
Abstract
Background
Little is known about clinicians' use of herbs and dietary supplements (HDS), how their personal HDS use changes with time and training, and how changes in their personal use affect their confidence or communication with patients about HDS.
Methods
We conducted a prospective cohort study of clinicians before and after an on-line curriculum about HDS in winter-spring, 2005.
Results
Of the 569 clinicians who completed surveys both at baseline and after the course, 25% were male and the average age was 42 years old; 88% used HDS before and after the course. The average number of supplements used fell slightly from 6.2 at baseline to 5.8 after the course (P < 0.01). The most commonly used supplements at baseline were: multivitamins (65%), calcium (42%), B vitamins (34%), vitamin C (34%), green tea (27%), fish oil (27%) and vitamin E (25%). Use of fish oil increased to 30% after the course (P = 0.01). Use of supplements traditionally used to treat colds decreased: vitamin C (34% to 27%), zinc (13% to 10%), and echinacea (7% to 5%, P < 0.05 for all three). Changes in personal HDS use were not associated with significant changes in confidence or communication with patients.
Conclusion
Many clinicians use HDS personally; use changes seasonally and to a small extent with professional education. Professional use of HDS is dynamic and seasonal. Additional research is needed to understand the impact of personal use on professional attitudes and behavior in populations with lower baseline uses of HDS.
Similar content being viewed by others


Background
Herbs and other dietary supplements (HDS) such as vitamins and minerals are among the most commonly used complementary therapies in the US [1–5]. Substantial numbers of all patient groups report using HDS, particularly those with chronic or recurrent illnesses. Rates of use have been shown to vary by demographic characteristics. For example, compared with men, women report higher use of HDS [6–9]. Among health care professionals (clinicians), HDS use tends to mirror patterns reported by the general public [10–16].
Clinicians' personal use of dietary supplements is of interest for at least two reasons[15]. Patients ask clinicians to provide advice about them. In fact, the labels on dietary supplement products frequently suggest that consumers ask clinicians for advice about using such products. Furthermore, clinicians' personal health habits may affect their professional behavior[3].
We previously reported a study comparing four different strategies for delivering on-line curriculum about HDS. All four delivery strategies were associated with similar, significant and sustained improvements in participants' knowledge, confidence and communication practices both immediately after and six to ten months after completing the course[17]. The on-line course included 40 self-instructional modules covering scientific evidence of risks, safety, and effectiveness of over 100 commonly used HDS; the modules were organized into ten topic areas covering common clinical questions and situations such as safety, women's health, aging, pediatrics, cardiology, pulmonary and gastrointestinal problems. Each module included links to additional sources of evidence-based clinical information.
We wondered whether completing the on-line curriculum (geared toward helping clinicians learn to answer patients' questions about HDS) might also affect clinicians' personal use of HDS because clinicians may also be interested in improving their own health or addressing their own health problems as well as those of patients. We expected that use of some HDS would be relatively stable over time (e.g. use of multivitamins, calcium and folate), while others would change seasonally (e.g., use of vitamin C, echinacea and zinc used to prevent or treat the common cold would decrease as cold/flu season ended) and some might change as a result of information provided during the course. Furthermore, we were curious about the relationship between changes in personal use of HDS and changes in communication practices.
Methods
To answer these questions, we prospectively compared participants' baseline (January) surveys with their responses to follow-up surveys completed within a month after course completion in spring (April – May), 2005. Subjects were eligible if they were participants enrolled in a randomized controlled trial evaluating different strategies for delivering an on-line curriculum about HDS. The eligibility criteria, recruitment strategies, curriculum content, and delivery strategies have been described previously [17–19] as have analyses of participants' personal use of HDS at baseline [16].
Briefly, participants were eligible if they were physicians, nurses, dietitians, pharmacists or trainees in one of these professions. They were recruited through email, a web site, flyers and mailings from the North Carolina Northwest Area Health Education Center (NW AHEC). Enrollment and follow-up surveys were completed on-line.
The surveys were based on our earlier pilot study evaluating the effects of an email-based curriculum about HDS [20]. They included questions about demographic and practice characteristics, personal use in the previous week of a list of 15 vitamins and minerals, 59 herbs and 12 other dietary supplements. The survey also included questions to assess participants' knowledge, confidence and communication practices about commonly used HDS [18] [see Additional file 1]; the confidence and communication scales had Cronbach alpha > 0.7. The same questions were used for both the baseline and follow-up surveys.
This analysis was restricted to participants from the winter-spring 2005 semester to assess seasonal impact on HDS use. For purposes of this study, we defined as "seasonal supplements": vitamin C, echinacea, zinc, astragalus, slippery elm bark, chamomile, elderberry, ginger, goldenseal, licorice, medicinal mushrooms and peppermint.
Analysis included simple descriptive statistics such as mean and standard deviation for normally distributed data; and medians and ranges for non-normally distributed data. We used Chi square methods to assess associations for categorical variables. Spearman correlation was used to assess associations for continuous variables. Mann-Whitney and Kruskal-Wallis tests were used to assess between group differences. Wilcoxon signed rank and McNemar tests were used to assess repeated measures for continuous and binomial measures, respectively.
All analyses were performed using SPSS 14.0 (SPSS, Inc., Chicago, IL).
This study was approved as "exempt" as an educational research project by the Wake Forest University School of Medicine Institutional Review Board.
Results
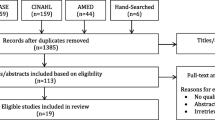
Of the 1268 course participants, 569 were spring enrollees who completed baseline and follow-up questionnaires (Table 1). At baseline the participants' average age was 40.3 ± 12.9 years and 25% percent were men. At baseline, 88% of enrollees used at least one dietary supplement and the average number used was 6.2. Table 2 lists the most commonly used HDS which included: multivitamins, calcium, B vitamins, vitamin C, green tea, and fish oil. Higher baseline use of HDS was associated with older age, female gender, professional group (highest in nurses and lowest in students and pharmacists), and higher scores on knowledge questions, the confidence scale and the communication practices scale [15].
Overall, there was little change in the use of HDS from before to after the course. After the course, 88% of enrollees still reported using at least one dietary supplement; the average number of supplements used fell slightly from 6.2 to 5.8 (P < 0.01). As expected, there were significant decreases in the use of seasonal HDS (Table 3). For example, use of vitamin C fell from 34% to 27% (P = 0.001). Overall, the average number of seasonal HDS products used fell more than 20% from baseline to after the course (P < 0.001), while the average number of non-seasonal products used fell less than 5% (P = 0.08). There were unexpectedly significant changes in the use of three non-seasonal HDS: an increase in the use of fish oil from 27% to 30% (P = 0.04) and declines in the use of vitamin E (25% to 20%, P = 0.002) and iron (10% to 6%, P = 0.005). Exploratory statistical analyses did not reveal any pattern of associations between use of fish oil, iron or vitamin E and demographic or practice characteristics.
Higher use of HDS at baseline was associated with higher scores on knowledge, confidence and communication practices scales and significantly greater improvements in knowledge and confidence after the course. However, there were no significant associations between changes in HDS use and improvements in knowledge, confidence or communication practices from before to after the course. Trainees reported a greater decrease in use of HDS than did practitioners (P = 0.02), but there were no significant associations between changes in HDS use and other baseline characteristics.
Discussion
This is the first study to examine changes in professionals' use of HDS over time, the impact of these changes associated with changes in professional behavior, and the impact of an on-line professional curriculum and seasonal changes on clinicians' personal use of these products. Generally, we found little change in HDS use over time except for the expected decrease in the use of seasonal cold/flu products. Unexpected changes included a significant increase in the use of fish oil (which was discussed in several modules as potentially helpful) and decreases in the use of iron and vitamin E (which were mentioned in modules, but not heavily emphasized).
Overall, the clinicians in this study used more HDS than the general public [1, 2, 21]. Although the self-selected participants in this study had higher usage rates, their patterns of use, i.e., the most popular supplements, were generally similar to those used by the general public. For example, in both these participants and the general public, multivitamins are the most commonly used supplements. On the other hand, our participants reported lower usage of supplements traditionally used to treat colds and flu (e.g. vitamin C, echinacea and zinc) than the general public. The lower use in our study may be due to the healthy worker effect [22]; on the other hand, we did not collect personal health information, and it is possible that the participants in this study had higher rates of chronic conditions that led to their greater use of HDS than that reported among the general public. Perhaps due to recent positive trials about the benefits of fish oil for a variety of health conditions, reported use of fish oil among our participants was higher than that previously reported among the general public[1, 2, 21]. Likewise, the decreasing use of vitamin E over time among our enrollees may have been due to course coverage of recent randomized trials casting doubt on its effectiveness in preventing heart disease as had been claimed in earlier epidemiologic studies.
This study has several limitations. First, we enrolled a highly self-selected sample of clinicians who were very high users of HDS before starting the course; results from this sample may not be generalizable to other groups of clinicians. Second, we did not collect personal health data or reasons for using HDS; this makes it difficult to speculate on reasons for changes in use beyond the obvious seasonal changes. Furthermore, we had no control over secular changes in information about HDS which might have influenced personal use; for example, during the study period, participants may have been exposed to articles in professional journals or the popular media about vitamin E, fish oil and seasonal remedies such as echinacea. Also, the curriculum provided information on more than 100 HDS; individual participants may have increased or decreased their personal use of individual supplements in significant ways not captured by the aggregate data. Given these limitations, we cannot speculate on the effect of the content of the curriculum on individual clinician's use of specific supplements. For example, we cannot tell whether increases in the use of fish oil or decreases in the use of vitamin E and iron are related to curriculum content, personal health factors, secular changes in supplement use, or simply artifacts related to testing changes in multiple supplements.
Conclusion
Although higher use of HDS is associated with greater knowledge and confidence in talking with patients about HDS, small seasonal changes in personal use of HDS do not appear to affect clinical behavior. Use of HDS is dynamic; use of some supplements varies seasonally and may be affected by numerous factors. Prevalence studies alone are insufficient to understand important facets of HDS use. Prospective cohort studies that include data on health conditions and use of over the counter and prescription medications are needed to better understand the scope and effects of HDS use among clinicians as well as patients.
References
Barnes PM, Powell-Griner E, McFann K, Nahin RL: Complementary and alternative medicine use among adults: United States, 2002. Adv Data. 2004, 1-19.
Ni H, Simile C, Hardy AM: Utilization of complementary and alternative medicine by United States adults: results from the 1999 national health interview survey. Med Care. 2002, 40 (4): 353-358. 10.1097/00005650-200204000-00011.
Fennell D: Determinants of supplement usage. Prev Med. 2004, 39 (5): 932-939. 10.1016/j.ypmed.2004.03.031.
Tindle HA, Davis RB, Phillips RS, Eisenberg DM: Trends in use of complementary and alternative medicine by US adults: 1997-2002. Altern Ther Health Med. 2005, 11 (1): 42-49.
Graham RE, Ahn AC, Davis RB, O'Connor BB, Eisenberg DM, Phillips RS: Use of complementary and alternative medical therapies among racial and ethnic minority adults: results from the 2002 National Health Interview Survey. J Natl Med Assoc. 2005, 97 (4): 535-545.
MacKichan C, Ruthman J: Herbal product use and perioperative patients. Aorn J. 2004, 79 (5): 948-59; quiz 960-1, 963-4. 10.1016/S0001-2092(06)60726-6.
Ball SD, Kertesz D, Moyer-Mileur LJ: Dietary supplement use is prevalent among children with a chronic illness. J Am Diet Assoc. 2005, 105 (1): 78-84. 10.1016/j.jada.2004.10.008.
Mahady GB, Parrot J, Lee C, Yun GS, Dan A: Botanical dietary supplement use in peri- and postmenopausal women. Menopause. 2003, 10 (1): 65-72.
Mackenzie ER, Taylor L, Bloom BS, Hufford DJ, Johnson JC: Ethnic minority use of complementary and alternative medicine (CAM): a national probability survey of CAM utilizers. Altern Ther Health Med. 2003, 9 (4): 50-56.
Ayuk-Egbe PW: A Survey of nurses' knowledge and attitudes regarding herbal therapies. National Academies of Practice Forum: Issues in Interdisciplinary Care (NAPF). 2000, 2 (3): 191-194 (17 ref).
Lindquist R, Tracy MF, Savik K: Personal use of complementary and alternative therapies by critical care nurses. Crit Care Nurs Clin North Am. 2003, 15 (3): 393-9, x. 10.1016/S0899-5885(02)00104-1.
Berman BM, Singh BK, Lao L, Singh BB, Ferentz KS, Hartnoll SM: Physicians' attitudes toward complementary or alternative medicine: a regional survey. J Am Board Fam Pract. 1995, 8 (5): 361-366.
Cashman LS, Burns JT, Otieno IM, Fung T: Massachusetts registered dietitians' knowledge, attitudes, opinions, personal use, and recommendations to clients about herbal supplements. J Altern Complement Med. 2003, 9 (5): 735-746. 10.1089/107555303322524580.
Steyn NP, Labadarios D, Nel JH, Heidi-Lee R: Development and validation of a questionnaire to test knowledge and practices of dietitians regarding dietary supplements. Nutrition. 2005, 21 (1): 51-58. 10.1016/j.nut.2004.09.008.
Gardiner P: Dietary Supplement Use Among Health Care Professionals enrolled in an Online Curriculum on Herbs and Dietary Supplements. BMC Complement Altern Med. 2006, 6: 21-10.1186/1472-6882-6-21.
Gardiner PL: Herb Use Among Health Care Professionals enrolled in an Online Curriculum on Herbs and Dietary Supplements. Journal of Herbal Pharmacotherapy. 2006, 6 (2): 51-64. 10.1300/J157v06n02_05.
Kemper KJ, Gardiner P, Gobble J, Mitra A, Woods C: Randomized Controlled Trial Comparing Four Strategies for Delivering e-Curriculum to Health Care Professionals [ISRCTN88148532]. BMC Med Educ. 2006, 6 (1): 2-10.1186/1472-6920-6-2.
Kemper KJ, Gardiner P, Gobble J, Woods C: Expertise about herbs and dietary supplements among diverse health professionals. BMC Complement Altern Med. 2006, 6 (1): 15-10.1186/1472-6882-6-15.
Beal T, Kemper KJ, Gardiner P, Woods C: Long-term impact of four different strategies for delivering an on-line curriculum about herbs and dietary supplements. BMC Med Educ. 2006, 6 (1): 39-10.1186/1472-6920-6-39.
Kemper KJ, Amata-Kynvi A, Sanghavi D, Whelan JS, Dvorkin L, Woolf A, Samuels RC, Hibberd P: Randomized trial of an internet curriculum on herbs and other dietary supplements for health care professionals. Acad Med. 2002, 77 (9): 882-889. 10.1097/00001888-200209000-00014.
Kaufman DW, Kelly JP, Rosenberg L, Anderson TE, Mitchell AA: Recent patterns of medication use in the ambulatory adult population of the United States: the Slone survey. JAMA. 2002, 287 (3): 337-344. 10.1001/jama.287.3.337.
Punnett L: Adjusting for the healthy worker selection effect in cross-sectional studies. Int J Epidemiol. 1996, 25 (5): 1068-1076. 10.1093/ije/25.5.1068.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1472-6882/7/21/prepub
Acknowledgements
Dr. Gardiner is supported by an NIH Institutional National Research Service Award, Grant No. T32-AT0051-03 from the National Center for Complementary and Alternative Medicine (NCCAM) Dr. Kemper was supported by NIH R01 LM007709 and the Fullerton Foundation in Gaffney, SC for this project. The views expressed in this manuscript are those of the authors and not necessarily those of any agency involved in funding it.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
KK conceived the project, wrote the initial drafts of the manuscript and revised the manuscript
PG assisted in developing the idea of the project, developing the study intervention, defined key parameters and assisted in drafting and revising the manuscript
CW assisted in designing the project, analyzing study data and revising the manuscript
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Kemper, K.J., Gardiner, P. & Woods, C. Changes in use of herbs and dietary supplements (HDS) among clinicians enrolled in an online curriculum. BMC Complement Altern Med 7, 21 (2007). https://doi.org/10.1186/1472-6882-7-21
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1472-6882-7-21