
Abstract
Background
Randomised, cluster-based study designs in schools are commonly used to evaluate children’s physical activity interventions. Sample size estimation relies on accurate estimation of the intra-cluster correlation coefficient (ICC), but published estimates, especially using accelerometry-measured physical activity, are few and vary depending on physical activity outcome and participant age. Less commonly-used cluster-based designs, such as stepped wedge designs, also need to account for correlations over time, e.g. cluster autocorrelation (CAC) and individual autocorrelation (IAC), but no estimates are currently available. This paper estimates the school-level ICC, CAC and IAC for England children’s accelerometer-measured physical activity outcomes by age group and gender, to inform the design of future school-based cluster trials.
Methods
Data were pooled from seven large English datasets of accelerometer-measured physical activity data between 2002–18 (> 13,500 pupils, 540 primary and secondary schools). Linear mixed effect models estimated ICCs for weekday and whole week for minutes spent in moderate-to-vigorous physical activity (MVPA) and being sedentary for different age groups, stratified by gender. The CAC (1,252 schools) and IAC (34,923 pupils) were estimated by length of follow-up from pooled longitudinal data.
Results
School-level ICCs for weekday MVPA were higher in primary schools (from 0.07 (95% CI: 0.05, 0.10) to 0.08 (95% CI: 0.06, 0.11)) compared to secondary (from 0.04 (95% CI: 0.03, 0.07) to (95% CI: 0.04, 0.10)). Girls’ ICCs were similar for primary and secondary schools, but boys’ were lower in secondary. For all ages, combined the CAC was 0.60 (95% CI: 0.44–0.72), and the IAC was 0.46 (95% CI: 0.42–0.49), irrespective of follow-up time. Estimates were higher for MVPA vs sedentary time, and for weekdays vs the whole week.
Conclusions
Adequately powered studies are important to evidence effective physical activity strategies. Our estimates of the ICC, CAC and IAC may be used to plan future school-based physical activity evaluations and were fairly consistent across a range of ages and settings, suggesting that results may be applied to other high income countries with similar school physical activity provision. It is important to use estimates appropriate to the study design, and that match the intended study population as closely as possible.
Similar content being viewed by others

Background
Evaluating the effectiveness of public health interventions is important to inform and develop policy recommendations. Randomised controlled trials (RCTs) are often used to evaluate public health interventions as they tend to be less susceptible to bias than other designs [1]. Often individuals fall naturally into groups (for example schools, workplaces, or geographical locations), or clusters, and it is important to take such clustering into account as individuals within the same cluster are often more similar to each other than to individuals in other clusters [2]. Cluster-based designs, such as cluster RCTs, cluster cross-over trials and stepped wedge designs, are studies in which clusters are randomised rather than the individuals within these groups [2]. Such designs are common in public health settings, where the intervention itself may also be implemented at the cluster level, for example a school programme to increase children’s physical activity, and thus not allow for individual-level randomisation. However, the design and analysis of cluster-based studies is more complex, with larger sample sizes required than for an individual randomised study. The larger the intra-cluster correlation coefficient (ICC), the larger the sample size required, and ignoring the clustering in the design can result in an underpowered study [2].
There is a wide literature concerning sample size estimation for cluster-based designs [2,3,4,5,6], although much is based in a clinical rather than public health setting. Approximate formulae are commonly provided in the form of an adjustment to the sample size required for an individually-randomised trial, and rely on the ICC, which captures the amount of variance explained at the group level [7, 8]. Depending on the study design, there may also be other correlations required for accurate sample size estimation. For example, studies with multiple measures over time in the same clusters, such as stepped wedge designs or cluster RCTs with baseline measurements, may need to take into account cluster autocorrelation (CAC) [9] which measures similarity in the outcome in the same cluster over time. In addition, cohort cluster designs with repeated measurements on the same individuals, should also account for individual autocorrelation (IAC) [4, 5], which captures similarity in outcome measures for the same individual. Accounting for these correlations is important for the same reason as accounting for clustering, as they all capture different ways in which measurements are correlated and thus can affect the required sample size. Note that the ICC, CAC and IAC are features of the clusters or individuals themselves and the outcome measure, and not under the control of the researcher. Reviews that summarise data on ICCs drawn from multiple datasets show considerable variability, with estimates between 0 and 0.2 depending on the outcome, type of cluster, country and population [10,11,12,13,14,15,16]. In particular, ICCs are typically larger for smaller cluster sizes, for example, varying between a median of 0.002 at district health level to 0.02 at postcode sector level [12]. Far less is known about the CAC, and the few estimates that have been published range between 0.3 and 0.9 with wide confidence intervals for a mix of clinical and risk factor outcomes, and so differences by outcome or cluster type are not clear [15, 16]. Finally an estimate of the IAC is also needed whenever the same individuals are measured at multiple time points; as this is an individual rather than cluster-level correlation, estimates are generally easier to derive from other studies of both cluster and individual trials. Accurate and precise estimation of the ICC and CAC, and the IAC for cohort designs, is therefore important in planning a study to ensure the sample size is sufficient to detect an intervention effect. However, pilot studies are typically too small to provide robust estimates [17], with a recent review of school-based ICCs finding very little correlation between ICCs estimated from a pilot and the full trial [18]. Therefore, pilot studies are generally not suitable for estimating ICCs or CACs, although can provide other data needed for sample size estimation and study design, including the IAC.
Cluster-based designs are particularly well-suited to evaluate children’s physical activity interventions, as schools form obvious clusters and make good targets for intervention. Estimates of ICCs for children’s physical activity vary, depending on the outcome used. Physical activity guidelines in the UK, and in many other countries, are for children to achieve an average of at least 60 min of moderate to vigorous physical activity (MVPA) per day [19, 20], and so whole-day MVPA is a common primary outcome in such studies. ICCs for MVPA are between 0.01–0.06 for self-reported physical activity [13, 21,22,23,24] and higher for accelerometer-measured physical activity at 0.06–0.13 [25,26,27,28]. Estimates of average sedentary time across the whole day are less often reported, but ICCs tend to be lower, at 0.02 for self-reported sedentary time [13] and 0.06–0.09 for accelerometer-measured sedentary time [29, 30]. These ICC estimates for both MVPA and sedentary time are often calculated using relatively few schools (< 30) and usually reported without confidence intervals. Unlike other health-related behavioural outcomes (such as smoking and alcohol), where much of the cluster dependence is due to demographic similarities within schools, this is not the case for physical activity, where MVPA ICCs adjusted for individual covariates remain similar to unadjusted estimates [13, 27]. As schools play a specific role in facilitating physical activity, with a requirement to provide a certain amount of activity within the school curriculum, there is a direct mechanism for similarities between children in the same school. This is reflected in variation in ICCs of MVPA throughout the day, for example, 0.25 in school and 0.06 after school [28], and differences between weekdays (0.13) and weekends (0.05) [27]. As school size, facilities, curriculum and structure of the school day will all impact on the ICC, we might also expect ICCs to be country-specific, and differ by type of school, and especially by age. For example, in the UK, primary schools (ages 4–11) are typically smaller in terms of pupil numbers and physical size, have fewer specialist sports facilities and have a single class teacher rather than multiple subject teachers, compared to secondary schools (ages 11–18). While reported ICCs for children’s MVPA tend to be higher than for adolescents [26], the majority of published estimates are for adolescents and so it is not clear if and how they differ. We are also not aware of any studies that compare ICCs between boys and girls in the same schools. As girls consistently engage in less physical activity than boys on average [31], this may be an important difference, for example if girls are more reliant on the school environment, especially as interventions are often specifically designed to target girls.
The aim of this paper is to estimate the ICC, CAC and IAC for UK children’s accelerometer-measured weekday and whole week MVPA and sedentary time by age group and where possible, gender, to help inform the design of future school-based cluster trials of physical activity interventions. We use secondary data from seven large observational studies of accelerometer physical activity data, where participants are clustered within schools and that include a sufficiently large number of schools for reliable estimates. We pool data to estimate ICCs for different age groups, stratified by gender, and compare these to ICCs for children’s self-report physical activity. We also estimate the CAC and IAC from those datasets that include longitudinal data. To the best of our knowledge, there is no literature that has explored whether there are differences in ICC by accelerometer type or processing protocols e.g. cut-points, epochs or definition and number of valid days, and so a secondary aim is to explore the effect of different accelerometer processing criteria on the ICCs. Finally, we will illustrate how these findings affect estimates of the required sample size in a worked example.
Methods
Data
This paper uses secondary data from seven English studies of children’s accelerometer-measured physical activity. We began by selecting studies which included data on school membership from the International Children’s Accelerometry Database (ICAD) [32], which pooled and harmonised accelerometer physical activity data on children and adolescents. We restricted to datasets from England as ICCs are likely to differ between countries due to differences in school structure, facilities and curriculum requirements [33]. We then identified additional studies from within the University of Bristol and from the literature which also used Actigraph waist-worn accelerometers, were based in England and contained data from at least 20 schools. The seven included studies were the Avon Longitudinal Study of Parents and Children (ALSPAC) [34, 35]; Sport, Physical activity and Eating behaviour: Environmental Determinants in Young people (SPEEDY) [36] and Personal and Environmental Associations with Children's Health (PEACH) [37] studies from ICAD, and the B-Proact1v study [38, 39], Action 3:30 feasibility trial (A3:30) [40], Active for Life Year 5 (AFLY5) trial [41, 42] and the Child Heart And health Study in England (CHASE) [43]. All studies received ethical approval and informed consent [44] (see individual studies for further details). The included studies consisted of four cohort studies, one cross-sectional study and two cluster RCT trials (Table 1). For the cluster RCT trials, we used baseline data from both arms and follow-up data from the control arm only. Data covered ages 5 to 16 years, comprising over 13,500 pupils from 540 schools, with 60% from primary schools and 40% from secondary schools.
All studies used hip-worn Actigraph accelerometers (Table S1). Data from the ICAD studies were harmonised to use 60s epochs, Evenson cut-points (with MVPA defined as < 2295 counts per minute (cpm)), and a valid day defined as a minimum of 480 min of wear time. Data from the B-Proact1v study was re-processed to the same criteria for comparability, while the other studies used smaller epochs of 5-10s. All but one study used Evenson cut-points and similar wear time of 480–500 min, with the remaining study using a lower MVPA threshold of 2000 cpm and a longer valid day of at least 600 min of wear time (Table S1). Note that the impact of different processing criteria is assessed in the Analysis section.
From each study, we extracted accelerometer data (mean minutes of MVPA, sedentary time and wear time for weekdays and the whole week), and demographics (age and gender) for each time point for each child. Age was grouped into categories based on England school year: Year 1 & 4 (age 5–6 and age 8–9; note that no studies provided data on children between ages 6 and 8), Year 5 (age 9–10), Year 6 (age 10–11), Year 7 (age 11–12), Year 8 & 9 (age 12–14) and Year 10 & 11 (age 14–16). Primary schools in England comprise Years 1–6, and secondary schools cover Years 7–11.
To compare ICCs for accelerometer-measures and self-report physical activity, we also used data from the Active Lives Children and Young People survey 2018–19 (ALCYP) [45, 46]. This is an annual cross-sectional survey commissioned by Sport England, which collects self-report physical activity data for children aged 7–16 from a large representative sample (n = 107,922 across 1815 schools) across the whole of England to inform UK government strategy. Children were asked detailed questions about participation and intensity in a range of activities both in and out of school on each day of the previous week. We excluded children aged 5–7 years where physical activity data were not comparable as the data were reported by parents rather than the children, and used the provided school year groups: Year 3 & 4 (age 7–9) Year 5 & 6 (age 9–11), Year 7 & 8 (age 11–13) and Year 9 & 11 (age 13–16). Weekday and whole week MVPA was calculated from the provided derived variables of minutes of MVPA by day.
Analysis
The primary outcome was mean weekday MVPA, with secondary outcomes of mean MVPA across the whole week, sedentary time for weekdays and the whole week. We restricted analysis to those pupils who provided at least two days of valid data. Physical activity outcomes and gender were summarised by school year group. All analysis was run in Stata v17 [47], and sample size estimates were calculated using the clusterpower package in R.
Intra-cluster correlation coefficients
To produce model-based estimates of the ICC by school year group, we used linear mixed effect models to take into account variability across studies, with separate models for primary and secondary schools, due to differences in total variability. Three-level mixed models included fixed terms for age and accelerometer wear time, and random effect terms for study, individual repeated measures and school-level random coefficients for each school year group. ICCs were calculated separately for each school year group from the total and between-school variance estimates, with approximate 95% confidence intervals obtained using the delta method [48] on the logit scale and back-transformed to give a 95% confidence interval for each ICC. We also ran subgroup analyses by gender. Models were run for weekday and whole week MVPA, and for weekday and whole week sedentary time. For longitudinal data, we also estimated ICCs for weekday MVPA adjusted for baseline (i.e. previous MVPA measurement), for primary and secondary schools. Due to smaller sample sizes we did not break down further by school year group, or stratify by gender. Finally, we ran models for weekday and whole week self-report MVPA using the ALCYP data (with no study random effect) using a linear model. We chose not to transform the data, despite being heavily right-skewed, as this is not often done in practice and so ICCs on the transformed scale would be less useful, and potentially misinterpreted.
Effect of accelerometer processing
To explore whether ICCs differ depending on the accelerometer processing, we ran a series of additional analyses. We used the B-Proact1v data from Year 6 only, where we had access to the raw accelerometer data and so could re-process in different ways, to look at differences in the cut points to determine MVPA (2000, 2295), resolution (5s 10s and 60s epochs), definition of a valid day (minimum wear time required for inclusion: 400 min, 480 min and 600 min), and the minimum number of valid days for inclusion (one, two or three days).
Cluster and individual autocorrelations
As the autocorrelations CAC and IAC may depend on the follow-up time between measurements, we used empirical estimates from the Pearson correlation coefficients for each study/follow-up time combination. Where studies covered the transition between primary and secondary school, we included only data within the same school for estimating the CAC, but used all measurements across multiple schools for the IAC. These were transformed using Fisher transformations for approximate normality, combined using meta-analysis and then back-transformed to produce joint estimates of the CAC and IAC by follow-up time. Due to the smaller numbers of pupils and schools available to calculate the autocorrelations, we did not separate by school type or gender. We also excluded schools with fewer than five pupils in calculating the school-level correlations for the CAC.
Example sample size calculations
To illustrate how the estimates produced in earlier sections can be used to estimate sample sizes in future cluster-based evaluations of children’s physical activity interventions, we estimated the number of schools required to detect an effect size of a 5 min increase in weekday MVPA (a difference likely to have a meaningful health impact [49]), with power 80% and significance level 5%, for six different study designs (cluster RCT, cluster RCT adjusted for baseline, cross-sectional and cohort stepped wedge designs with two and three steps). We calculated sample sizes for Year 5 (primary) and Year 10/11 (secondary) separately, using estimates of the total variation, ICC, CAC and IAC from the analysis above. We used two values of the ICC, the point estimate and the upper bound of the 95% confidence interval, to investigate how sensitive the resulting sample sizes were to different values of ICC. We assumed an achieved sample size of 25 pupils per school for primary and 50 for secondary; these are smaller than typical year groups to allow for nonresponse. We also explored different values of ICC and varying the number of pupils per school.
Results
The sample comprised 13,650 children from 540 schools across seven studies, measured at a total of 19 time points (Table 2). Around half the pupils (53%) were female, with 60% of the measurements taken in primary schools and 40% in secondary schools. Missing accelerometer data was around 4–10% for most studies (with a higher missingness rate of 20% for weekdays in the AFLY5 study) resulting in 21,076 valid weekday measurements and 21,649 valid measurements across the whole week (Table S2).
Intra-cluster correlation coefficients
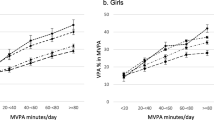
Modelled ICCs for weekday accelerometer MPVA are shown in Fig. 1, with full estimates and 95% confidence intervals given in Table 3. ICCs were slightly higher for children in primary schools (between 0.07 (95% CI: 0.05, 0.10) for Years 1 & 4, and 0.08 (95% CI: 0.06 – 0.11) in Year 6) compared to secondary (between 0.04 (95% CI: 0.03, 0.07) for Year 7, and 0.07 (95% CI: 0.04 – 0.1) in Years 8 & 9). There were only small differences by school year group, with ICCs increasing slightly in primary school with age, and highest in secondary school at Year 8/9. ICCs for boys and girls (Figure S1; Tables S3 & S4) were similar in primary schools, but in secondary schools ICCs were higher for girls than for boys (a maximum of 0.10 (95% CI: 0.06, 0.15) for girls, and 0.04 (95% CI: 0.02 – 0.08) for boys). ICCs for whole week MVPA were slightly lower than weekdays only. ICCs for sedentary time were lower than for MVPA, with estimates of between 0.03 (Years 1 & 4; 95% CI: 0.01, 0.06) and 0.05 (Year 6; 95% CI: 0.03 – 0.11) in primary schools and < 0.01 in secondary schools. ICCs for sedentary time did not differ notably by gender. However, total within-study variation was larger in secondary schools vs primary schools and in boys vs girls for all physical activity outcomes (Table S5).

Estimated intra-cluster correlation coefficient (ICC) and 95% confidence intervals by age group
ICCs adjusted for baseline (that is, the previous available measurement; Table S6) were slightly smaller (0.06 for primary; 0.04 for secondary) than unadjusted ICCs but showed similar patterns, with higher ICCs for primary schools compared to secondary, for weekdays compared to the whole week and for MVPA compared to sedentary time. The total variation was lower in models adjusted for baseline (Table S5). Self-report MVPA was highly skewed, with ICCs similar to those for accelerometer-measured MVPA, but no substantial differences between girls and boys or between weekday and whole week estimates (Table S7).
Effect of accelerometer processing
Looking at the BProact1v Year 6 data only, the choice of MVPA cut-point, resolution, definition of a valid day and minimum number of valid days made only minor differences to the ICCs (Table S8). All ICCs were estimated between 0.127 and 0.147, compared to 0.137 for data processed to the criteria used in the main analysis. The largest differences were for a lower MVPA threshold of 2000 (slightly higher ICC of 0.147) and for a longer valid day of 10h (slightly lower ICC of 0.127).
Cluster and individual autocorrelations
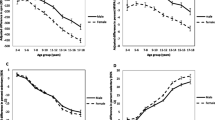
The CAC (Fig. 2; Table S9) ranged between 0.24 and 0.70 with no consistent pattern over time, and wide confidence intervals, due to relatively small numbers of schools. The estimated CAC for weekday MVPA follow-up times of 1–5 years was 0.60 (95% CI: 0.44—0.72). The CAC for follow-up of less than a year was around half the size, but is based on only one study comprising 10 schools. CACs for sedentary time were slightly lower. The individual autocorrelations for MVPA (Fig. 3; Table S10) showed a possible slow decrease over time, from 0.52 after one year, to 0.34 after 5 years, but confidence intervals were wide. IACs for sedentary time were slightly lower, but showed a similar decreasing pattern with length of follow-up. There were no differences in IAC between weekday and the whole week.

Cluster autocorrelation (CAC) by length of follow-up

Individual autocorrelation (IAC) by length of follow-up
Example sample size calculations
Table 4 and Tables S11 & S12 estimate the number of schools required to detect an effect size of a 5 min increase in weekday MVPA for a future cluster-based evaluation of children’s physical activity interventions, with power 80% and significance level 5%, and using estimates of the total variation, ICC, CAC and IAC from the results presented above. We considered six different study designs: cluster RCT, cluster RCT adjusted for baseline, cross-sectional and cohort stepped wedge designs with two and three steps. Table 4 shows that the achieved number of schools required would range substantially from 33–94 for primary and 24–96 for secondary schools, depending on the cluster design used, and assumptions about the ICC and autocorrelations. Although the ICC in secondary schools is lower, more secondary schools are needed than primary for the same effect size and power, due to the higher total variability. The number of schools required increased notably if the upper bound of the ICC 95% confidence interval was used rather than the point estimate, with 6 extra schools required for the cluster RCT in primary schools, and 14 additional secondary schools required for the same power. The simplest design, the two-arm cluster RCT, required the most schools (68–96 depending on parametrisation). Repeated measures, either in schools or pupils, increased the power and reduced the required sample size. For example, the cross-sectional two-step stepped wedge and cluster RCT adjusted for baseline both reduced the number of schools required by around 30% (from 82 to 54–62 schools in primary and from 68 to 46–50 schools in secondary). The cohort two-step stepped wedge and cross-sectional three-step stepped wedge reduced by around half (to 39–48 primary schools and 30–40 secondary schools) and the largest reductions were for the cohort three-step stepped wedge by nearly two thirds (30 primary schools, 24 secondary schools). Increasing the number of pupils per school reduced the sample size to a lesser degree with up to 20–30% reduction for an increase of 25 in number of pupils (Table S11 & S12), but this had less effect for larger ICCs and as pupils numbers increased beyond 50. The larger reductions were in the stepped wedge designs, which exploit correlation between pupils at different time points.
Discussion
In this paper we have combined data from over 13,500 pupils from 540 schools to provide a comprehensive set of estimates of school-level ICCs and autocorrelations for accelerometer-measured physical activity in children and adolescents which can be used to plan new school-based cluster trials of physical activity interventions in schools. The ICC estimates for weekday MVPA are broadly consistent with other accelerometer-measured estimates reported in the literature, which range between 0.07 to 0.13 [25,26,27], although these studies all involved fewer schools and estimates were presented without measures of precision. ICCs were slightly higher in primary schools, compared to secondary schools, as seen elsewhere [26], with only small differences by age within school type. Due to using secondary data sources, we looked at physical activity summaries across the whole day only, although other studies suggest that ICC estimates for activity during school hours only are likely to be much higher [28]. The specific criteria used in accelerometer processing had very little effect on the ICC, and we saw no differences by MVPA cut-points, resolution, definition of a valid day or number of days included. While these factors can affect estimates of minutes of MVPA themselves, the ICC is a relative measure that captures similarity between measurements and is thus less influenced by these choices as all individual measurements within a school are higher or lower in the same way. We were unable to explore the impact of wear and non-wear definitions, which tend to affect sedentary time in particular, but it seems reasonable to assume that such definitions will similarly have less impact on ICC estimates than on physical activity estimates themselves. All estimates of ICCs were between 0.04–0.08 with overlapping confidence intervals, suggesting that accelerometer-measured ICCs are fairly consistency across a range of ages and settings. This therefore suggests that the results presented here may be useful more widely, for example in other UK nations and other high income countries that have similar physical activity provision within schools. In such cases, we suggest that in the absence of more specific estimates, an ICC of 0.10 for weekday MVPA could be used for sample size calculations, based on the upper 95% CI bounds to reduce the risk of underpowering a study. Corresponding estimates for sedentary time are thus 0.05 -0.06 for ages 6–11 (English primary schools) and 0.02–0.03 for ages 11–16 (English secondary schools).
When considering boys and girls separately, in primary schools, both genders had similar ICCs for weekday MVPA of 0.08–0.12. Note that these ICCs are a little higher than the estimate of 0.07–0.08 for boys and girls combined. This apparently counter-intuitive result is because ICCs are relative measures that depend on the total variation denominator, which differs between genders, with higher individual variability for boys than for girls. In secondary schools, ICCs were lower for boys, but for girls they remained at similar levels to primary school. Girls typically engage in less physical activity than boys especially in adolescence [31], and so the ICC will be higher as the total variation is lower in a less active population. These results highlight the importance of using ICCs that are closest to the intended population in planning a study, especially when considering subgroups, where ICCs for combined groups may differ due to differences in total variation. For example, a study involving Year 7 girls only using the ICC for girls would require 60 schools for 80% power. However, if an ICC of 0.04 based on boys and girls together is used, the required number of schools is estimated at only 42, which would result in an underpowered study at 65% power.
It is always important that studies are adequately powered, but in public health underpowered studies may risk missing interventions that have relatively small individual effects, but have the potential for much greater impact at population level. Our examples of sample size calculation suggest that relatively small differences of 0.02 in the ICC can increase the number of schools required by around 20% (corresponding to an increase of 14–18 for a two-arm cluster RCT for an effect size of 5 min of MVPA). This is particularly an issue for school-based trials of physical activity interventions, as recruiting the additional schools this requires is resource-intensive. Developing interventions in this area is very important as we know that children’s physical activity patterns have changed since the COVID-19 pandemic [50,51,52,53], but it is equally important that such interventions are properly evaluated. The sensitivity of school sample sizes to relatively small differences in the ICC means that considering a plausible range of ICCs can lead to much larger studies than in other settings, which may have funding implications for the amount and availability of sufficient funding to test interventions at the necessary scale. While an increase in ICC can be offset to some extent by increasing the number of pupils recruited per school, the eligible population is restricted, especially in primary schools, and increases in power are limited after around 50 pupils per school. However, using ICCs based on the wrong age group, population or from non-physical activity outcomes can also potentially result in an under-powered study. For example, from our estimates, a primary school study of Y5 pupils should use an ICC of 0.08 for weekday MVPA, with 82 schools required for a two-arm cluster RCT with 80% power. If, instead, an ICC of 0.04 is used, based on secondary schools MVPA across the whole week, the calculated sample size is 56 schools, with true power 64%. Using ICC estimates of self-reported physical activity outcomes from the literature [13, 21, 22] of around 0.02 will reduce this even further to 44 schools and 53% power. The adequate powering of studies is important in terms of moving the evidence for effective physical activity strategies in children and adolescences forward [33], and so we recommend that a range of plausible ICC values should be explored, to assess the sensitivity of the estimated sample sizes to different values, such as using the upper 95% bound as well as the point estimate, as in our example.
There are a number of observations that we can make with respect to the efficient design of cluster-based trials of physical activity outcomes in children and adolescence. Designs which involve repeated measurements increase the power of the study, or reduce the number of schools required. Note that when designing a cluster RCT adjusted for baseline, it is important to use both ICC and total variation estimates that have also been adjusted for baseline, and studies that report ICCs should be clear about whether any adjustment has been made. While the ICCs adjusted for baseline are only slightly smaller than unadjusted ICCs in our results, repeated measurements on the same children reduce the total variation and so fewer schools are needed for a study with the same power. This study design implicitly takes account of the autocorrelation between successive measurements, and is related to including the CAC and IAC in the stepped wedge design [5]. An advantage of the stepped wedge design is that it can be used for both cross-sectional and cohort samples as it does not require the same pupils to be measured [4]. However, it is more complex to design, run and analyse, and while the cohort design has substantial benefits in terms of required sample sizes, the numbers presented in Table 4 assume that repeated measurements at baseline and each step are achieved for all pupils. In practice, repeated measures may result in lower pupil numbers, especially as the number of steps increases. Accurate estimates of power for the stepped wedge design should also account for the CAC and IAC, with the former particularly important, as some simplified models for sample size estimation assume a CAC of 1 [54], which will result in under-powering of the study [4]. While we were able to produce reasonable estimates for the IAC, the estimate of the CAC was still not precise even when pooling schools from multiple studies. Models and sample size formulae have been developed to consider CAC correlation structures that decay over time [55]. Unfortunately, our analysis was unable to provide accurate or precise estimates of the CAC under a year, due to limited data and seasonality in physical activity outcomes. Our results indicate that after one year, any further decay is weak, with the CAC levelling at around 0.5–0.6, reflecting that schools are more consistent over time than individuals. While we are unable to provide reliable estimates for shorter-term CACs, we suggest that a range of plausible values are considered at the design stage. However, care should be taken in using complex correlation structures in sample size calculations for evaluating children’s physical activity (although such models may be useful in analysis) as this might artificially increase power due to overconfidence in estimates.
The primary focus of this paper is on estimating ICCs for use in sample size estimation. However, unlike clinical or primary care settings, where clustering is often a nuisance factor related to the data collection process, in physical activity and many other public health contexts, the clustering is a direct feature of physical activity and even the intervention itself. As a measure of clustering, the ICC tells us about the extent to which schools (and/or classes), and school-related factors, explain between-child variation in physical activity. Thus school factors, such as playground equipment, active travel, PE provision and active after-school clubs [56, 57], play more of a role in primary schools than in secondary schools. Similarly, the higher ICC for girls in secondary school may reflect that girls do comparatively little physical activity outside the school context and so the influence of schools is greater, even though they typically engage in less physical activity than boys. This makes schools potentially good targets for developing interventions, although it is worth noting that the largest source of variation between children is still due to individual factors [57]. Unfortunately we were unable to separate school-level and class-level variability, and so the reported ICCs combine both sources of variation; it is likely that a substantial proportion of the observed school-level clustering is at the class level. Understanding different levels of variation can help determine whether interventions should be focused on group or individual level, similar to applications in occupational health [58]. However, it also makes interventions and their evaluation more complex, and instead of just estimating ICCs we need to properly understand when and how clustering affects physical activity outcomes, especially when dealing with a complex intervention that may affect the ICC itself.
Strengths and limitations
This paper has a number of strengths. We have combined data on over 500 schools, which has allowed more precise estimates of ICCs and autocorrelations than have been previously reported. Combining data from seven different studies covering a wide age range of ages 6–16 years, and has enabled us to explore patterns by age and gender. The mixed effects model used to estimate the ICCs is consistent with that used for sample size formulae and analysis of the various cluster-based designs considered. We were also able to produce estimates of the autocorrelations, CAC and IAC. However, estimates of autocorrelation were limited in their ability to explore short-term follow-ups of less than a year, and in particular estimates of the CAC were still imprecise despite the large sample sizes. Although the studies covered a wide age range, each age group was often dominated by a single study, which means that observed patterns by age may be related to differences in studies rather than school year group. As this was a secondary analysis, we do not have any information on missing data beyond no value being provided in the dataset. Accelerometer processing criteria differed between studies, in terms of wear time definitions, criteria for valid days and number of days included in the study, which may affect results, although our limited sensitivity analysis suggests that unlike physical activity estimates themselves, ICC estimates are reasonably robust to these differences. We were also unable to look at ICCs for during school hours only, or to explore class-level variability. Finally, we intentionally restricted to England-based studies as differences in school systems may affect clustering. While estimates appear to be consistent across the different ages considered here and with values reported elsewhere, the extent to which these ICCs are generalisable to other countries should be explored further.
Conclusions
Adequately powered studies are important to move forward the evidence for effective physical activity strategies. We have provided a comprehensive set of estimates of school-level ICCs and autocorrelations for accelerometer-measured physical activity in children and adolescents in England which can be used to plan new school-based cluster trials of physical activity interventions in schools. Estimates of the ICC were fairly consistent across a range of ages and settings, with estimates for weekday MVPA between 0.04 and 0.07 depending on age. It is important to use estimates appropriate to the study design, and that match the intended study population as closely as possible.
Availability of data and materials
The ICAD is open for data requests as a supported access resource. Information regarding the application process to access the data can be found at https://www.mrc-epid.cam.ac.uk/research/studies/icad/. Anonymised versions of the data from the Action 3:30 project have been deposited in the University of Bristol Research Data Repository (http://data.bris.ac.uk/data/). Data from the Active Lives Children and Young People Survey is available from the UK Data Service (SN 8854: https://doi.org/10.5255/UKDA-SN-8854–2). Data from B-Proact1v, AFLY5 and CHASE are available from the study investigators on reasonable request; see study citations for the relevant contact details.
Abbreviations
- AFLY5:
-
Active for Life Year 5
- ALCYP:
-
Active Lives Children and Young People
- ALSPAC:
-
Avon Longitudinal Study of Parents and Children
- CAC:
-
Cluster autocorrelation
- CHASE:
-
Child Heart And health Study in England
- ICAD:
-
International Children’s Accelerometry Database
- IAC:
-
Individual autocorrelation
- ICC:
-
Intra-cluster correlation coefficient
- MVPA:
-
Moderate-to-vigorous physical activity
- PEACH:
-
Personal and Environmental Associations with Children's Health
- RCT:
-
Randomised controlled trial
- SPEEDY:
-
Sport, Physical Activity and Eating Behaviour: Environmental Determinants in Young people
References
Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, Boyd KA, Craig N, French DP, McIntosh E, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. 2021;374:n2061.
Hayes RJ, Moulton LH. Cluster randomised trials. 2nd ed. Florida: CRC Press; 2017.
Eldridge S, Kerry SM. A practical guide to cluster randomised trials in health services research. London: Arnold; 2012.
Hooper R, Teerenstra S, de Hoop E, Eldridge S. Sample size calculation for stepped wedge and other longitudinal cluster randomised trials. Stat Med. 2016;35(26):4718–28.
Hooper R, Forbes A, Hemming K, Takeda A, Beresford L. Analysis of cluster randomised trials with an assessment of outcome at baseline. BMJ. 2018;360:k1121.
Murray DM. Influential methods reports for group-randomized trials and related designs. Clin Trials. 2022;19(4):353–62.
Eldridge SM, Ukoumunne OC, Carlin JB. The intra-cluster correlation coefficient in cluster randomized trials: a review of definitions. Int Stat Rev. 2009;77(3):378–94.
Kerry SM, Bland JM. The intracluster correlation coefficient in cluster randomisation. BMJ. 1998;316:1455.
Baio G, Copas A, Ambler G, Hargreaves J, Beard E, Omar RZ. Sample size calculation for a stepped wedge trial. Trials. 2015;16:354.
Adams G, Gulliford MC, Ukoumunne OC, Eldridge S, Chinn S, Campbell MJ. Patterns of intra-cluster correlation from primary care research to inform study design and analysis. J Clin Epidemiol. 2004;57(8):785–94.
Murray DM, Blistein JL. Methods to reduce the impact of intraclass correlation in group-randomized trials. Eval Rev. 2003;27(1):79–103.
Gulliford MC, Ukoumunne OC, Chinn S. Components of variance and intraclass correlations for the design of community-based surveys and intervention studies: data from the health survey for England 1994. Am J Epidemiol. 1999;149(9):876–83.
Hale DR, Patalay P, Fitzgerald-Yau N, Hargreaves DS, Bond L, Gorzig A, Wolpert M, Stansfeld SA, Viner RM. School-level variation in health outcomes in adolescence: analysis of three longitudinal studies in England. Prev Sci. 2014;15(4):600–10.
Shackleton N, Hale D, Bonell C, Viner RM. Intraclass correlation values for adolescent health outcomes in secondary schools in 21 European countries. SSM Popul Health. 2016;2:217–25.
Korevaar E, Kasza J, Taljaard M, Hemming K, Haines T, Turner EL, Thompson JA, Hughes JP, Forbes AB. Intra-cluster correlations from the CLustered OUtcome Dataset bank to inform the design of longitudinal cluster trials. Clin Trials. 2021;18(5):529–40.
Martin J, Girling A, Nirantharakumar K, Ryan R, Marshall T, Hemming K. Intra-cluster and inter-period correlation coefficients for cross-sectional cluster randomised controlled trials for type-2 diabetes in UK primary care. Trials. 2016;17:402.
Eldridge SM, Costelloe CE, Kahan BC, Lancaster GA, Kerry SM. How big should the pilot study for my cluster randomised trial be? Stat Methods Med Res. 2016;25(3):1039–56.
Parker K, Nunns M, Xiao Z, Ford T, Ukoumunne OC. Characteristics and practices of school-based cluster randomised controlled trials for improving health outcomes in pupils in the United Kingdom: a methodological systematic review. BMC Med Res Methodol. 2021;21(1):152.
UK Chief Medical Officers. UK Chief Medical Officers’ Physical Activity Guidelines. London: Department of Health and Social Care; 2019.
Chaput JP, Willumsen J, Bull F, Chou R, Ekelund U, Firth J, Jago R, Ortega FB, Katzmarzyk PT. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5–17 years: summary of the evidence. Int J Behav Nutr Phys Act. 2020;17(1):141.
Murray D, Catellier DJ, Hannan PJ, Treuth MS, Stevens J, Schmitz KH, Rice JC, Conway TL. School-level intraclass correlation for physical activity in adolescent girls. Med Sci Sports Exerc. 2004;36:876–82.
Hobin E, Leatherdale S, Manske S, Dubin J, Elliott S, Veugelers P. A multilevel examination of factors of the school environment and time spent in moderate to vigorous physical activity among a sample of secondary school students in grades 9–12 in Ontario, Canada. Int J Public Health. 2012;57(4):699–709.
Harvey A, Faulkner G, Giangregorio L, Leatherdale ST. An examination of school- and student-level characteristics associated with the likelihood of students’ meeting the Canadian physical activity guidelines in the COMPASS study. Can J Public Health. 2017;108(4):348–54.
Steenholt CB, Pisinger VSC, Danquah IH, Tolstrup JS. School and class-level variations and patterns of physical activity: a multilevel analysis of Danish high school students. BMC Public Health. 2018;18(1):255.
Faulkner G, Zeglen L, Leatherdale S, Manske S, Stone M. The relationship between school physical activity policy and objectively measured physical activity of elementary school students: a multilevel model analysis. Arch Public Health. 2014;72(1):20.
Kristensen PL, Olesen LG, Ried-Larsen M, Grontved A, Wedderkopp N, Froberg K, Andersen LB. Between-school variation in physical activity, aerobic fitness, and organized sports participation: a multi-level analysis. J Sports Sci. 2013;31(2):188–95.
Salway R, Emm-Collison L, Sebire SJ, Thompson JL, Lawlor DA, Jago R. A multilevel analysis of neighbourhood, school, friend and individual-level variation in primary school children’s physical activity. Int J Environ Res Public Health. 2019;16(24):4889.
Fairclough SJ, Beighle A, Erwin H, Ridgers ND. School day segmented physical activity patterns of high and low active children. BMC Public Health. 2012;12:406.
Gomes TN, dos Santos FK, Santos D, Pereira S, Chaves R, Katzmarzyk PT, Maia J. Correlates of sedentary time in children: a multilevel modelling approach. BMC Public Health. 2014;14:890.
Mantjes JA, Jones AP, Corder K, Jones NR, Harrison F, Griffin SJ, van Sluijs E. School related factors and 1yr change in physical activity amongst 9–11 year old English schoolchildren. Int J Behav Nutr Phys Act. 2012;9:153.
Fairclough SJ, Rowlands AV, Del Pozo CB, Crotti M, Foweather L, Graves LEF, Hurter L, Jones O, MacDonald M, McCann DA, et al. Reference values for wrist-worn accelerometer physical activity metrics in England children and adolescents. Int J Behav Nutr Phys Act. 2023;20(1):35.
Sherar LB, Griew P, Esliger DW, Cooper A, Ekelund U, Judge K, Riddoch CJ. International children’s accelerometry database (ICAD): design and methods. BMC Public Health. 2011;11:485.
Jago R, Salway R, House D, Beets M, Lubans DR, Woods C, de Vocht F. Rethinking children’s physical activity interventions at school: a new context-specific approach. Front Public Health. 2023;11:1149883.
Boyd A, Golding J, Macleod J, Lawlor DA, Fraser A, Henderson J, Molloy L, Ness A, Ring S, Davey Smith G. Cohort profile: the ‘children of the 90s’–the index offspring of the Avon Longitudinal Study of Parents and Children. Int J Epidemiol. 2013;42(1):111–27.
Fraser A, Macdonald-Wallis C, Tilling K, Boyd A, Golding J, Davey-Smith G, Henderson J, Macleod J, Molloy L, Ness A, et al. Cohort profile: the Avon Longitudinal Study of Parents and Children: ALSPAC mothers cohort. Int J Epidemiol. 2013;42:97–110.
van Sluijs EM, Skidmore PM, Mwanza K, Jones AP, Callaghan AM, Ekelund U, Harrison F, Harvey I, Panter J, Wareham NJ, et al. Physical activity and dietary behaviour in a population-based sample of British 10-year old children: the SPEEDY study (Sport, Physical activity and Eating behaviour: environmental Determinants in Young people). BMC Public Health. 2008;8: 388.
Page A, Cooper AR, Griew P, Jago R. Independent mobility, perceptions of the built environment and children’s participation in play, active travel and structured exercise and sport: the PEACH Project. Int J Behav Nutr Phys Act. 2010;7:17.
Jago R, Solomon-Moore E, Macdonald-Wallis C, Sebire SJ, Thompson JL, Lawlor DA. Change in children’s physical activity and sedentary time between Year 1 and Year 4 of primary school in the B-PROACT1V cohort. Int J Behav Nutr Phys Act. 2017;14:33.
Jago R, Salway R, Emm-Collison L, Sebire SJ, Thompson JL, Lawlor DA. Association of BMI category with change in children’s physical activity between ages 6 and 11 years: a longitudinal study. Int J Obes. 2020;44:104–13.
Jago R, Sebire SJ, Davies B, Wood L, Edwards MJ, Banfield K, Fox KR, Thompson JL, Powell JE, Mongomery AA. Randomised feasibility trial of a teaching assistant led extracurricular physical activity intervention for 9 to 11 year olds: action 3:30. Int J Behav Nutr Phys Act. 2014;11:114.
Lawlor D, Jago R, Noble SM, Chittleborough C, Campbell R, Mytton J, Howe LD, Peters TJ, Kipping R. The Active for Life Year 5 (AFLY5) school based cluster randomised controlled trial: study protocol for a randomized controlled trial. Trials. 2011;12:181.
Anderson EL, Howe LD, Kipping RR, Campbell R, Jago R, Noble SM, Wells S, Chittleborough C, Peters TJ, Lawlor DA. Long-term effects of the Active for Life Year 5 (AFLY5) school-based cluster-randomised controlled trial. BMJ Open. 2016;6(11):e010957.
Owen CG, Nightingale CM, Rudnicka AR, Sattar N, Cook DG, Ekelund U, Whincup PH. Physical activity, obesity and cardiometabolic risk factors in 9- to 10-year-old UK children of white European, South Asian and black African-Caribbean origin: the Child Heart And health Study in England (CHASE). Diabetologia. 2010;53(8):1620–30.
Jago R, Bailey R. Ethics and paediatric exercise science: issues and making a submission to a local ethics and research committee. J Sports Sci. 2001;19:527–35.
Sport England. Active lives children and young people survey, Academic Year 2018–19. UK: Sport England; 2019.
Sport England. Active lives children and young people survey, 2018–2019. [data collection]. UK Data Service; 2024.
StataCorp. Stata statistical software: release 17. College Station: StataCorp LLC; 2021.
Ver Hoef JM. Who invented the delta method? Am Stat. 2012;66(2):124–7.
Metcalf B, Henley W, Wilkin T. Effectiveness of intervention on physical activity of children: systematic review and meta-analysis of controlled trials with objectively measured outcomes (EarlyBird 54). BMJ. 2012;345:e5888.
Salway R, Foster C, de Vocht F, Tibbitts B, Emm-Collison L, House D, Williams JG, Breheny K, Reid T, Walker R, et al. Accelerometer-measured physical activity and sedentary time among children and their parents in the UK before and after COVID-19 lockdowns: a natural experiment. Int J Behav Nutr Phys Act. 2022;19(1):51.
Jago R, Salway R, House D, Walker R, Emm-Collison L, Sansum K, Breheny K, Reid T, Churchward S, Williams JG, et al. Short and medium-term effects of the COVID-19 lockdowns on child and parent accelerometer-measured physical activity and sedentary time: a natural experiment. Int J Behav Nutr Phys Act. 2023;20(1):42.
Walker R, House D, Salway R, Emm-Collison L, Hollander LE, Sansum K, Breheny K, Churchward S, Williams JG, de Vocht F, et al. The new normal for children’s physical activity and screen viewing: a multi-perspective qualitative analysis of behaviours a year after the COVID-19 lockdowns in the UK. BMC Public Health. 2023;23(1):1432.
Walker R, Salway R, House D, Emm-Collison L, Breheny K, Sansum K, Churchward S, Williams JG, Vocht FD, Hollingworth W, Jago R. The status of active after-school clubs among primary school children in England (UK) after the COVID-19 lockdowns: implications for policy and practice. Int J Behav Nutr Phys Act. 2023;20(1):120.
Hussey MA, Hughes JP. Design and analysis of stepped wedge cluster randomized trials. Contemp Clin Trials. 2007;28(2):182–91.
Kasza J, Hemming K, Hooper R, Matthews J, Forbes AB. Impact of non-uniform correlation structure on sample size and power in multiple-period cluster randomised trials. Stat Methods Med Res. 2019;28(3):703–16.
Emm-Collison L, Salway R, Matthews J, Reid T, Jago R. Associations between the built environment, policies and curriculum in schools and primary school children’s physical activity. Wellcome Open Res. 2023;8:85.
Salway R, House D, Walker R, Emm-Collison L, Breheny K, Sansum K, Williams J, Hollingworth W, de Vocht F, Jago R. School-level variation in children’s moderate to vigorous intensity physical activity before and after COVID-19: a multilevel model analysis’. NIHR Public Health Res. (In press).
Kromhout H, Symanski E, Rappaport SM. A comprehensive evaluation of within- and between-worker components of occupational exposure to chemical agents. Ann Occup Hyg. 1993;37(3):253–70.
Acknowledgements
We would like to thank all participants and funders of the original studies that contributed data to ICAD. We gratefully acknowledge the past contributions of Prof Chris Riddoch, Prof Ken Judge, Prof Ashley Cooper and Dr Pippa Griew to the development of ICAD. The ICAD was made possible thanks to the sharing of data from the following contributors (study name): Prof LB Andersen, Faculty of Teacher Education and Sport, Western Norway University of Applied Sciences, Sogndal, Norway (Copenhagen School Child Intervention Study (CoSCIS)); Prof S Anderssen, Norwegian School for Sport Science, Oslo, Norway (European Youth Heart Study (EYHS), Norway); Prof G Cardon, Department of Movement and Sports Sciences, Ghent University, Belgium (Belgium Pre-School Study); Centers for Disease Control and Prevention (CDC), National Center for Health Statistics (NCHS), Hyattsville, MD USA (National Health and Nutrition Examination Survey (NHANES)); Dr R Davey, Centre for Research and Action in Public Health, University of Canberra, Australia (Children’s Health and Activity Monitoring for Schools (CHAMPS)); Dr P Hallal, Postgraduate Program in Epidemiology, Federal University of Pelotas, Brazil (1993 Pelotas Birth Cohort); Prof R Jago, Centre for Public Health, University of Bristol, UK (Personal and Environmental Associations with Children's Health (PEACH)); Prof S Kriemler, Epidemiology, Biostatistics and Prevention Institute, University of Zürich, Switzerland (Kinder-Sportstudie (KISS)); Dr S Kwon, Feinberg School of Medicine, Northwestern Medicine, Northwestern University, Chicago, Illinois, US (Iowa Bone Development Study); Dr N Møller, University of Southern Denmark, Odense, Denmark (European Youth Heart Study (EYHS), Denmark); Dr K Northstone, Population Health Sciences, Bristol Medical School, University of Bristol, UK (Avon Longitudinal Study of Parents and Children (ALSPAC)); Prof R Pate, Department of Exercise Science, University of South Carolina, Columbia, US (Physical Activity in Pre-school Children (CHAMPS-US) and Project Trial of Activity for Adolescent Girls (Project TAAG)); Dr JJ Puder, Service of Endocrinology, Diabetes and Metabolism, Centre Hospitalier Universitaire Vaudois, University of Lausanne, Switzerland (Ballabeina Study); Prof J Reilly, Physical Activity for Health Group, School of Psychological Sciences and Health, University of Strathclyde, Glasgow, UK (Movement and Activity Glasgow Intervention in Children (MAGIC)); Prof J Salmon, Institute for Physical Activity and Nutrition (IPAN), School of Exercise and Nutrition Sciences, Deakin University, Geelong, Australia (Children Living in Active Neigbourhoods (CLAN) & Healthy Eating and Play Study (HEAPS)); Prof LB Sardinha, Exercise and Health Laboratory, Faculty of Human Movement, Universidade de Lisboa, Lisbon, Portugal (European Youth Heart Study (EYHS), Portugal); Dr EMF van Sluijs, MRC Epidemiology Unit, University of Cambridge, UK (Sport, Physical activity and Eating behaviour: Environmental Determinants in Young people (SPEEDY)). We are extremely grateful to all the families who took part in the ALSPAC study, the midwives for their help in recruiting them, and the whole ALSPAC team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists and nurses. We also thank all those who took part in the Action 3:30, AFLY5, BProact1v, CHASE, PEACH and SPEEDY studies.
International Children’s Accelerometry Database (ICAD) Collaborators
Dr Andrew Atkin7, Prof Ulf Ekelund8, Dr Dale Esliger9, Dr Bjorge H Hansen8, Dr Lauren Sherar9, Dr Esther van Sluijs6
7Faculty of Medicine and Heath Sciences, University of East Anglia, East Anglia, United Kingdom
8Department of Sport Medicine, Norwegian School of Sport Sciences, Oslo, Norway
9School of Sports, Exercise and Health Sciences, Loughborough University, Loughborough, United Kingdom
Funding
This project is funded by UKRI REF EP/X023508/1 (Frontier Research Grant). RJ is partly supported by the National Institute for Health and Care Research Bristol Biomedical Research Centre and the National Institute for Health and Care Research Applied Research Collaboration West (NIHR ARC West). FdV is partly supported by the National Institute for Health and Care Research Applied Research Collaboration West (NIHR ARC West). AP is supported by the National Institute for Health and Care Research Bristol Biomedical Research Centre (Bristol BRC). EvS is supported by the Medical Research Council [grant number MC_UU_00006/5].
Action 3:30 was funded by the National Prevention Research Initiative which is supported by Alzheimer’s Research Trust; Alzheimer’s Society; Biotechnology and Biological Sciences Research Council; British Heart Foundation; Cancer Research UK; Chief Scientist Office, Scottish Government Health Directorate; Department of Health; Diabetes UK; Economic and Social Research Council; Health and Social Care Research and Development Division of the Public Health Agency (HSC R&D Division); Medical Research Council; The Stroke Association; Wellcome Trust; Welsh Assembly Government; and World Cancer Research Fund (MRC reference—MR/J000191/1).
The AFLY5 RCT was funded by the UK National Institute for Health Research (NIHR) Public Health Research Programme (09/3005/04).
CHASE was supported by grants from the Wellcome Trust (068362/Z/02/Z), the British Heart Foundation (PG/06/003) and by the National Prevention Research Initiative (NPRI).
The B-Proact1v study was funded by grants from the British Heart Foundation (ref PG/11/51/28986 and SP 14/4/31123).
The UK Medical Research Council and Wellcome (Grant reference: 217065/Z/19/Z) and the University of Bristol provide core support for ALSPAC. A comprehensive list of grants funding is available on the ALSPAC Web site.
PEACH was supported by the National Prevention Research Initiative [G0501311] and World Cancer Research Fund (WCRF UK).
The SPEEDY study was funded by the National Prevention Research Initiative http://www.npri.org.uk, consisting of the following Funding Partners: British Heart Foundation; Cancer Research UK; Department of Health; Diabetes UK; Economic and Social Research Council; Medical Research Council; Research and Development Office for the Northern Ireland Health and Social Services; Chief Scientist Office, Scottish Executive Health Department; Welsh Assembly Government and World Cancer Research Fund. The study was additionally supported by the Medical Research Council [MC_UU_12015/3; MC_UU_12015/7].
The ICAD data pooling project was funded through a grant from the National Prevention Research Initiative (G0701877) (http://www.mrc.ac.uk/research/initiatives/national-prevention-research-initiative-npri/), with funding partners: British Heart Foundation; Cancer Research UK; Department of Health; Diabetes UK; Economic and Social Research Council; Medical Research Council; Research and Development Office for the Northern Ireland Health and Social Services; Chief Scientist Office; Scottish Executive Health Department; The Stroke Association; Welsh Assembly Government and World Cancer Research Fund. The ICAD was additionally supported by the Medical Research Council [MC_UU_12015/3; MC_UU_12015/7], The Research Council of Norway (249932/F20), Bristol University, Loughborough University and Norwegian School of Sport Sciences.
The views and opinions expressed herein are those of the authors and do not necessarily reflect those of any funder, including UKRI, NIHR or the Department of Health and Social Care. Funders were not involved in data analysis, data interpretation, or writing of the paper.
Author information
Authors and Affiliations
Consortia
Contributions
The paper was conceived by RJ and RS. RS planned and undertook the statistical analyses and wrote the first draft. RJ is the study Principal Investigator and RJ, RK, CGO, MTH, KN and EvS contributed data from original studies. FdV, DH, AP and RW commented on early drafts. All authors reviewed and revised the paper and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All studies in this paper were approved by local ethics committees, and informed parental consent was obtained for all participants. Ethical approval was obtained from the School for Policy Studies Research Ethics Committee at the University of Bristol for Action 3:30, PEACH and B-Proact1v; from the University of Bristol Faculty of Medicine and Dentistry Committee for Ethics for AFLY5; from the relevant Multi-Centre Research Ethics Committee for CHASE; from the ALSPAC Ethics and Law Committee and the Local Research Ethics Committees (http://www.bristol.ac.uk/alspac/researchers/research-ethics/) for ALSPAC; and the University of East Anglia Research Ethics Committee for SPEEDY.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Salway, R., Jago, R., de Vocht, F. et al. School-level intra-cluster correlation coefficients and autocorrelations for children’s accelerometer-measured physical activity in England by age and gender. BMC Med Res Methodol 24, 179 (2024). https://doi.org/10.1186/s12874-024-02290-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12874-024-02290-7