
Abstract
Reducing lung cancer risk by modifying diet is highly desirable. We investigated whether different U.S. dietary patterns were associated with lung cancer risk. Dietary patterns were derived using exploratory factor analysis for 2139 non-small cell lung cancer (NSCLC) cases and 2163 frequency-matched controls. Logistic regression was used to estimate odds ratios (ORs) and 95% confidence intervals (95% CIs). Highest adherence (highest vs. lowest quintile) to the “Tex-Mex”, “fruits and vegetables” and “American/Western” patterns was associated with a 55% reduced (OR = 0.45; 95% CI = 0.37–0.56; P < 0.001), 32% reduced (OR = 0.68; 95% CI = 0.55–0.85; P = 0.001) and 45% increased (OR = 1.45; 95% CI = 1.18–1.78; P < 0.001) risk of lung cancer, respectively. The effects were stronger for squamous cell carcinoma and ever smokers for the “fruits and vegetables” pattern and stronger for other non-small cell lung cancer and never smokers for the “American/Western” pattern. Among six genome-wide association (GWA) studies-identified lung cancer susceptibility loci assessed, a variant (rs2808630) of the C-reactive protein gene modified the associations for the “fruits and vegetables” (P for interaction = 0.03) and “American/Western” (P for interaction = 0.02) patterns. Our study first showed that the “Tex-Mex” dietary pattern was associated with a reduced lung cancer risk. Also, the “fruits and vegetables” and “American/Western” patterns affected lung cancer risk and the effects were further modified by host genetic background.
Similar content being viewed by others

Introduction
Lung cancer is the second most common cancer in both men and women in the U.S.1. Smoking is the most important risk factor for lung cancer1. In addition to smoking, other factors such as diet may also play a role in lung carcinogenesis2. Previous studies suggested that consumption of fruits as well as foods containing carotenoids probably decreased lung cancer risk2; however evidence on other dietary factors is not conclusive2. Typically, previous studies have focused on the effects of specific nutrients, but it is difficult to discriminate the effect of a specific nutrient due to the strong correlations between nutrients.
Dietary pattern analysis (e.g., factor analysis) is a novel way to examine the effect of diet on cancer3. A few studies have investigated the associations between dietary patterns and lung cancer risk using factor analysis4,5,6,7,8. Though the findings are not definitive, they all suggest that a “healthy” diet characterized by high vegetable intake is associated with a decreased risk of lung cancer, while a “Western” diet characterized by high fat and red meat intake is associated with an increased risk. However, most of the studies were conducted outside of the U.S.5,6,7,8, except one small study4. Also, evidence on other American dietary patterns is very limited. For example, Texas Mexican cuisine (“Tex-Mex”) is an American regional cuisine which is the most popular in the state of Texas and spreads to the rest of the U.S. as well as Canada.
Several studies showed that the associations of dietary patterns and lung cancer could be modified by host smoking status4,5,6,9,10. Due to the complex gene-diet interaction, the association of dietary patterns and lung cancer risk may be modified by host genetic background, which has not been investigated in previous studies. Previous genome-wide association (GWA) studies have identified multiple lung cancer susceptibility loci among individuals of European ancestry11,12,13,14,15,16 and two of the identified loci are mapped to the C-reactive protein (CRP) gene and interleukin 1 receptor accessory protein (IL1RAP) gene, respectively. Both genes play an important role in host inflammatory response which is closely linked to lung cancer development17. Since dietary factors are known to have a major effect on host inflammatory response18,19, it is likely that the associations of dietary patterns with lung cancer risk will be modified by these inflammation-related loci.
In the present study, we investigated the associations between three dietary patterns derived by factor analysis (“fruits and vegetables”, “American/Western” and “Tex-Mex”) and non-small cell lung cancer (NSCLC) risk using data from a large ongoing Texas-based case-control study. Further, we investigated whether the associations differed by major histological types of NSCLC and whether the associations could be modified by host smoking status and lung cancer susceptibility loci identified in previous GWA studies.
Results
Identified dietary patterns and host characteristics
Exploratory factor analysis identified three dietary patterns that together accounted for 26% of the total variance and the top 10 food items/groups contributing to each factor are listed in Table 1. The three dietary patterns were named “fruits and vegetables”, “American/Western” and “Tex-Mex” based on the food items/groups that were strongly correlated with each dietary pattern. The spearman correlation coefficients of the factor scores for the three dietary patterns with nutrient intake are shown in Supplementary Table 1.
Selected characteristics of the 2139 NSCLC cases and 2163 controls are presented in Table 2. Cases and controls differed in education, smoking pack-year, family history of lung cancer among first degree relatives, body mass index (BMI), physical activity and daily intake of protein.
Associations of dietary patterns with non-small cell lung cancer risk
Age- and sex-adjusted and multivariable-adjusted associations of dietary patterns with lung cancer risk are presented in Table 3. In age- and sex-adjusted models, all three dietary patterns were associated with lung cancer risk (P for trend < 0.001). In multivariable-adjusted models, compared to the lowest quintile of the score on the “fruits and vegetables” pattern, the highest quintile was associated with a 32% decreased risk (ORQ5 vs. Q1 = 0.68; 95% CI = 0.55–0.85; P for trend = 0.001). Higher adherence to the “American/Western” dietary pattern was associated with an increased risk of lung cancer (ORQ5 vs. Q1 = 1.45; 95% CI = 1.18–1.78; P for trend < 0.001). Higher adherence to the “Tex-Mex” pattern was associated with a decreased risk (ORQ5 vs. Q1 = 0.45; 95% CI = 0.37–0.56; P for trend < 0.001).
Stratified associations by histological types of non-small cell lung cancer and smoking status
The stratified associations by major histological type of NSCLC and smoking status are summarized in Tables 4 and 5, respectively. The three dietary patterns were associated with risks of all three major histological types. The protective effects of the “fruits and vegetables” pattern were more evident for squamous cell carcinoma. The harmful effects of the “American/Western” pattern were more pronounced for other NSCLC. The effects of the “Tex-Mex” pattern were similar across all histological types.
The negative association of the “fruits and vegetables” pattern with lung cancer risk was present among current or former smokers and not present among never smokers and the P for interaction was 0.03. The “American/Western” pattern was associated with an increased risk of lung cancer irrespective of smoking status; however, the association was stronger among never smokers, although the P for interaction (0.44) was not statistically significant. The association for the “Tex-Mex” pattern did not differ by smoking status (P for interaction = 0.87).
Stratified associations by GWA studies-identified susceptibility loci
The overall associations between dietary patterns and lung cancer risk in this subset of study population were similar to these in the total study population (Table 3). Among the six selected SNPs, four (rs1051730, rs2808630, rs7626795, rs6495309) were associated with lung cancer risk in this sample (P < 0.05). The stratified associations of dietary patterns with lung cancer risk by genotype at rs2808630 of the CRP gene are summarized in Table 6. The “fruits and vegetables” pattern was associated with a reduced risk of lung cancer only among those without a copy of the minor allele (ORQ5 vs. Q1 = 0.42; 95% CI = 0.26-0.69; P for trend = 0.001; P for interaction = 0.03). In contrast, the “American/Western” pattern was associated with an increased risk of lung cancer only among those with at least one copy of the minor allele (ORQ5 vs. Q1 = 1.93; 95% CI = 1.27–2.93; P for trend = 0.001; P for interaction = 0.02). The “Tex-Mex” pattern was associated with a reduced risk of lung cancer irrespective of the genotype at CRP rs2808630 (P for interaction = 0.27). No statistically significant interactions (P for interaction > 0.05) were found between dietary patterns and the other five (rs1051730, rs3117582, rs7626795, rs402710, rs6495309) selected variants (Supplementary Table 2).
Discussion
In this large Texas-based case-control study, we identified three dietary patterns using factor analysis: “fruits and vegetables”, “American/Western” and “Tex-Mex”. Our study is the first to show that the “Tex-Mex” pattern was associated with a substantially reduced lung cancer risk. In addition, we found that the “fruits and vegetables” pattern was associated with a reduced risk and the protective effects were more evident for squamous cell carcinoma and among ever smokers. In contrast, the “American/Western” pattern was associated with an increased risk and the harmful effects were more pronounced for other NSCLC and among never smokers. Finally, for the first time, we found that the effects of the “fruits and vegetables” and “American/Western” patterns were further modified by a variant (rs2808630) of the CRP gene.
Our study is the first report to show that the “Tex-Mex” dietary pattern is associated with substantially reduced lung cancer risk and the effects are consistent and stable across different sub-groups. Except our previous study with a smaller sample size which reported a non-statistically significant protective effect on renal cell carcinoma20, there has been no other studies on the “Tex-Mex” dietary pattern and cancer. The mechanism(s) linking high adherence to the “Tex-Mex” pattern with a decreased risk of lung cancer is unclear. “Tex-Mex” cuisine is characterized by its heavy use of legumes, spices and shredded cheese. Legumes are rich sources of dietary fiber, a variety of micronutrients and phytoestrogens with potential cancer-preventive effects21. In particular, our previous study showed that higher intake of phytoestrogens was associated with a decreased risk of lung cancer22. Also, spices or their bioactive components may prevent cancer through their anti-microbial, anti-oxidant and inhibition of carcinogen bioactivation effects23. Finally, high levels of cheese intake were found to be associated with a reduction in lung cancer risk in multiple studies24,25,26 and menaquinones and conjugated dienoic derivatives of linoleic acid in cheese were suspected to mediate the protective effects27,28.
Our findings on the “fruits and vegetables” and “American/Western” dietary patterns are consistent with findings from previous studies on dietary pattern and lung cancer. Previous studies using factor analysis4,5,6,7,8 found that a “healthy” diet characterized by high vegetable intake was associated with a decreased risk of lung cancer, while a “Western” diet characterized by high fat and red meat intake was associated with increased risk. In addition to dietary patterns derived from factor analysis, several studies also investigated index-based dietary patterns. Three studies found that diet quality index was inversely associated with subsequent lung cancer risk10,29,30 and diet quality was assessed by the recommended foods score or dietary guideline index, which reflects compliance with the current dietary guidance of increasing consumption of fruits, vegetables, whole grains, lean meats or meat alternatives and low-fat dairy. Additionally, a Mediterranean dietary pattern was found to be inversely associated with lung cancer risk9.
In our study, we found that the inverse associations of the “fruits and vegetables” pattern with lung cancer risk were only present among current or former smokers but not present among never smokers. This observation was consistent with the findings from previous dietary pattern studies on lung cancer that the beneficial effects of dietary patterns characterized by high consumption of fruits or vegetables were only evident in current or former smokers4,5,6,9,10. Smoking causes lung cancer in part through its pro-oxidant properties31. It is believed that the protective effects of fruits and vegetables are due to their rich collection of various antioxidants32,33,34 and this may explain why the protective effects were only seen in ever smokers. In addition, this is in line with our observation that the protective effects of the “fruits and vegetables” pattern were more evident for squamous cell carcinoma, which is most strongly associated with smoking among the main histological types of NSCLC35.
For the first time, we found that the “fruits and vegetables” and “American/Western” patterns interacted with a lung cancer susceptibility locus (rs2808630). The rs2808630 locus is mapped to the 3′ untranslated region of the CRP gene, which is a key gene in host inflammatory response17. Previous studies showed that higher fruit and vegetable intake was associated with lower circulating CRP levels36,37. Also, it is known that the “American/Western” diet leads to increased systemic inflammation19,38,39,40. According to a recent meta-analysis of 10 prospective studies41, circulating CRP levels, a marker for systemic inflammation, were positively associated with lung cancer risk. The CRP rs2808630 polymorphism has been shown to affect circulating CRP levels42,43. More importantly, one study showed that the GG genotype at CRP rs2808630, compared with the AA or AG genotype, was associated with a larger CRP increase in response to pro-inflationary stimuli and this may explain our observation that the harmful effects of the “American/Western” pattern were only evident among those with the GG or AG genotype.
Our study has several limitations. First, the dietary data were collected for the year before diagnosis (cases) or enrollment (controls) and it may not represent the time window of interest (e.g., many years prior to lung cancer diagnosis when lung cancer has not been initiated yet). However, longitudinal studies showed that a single food frequency questionnaire measurement at one time point could characterize dietary habits for a period of at least 5–10 years44 and dietary patterns assessed with a food-frequency questionnaire were stable over time45. Second, our study is subject to recall bias because cases and controls may recall dietary intakes differently. Nevertheless, the direction and magnitude of the associations for the “fruits and vegetables” and “American/Western” patterns in our study were consistent with and comparable to those found in a prospective study where dietary data were collected around ten years prior to diagnosis5. Since the impact of the “Tex-Mex” dietary pattern on human health was not reported and therefore not publicized before, the findings for the “Tex-Mex” dietary pattern are less likely to be biased due to differential recall. Third, our analysis was limited to non-Hispanic whites and caution should be taken when generalizing our results to other populations.
Despite these limitations, our study has several strengths. First, to our knowledge, this study is the first to show a protective effect of the “Tex-Mex” dietary pattern on lung cancer and the first to assess the interaction between dietary patterns and genetic variations on lung cancer risk. Second, our study had the largest sample size in terms of number of cases among the studies on dietary pattern and lung cancer risk using factor analysis. Third, the FFQ used in this study was previously validated. Finally, the two dietary patterns that explained the most variation in our study have been consistently identified in previous studies4,5,6,7,8 and we were able to assess a third dietary pattern (the “Tex-Mex” pattern) because consumption of “Tex-Mex” foods is relatively common in this Texas-based case-control study.
In summary, our study adds to the growing evidence that diet plays an important role in lung carcinogenesis which is thought by many to be caused solely by smoking. In particular, our study suggests that “Tex-Mex” cuisine may reduce lung cancer risk and more studies are needed to confirm this novel finding and to explore the underlying mechanism(s). Also, our study together with previous studies supports that maintaining a “healthy” diet (increasing consumption of fruits and vegetables and limiting energy-dense and processed foods) may prevent lung cancer and the beneficial effects are further modified by genetic background.
Methods
Study population
Cases and frequency-matched controls were accrued from a large ongoing case-control study of lung cancer. Cases were newly-diagnosed and histologically confirmed NSCLC patients from The University of Texas MD Anderson Cancer Center. There were no restrictions on age, sex, race/ethnicity, or stage. Healthy controls without a history of cancer (except for nonmelanoma skin cancer) were recruited from the Kelsey-Seybold Clinics, the largest private multispecialty physician group in the Houston metropolitan area with 18 clinics, more than 325 physicians and over 400,000 patients. The rationale of recruiting controls from the Kelsey-Seybold Clinic has been previously discussed46. When potential control participants visited the Kelsey-Seybold Clinic for annual physical exams, Kelsey-Seybold Clinic staff distributed a brief questionnaire to elicit the patients’ willingness to be contacted by staff at MD Anderson and to collect preliminary demographic data for frequency-matching. For those who were willing to participate, staff at MD Anderson then contacted them by telephone to confirm their willingness to participate and to schedule an in-person interview at a Kelsey-Seybold Clinic convenient to the participant. Controls were frequency-matched on age (±5 years), sex, race/ethnicity and smoking status (current, former, never). To date, the response rate among both cases and controls has been approximately 80%. All participants provided written informed consent prior to participation in the study. This study was approved by The University of Texas MD Anderson Cancer Center and Kelsey-Seybold institutional review boards and all methods and analyses were conducted in accordance with this approval.
Data collection
MD Anderson staff interviewers conducted interviews to collect epidemiological data on demographics, education, smoking, family history of cancer, height, weight and physical activity. Additionally, dietary intake during the year prior to diagnosis (cases) or study enrollment (controls) was assessed with a previously validated food frequency questionnaire (FFQ, a modified version of the National Cancer Institute’s Health Habits and History Questionnaire)47. The questionnaire has been shown to be a valid and reliable food frequency survey tool across various populations48,49. This questionnaire asks about the frequency and portion size of food and beverage items, ethnic foods commonly consumed in the Houston area, an open-ended section and other dietary behavior questions regarding such factors as dining at restaurants and food preparation methods. From the dietary information obtained in the FFQ, total energy intake and amount consumed (g/day) for each food or beverage item were calculated based on the United States Department of Agriculture (USDA) National Nutrient Database for Standard Reference50. For multi-ingredient foods items not included in Standard Reference, calculations were based on the US Department of Agriculture Food and Nutrient Database for Dietary Studies51. Blood samples (40 mL each) were collected from the study participants for genotyping.
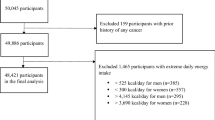
Exclusions and eligibility
The exclusions and eligibility criteria for this study were previously reported46. For the present study, we limited the analysis to non-Hispanic whites because of the existing dietary variations between non-Hispanic whites and other racial/ethnic groups52,53 as well as insufficient statistical power for other racial/ethnic groups. Also, we further excluded those (n = 138) with outlying total energy intake. The final analysis in this study included 2139 cases and 2163 controls.
Dietary pattern analysis
The details of dietary pattern analysis were reported in our previous study20. Briefly, 117 out of 159 food and beverage items in the FFQ were included in the final dietary pattern analysis. We excluded foods with low frequency of consumption (<5%) in our study population. Also, several dietary items were grouped into predefined food groups according to current US Department of Agriculture food-group guidelines. For the remaining 117 dietary items, the daily intake was log-transformed and then energy-adjusted using the residual method54.
We conducted an exploratory factor analysis with the FACTOR command in Stata 13.0 (StataCorp LP, College Station, Texas) to reduce the number of dietary items into a small number of factors and the factors were then rotated using a varimax rotation, an orthogonal rotation procedure. The Kaiser-Meyer-Olkin statistic was equal to 0.85, suggesting a “meritorious” sampling adequacy (relative to the number of dietary items) for conducting dietary pattern analysis. The number of factors that best represented the data was chosen on the basis of eigenvalues greater than one, identification of a break point in the scree plot, interpretability and our previous dietary pattern analysis on renal cell carcinoma20. We identified three factors that best represented the dietary input data and these three dietary patterns were identical to the three patterns identified in our previous study of renal cell carcinoma20. The final analysis was restricted only to the three chosen factors. For each participant, a factor score was computed for each of the three identified factors to indicate levels of adherence to one dietary pattern with higher scores indicating higher adherence. Factor scores were categorized into quintiles based on the sex-specific distribution in the control group.
Selection of SNPs
We initially selected nine common (minor allele frequency >5%) single-nucleotide polymorphisms (SNPs, rs1051730, rs3117582, rs8034191, rs2808630, rs7626795, rs401681, rs402710, rs8042374 and rs17879961) that were identified in previous GWA studies among individuals of European ancestry11,12,13,14,15,16. Among them, seven SNPs (except rs8042374 and rs17879961) were directly genotyped for a subset of 855 cases and 1036 controls in our previous GWAS and rs6495309 was selected as a proxy for rs8042374 because they are in high linkage disequilibrium (LD r2 = 0.95). Genotyping procedures were previously reported in details11. One SNP (rs401681) was not included because it was not in Hardy-Weinberg equilibrium (P = 0.02). Furthermore, rs1051730 and rs8034191 are highly correlated (LD r2 = 0.85), so only rs1051730 was included in the analysis, leaving six SNPs (rs1051730, rs3117582, rs2808630, rs7626795, rs402710 and rs6495309) included in the final analysis.
Statistical Analysis
Baseline characteristics of cases and controls were compared using the Student’s t-test for continuous variables and Chi-squared test for categorical variables. Unconditional multivariate logistic regression was used to calculate odds ratios (OR) with 95% confidence intervals (95% CI) after adjustment of potential confounders based on a priori knowledge. Patients with missing covariates were not included in the multivariate analyses. Trend tests were conducted by including the quintiles of the dietary pattern factor score as an ordinal variable. We also assessed whether smoking status and GWAS-identified lung cancer susceptibility loci modified the associations between dietary patterns and lung cancer risk. Multiplicative interaction was assessed by the likelihood ratio test. All statistical analyses were performed in Stata 13.0 (StataCorp LP, College Station, Texas). A P value < 0.05 (two-sided) was considered statistically significant.
Additional Information
How to cite this article: Tu, H. et al. Different dietary patterns and reduction of lung cancer risk: A large case-control study in the U.S. Sci. Rep. 6, 26760; doi: 10.1038/srep26760 (2016).
References
American Cancer Society. Cancer Facts & Figures 2015. Available at: http://www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-044552.pdf. (Accessed: 26th April 2016).(2015).
World Cancer Research Fund/American Institute for Cancer Research. Food, Nutrition, Physical Activity and the Prevention of Cancer: a Global Perspective. Available at: http://www.aicr.org/assets/docs/pdf/reports/Second_Expert_Report.pdf. (Accessed: 26th April 2016).(2007).
Hu, F. B. Dietary pattern analysis: a new direction in nutritional epidemiology. Curr Opin Lipidol. 13, 3–9 (2002).
Gorlova, O. Y., Weng, S. F., Hernandez, L., Spitz, M. R. & Forman, M. R. Dietary patterns affect lung cancer risk in never smokers. Nutr Cancer. 63, 842–849 (2011).
Balder, H. F., Goldbohm, R. A. & van den Brandt, P. A. Dietary patterns associated with male lung cancer risk in the Netherlands Cohort Study. Cancer Epidemiol Biomarkers Prev. 14, 483–490 (2005).
De Stefani, E. et al. Nutritional patterns and lung cancer risk in Uruguayan men. Cancer Ther. 4, 153–162 (2006).
De Stefani, E. et al. Nutrient patterns and risk of lung cancer: a factor analysis in Uruguayan men. Lung Cancer. 61, 283–291 (2008).
Gnagnarella, P. et al. Nutrient intake and nutrient patterns and risk of lung cancer among heavy smokers: results from the COSMOS screening study with annual low-dose CT. Eur J Epidemiol. 28, 503–511 (2013).
Couto, E. et al. Mediterranean dietary pattern and cancer risk in the EPIC cohort. Br J Cancer. 104, 1493–1499 (2011).
Anic, G. M., Park, Y., Subar, A. F., Schap, T. E. & Reedy, J. Index-based dietary patterns and risk of lung cancer in the NIH-AARP diet and health study. Eur J Clin Nutr. 70, 123–129 (2016).
Amos, C. I. et al. Genome-wide association scan of tag SNPs identifies a susceptibility locus for lung cancer at 15q25.1. Nat Genet. 40, 616–622 (2008).
McKay, J. D. et al. Lung cancer susceptibility locus at 5p15.33. Nat Genet. 40, 1404–1406 (2008).
Wang, Y. et al. Common 5p15.33 and 6p21.33 variants influence lung cancer risk. Nat Genet. 40, 1407–1409 (2008).
Hung, R. J. et al. A susceptibility locus for lung cancer maps to nicotinic acetylcholine receptor subunit genes on 15q25. Nature. 452, 633–637 (2008).
Thorgeirsson, T. E. et al. A variant associated with nicotine dependence, lung cancer and peripheral arterial disease. Nature. 452, 638–642 (2008).
Wang, Y. et al. Rare variants of large effect in BRCA2 and CHEK2 affect risk of lung cancer. Nat Genet. 46, 736–741 (2014).
Engels, E. A. Inflammation in the development of lung cancer: epidemiological evidence. Expert Rev Anticancer Ther. 8, 605–615 (2008).
Galland, L. Diet and inflammation. Nutr Clin Pract. 25, 634–640 (2010).
Myles, I. A. Fast food fever: reviewing the impacts of the Western diet on immunity. Nutr J. 13, 61 (2014).
Melkonian, S. C. et al. Joint association of genome-wide association study-identified susceptibility loci and dietary patterns in risk of renal cell carcinoma among non-Hispanic whites. Am J Epidemiol. 180, 499–507 (2014).
Messina, M. J. Legumes and soybeans: overview of their nutritional profiles and health effects. Am J Clin Nutr. 70, 439S–450S (1999).
Schabath, M. B., Hernandez, L. M., Wu, X., Pillow, P. C. & Spitz, M. R. Dietary phytoestrogens and lung cancer risk. JAMA. 294, 1493–1504 (2005).
Kaefer, C. M. & Milner, J. A. The role of herbs and spices in cancer prevention. J Nutr Biochem. 19, 347–361 (2008).
Kreuzer, M. et al. Risk factors for lung cancer among nonsmoking women. Int J Cancer. 100, 706–713 (2002).
Mayne, S. T. et al. Dietary beta carotene and lung cancer risk in U.S. nonsmokers. J Natl Cancer Inst. 86, 33–38 (1994).
Brennan, P. et al. A multicenter case-control study of diet and lung cancer among non-smokers. Cancer Causes Control. 11, 49–58 (2000).
Nimptsch, K., Rohrmann, S., Kaaks, R. & Linseisen, J. Dietary vitamin K intake in relation to cancer incidence and mortality: results from the Heidelberg cohort of the European Prospective Investigation into Cancer and Nutrition (EPIC-Heidelberg). Am J Clin Nutr. 91, 1348–1358 (2010).
Pariza, M. W. & Ha, Y. L. Conjugated dienoic derivatives of linoleic acid: mechanism of anticarcinogenic effect. Prog Clin Biol Res. 347, 217–221 (1990).
Mai, V. et al. Diet quality and subsequent cancer incidence and mortality in a prospective cohort of women. Int J Epidemiol. 34, 54–60 (2005).
Harnack, L., Nicodemus, K., Jacobs, D. R. Jr. & Folsom, A. R. An evaluation of the Dietary Guidelines for Americans in relation to cancer occurrence. Am J Clin Nutr. 76, 889–896 (2002).
US. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. Available at: http://www.ncbi.nlm.nih.gov/books/NBK53017/pdf/Bookshelf_NBK53017.pdf. (Accessed: 26th April 2016) (2010).
Varraso, R., Fung, T. T., Hu, F. B., Willett, W. & Camargo, C. A. Prospective study of dietary patterns and chronic obstructive pulmonary disease among US men. Thorax. 62, 786–791 (2007).
Buchner, F. L. et al. Variety in fruit and vegetable consumption and the risk of lung cancer in the European prospective investigation into cancer and nutrition. Cancer Epidemiol Biomarkers Prev. 19, 2278–2286 (2010).
Young, R. P. & Hopkins, R. J. A review of the Hispanic paradox: time to spill the beans? Eur Respir Rev. 23, 439–449 (2014).
Khuder, S. A. Effect of cigarette smoking on major histological types of lung cancer: a meta-analysis. Lung Cancer. 31, 139–148 (2001).
Esmaillzadeh, A. et al. Fruit and vegetable intakes, C-reactive protein and the metabolic syndrome. Am J Clin Nutr. 84, 1489–1497 (2006).
Wannamethee, S. G., Lowe, G. D., Rumley, A., Bruckdorfer, K. R. & Whincup, P. H. Associations of vitamin C status, fruit and vegetable intakes and markers of inflammation and hemostasis. Am J Clin Nutr. 83, 567–574 (2006).
Bosma-den Boer, M. M., van Wetten, M. L. & Pruimboom, L. Chronic inflammatory diseases are stimulated by current lifestyle: how diet, stress levels and medication prevent our body from recovering. Nutr Metab (Lond). 9, 32 (2012).
Manzel, A. et al. Role of “Western diet” in inflammatory autoimmune diseases. Curr Allergy Asthma Rep. 14, 404 (2014).
Thorburn, A. N., Macia, L. & Mackay, C. R. Diet, metabolites and “western-lifestyle” inflammatory diseases. Immunity. 40, 833–842 (2014).
Zhou, B., Liu, J., Wang, Z. M. & Xi, T. C-reactive protein, interleukin 6 and lung cancer risk: a meta-analysis. PLoS One. 7, e43075 (2012).
Hu, M., Lee, M. H., Mak, V. W. & Tomlinson, B. Effect of central obesity, low high-density lipoprotein cholesterol and C-reactive protein polymorphisms on C-reactive protein levels during treatment with Rosuvastatin (10 mg Daily). Am J Cardiol. 106, 1588–1593 (2010).
Crawford, D. C. et al. Genetic variation is associated with C-reactive protein levels in the Third National Health and Nutrition Examination Survey. Circulation. 114, 2458–2465 (2006).
Goldbohm, R. A. et al. Reproducibility of a food frequency questionnaire and stability of dietary habits determined from five annually repeated measurements. Eur J Clin Nutr. 49, 420–429 (1995).
Hu, F. B. et al. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am J Clin Nutr. 69, 243–249 (1999).
Hudmon, K. S. et al. Identifying and recruiting healthy control subjects from a managed care organization: a methodology for molecular epidemiological case-control studies of cancer. Cancer Epidemiol Biomarkers Prev. 6, 565–571 (1997).
Block, G., Coyle, L. M., Hartman, A. M. & Scoppa, S. M. Revision of dietary analysis software for the Health Habits and History Questionnaire. Am J Epidemiol. 139, 1190–1196 (1994).
Block, G. et al. A data-based approach to diet questionnaire design and testing. Am J Epidemiol. 124, 453–469 (1986).
Block, G., Thompson, F. E., Hartman, A. M., Larkin, F. A. & Guire, K. E. Comparison of two dietary questionnaires validated against multiple dietary records collected during a 1-year period. J Am Diet Assoc. 92, 686–693 (1992).
US. Department of Agriculture, Agricultural Research Service. USDA National Nutrient Database for Standard Reference, Release 27. Available at: http://www.ars.usda.gov/Services/docs.htm?docid=25706. (Accessed: 26th April 2016) (2014).
US. Department of Agriculture, Agricultural Research Service, Food Surveys Research Group. USDA Food and Nutrient Database for Dietary Studies, 4.1. Available at: http://www.ars.usda.gov/News/docs.htm?docid=12068. (Accessed: 26th April 2016) (2010).
Patterson, B. H., Block, G., Rosenberger, W. F., Pee, D. & Kahle, L. L. Fruit and vegetables in the American diet: data from the NHANES II survey. Am J Public Health. 80, 1443–1449 (1990).
Diaz, V. A., Mainous, A. G., 3rd, Koopman, R. J., Carek, P. J. & Geesey, M. E. Race and diet in the overweight: association with cardiovascular risk in a nationally representative sample. Nutrition. 21, 718–725 (2005).
Willett, W. & Stampfer, M. J. Total energy intake: implications for epidemiologic analyses. Am J Epidemiol. 124, 17–27 (1986).
Acknowledgements
This work was supported in part by grants from the NIH (P50 CA070907, R01 CA176568) (to X. Wu), Cancer Prevention & Research Institute of Texas (RP130502) (to X. Wu) and The University of Texas MD Anderson Cancer Center institutional support for the Center for Translational and Public Health Genomics.
Author information
Authors and Affiliations
Contributions
X.W. had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: X.W. Acquisition, analysis, or interpretation of data: H.T., J.V.H., C.P.W., Y.Y., J.A.P., J.A.R. and X.W. Drafting of the manuscript: H.T., Y.Y. and X.W. Critical revision of the manuscript for important intellectual content: H.T., J.V.H., C.P.W., Y.Y., J.A.P., J.A.R. and X.W. Statistical analysis: H.T. and Y.Y. Obtained funding: X.W. Study supervision: X.W.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Tu, H., Heymach, J., Wen, CP. et al. Different dietary patterns and reduction of lung cancer risk: A large case-control study in the U.S.. Sci Rep 6, 26760 (2016). https://doi.org/10.1038/srep26760
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep26760
- Springer Nature Limited
This article is cited by
-
Dietary Patterns and Risk of Lung Cancer: A Systematic Review and Meta-Analyses of Observational Studies
Current Nutrition Reports (2023)
-
Dietary quality using four dietary indices and lung cancer risk: the Golestan Cohort Study (GCS)
Cancer Causes & Control (2021)
-
Dietary patterns, BCMO1 polymorphisms, and primary lung cancer risk in a Han Chinese population: a case-control study in Southeast China
BMC Cancer (2018)