
Abstract
Background
It is well known that the prevalence of overweight and obesity is considerably higher among youth from lower socio-economic families, but there is little information about the role of some energy balance-related behaviors in the association between socio-economic status and childhood overweight and obesity. The objective of this paper was to assess the possible mediation role of energy balance-related behaviors in the association between parental education and children’s body composition.
Methods
Data were obtained from the cross sectional study of the “EuropeaN Energy balance Research to prevent excessive weight Gain among Youth” (ENERGY) project. 2121 boys and 2516 girls aged 10 to 12 from Belgium, Greece, Hungary, the Netherlands, Norway, Slovenia and Spain were included in the analyses. Data were obtained via questionnaires assessing obesity related dietary, physical activity and sedentary behaviors and basic anthropometric objectively measured indicators (weight, height, waist circumference). The possible mediating effect of sugared drinks intake, breakfast consumption, active transportation to school, sports participation, TV viewing, computer use and sleep duration in the association between parental education and children’s body composition was explored via MacKinnon’s product-of-coefficients test in single and multiple mediation models. Two different body composition indicators were included in the models, namely Body Mass Index and waist circumference.
Results
The association between parental education and children’s body composition was partially mediated by breakfast consumption, sports participation, TV viewing and computer use. Additionally, a suppression effect was found for sugared drinks intake. No mediation effect was found for active transportation and sleep duration. The significant mediators explained a higher proportion of the association between parental education and waist circumference compared to the association between parental education and BMI.
Conclusions
Tailored overweight and obesity prevention strategies in low SES preadolescent populations should incorporate specific messages focusing on the importance of encouraging daily breakfast consumption, increasing sports participation and decreasing TV viewing and computer use. However, longitudinal research to support these findings is needed.
Similar content being viewed by others


Background
Overweight and obesity are important determinants of avoidable burden of disease [1]. Despite a leveling-off of obesity prevalence in some countries in the last years, childhood obesity still shows a high prevalence [2]. Recent cross-European data from the ENERGY project confirmed these high prevalence rates of overweight and obesity among schoolchildren [3]. It is also known that overweight and obesity track from childhood to adulthood [4, 5]. Recent research and literature reviews show that, among schoolchildren, some specific energy balance-related behaviors (EBRBs) are associated with overweight and obesity prevalence and may be important for obesity prevention [6–9]. These behaviors comprise, among others, the intake of sugared drinks, skipping breakfast, screen viewing behavior (TV viewing and sedentary computer activities) and lack of regular physical activity, like active commuting to school, participation in sports and recreational physical activity. In addition, recent evidence suggests that sleeping habits may also be relevant for energy balance [10, 11]. Despite the associations with overweight, many schoolchildren engage in these risk behaviors [3]. It is also well known that the prevalence of overweight and obesity is considerably higher among youth from lower socio-economic families [12–16].
There is little information about the role of those EBRBs in the association between indicators of socio-economic status and childhood overweight and obesity. Morgenstern et al. [17] have recently shown that the effect of socioeconomic status (SES) on overweight was partially mediated by media exposure in children and adolescents aged 10 to 17. Previous studies found that some behavioral factors (e.g. screen time, physical activity and dietary habits) may partially explain the association between SES and excess overweight prevalence, but did not include formal tests of mediation [17–19].
In the ENERGY cohort overweight and obesity were also more prevalent among children from parents with lower levels of education [3]. Moreover, the ENERGY project included data on the most important EBRBs. Therefore, the aim of this paper was to assess the possible mediation role of EBRBs in the association between parental education and children’s body composition. More specifically, the current study aims to assess: 1) the total associations of parental education with two different body composition outcomes: Body Mass Index (BMI) and waist circumference; 2) the associations of parental education with EBRBs (i.e. sugared drinks intake, breakfast consumption, active transportation to school, sports participation, TV viewing, computer use and usual sleep duration) as potential mediating variables; and 3) to assess the mediated pathways of EBRBs on BMI and waist circumference.
Methods
Study population and design
Data were obtained from the cross sectional study of the “EuropeaN Energy balance Research to prevent excessive weight Gain among Youth” (ENERGY) project [20]. This cross-sectional study was carried out between March and July 2010 in Belgium, Greece, Hungary, the Netherlands, Norway, Slovenia and Spain, among pupils in the final years of primary education (aged 10–12) [21]. The aim of the survey was to provide up to date information on the prevalence of overweight and obesity, on the most important energy balance related behaviors (EBRBs) and their social, cognitive and school environmental determinants. Based on previous cross-European studies [22], a minimum sample of 1000 schoolchildren per country and one parent/caretaker for each child were aimed for. The schools were randomly selected concerning the degree of urbanization of the different provinces and the socioeconomic status (SES) of the different areas within the selected provinces. Samples were national in Greece, Hungary, the Netherlands and Slovenia. In Spain, schools of the region of Aragón were selected; Belgium selected schools from Flanders and Norway selected schools from the southern regions of the country [21]. Descriptions of the rationale and design of the entire ENERGY project [20] and the procedures and methodology of the ENERGY school-based survey [21] are published elsewhere. All participants provided written informed consent prior their enrollment. The studies were approved by the corresponding local ethics committees in all participating countries. In Belgium the survey was approved by the Medical Ethics Committee of the University Hospital Ghent; In Greece the survey was approved by the Bioethics Committee of Harokopio University; In Hungary the survey was approved by the Scientific and Ethics Committee of Health Sciences Council; in the Netherlands the survey was approved by the Medical Ethics Committee of the VU University Medical Center; in Norway the survey was approved by the National Committees for Research Ethics in Norway; in Slovenia the survey was approved by the National Medical Ethics Committee of the Republic of Slovenia; and in Spain the survey was approved by Clinical Research Ethics Committee of the Government of Aragon. The project adhered to the Helsinki Declaration and the conventions of the Council of Europe on human rights and biomedicine.
Measures
Measurements were conducted following standardized protocols. The children and the parents were asked to complete printed questionnaires assessing obesity related dietary, physical activity and sedentary behaviors, as well as potential determinants of engaging in these behaviors. The questionnaires and anthropometric measurements were completed during school hours. Test-retest reliability was tested by administrating the questionnaire twice with a one-week interval among 720 schoolchildren across the participating countries. In the paragraphs hereafter information on the intraclass correlation coefficients (ICC) is provided for the specific included items. Detailed information regarding the procedures, staff training and questionnaires development [21], and test-retest reliability and construct validity of the questionnaires are published elsewhere [23, 24].
Anthropometric measurements
Body height, weight and waist circumference were measured by trained research assistants. Children were measured in light clothing without shoes. Body height was measured with a SECA Leicester Portable stadiometer (to the nearest 0.1 cm). Weight was measured with a calibrated electronic scale SECA 861 (to the nearest 0.1 kg), and waist circumference with a SECA 201 measuring band (to the nearest 0.1 cm). Two readings of each measurement were obtained. A third measurement was taken if the two readings differed more than 1%. Body Mass Index (BMI) and weight categories based on the International Obesity Task Force criteria (IOTF) [25] were calculated.
Parental educational level
As an indicator of socio-economic status, the parent respondents were asked to report their own level of education, as well as the level of education of the other parent/caregiver. Because educational systems differ considerably across Europe, years of formal education since preschool were used as the indicator for level of education. Answer categories were as follows: a) less than 7 years, b) 7–9 years, c) 10–11 years, d) 12–13 years and e) 14 years or more. After preliminary analyses of the distribution of the variable, it was concluded that to recode into low, medium and high parental education level was not possible due to the small sample size in the low category. Thus, parental education was categorized as being high (at least one parent more than 14 years of education) or low (both parents less than 14 years of education), which approximately distinguishes families with at least one caregiver who has completed medium or higher vocational, college or university training from other families.
Children’s energy balance-related behaviors
Sugared drinks consumption, breakfast consumption, active transportation, sports participation, TV viewing and computer use were reported by the children, while sleep duration was reported by the parents.
Dietary behaviors
Intakes of soft drinks and fruit juices were assessed with two food frequency questions. Children answered how many days per week they drank the beverage, answering on a seven-point scale from never to more than once every day. Afterwards they were asked to indicate how much they drank by ticking the number of glasses or small bottles (e.g. 250 ml), cans (i.e. 330 ml) and large bottles (i.e. 500 ml) for soft drinks, or glasses/small cartons (i.e. 250 ml) and regular cartons (330 ml) for fruit juices. The questionnaire included pictures of the serving sizes. These items showed moderate to good reliability (intraclass correlation coefficients (ICCtest-retest) between 0.53 – 0.71). Mean intake in ml per day was calculated from these two questions. In addition, children were asked to fill in how much of the beverages they had consumed on the day before, following the same classification. For the purposes of this analysis, liters/day of sugared drinks (soft drinks + fruit juices) were taken into account. Breakfast consumption was assessed with two food frequency questions. Children answered how many days they usually eat breakfast during school days (ICCtest-retest = 0.73) and in the weekend (ICCtest-retest = 0.52). For the purposes of this analysis, total weekly days having breakfast were taken into account.
Physical activity behaviors
Active transportation to school was assessed by two questions about how many days per week the child cycled and/or walked to school (ICCtest-retest = 0.94 and 0.91), ranging from never to 5 days/week, and two questions on the duration of biking or walking to school, with 4 answer categories ranging from 1–5 minutes to more than 15 minutes (ICCtest-retest = 0.81 and 0.70). Total active transportation time per week was calculated by adding up total bike and walk times and multiplying the number of days with the mean time of the answering category times 2. Organized sports participation was assessed with specific questions about how many hours per week children participated in one or two sports (ICCtest-retest = 0.74 and 1.00). Based on the answers, average time of sports participation per week was calculated. Finally, minutes/week of active transportation and hours/week of sports participation were included in the analysis.
Sedentary behaviors
Screen time (i.e. TV and computer time) was assessed separately for weekdays and weekend days by two questions about time spent watching TV (including video and DVD) (ICCtest-retest = 0.67 and 0.68) and computer activities (ICCtest-retest = 0.67 and 0.67). Mean TV, computer and total screen time per day were calculated. For the analysis, total hours/week of TV viewing and total hours/week of computer use were taken into account.
Sleep duration
Child’s sleep duration reported by the parents included the number of hours the child sleeps per night on average, separately for weekdays (ICCtest-retest = 0.81) and weekend days (ICCtest-retest = 0.78). For the purpose of this paper, only weekdays (hours/day of sleep duration) were taken into account as sleep during weekdays is likely to be more representative of usual sleep duration, due to the more regular bed- and get-up routine [11].
Statistical analysis
Means and standard deviations were calculated for the key variables, separately for boys and girls. A complete cases design was used; therefore only children having valid data for the variables included in the analysis were taken into account. Children not included in the final analysis had slightly lower BMI and were slightly older compared to the included sample (data not shown). Multilevel analysis intraclass correlation coefficients (ICCs) were calculated, in order to check whether a school level clustered design was needed. The obtained school ICCs were low (all <0.06), reflecting no clustering effect at school level. Therefore, the analyses were adjusted only for country level.
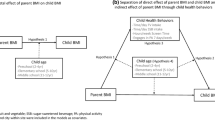
Mediation analysis: To assess whether the associations between parental education and body composition outcomes were mediated by the EBRBs, the product-of-coefficients test proposed by MacKinnon was performed [26]. To qualify as a mediator, the presumed mediator has to be associated with the predictor variable and with the outcome variable [27]. To define the final regression models, the included EBRBs, as the presumed mediators, had to fulfill two requirements: (1) the parental education indicator (X) has to be associated with the mediator (M) (path a); and (2) the mediator has to be associated with the body composition outcome (Y) in a regression model adjusted for the predicting variable (X) (path b) (see Figure 1). The potential mediators meeting these criteria were included in the final multiple mediator models and mediation effects and mediated proportions were calculated. The product-of-coefficients method (ai*bi) was used to calculate the mediated effect. The total mediated effect was calculated as the sum of the individual mediated effects (Σ[ai*bi]). The mediated proportions were calculated as the mediation effect divided by the total effect (path c) ([ai*bi]/c) and (Σ[ai*bi]/c). Total effects were estimated by regression models without the potential mediators. Standard errors were calculated and used to construct the 95% confidence intervals (CI) for the direct and total effects. Bootstrap corrected CI were used for indirect, mediated, effects by means of the SPSS macro developed by Preacher and Hayes [28].

Multiple mediator model. X: predictor variable; Y: outcome variable; Mi: mediator variable; ai: association between predictor (X) and potential mediator (Mi); bi: association between potential mediator (Mi) and outcome variable (Y); c: overall association between predictor variable (X) and outcome variable (Y); c’: direct effect (unmediated) of predictor variable (X) on outcome variable (Y).
All regression models were adjusted for potential confounders (gender, age, country). Additionally, a potential effect modification of the total association by gender was assessed using an interaction term (gender*parental education). In case of significant interaction term, analysis would be stratified by sex. Analyses were conducted using IBM SPSS Statistics 19.
Results
Table 1 describes the basic characteristics of the eligible children (2121 boys and 2516 girls). Differences on sugared drinks consumption, sports participation, TV viewing and computer use were found according to gender, while active transportation, breakfast consumption and sleep duration did not differ. Boys reported higher intake of sugared drinks, higher sports participation and higher TV and computer use compared to girls. There was also a higher proportion of overweight boys compared to girls, but no differences in obesity prevalence [3].
Parental education and children’s body composition (c-path)
Analyses for effect modification by sex did not show significant results (all p-values > 0.324). Subsequently, all analyses below are presented for boys and girls together. The results showed that parental education was significantly inversely related with BMI (ß = −0.43; CI: -0.64, -0.23) and waist circumference (ß = −0.94; CI: -1.47, -0.41).
Associations between parental education and energy balance-related behaviors (a-path)
As described in Tables 2 and Table 3 significant associations with parental education were found for sugared drinks, breakfast consumption, sports participation, TV viewing and computer use (all p < 0.001). Parental education was positively associated with sports participation and breakfast consumption, while sugared drinks, TV viewing and computer use were negatively associated with the parental education. Parental education was negatively associated with active transportation in the BMI model, but not in the waist circumference model.
Associations between energy balance-related behaviors and children’s body composition (path-b)
TV viewing and computer use were positively associated with both BMI and waist circumference, while sports participation, breakfast consumption and sleep duration were negatively associated with both BMI and waist circumference (all p < 0.01). Sugared drinks consumption was also negatively associated with BMI (p < 0.05), but not with waist circumference. These variables were selected to be included in the final multiple mediator models, as shown in the third column of Table 2 and Table 3.
Mediation effects (a*b)
The fourth and sixth columns of Tables 2 and Table 3 show the estimated mediation effects and the proportion mediated. Indirect effects (see Figure 1) were statistically significant for breakfast consumption, sports participation, TV viewing and computer use in both models, and for sugared drinks in the BMI model. The mediated proportions varied, with the highest proportion for breakfast consumption (12.6%-13.5%) and the smallest for computer use (5.4%-7.4%). The total proportions of the overall effect mediated by all the mediators were 18.7% for the BMI model and 35.8% for the waist circumference model.
Sugared drinks consumption had a suppressive effect on the relationship between parental education and BMI (−6.1%), due to opposite directions of the direct and indirect associations.
Direct association (path-c’)
As can be seen in Tables 2 and Table 3, there were significant direct associations between parental education and BMI and waist circumference, after inclusion of the presumed mediators in the model.
Discussion
The present study aimed to explore the mechanisms through which parental education differences are associated with children’s body composition. Current results first confirmed that parental educational level was inversely associated with children’s BMI and waist circumference. Next, the results showed that the association between parental education and children’s body composition was partially mediated by certain EBRBs, namely breakfast consumption, sports participation, TV viewing and computer use. Additionally, a suppression effect was found for sugared drinks intake. No mediation effect was found for active transportation and sleep duration.
Although previous studies looked at the separate relationships and not at the mediation effect, the results are in line with previous reports in which higher parental education was associated with lower childhood overweight indices [29, 30]. The associations between parental education and the EBRBs are also in line with available literature showing a negative association between several SES-indicators (including parental education) and breakfast skipping [31], sedentary habits [32], sugared drinks intake [33] and active transportation [34], and a positive association between SES and physical activity [32].
The current results on the association between the different EBRBs and the body composition outcomes are also in agreement with previous reports. Physical activity level, TV viewing, sugared drinks intake, breakfast consumption and sleep duration have been clearly associated with childhood overweight, while computer use was found to be related only in some studies [9, 35–38]. Previous reports on the association between active transportation and overweight did not show a consistent relationship [18, 39].
Although sleep duration has been associated negatively with childhood overweight – which was also confirmed in the present data-, the current analysis did not show a mediation effect of sleep duration, due to a non-significant association between parental education and sleep duration. In contrast, parental education was associated with active transportation, but active transportation was not associated with body composition indices. Recent reports showed positive associations between parental education and cycling to school while negative associations between cycling to school and overweight have been reported [40, 41]. Therefore, the single mediation analysis was also repeated for the two active transportation categories separately, in order to look at the specific trends. We found a negative association between parental education and walking to school but no association between parental education and cycling to school. In both cases no association with body composition indices was found (data not shown).
A suppression effect was found for sugared drinks intake. This effect could be due to a lower intake of sugared drinks in overweight children, or a higher impact of underreporting in this group [42–44]. It is also noteworthy that sugared drinks consumption was a suppressor only in the BMI model, but not in the waist circumference model.
The analyses included two different body composition indicators, namely BMI and waist circumference. The significant mediators explained 36% of the relationship between parental education and waist circumference, while only 19% of the relationship between parental education and BMI was explained. This finding could reflect the differences between BMI and waist circumference as measures of childhood adiposity. Waist circumference has been observed in cross-sectional studies to be a good abdominal fat estimate [45], a better predictor of cardiovascular disease risk factors in childhood [46, 47], and to predict cardio-metabolic health risk in adults beyond that explained by BMI [48, 49].
To our knowledge, this is one of the first studies trying to disentangle the complex interaction between parental education, several EBRBs and children’s body composition by applying mediation analysis. The proportion of the associations explained by the included mediators in both models was moderate, remaining the direct associations (c-path) still significant after adjusting for the mediators (c’-path). These results suggest that other variables not included in the analyses may play a mediating role in the relationship between parental education and children’s body composition. Future analyses including other potential mediators, not only behavioral but also environmental factors, like availability or accessibility, could enhance the knowledge about the complex relationship between parental education and children’s body composition.
It has to be kept in mind that this study is subject to some limitations. First, this concerns a cross-sectional study providing evidence for associations but not causation. Further, data on dietary, physical activity and sedentary behaviors were based on self-reports, and thus possibly biased. However, the measures showed good test-retest reliability and construct validity [23, 24]. When considering sedentary behaviors it is also important to note that some sedentary activities, like reading or studying were not included in the present study. Is therefore possible that questionnaires did not reflect the real, total time spent in sedentary behaviors. Parental education was reported taking into account both parents, and therefore we were not able to assess the differential influence of paternal and maternal educational levels on children’s EBRBs. Although the use of central adiposity indicators like waist circumference is useful as a good predictor of future health problems, it could be helpful to control for the maturation level when assessing pre- and adolescent population [50]. Unfortunately, no information on maturation level was collected in the ENERGY cross-sectional study. Finally, the differences between selected participants and those not included in the analysis may influence the generalizability of the results. However, differences were small and, although significant, probably not relevant.
Strengths of the present study include the large multinational sample from different regions across Europe, the available measured weight, height and waist circumference and the standardized data collection protocol across the different centers.
Conclusions
The association between parental education and children’s body composition was partially mediated by breakfast consumption, sports participation, TV viewing and computer use. The significant mediators explained a higher proportion of the association between parental education and waist circumference compared to the association between parental education and BMI. Tailored overweight and obesity prevention strategies in low SES preadolescent populations should develop specific messages focusing on the importance of encouraging daily breakfast consumption, increasing sports participation and decreasing TV viewing and computer use.
Author’s contributions
JMFA carried out the statistical analysis and drafted the manuscript. SJTV supervised the statistical analysis and design. IDB, EB, YM, EK, NJ and LAM collected the data in their countries or supervised data collection. JB is the coordinator of the ENERGY-project and helped to draft the manuscript. LAM supervised the statistical analysis and helped to draft the manuscript. All co-authors read and approved the final version of the manuscript.
References
Dietz WH: Health consequences of obesity in youth: childhood predictors of adult disease. Pediatrics. 1998, 101: 518-525.
Rokholm B, Baker JL, Sorensen TI: The levelling off of the obesity epidemic since the year 1999–a review of evidence and perspectives. Obesity reviews: an official journal of the International Association for the Study of Obesity. 2010, 11: 835-846. 10.1111/j.1467-789X.2010.00810.x.
Brug J, Van Stralen M, Te Velde S, Chinapaw M, De Bourdeaudhuij I, Lien N, Bere E, Maskini V, Singh A, Maes L, et al: Differences in weight status and energy-balance related behaviors among schoolchildren across Europe: The ENERGY-project. PLoS One. 2012, 7 (4): e34742-10.1371/journal.pone.0034742.
Singh AS, Mulder C, Twisk JW, Van Mechelen W, Chinapaw MJ: Tracking of childhood overweight into adulthood: a systematic review of the literature. Obesity reviews: an official journal of the International Association for the Study of Obesity. 2008, 9: 474-488. 10.1111/j.1467-789X.2008.00475.x.
Nader PR, O'Brien M, Houts R, Bradley R, Belsky J, Crosnoe R, Friedman S, Mei Z, Susman EJ: Identifying risk for obesity in early childhood. Pediatrics. 2006, 118: e594-601. 10.1542/peds.2005-2801.
Summerbell CD, Douthwaite W, Whittaker V, Ells LJ, Hillier F, Smith S, Kelly S, Edmunds LD, Macdonald I: The association between diet and physical activity and subsequent excess weight gain and obesity assessed at 5 years of age or older: a systematic review of the epidemiological evidence. Int J Obes. 2009, 33 (Suppl 3): S1-92.
Jimenez-Pavon D, Kelly J, Reilly JJ: Associations between objectively measured habitual physical activity and adiposity in children and adolescents: Systematic review. International journal of pediatric obesity: IJPO: an official journal of the International Association for the Study of Obesity. 2010, 5: 3-18. 10.3109/17477160903067601.
Moreno LA, Rodriguez G: Dietary risk factors for development of childhood obesity. Curr Opin Clin Nutr Metab Care. 2007, 10: 336-341. 10.1097/MCO.0b013e3280a94f59.
Rey-Lopez JP, Vicente-Rodriguez G, Biosca M, Moreno LA: Sedentary behaviour and obesity development in children and adolescents. Nutrition, metabolism, and cardiovascular diseases: NMCD. 2008, 18: 242-251. 10.1016/j.numecd.2007.07.008.
Must A, Parisi SM: Sedentary behavior and sleep: paradoxical effects in association with childhood obesity. Int J Obes. 2009, 33 (Suppl 1): S82-86.
Hense S, Pohlabeln H, De Henauw S, Eiben G, Molnar D, Moreno LA, Barba G, Hadjigeorgiou C, Veidebaum T, Ahrens W: Sleep duration and overweight in European children: is the association modified by geographic region?. Sleep. 2011, 34: 885-890.
Lobstein T, Frelut ML: Prevalence of overweight among children in Europe. Obesity reviews: an official journal of the International Association for the Study of Obesity. 2003, 4: 195-200. 10.1046/j.1467-789X.2003.00116.x.
Gordon-Larsen P, Adair LS, Popkin BM: The relationship of ethnicity, socioeconomic factors, and overweight in US adolescents. Obes Res. 2003, 11: 121-129. 10.1038/oby.2003.20.
Brug J, Lien N, Klepp KI, Van Lenthe FJ: Exploring overweight, obesity and their behavioural correlates among children and adolescents: results from the Health-promotion through Obesity Prevention across Europe project. Public Health Nutr. 2010, 13: 1676-1679. 10.1017/S1368980010002211.
Te Velde SJ, De Bourdeaudhuij I, Thorsdottir I, Rasmussen M, Hagstromer M, Klepp KI, Brug J: Patterns in sedentary and exercise behaviors and associations with overweight in 9–14-year-old boys and girls–a cross-sectional study. BMC Publ Health. 2007, 7: 16-10.1186/1471-2458-7-16.
Johnson F, Pratt M, Wardle J: Socio-Economic Status and Obesity in Childhood. In Epidemiology of Obesity in Children and Adolescents Prevalence and Etiology, Springer (Series Editor. 1st edition. Edited by Moreno LA, Pigeot I, Ahrens W. Springer: Series on Epidemiology and Public Health; 2010.
Morgenstern M, Sargent JD, Hanewinkel R: Relation between socioeconomic status and body mass index: evidence of an indirect path via television use. Arch Pediatr Adolesc Med. 2009, 163: 731-738. 10.1001/archpediatrics.2009.78.
Wijga AH, Smit HA, Brunekreef B, Koppelman GH, Kerkhof M, Bemelmans WJ, Scholtens S: Diet, Screen Time, Physical Activity, and Childhood Overweight in the General Population and in High Risk Subgroups: Prospective Analyses in the PIAMA Birth Cohort. J Obes. 2010, 2010 (42396): 9.
Lioret S, Touvier M, Lafay L, Volatier JL, Maire B: Dietary and physical activity patterns in French children are related to overweight and socioeconomic status. J Nutr. 2008, 138: 101-107.
Brug J, Te Velde SJ, Chinapaw MJ, Bere E, De Bourdeaudhuij I, Moore H, Maes L, Jensen J, Manios Y, Lien N, et al: Evidence-based development of school-based and family-involved prevention of overweight across Europe: the ENERGY-project's design and conceptual framework. BMC Publ Health. 2010, 10: 276-10.1186/1471-2458-10-276.
Van Stralen MM, Te Velde SJ, Singh AS, De Bourdeaudhuij I, Martens MK, van der Sluis M, Manios Y, Grammatikaki E, Chinapaw MJ, Maes L, et al: EuropeaN Energy balance Research to prevent excessive weight Gain among Youth (ENERGY) project: Design and methodology of the ENERGY cross-sectional survey. BMC Publ Health. 2011, 11: 65-10.1186/1471-2458-11-65.
Klepp KI, Perez-Rodrigo C, De Bourdeaudhuij I, Due PP, Elmadfa I, Haraldsdottir J, Konig J, Sjostrom M, Thorsdottir I, De Almeida MD V, et al: Promoting fruit and vegetable consumption among European schoolchildren: rationale, conceptualization and design of the pro children project. Ann Nutr Metab. 2005, 49: 212-220. 10.1159/000087245.
Singh AS, Vik FN, Chinapaw J, Uijtdewiligen L, Verloigne M, Fernández-Alvira JM, Stomfai S, Manios Y, Martens M, Brug J: Test-retest reliability and construct validity of the ENERGY-child questionnaire on energy balance-related behaviours and their potential determinants: the ENERGY-project. Int J Behav Nutr Phys Act. 2011, 8: 136-10.1186/1479-5868-8-136.
Singh AS, Chinapaw MJ, Uijtdewilligen L, Vik FN, Van Lippevelde W, Fernandez-Alvira JM, Stomfai S, Manios Y, van der Sluis M, Terwee C, Brug J: Test-retest reliability and construct validity of the ENERGY-parent questionnaire on parenting practices, energy balance-related behaviours and their potential behavioural determinants: the ENERGY-project. BMC Res Notes. 2012, 5: 434-10.1186/1756-0500-5-434.
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH: Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000, 320: 1240-1243. 10.1136/bmj.320.7244.1240.
MacKinnon DP, Fairchild AJ, Fritz MS: Mediation analysis. Annu Rev Psychol. 2007, 58: 593-614. 10.1146/annurev.psych.58.110405.085542.
Mackinnon D: Introduction to Statistical Mediation Analysis. 2008, New York: Lawrence Erlbaum Associates
Preacher KJ, Hayes AF: Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008, 40: 879-891. 10.3758/BRM.40.3.879.
Lamerz A, Kuepper-Nybelen J, Wehle C, Bruning N, Trost-Brinkhues G, Brenner H, Hebebrand J, Herpertz-Dahlmann B: Social class, parental education, and obesity prevalence in a study of six-year-old children in Germany. Int J Obes. 2005, 29: 373-380. 10.1038/sj.ijo.0802914.
Shrewsbury V, Wardle J: Socioeconomic status and adiposity in childhood: a systematic review of cross-sectional studies 1990–2005. Obesity. 2008, 16: 275-284. 10.1038/oby.2007.35.
Dubois L, Girard M, Potvin Kent M: Breakfast eating and overweight in a pre-school population: is there a link?. Public Health Nutr. 2006, 9: 436-442.
Drenowatz C, Eisenmann JC, Pfeiffer KA, Welk G, Heelan K, Gentile D, Walsh D: Influence of socio-economic status on habitual physical activity and sedentary behavior in 8- to 11-year old children. BMC Publ Health. 2010, 10: 214-10.1186/1471-2458-10-214.
Cullen KW, Ash DM, Warneke C, De Moor C: Intake of soft drinks, fruit-flavored beverages, and fruits and vegetables by children in grades 4 through 6. Am J Public Health. 2002, 92: 1475-1478. 10.2105/AJPH.92.9.1475.
Brophy S, Cooksey R, Lyons RA, Thomas NE, Rodgers SE, Gravenor MB: Parental factors associated with walking to school and participation in organised activities at age 5: analysis of the Millennium Cohort Study. BMC Publ Health. 2011, 11: 14-10.1186/1471-2458-11-14.
Janssen I, Katzmarzyk PT, Boyce WF, Vereecken C, Mulvihill C, Roberts C, Currie C, Pickett W: Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obesity reviews : an official journal of the International Association for the Study of Obesity. 2005, 6: 123-132. 10.1111/j.1467-789X.2005.00176.x.
Rampersaud GC, Pereira MA, Girard BL, Adams J, Metzl JD: Breakfast habits, nutritional status, body weight, and academic performance in children and adolescents. J Am Diet Assoc. 2005, 105: 743-760. 10.1016/j.jada.2005.02.007. quiz 761–742
Ludwig DS, Peterson KE, Gortmaker SL: Relation between consumption of sugar-sweetened drinks and childhood obesity: a prospective, observational analysis. Lancet. 2001, 357: 505-508. 10.1016/S0140-6736(00)04041-1.
Chen X, Beydoun MA, Wang Y: Is sleep duration associated with childhood obesity? A systematic review and meta-analysis. Obesity. 2008, 16: 265-274. 10.1038/oby.2007.63.
Davison KK, Werder JL, Lawson CT: Children's active commuting to school: current knowledge and future directions. Prev Chronic Dis. 2008, 5: A100.
Borrestad LA, Andersen LB, Bere E: Seasonal and socio-demographic determinants of school commuting. Prev Med. 2011, 52: 133-135. 10.1016/j.ypmed.2010.12.006.
Bere E, Seiler S, Eikemo TA, Oenema A, Brug J: The association between cycling to school and being overweight in Rotterdam (The Netherlands) and Kristiansand (Norway). Scand J Med Sci Sports. 2011, 21: 48-53. 10.1111/j.1600-0838.2009.01004.x.
Singh R, Martin BR, Hickey Y, Teegarden D, Campbell WW, Craig BA, Schoeller DA, Kerr DA, Weaver CM: Comparison of self-reported, measured, metabolizable energy intake with total energy expenditure in overweight teens. Am J Clin Nutr. 2009, 89: 1744-1750. 10.3945/ajcn.2008.26752.
Livingstone MB, Robson PJ: Measurement of dietary intake in children. Proc Nutr Soc. 2000, 59: 279-293. 10.1017/S0029665100000318.
Livingstone MB, Robson PJ, Wallace JM: Issues in dietary intake assessment of children and adolescents. Br J Nutr. 2004, 92 (Suppl 2): S213-222.
Brambilla P, Bedogni G, Moreno LA, Goran MI, Gutin B, Fox KR, Peters DM, Barbeau P, De Simone M, Pietrobelli A: Crossvalidation of anthropometry against magnetic resonance imaging for the assessment of visceral and subcutaneous adipose tissue in children. Int J Obes. 2006, 30: 23-30. 10.1038/sj.ijo.0803163.
Savva SC, Tornaritis M, Savva ME, Kourides Y, Panagi A, Silikiotou N, Georgiou C, Kafatos A: Waist circumference and waist-to-height ratio are better predictors of cardiovascular disease risk factors in children than body mass index. International journal of obesity and related metabolic disorders: journal of the International Association for the Study of Obesity. 2000, 24: 1453-1458. 10.1038/sj.ijo.0801401.
Moreno LA, Pineda I, Rodriguez G, Fleta J, Sarria A, Bueno M: Waist circumference for the screening of the metabolic syndrome in children. Acta Paediatr. 2002, 91: 1307-1312. 10.1111/j.1651-2227.2002.tb02825.x.
Janssen I, Katzmarzyk PT, Ross R: Body mass index, waist circumference, and health risk: evidence in support of current National Institutes of Health guidelines. Arch Intern Med. 2002, 162: 2074-2079. 10.1001/archinte.162.18.2074.
Schmidt MD, Dwyer T, Magnussen CG, Venn AJ: Predictive associations between alternative measures of childhood adiposity and adult cardio-metabolic health. Int J Obes. 2011, 35: 38-45. 10.1038/ijo.2010.205.
Bratberg GH, Nilsen TI, Holmen TL, Vatten LJ: Early sexual maturation, central adiposity and subsequent overweight in late adolescence. a four-year follow-up of 1605 adolescent Norwegian boys and girls: the Young HUNT study. BMC Publ Health. 2007, 7: 54-10.1186/1471-2458-7-54.
Acknowledgements
The ENERGY-project is funded by the Seventh Framework Programme (CORDIS FP7) of the European Commission, HEALTH (FP7-HEALTH-2007-B). The content of this article reflects only the authors’ views and the European Community is not liable for any use that may be made of the information contained therein.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Fernández-Alvira, J.M., te Velde, S.J., De Bourdeaudhuij, I. et al. Parental education associations with children’s body composition: mediation effects of energy balance-related behaviors within the ENERGY-project. Int J Behav Nutr Phys Act 10, 80 (2013). https://doi.org/10.1186/1479-5868-10-80
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1479-5868-10-80