon 20 insertions. J Thorac Oncol 8, 179 (2013).
Pao, W. et al. Acquired resistance of lung adenocarcinomas to gefitinib or erlotinib is associated with a second mutation in the EGFR kinase domain. PLoS Med 2, e73 (2005).
Wu, J.-Y. et al. Lung cancer with epidermal growth factor receptor exon 20 mutations is associated with poor gefitinib treatment response. Clin Cancer Res 14, 4877–4882 (2008).
Yasuda, H., Kobayashi, S. & Costa, D. B. EGFR exon 20 insertion mutations in non-small-cell lung cancer: preclinical data and clinical implications. Lancet Oncol 13, e23–e31 (2012).
Gauthier, H. et al. Two Cases of Non-small-cell lung cancer with rare complex mutation of EGFR exon 18 but different response to targeted therapy. J Thorac Oncol 9, e78–79 (2014).
Beau-Faller, M. et al. Rare EGFR exon 18 and exon 20 mutations in non-small-cell lung cancer on 10 117 patients: a multicentre observational study by the French ERMETIC-IFCT network. Ann Oncol 25, 126–131 (2013).
Keam, B. et al. Rare and complex mutations of epidermal growth factor receptor and efficacy of tyrosine kinase inhibitor in patients with non-small cell lung cancer. Int J Clin Oncol 19, 594–600 (2013).
Watanabe, S. et al. Effectiveness of gefitinib against non–small-cell lung cancer with the uncommon EGFR mutations G719X and L861Q. J Thorac Oncol 9, 189–194 (2014).
Wu, J. Y. et al. Effectiveness of tyrosine kinase inhibitors on “uncommon” epidermal growth factor receptor mutations of unknown clinical significance in non-small cell lung cancer. Clin Cancer Res 17, 3812–3821 (2011).
Peng, L., Song, Z. G. & Jiao, S. C. Efficacy analysis of tyrosine kinase inhibitors on rare non-small cell lung cancer patients harboring complex EGFR mutations. Sci Rep 4, 6104, 10.1038/srep06104 (2014).
Gow, C.-H. et al. Comparison of epidermal growth factor receptor mutations between primary and corresponding metastatic tumors in tyrosine kinase inhibitor-naive non-small-cell lung cancer. Ann Oncol. mdn679 (2008).
Kalikaki, A. et al. Comparison of EGFR and K-RAS gene status between primary tumours and corresponding metastases in NSCLC. Br J Cancer 99, 923–929 (2008).
de Bruin, E. C. et al. Spatial and temporal diversity in genomic instability processes defines lung cancer evolution. Science 346, 251–256 (2014).
Yatabe, Y., Matsuo, K. & Mitsudomi, T. Heterogeneous distribution of EGFR mutations is extremely rare in lung adenocarcinoma. J Clin Oncol 29, 2972–2977 (2011).
Pan, Y. et al. Prevalence, clinicopathologic characteristics and molecular associations of EGFR exon 20 insertion mutations in east asian patients with lung adenocarcinoma. Ann Surg Oncol 21 Suppl 4, 490–496 (2014).
Rosell, R. et al. Screening for epidermal growth factor receptor mutations in lung cancer. N Engl J Med 361, 958–967 (2009).
Travis, W. D. et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol 6, 244–285 (2011).
Detterbeck, F. C., Boffa, D. J. & Tanoue, L. T. The new lung cancer staging system. Chest 136, 260–271 (2009).
Acknowledgements
This work was funded by the National Natural Science Foundation of China (81330056, 81401886, 81401891, 81422029, 81472173 and 81372525), the Key Project of Science and Technology Commission of Shanghai Municipality (JGGG1302) and the Shen-Kang Center Project (SKMB1201).
Author information
Authors and Affiliations
Contributions
C.C. and R.W. designed this study, performed experiments and wrote the main manuscript. Y.L. and X.X.S. reviewed the pathologic slides and collected the pathologic data. Y.J.P., Y.Z., H.L., D.F.Z. and S.B.Z. collected the clinical data, tumor samples and performed experiments. H.Q.C. and Y.H.S. designed and directed the overall project. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Cheng, C., Wang, R., Li, Y. et al. EGFR Exon 18 Mutations in East Asian Patients with Lung Adenocarcinomas: A Comprehensive Investigation of Prevalence, Clinicopathologic Characteristics and Prognosis. Sci Rep 5, 13959 (2015). https://doi.org/10.1038/srep13959
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep13959
- Springer Nature Limited
This article is cited by
-
Global prognostic impact of driver genetic alterations in patients with lung adenocarcinoma: a real-life study
BMC Pulmonary Medicine (2022)
-
Prediction of sensitivity to gefitinib/erlotinib for EGFR mutations in NSCLC based on structural interaction fingerprints and multilinear principal component analysis
BMC Bioinformatics (2018)
-
Third generation EGFR TKIs: current data and future directions
Molecular Cancer (2018)
-
Response to Tyrosine Kinase Inhibitors in Lung Adenocarcinoma with the Rare Epidermal Growth Factor Receptor Mutation S768I: a Retrospective Analysis and Literature Review
Targeted Oncology (2017)
-
EGFR tyrosine kinase inhibitors versus chemotherapy as first-line therapy for non-small cell lung cancer patients with the L858R point mutation
Scientific Reports (2016)