
Abstract
Welding fume exposure is associated with heart rate variability (HRV) reduction. It is still unknown whether respirator can reduce effect of welding fume on HRV among welding workers in a shipyard. We recruited 68 welding workers with respirator and 52 welding workers without respirator to measure HRV indices, including standard deviation of normal-to-normal intervals (SDNN) and square root of the mean squared differences of successive intervals (r-MSSD) by ambulatory electrocardiographic (ECG). Personal exposure to particulate matter less than or equal to 2.5 μm in diameter (PM2.5) was measured by a dust monitor. The association between 5-minute mean PM2.5 and log10-transformed HRV indices was analyzed by mixed-effects models. We found 5-minute mean PM2.5 was associated with 8.9% and 10.3% decreases in SDNN and r-MSSD. Effect of PM2.5 on HRV indices was greatest among workers without respirator {SDNN: 12.4% (95% confidence interval = −18.8–−6.9); r-MSSD: 14.7% (95% confidence interval = −20.8–−8.6)}. Workers with respirator showed slight decreases in HRV indices {SDNN: 2.2% (95% confidence interval = −6.3–−1.9); r-MSSD: 4.0% (95% confidence interval = −6.4–−1.6)}. We conclude that respirator use reduces the effect of PM2.5 exposure on HRV among workers performing welding in a shipyard.
Similar content being viewed by others

Introduction
Welding is a fabrication process to join materials, such as metal, by intense heat. Electric welding by electrode is frequently used to improve the assembly of the larger metal pieces in shipyard. Welding fume, a complex mixture of metals, gases and particles, arises from the base metal, especially from electrodes while welding1. Previous studies have reported that welding workers are exposed to welding fumes generated during the welding process2. The majority of welding fume particles is found to be in coarse and fine size ranges by mass concentration3. Compared with coarse particles, fine particles {particulate matter (PM) less than or equal to 2.5 μm in diameter (PM2.5)} is often measured due to its ability to penetrate deep into the alveolar regions of the lung and induce adverse cardiovascular effects (4. Evidence from epidemiological studies suggest that heart rate variability (HRV) can be used as an early disease marker of PM-induced adverse cardiovascular effects5,6,7. Decrease in HRV has been reported to alter the heart’s ability to respond to external signals, leading to myocardial infarction and sudden cardiac death8.
Recent studies have shown that workers exposed to metal fume are associated with HRV changes. Magari et al.9 reported that exposure to high levels of PM2.5 was associated increased standard deviation of normal-to-normal intervals (SDNN) among a cohort of 39 boilermakers9. Cavallari et al.10 found that high concentrations of PM2.5 were associated with decreased night square root of the mean squared differences of successive intervals (r-MSSD) for 26 male boilermaker construction workers 10. Fan et al.11 observed that acute decline of HRV was associated with exposure to welding PM2.5 among 66 welders11. On the other hand, Scharrer et al.12 found no effect of clinical significance of a short-term high-level exposure to welding fumes on time- and frequency-domain parameters of HRV among 20 healthy individuals12. According to these studies, the findings on the association between welding particles and HRV changes are still inconsistent. Moreover, it is still unknown whether respirator can reduce adverse effect of welding fume on HRV.
In order to answer whether occupational exposure to welding fume is associated with impaired cardiac autonomic control and the effectiveness of respirator on protecting workers from welding fume, we recruited a panel of welding workers in Taiwan to clarify these scientific questions.
Results
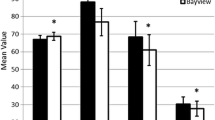
Summarized statistics for 120 participants’ characteristics, heart rate variability monitoring, PM2.5 exposure and climate conditions are presented in Table 1. The study participants were adult workers with a mean age of 51.1 years {standard deviation (SD) = 10.3 years}, 37.5% were current smokers and 56.7% used respirator while working. There were no female workers among our population. No significant different was observed in age, BMI and seniority between workers with and without respirators. For PM2.5, temperature and humidity monitoring, no significant difference was observed in PM2.5 exposure and climate conditions between workers with and without respirators during the study period. For HRV monitoring, the workers with respirators had significantly higher values of HRV indices (Log10 SDNN and Log10 r-MSSD) than did the workers without respirators.
The results of associations between concurrent PM2.5 and HRV indices estimated by the mixed-effects models are shown in Tables 2. With age, BMI, smoking, temperature and relative humidity being adjusted in all mixed-effects models, we found that PM2.5 exposure was associated with HRV changes for welding workers in general. It is noteworthy that PM2.5 exposure significantly decreased HRV indices for workers without respirators. Log10 SDNN decreased by 12.4% per IQR of PM2.5 at 5-minute mean among workers without respirators. No significant association between PM2.5 and Log10 SDNN was observed among workers with respirators. Likewise, r-MSSD decreased by 14.7% per IQR of PM2.5 at 5-minute mean among workers without respirators but only decreased by 4.0% among workers with respirators.
Table 3 shows the results of associations of concurrent PM2.5 with HRV indices estimated by the mixed-effects models stratified by smoking. With age, BMI, temperature and relative humidity being adjusted in all mixed-effects models, we found that PM2.5 exposure was associated with HRV reduction for both smoking and non-smoking workers without respirators. No significant association of PM2.5 with HRV reduction was observed among workers with respirators except Log10 r-MSSD in smoking workers.
We further assessed effect modification in mixed-effects models and found an effect modification of PM2.5 by respirator usage (Table 4). Workers without respirators showed a decrease of 7.4% in Log10 SDNN, which was associated with an increased 5-minute mean PM2.5. In contrast, workers with respirators showed no significant change in Log10 SDNN. Likewise, workers without respirators showed a decrease of 10.2% in Log10 r-MSSD by PM2.5 exposure, but workers with respirators only showed a mild decrease of 3.5% in Log10 r-MSSD.
Discussion
Welding fume has been commonly measured as total dust or inhalable particles in past studies. However, fine particles, which can reach the alveoli, are more specific with regard to cardiopulmonary diseases and systemic particles exposure from welding fume14. Previous studies demonstrate the association of environmental exposure to PM2.5 with decreased HRV in human subjects5,6,7. Recent studies further report the association between occupational exposure to PM2.5, mainly from welding and HRV changes in workers9,10,11,12. The present study confirms that occupational exposure to PM2.5 has comparable magnitudes of effects on decreasing HRV indices in workers. Magari et al.9 showed that SDNN decreased by 1.4% per 1 mg/m3 of concurrent PM2.5 (−0.77 msec) among 39 boilermakers9. Cavallari et al.10 reported that total PM2.5 exposure was associated with decline in night r-MSSD by 18.8% (−0.006 msec/μg/m3) among 26 boilermakers10.
In addition to the PM2.5 effects on HRV indices, the present study shows respirator could modify the association between PM2.5 and HRV. As the results of mixed-effects model with effect modifier showed (Table 3), workers without respirators had higher effects of PM2.5 on HRV reduction compared to those in workers with respirators. This finding is the first one to demonstrate the protective effect of respirator on reducing PM2.5 exposure and cardiovascular adverse effects. Our finding also provides further evidence to support that respirator can be the last resort in controlling welding fume exposure to worker in the aspect of occupational safety and health management system15,16.
The possible pathophysiological mechanism between PM2.5 and autonomic alteration has been well discussed in previous studies. In brief, inhaled PM2.5 may exacerbate the autonomic function of the heart via induced inflammation in lung and proinflammatory cytokine expression in cardiac macrophages17. The time course of PM2.5 on HRV in workers at 5-minute mean is in agreement with the findings of previous studies among workers18, young adults19 and general population20. It has been reported that fine particles can affect both sympathetic and parasympathetic nervous systems immediately. The biological mechanism is PM-induced activation of pulmonary neural reflexes secondary to autonomic alteration after PM inhalation21,22,23.
Several limitations should be addressed in the present study. First, the measurement of PM2.5 might not be representative of welding fume exposure in this study because it was monitored by only personal dust monitor. There might be unmeasured gaseous pollutants that could contribute to the observed HRV reduction. However, if the present findings were driven by gaseous pollutants, there would be no effect modification by respirator status. Therefore, the observed HRV reduction was less likely due to gaseous pollutants as gases travel freely through respirators. Second, the unmeasured meteorological variables, such as wind speed and wind direction, were likely to influence the level of personal PM2.5 exposure24. Such limitation might lead to exposure misclassification and bias the pollution effects on HRV reduction toward null25. Third, we could not exclude the respiration’s confounding effects on the association of personal PM2.5 exposure with HRV reduction because our participants’ physical activities and breathing patterns were not measured in the present study26. Lastly, short-term reduction of HRV has not been associated with higher risk of cardiovascular disease clinically. Cohort study is needed to elucidate the effect of respirator on the relationship between welding fume and cardiovascular health.
Conclusion
The present study found that personal exposure to welding fume was significantly associated with decreased HRV. Such adverse cardiovascular effect was lower among welders with respirators than among welders without respirators. The use of a respirator is therefore beneficial for occupational health management and welder health improvement. Therefore, we encourage employers to provide suitable respirators and adequate training for employees.
Methods
Ethics
The Ethics Committee of the Taipei Medical University-Joint Institutional Review Board approved the study protocol. The methods were carried out in accordance with the approved guidelines. All subjects received written and oral information prior to inclusion and provided informed consent.
Study participants
We recruited 120 healthy male welding workers from a shipyard located in Taiwan as our study participants for this panel study in July and August in 2013 and 2014. The main duty of these welding workers was to weld all types of steel plates of varying sizes and shapes with electric welder. The company was obligated to provide respirators and training courses for all welding workers before they performed arc welding. The type of respirator was disposable activated-carbon facemask. We assigned a well-trained assistant to conduct eight-hour continuous personal PM2.5 exposure monitoring and HRV monitoring for each participant while working (from 09:00 am to 17:00 pm). Each participant’s age, body mass index (BMI), smoking, work history, current health status, respirator usage and work-activity pattern, including sitting, walking, talking, welding, dining, etc. were obtained from a questionnaire by a professionally trained nurse. None of participants had hyperthyroidism, hypoxemia, acute cardiopulmonary failure and paced cardiac rhythm. They were informed of the objective of this study, the benefits and possible danger to health. The ethic committee of the Taipei Medical University Joint Institutional Review Board (Taipei, Taiwan) approved this study (TMU-JIRB No.: 201306041). An informed consent was obtained from each participant before the study embarked and the individuals were allowed to give up at any moment.
HRV monitoring
We performed continuous ambulatory electrocardiographic (ECG) monitoring for each participant while working by using a PacerCorder 3-channel device (model 461A; Del Mar Medical Systems LLC, Irvine, CA, USA) with a sampling rate of 250 Hz (4msec). All ECG tapes were analyzed by using a Delmar Avionics model Strata Scan 563 (Irvine, CA, USA). Each 5-minute segment of normal-to-normal (NN) intervals was taken for HRV analysis. The time domain measurements of HRV were SDNN and r-MSSD. Each participant obtained approximately 12 successful segments of 5-minute HRV measurements per hour for data analysis.
Personal PM2.5 exposure monitoring
We conducted continuous monitoring of PM2.5 and meteorological conditions for each participant while working. PM2.5, temperature and relative humidity were measured continuously by a personal dust monitor (DUSTcheck Portable Dust Monitor, model 1.108; temperature and humidity sensor, model 1.153FH; Grimm Labortechnik Ltd., Ainring, Germany), which measured and recorded 1-min mass concentrations of PM2.5 as well as temperature and relative humidity in the breathing zone. After monitoring, the raw data for 1-min PM2.5, temperature and relative humidity were matched with the monitoring time of HRV for data analysis.
Statistical analysis
We applied mixed-effects models to examine the association of PM2.5 with SDNN and r-MSSD for our study participants by running R statistical software version 2.15.1. The SDNN and r-MSSD were log10-transformed to improve normality and stabilize the variance. We treated each participant’s age, BMI, smoking (Yes vs. No), respirator usage as time-invariant variables, while 5-minute mean PM2.5, 5-minute mean temperature, 5-minute mean relative humidity, log10 SDNN and log10 r-MSSD as time-varying variables in our data analysis. The outcome variables were log10 SDNN and log10 r-MSSD and the exposure variables were 5-minute mean PM2.5. We treated each participant as a random effect in our mixed-effects models. In further analyses, we investigated if PM2.5 effects differed among smokers and non-smokers using mixed-effects models stratified by smoking.
Effect modification by respirators usage (Yes vs. No) was assessed in a separate mixed model by including interaction terms between PM2.5 exposure and respirators usage among all workers. Minimizing Akaike’s Information Criterion (AIC)13 was used as the criteria of model selection. The pollution effects are expressed as percent changes in HRV by an interquartile range (IQR) change in pollution levels for PM2.5.
Additional Information
How to cite this article: Han, B.-C. et al. Effect of welding fume on heart rate variability among workers with respirators in a shipyard. Sci. Rep. 6, 34158; doi: 10.1038/srep34158 (2016).
References
Berlinger, B. et al. Physicochemical characterisation of different welding aerosols. Anal. Bioanal. Chem. 399, 1773–1780 (2011).
Taube, F. Manganese in occupational arc welding fumes-aspects on physiochemical properties, with focus on solubility. Ann. Occup. Hyg. 57, 6–25 (2013).
Chang, C. et al. Physicochemical and toxicological characteristics of welding fume derived particles generated from real time welding processes. Environ. Sci. Process. Impacts. 15, 214–224 (2013).
Adar. S. D. & Kaufman, J. D. Cardiovascular disease and air pollutants: evaluating and improving epidemiological data implicating traffic exposure. Inhal. Toxicol. 19 Suppl 1, 135–149 (2007).
Gold, D. R. et al. Ambient pollution and heart rate variability. Circulation 101, 1267–1273 (2000).
Pope, 3rd, C. A. et al. Cardiovascular mortality and long-term exposure to particulate air pollution: epidemiological evidence of general pathophysiological pathways of disease. Circulation 109, 71–77 (2004).
Chuang, K. J. et al. The effect of urban air pollution on inflammation, oxidative stress, coagulation and autonomic dysfunction in young adults. Am. J. Respir. Crit. Care. Med. 176, 370–376 (2007).
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: standards of measurement, physiological interpretation and clinical use. Circulation 93, 1043–1065 (1996).
Magari, S. R. et al. The association of particulate air metal concentrations with heart rate variability. Environ. Health. Perspect. 110, 875–880 (2002).
Cavallari, J. M. et al. PM2.5 metal exposures and nocturnal heart rate variability: a panel study of boilermaker construction workers. Environ. Health. 7, 36 (2008).
Fan, T. et al. Heart rate variability and DNA methylation levels are altered after short-term metal fume exposure among occupational welders: a repeated-measures panel study. BMC Public Health 14, 1279 (2014).
Scharrer, E. et al. Heart rate variability, hemostatic and acute inflammatory blood parameters in healthy adults after short-term exposure to welding fume. Int. Arch. Occup. Environ. Health. 80, 265–272 (2007).
Akaike, H. A new look at the statistical model identification. IEEE. Trans. Auto. Control. 19, 716–723 (1974).
Hobson, A. et al. Estimation of particulate mass and manganese exposure levels among welders. Ann. Occup. Hyg. 55, 113–125 (2011).
Myers, W. R., Zhuang, Z. & Nelson, T. Field performance measurements of half-facepiece respirators–foundry operations. Am. Ind. Hyg. Assoc. J. 57, 166–174 (1996).
Aiba, Y. et al. [A survey on the use of respirators among dust workers in outdoor working environments]. Sangyo Eiseigaku Zasshi 56, 268–274 (2014).
Magari, S. R. et al. Association of heart rate variability with occupational and environmental exposure to particulate air pollution. Circulation 104, 986–991 (2001).
Liu, W. T. et al. Effects of commuting mode on air pollution exposure and cardiovascular health among young adults in Taipei, Taiwan. Int. J. Hyg. Envir. Heal. 218, 319–323 (2015).
Lin, L. Y. et al. Reducing indoor air pollution by air conditioning is associated with improvements in cardiovascular health among the general population. Sci. Total. Environ. 463–464, 176–181 (2013).
Stone, P. H. & Godleski, J. J. First steps toward understanding the pathophysiologic link between air pollution and cardiac mortality. Am. Heart. J. 138, 804–807 (1999).
Lai, C. J. & Kou, Y. R. Stimulation of vagal pulmonary C-fibers by inhaled wood smoke in rats. J. Appl. Physiol. 84, 30–36 (1998).
Kodavanti, U. P. et al. The spontaneously hypertensive rat as a model of human cardiovascular disease: evidence of exacerbated cardiopulmonary injury and oxidative stress from inhaled emission particulate matter. Toxicol. Appl. Pharmacol. 164, 250–263 (2000).
Nemmar, A. et al. Passage of inhaled particles into the blood circulation in humans. Circulation 105, 411–414 (2002).
Schwartz, J. et al. Traffic related pollution and heart rate variability in a panel of elderly subjects. Thorax 60, 455–461 (2005).
Zeka, A. & Schwartz, J. Estimating the independent effects of multiple pollutants in the presence of measurement error: an application of a measurement-error resistant technique. Environ. Health. Perspect. 112, 1686–1690 (2004).
Yasuma, F. & Hayano, J. Respiratory sinus arrhythmia: why does the heartbeat synchronize with respiratory rhythm? Chest 125, 683–690 (2004).
Acknowledgements
This study was supported by grants from the Institute of Labor, Occupational Safety and Health, Ministry of Labor of Taiwan (IOSH102-M321 and ILOSH103-A321) and the Ministry of Science and Technology of Taiwan (MOST 104-2621-M-038-001-MY2). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
B.-C.H., I.-J.L., H.–C.C., C.-H.P. performed air sampling and heart rate variability monitoring and wrote the manuscript. K.-J.C., designed research, performed air sampling, analyzed data and wrote the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Han, BC., Liu, IJ., Chuang, HC. et al. Effect of welding fume on heart rate variability among workers with respirators in a shipyard. Sci Rep 6, 34158 (2016). https://doi.org/10.1038/srep34158
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep34158
- Springer Nature Limited