
Abstract
Background
Physical activity and a healthy diet are important in helping to maintain mobility with aging. This umbrella review aims to identify group-based physical activity and/or nutrition interventions for community-dwelling older adults that improve mobility-related outcomes.
Methods
Five electronic databases (MEDLINE, Embase, CINAHL, Cochrane CENTRAL, Sociological Abstracts) were searched from inception to December 2021. Eligibility criteria included systematic reviews exploring the effectiveness of physical activity or structured exercise, alone or combined with nutrition interventions on mobility-related outcomes (aerobic capacity, physical function, balance, falls/safety, muscle strength, health-related quality of life/wellbeing). Interventions must have been delivered in a group setting to community-dwelling older adults aged 55+. Two reviewers independently performed eligibility screening, critical appraisal (using AMSTAR 2) and data extraction. The GRADE approach was used to reflect the certainty of evidence based on the size of the effect within each mobility-related outcome category. Older adult/provider research partners informed data synthesis and results presentation.
Results
In total, 62 systematic reviews (1 high, 21 moderate, 40 low/critically low quality) were identified; 53 included physical activity only, and nine included both physical activity and nutritional supplements. No reviews included nutrition interventions alone. Combined aerobic/resistance, general physical activity, and mind-body exercise all improved physical function and balance (moderate-high certainty). Aerobic/resistance training improved aerobic capacity (high certainty). Resistance training and general physical activity improved muscle strength (moderate certainty). Aerobic/resistance training and general physical activity are likely to reduce falls among older adults (moderate certainty). There was no evidence of benefit for nutritional supplementation with physical activity.
Conclusions
Group-based physical activity interventions that combine aerobic and resistance, general PA and mind-body exercise can improve measures of mobility in community-dwelling older adults. We found no reviews focused on nutrition only, highlighting a gap in the literature.
Similar content being viewed by others

Background
Mobility is a multifaceted construct, influenced by a range of modifiable (e.g., physical, cognitive, psychosocial, financial) and non-modifiable (e.g., environmental, gender, cultural, and biographical) factors [1]. A comprehensive view of mobility reflects one’s ability to move within their immediate home environment and the broader community [1]. Reductions in mobility and the ability to carry out activities of daily living are common with aging and are recognized precursors to frailty, falls, hospitalization, and death [2,3,4]. Although some factors influencing mobility among older adults are non-modifiable, several modifiable risk factors have been identified, including physical function, balance, muscular strength, aerobic endurance, and psychosocial wellbeing [5, 6]. Nutritional risk factors (e.g., inadequate food/fluid intake to support optimal physical functioning) are also predictive of reduced mobility in older adults [5, 7].
The beneficial effect of physical activity (PA) and improved diet quality on modifiable mobility-related outcomes has been widely demonstrated; however, inactivity and malnutrition continue to affect the well-being and mobility of older adults [8,9,10,11,12]. Community-based physical activity and nutrition programs delivered in group settings can address both the physical and psychosocial aspects of mobility, promoting a sense of belonging which aids in long-term adherence [13, 14]. The Enhancing physical and community MoBility in OLDEr adults with health inequities using commuNity co-design (EMBOLDEN) trial is a multi-year program of research from XX University in [City, Country] (Trial ID: NCT05008159) [15]. The transdisciplinary team of EMBOLDEN researchers, older adults and community partners have used community-based co-design to integrate local community needs, preferences, and resources with high-quality scientific evidence to develop a mobility-enhancing program that supports physical activity, healthy eating, and social participation among older adults.
Several systematic reviews have been published exploring a broad range of PA and/or nutrition interventions for older adults, making it challenging to bring together the best scientific evidence to inform program design. Umbrella reviews provide a rigorous methodology for synthesizing evidence from multiple existing systematic reviews [16], and may be particularly useful for a phenomenon such as mobility given the wide variety of interventions and uncertainty as to which interventions are more effective when delivered individually or in combination and within different populations and/or settings. To date, two umbrella reviews have reported the effectiveness of exercise interventions in pre-frail, frail, or sarcopenic older adults [17, 18], and one umbrella review has described the impact of nutritional interventions for community-dwelling older adults on body composition [19]. Given the lack of recent, relevant synthesized evidence to meet our needs, our team undertook this umbrella review to help inform intervention design and provide a foundation for the EMBOLDEN research program. This umbrella review aims to synthesize evidence from existing systematic reviews regarding the effectiveness of group-based PA and/or nutrition interventions to improve measures of mobility in community-dwelling older adults.
Methods
This review was conducted following the Joanna Briggs Institute (JBI) guidance for umbrella reviews [16], and was registered with PROSPERO (CRD42020141352). Although originally conceptualized as a systematic review, upon initiation of screening it was determined that many systematic reviews existed, and an umbrella review was most appropriate.
Search strategy
A trained librarian conducted a search of MEDLINE, Embase, CINAHL, Cochrane CENTRAL, and Sociological Abstracts from inception to December 2021 (Additional file 1). Searches were limited to systematic reviews/meta-analyses and randomized controlled trials (RCTs) published in English.
Study selection
Citations were imported into DistillerSR (Evidence Partners, Ottawa, Canada) and duplicates were removed. Citations were reviewed by two independent reviewers using pre-determined criteria. At the title/abstract level, a study must have been selected by one reviewer for inclusion, while exclusion required two reviewers to agree. At the full-text level, disagreements were resolved through discussion by two reviewers, with input from a third team member as needed.
Eligibility criteria
Types of studies
Systematic reviews (narrative summary, meta-analysis, or network meta-analysis) of interventions were eligible. Scoping or narrative reviews that did not include critical appraisal of primary studies were excluded. Eligible reviews could include RCTs and non-randomized intervention studies, however, at least 80% of single studies included must have been interventions (i.e., not descriptive, qualitative, or observational). To balance feasibility, while ensuring we captured the most recent and relevant intervention data, we chose to include only reviews that were published in 2010 or later; although eligible reviews did include single studies that were conducted prior to 2010.
Types of participants
Eligible systematic reviews included studies involving community-dwelling older adults. Reviews were included if the pooled mean age or inclusion criteria identified an age of ≥ 55 years. If this information was not available, at least 70% of included studies must have reported a mean sample age of ≥ 55 years. Reviews in which studies were selected based on a specific health or disease status (e.g., cancer, sarcopenia) were excluded. In reviews that did not restrict by disease status, 70% of included studies must have been conducted in a general sample of older adults. The choice of 70% was intended to include reviews in which the majority of included studies were relevant to the general population; most studies were either well above or well below this threshold.
Interventions
Eligible reviews must have included single studies of any PA (any movement resulting in energy expenditure), structured exercise (planned and repetitive movements), and/or nutrition intervention (e.g., education, counselling, dietary changes and/or supplementation) that could reasonably be delivered in a group-based setting [20]. Exercise or PA interventions were categorized as: aerobic exercise, resistance exercise, combined aerobic and resistance exercise, general physical activity (reviews in which a variety of types of physical activity and/or exercise were synthesized together), mind-body exercise (e.g., Tai Chi, yoga, Pilates), and dance.
Context
Single studies within eligible reviews must have been delivered in a community setting. Reviews that focused exclusively on interventions delivered in hospitals, rehabilitation centers, long-term care homes, or clinics were excluded. When the reviews did not set inclusion criteria by setting, at least 70% of included single studies were required to be community-based.
Outcomes
Reviews must have synthesized (narratively or via meta-analysis) outcomes related to physical or community mobility. These outcomes were broadly classified into six domains based on modifiable risk factors related to mobility that could be reasonably addressed through PA and/or nutrition interventions, as described above. The mobility-related outcomes explored include aerobic capacity, physical function, balance, falls/safety, muscular strength, and self-reported mental wellbeing/quality of life. Reviews that focused exclusively on cognitive function or body composition were excluded. These criteria were not part of our original protocol as registered in PROSPERO but added at the full text screening level as the goals of these interventions and associated outcomes were quite distinct.
Assessment of methodological quality
Eligible reviews were critically appraised using A MeaSurement Tool to Assess systematic Reviews (AMSTAR 2) [21]. AMSTAR 2 was completed independently by two reviewers, with conflicts resolved through discussion or the input of a third reviewer, as needed. Following consensus, results were entered into the online AMSTAR checklist, which provides an assessment of overall quality as critically low, low, moderate, or high based on seven critical domains [22].
Data extraction
Data were extracted by two independent reviewers using a standardized form. Disagreements were resolved through discussion or by a third reviewer. Data were extracted related to review methodology (e.g., sources searched, publication date range, methodological quality of included studies, noted limitations) and details of included studies (e.g., study designs, participant characteristics, intervention descriptions, setting). To explore issues of equity, diversity and inclusion, any data regarding material deprivation, and the percentage of low-income and/or immigrant populations were also extracted. Results from both narrative syntheses and meta-analyses were extracted within the six outcome categories described above. Any outcomes within these categories or composite outcomes in these areas (e.g., when multiple outcome measures were grouped and reported as standardized mean difference in a meta-analysis) were extracted, as reported. Data collection forms and full extracted data are available upon request.
Data synthesis and certainty of evidence
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess the overall certainty of the evidence [23]. The GRADE process was adapted to accommodate the umbrella review by considering both the findings across included reviews and across single studies within reviews by intervention type and outcome. Following the GRADE approach, reviews including primarily RCTs start at ‘high’ certainty, while reviews primarily including non-randomized studies start at ‘low’ certainty. The level of certainty was further downgraded based on the risk of bias, inconsistency of findings, indirectness of interventions/outcomes, imprecision of effect measures, and/or publication bias, and were upgraded based on the magnitude of effect size, dose-response relationship, and accounting for confounding. A narrative approach to data synthesis was used, with results presented in supporting tables and figures. Informative statements reflecting both the certainty of evidence and importance of the size of the effect are presented to communicate overall findings within each intervention type and outcome category, in line with published recommendations [24]. Only results that compared an intervention group to a control group were included in GRADE, although subgroup analyses are presented in accompanying tables.
The review team synthesized data with feedback and input from the larger research team and key stakeholders. After an initial draft, preliminary results and categories were presented to four older adult citizen and service provider partners from an established stakeholder group within the EMBOLDEN research program who were consulted via a one-time, virtual meeting. The aim of this engagement was to allow for feedback and discussion about the appropriateness of intervention/outcome groupings and to identify priority outcome measures (e.g., prioritize general physical function outcomes over measures such as body composition). Our older adult and service provider partners also contributed to developing public-facing documents, including a plain-language summary and infographic.
Results
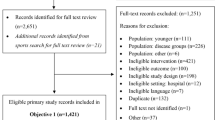
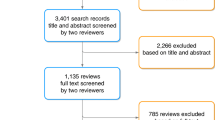
The search identified 41,157 unique citations, of which 1547 were potentially relevant; at this point, the team elected to limit to systematic reviews (Fig. 1). A second screen identified 453 citations for full-text review, of which 62 were included (Table 1). A list of excluded studies with reasons is provided in Additional file 2.

PRISMA Flow Diagram
Included reviews reported on several types of interventions, with some reporting separate results for more than one intervention type. Most reviews focused on exercise or PA only (n = 53) [26,27,28,29,30,31,32,33,34,35, 37,38,39,40, 42, 44, 45, 47, 49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75, 77, 78, 80,81,82,83,84, 86], while others included exercise with nutritional supplements (n = 9) [25, 36, 41, 43, 46, 48, 76, 79, 85]. No reviews included group-based nutrition interventions alone. Exercise or PA interventions were categorized as resistance exercise (n = 12) [26, 35, 47, 49, 52, 60, 65, 69, 72, 78, 80, 81], aerobic exercise (n = 5) [28, 29, 33, 38, 66], combined aerobic and resistance exercise (n = 9) [27, 34, 47, 50, 57, 60, 64, 65, 81], general PA (n = 12) [42, 44, 45, 49, 54, 58, 62, 63, 67, 69, 70, 86], mind-body exercise (e.g., Tai Chi, yoga, Pilates) (n = 11) [31, 32, 37, 40, 49, 56, 59, 71, 74, 75, 84], dance (n = 5) [39, 51, 61, 73, 81], and other (e.g., aquatics, stretching) (n = 10) [30, 47, 49, 53, 55, 68, 77, 81,82,83]. Nutritional supplements included protein (n = 5) [41, 43, 48, 79, 85], creatine (n = 2) [36, 76], vitamin D (n = 1) [25], or dairy (n = 1) [46]. Meta-analyses were undertaken in 39 reviews [25, 26, 29, 31,32,33,34,35,36,37, 40,41,42, 44, 46,47,48,49,50, 54,55,56, 60, 61, 65, 66, 68,69,70, 72, 75, 78,79,80,81, 83,84,85,86], 22 reviews presented findings narratively [27, 28, 38, 39, 43, 45, 51,52,53, 57,58,59, 62,63,64, 67, 71, 73, 74, 76, 77, 82], and one performed a network meta-analysis [30]. Total sample sizes ranged from 153 to 28,523 when reported. Participants ranged from 42 to 98 years old, with most reviews only including studies with participants aged 60 and older. No reviews extracted data on material deprivation, low income, or immigrant populations.
Eligible reviews included 1339 primary studies, of which 962 were unique (28.2% overlap across reviews, although some duplicates were included in reviews focused on different intervention types). Reviews with the most overlap by intervention type were exercise with nutritional supplements (36.2% overlap), dance (31.9% overlap), and resistance exercise (26.3% overlap). Single studies were published between 1983 and 2021 (range 5 to 99 studies per review). Of these, 83% were randomized controlled trials and 17% were quasi-experimental, observational, or not reported.
Methodological quality of included reviews
Methodological quality of the reviews was variable (summary in Fig. 2, full assessment in Additional file 3), with one review [49] rated as having high confidence in findings. The confidence for the remaining reviews were moderate (n = 21) [25, 28, 30, 35, 36, 42,43,44, 46, 50, 53, 66, 67, 71, 72, 75, 77, 80,81,82,83], low (n = 17) [31, 34, 39, 40, 48, 54,55,56, 60, 63, 69, 70, 73, 74, 76, 85, 86], and critically low (n = 23) [26, 27, 29, 32, 33, 37, 38, 41, 45, 47, 51, 52, 57,58,59, 61, 62, 64, 65, 68, 78, 79, 84]. Most reviews did not report protocol registration, describe an adequate search strategy, justify excluded studies, or incorporate risk of bias in interpreting review findings.

AMSTAR 2 Summary of Systematic Review Quality. Legend: RCT = randomized controlled trial, NRSI = non-randomized studies of interventions
Findings of reviews
A summary of findings by intervention type and outcome category, alongside review quality is listed in Table 2, with a summary of the certainty of evidence (GRADE) in Fig. 3.

GRADE Summary of Certainty of Evidence. Legend: a start at low certainty due to non-randomized study designs. b downgraded due to risk of bias. c downgraded due to inconsistency in effects. d downgraded due to indirectness of interventions/outcomes. e downgraded due to imprecision in effect estimate. f downgraded due to publication bias. g upgraded due to large effect. h upgraded due to dose-response relationship. i upgraded due to accounting for confounding
Aerobic capacity
The effect of interventions on aerobic capacity was reported in 15 reviews [27,28,29,30,31, 33, 37, 45, 50, 66, 72,73,74, 76, 83] (Additional file 4). Across reviews, 109 studies were reported, of which 104 were unique (overlap, 4.6% across intervention types). Aerobic capacity was most often assessed using measured or predicted maximal or peak oxygen consumption (VO2 peak). Based on high-certainty evidence, a combination of aerobic and resistance training results in meaningful improvements in aerobic capacity in older adults. Based on moderate certainty evidence, aerobic exercise probably results in improvements in aerobic capacity. Dance interventions may result in increased aerobic capacity, although this is based on low-certainty evidence and findings may change as more information becomes available. Interventions that combined exercise with nutritional supplements may make little to no difference in aerobic capacity of older adults, although this is based on low-certainty evidence. The evidence is very uncertain about the effect of mind-body exercise, general physical activity, or resistance exercise alone on aerobic capacity in older adults (very low certainty evidence). Other exercise types, including aquatic exercise and a combination of PA and cognitive training, were also examined for their effect on aerobic capacity.
Physical function
In total, 51 reviews [25, 27, 28, 30,31,32,33,34,35,36,37,38,39,40, 42,43,44,45,46,47,48,49,50,51,52,53, 57,58,59,60,61,62,63, 65, 67, 69,70,71,72,73,74,75,76,77, 79,80,81,82,83,84, 86] reported on 596 single studies, of which 434 were unique (27.2% overlap across intervention types). Physical function was typically assessed using the Timed Up and Go test, chair stands, gait speed, and six-minute walk test; often findings from single studies were compiled into a composite score for self-reported and/or measured physical function within meta-analyses (Additional file 5). Based on moderate certainty evidence, interventions that included a combination of aerobic and resistance exercise, interventions focused on general PA, and mind-body exercise interventions are all likely to result in improvements in physical function in older adults. Resistance training and dance interventions may also increase physical function (low certainty evidence). Low certainty evidence suggests that aerobic exercise interventions and exercise combined with nutritional supplements may have little to no impact on physical function.
Balance
In total, 30 reviews [27, 31,32,33, 37,38,39,40, 42, 44, 49, 51, 55,56,57, 59, 60, 62,63,64,65, 71, 73,74,75, 80, 82,83,84] reported on 275 single studies, of which 226 were unique (17.8% overlap). Static and dynamic balance tests (e.g., single-leg stance, Berg Balance Scale) and composite balance measures were used across reviews (Additional file 6). High certainty evidence suggests that participation in mind-body exercise interventions increases balance in older adults. General PA interventions and interventions that combined aerobic and resistance training are also likely to result in improvements in balance in older adults, based on moderate-certainty evidence. Dance interventions may improve balance; however, this is based on low certainty evidence. Also based on low certainty evidence, resistance training and aerobic exercise alone may result in little to no change in balance. No included reviews explored the effects of exercise and nutritional supplements on balance.
Falls and safety
Number of falls, risk of falling, and fall-related injuries were measured across 14 reviews [27, 28, 38, 40, 44, 56, 59, 60, 62, 63, 69, 72, 73, 82] including 108 single studies, 98 of which were unique (9.3% overlap). Interventions that combine aerobic and resistance exercise and interventions focused on general PA are likely to result in a small reduction in the risk of falls or fall-related injuries in older adults, based on moderate certainty evidence (Additional file 7). Based on low-certainty evidence, mind-body exercises may have little to no meaningful effect on fall risk, although these findings may change as more data are available. Dance interventions and aerobic exercise only may reduce falls, but the evidence is of very low certainty. Also based on very low certainty evidence, resistance training alone may have little to no effect on falls risk. No reviews reported the risk of falls within interventions that combined exercise and nutrition.
Muscle strength
Within reviews reporting muscle strength outcomes, 40 reviews [25,26,27,28, 31,32,33, 36,37,38,39,40,41,42,43,44, 46, 48, 52, 54, 58,59,60, 62, 65, 68, 71,72,73,74,75,76, 78,79,80, 82,83,84,85,86] reported on 452 single studies, of which 349 were unique (22.8% overlap). Various measures were reported, including handgrip strength, upper body strength, lower body strength, muscle mass, and overall muscle strength (Additional file 8). Both resistance exercise interventions and general PA interventions likely increase upper and lower body strength (moderate certainty evidence). Aerobic exercise alone, combined aerobic and resistance exercise, mind-body exercise, and dance interventions may result in improvements in muscle strength, however, this is based on low certainty evidence and findings may change as more data become available. Also based on low certainty evidence, interventions that combined exercise with nutritional supplements may not improve muscle strength.
Health-related quality of life and self-reported wellbeing
In total, 14 reviews [27, 28, 32, 33, 38, 42, 44, 60, 61, 63, 72, 73, 75, 82] reported health-related quality of life and self-reported wellbeing outcomes (Additional file 9). Given the variation in constructs measured within this domain (e.g., activities of daily living, quality of life (SF-36), perceived mental health) and limited number of reviews for each outcome type, these results were not incorporated into the overall summary of findings using GRADE.
Discussion
We provide a high-level comprehensive synthesis regarding the overall effectiveness of group-based PA and/or nutrition interventions to improve mobility among community-dwelling older adults. Within this review, we take a broad view of mobility, which captures several modifiable risk factors that influence older adults’ ability to move within and beyond their immediate environments [1, 5]. Interventions that combined aerobic and resistance exercise, and general PA interventions were found to result in meaningful improvements in physical function, balance, and muscle strength in older adults and are also likely to reduce falls and fall-related injuries. Mind-body exercise is also effective at improving physical function and balance, as is combined aerobic and resistance exercise for aerobic capacity.
Our findings support a multifaceted approach to health and wellbeing among community-dwelling older adults. Similar findings are reflected in two overviews of reviews focused on all adults over the age of 18, including older adults [87, 88], which informed the recent Canadian 24-Hour Movement Guidelines [89]. These guidelines also recommend a combination of aerobic, resistance, and balance exercises for adults aged 65+. Recent evidence has found that older adults face unique barriers and hesitancy to engage in certain types of exercise, such as resistance training [90]. It is encouraging that benefits for each of our outcome domains were seen across a range of intervention types. This suggests that effective interventions for older adults can incorporate a variety of types of exercises or physical activities that are most likely to foster enjoyment. This notion is consistent with emerging literature regarding the role of intrinsic motivation (i.e., enjoyment in physical activity) as an important predictor of physical activity engagement among older adults [91]. This approach can also improve accessibility to PA within this population by building upon existing community services and group-based PA programs that provide the additional benefit of social participation, which enhances enjoyment, adherence, and sustainability of PA [92]. The importance of social participation for older adults is supported by recent research informed by social-cognitive and socio-emotional theories, suggesting that older adults experiencing social isolation may derive meaningful social benefits from interactions with other participants in group-based exercise programs [93].
Our findings did not provide any convincing evidence for the addition of protein, creatine, vitamin D, or dairy supplementation to PA interventions to improve mobility-related outcomes within community-dwelling older adults. However, the overall quality of the systematic reviews and single studies was low to moderate, and numerous distinct comparator groups were used to test intervention effectiveness. These reviews typically synthesized highly heterogeneous single studies, including a wide range in “dose” of both exercise and dietary supplement components of the interventions; this may have limited the ability to see effects of specific combinations of interventions when synthesized together. Future high-quality studies with similar intervention and comparator groups may provide a better understanding of the role of combined diet and nutrition interventions on mobility-related outcomes in older adults. No reviews focused on group-based nutrition interventions alone, nor did any explore or report on domains of equity, diversity, and inclusion, highlighting priorities for future research.
There are several inherent limitations of this umbrella review that should be considered in interpreting results. Included reviews were limited to those in English, published since 2010. Considering the redundancy in single studies across the reviews dating back as early as 1983, we feel our strategy is robust, captures relevant data from much earlier than 2010, and conclusions are highly unlikely to be changed by older studies that employed less relevant methodologies and practices compared to those used today. Given the large number of included reviews, the overlap in single studies across reviews is unsurprising. The highest amount of overlap of studies evaluating physical function outcomes is attributable to our broad characterization of this outcome and the overlap in single studies among reviews focused on resistance, exercise and nutrition, and dance interventions. Although 28.2% overlap in single studies exists, each review contributing to these results focused on specific outcomes (e.g., gait speed alone, composite physical function measures), and we do not anticipate this greatly influenced our overall certainty of evidence. At the systematic review level, it was not possible to extract specific intervention “doses” and we did not examine single studies to collect this data. Although we would expect targeted aerobic, resistance, or combined aerobic and resistance exercise to be more effective than general PA interventions, certainty in the evidence was influenced by higher risk of bias and heterogeneity across both single studies and reviews of aerobic, resistance, and combined interventions, reflective of variation in types of interventions and tools used to assess outcomes. Finally, changing behaviour is a necessary precursor to changes in mobility-related health outcomes. For example, if an intervention fails to increase physical activity levels of older adults, an improvement in cardiovascular fitness or muscular strength will not occur. An understanding of interventions or techniques that are most effective to change older adults’ physical activity and/or nutrition-related behaviour is an important area of study, particularly when considering sustainability of change beyond the research study. A synthesis of the literature to answer this question is warranted but is outside of the scope of this review.
A strength of this umbrella review was the collaboration with older adults and service provider partners to inform the protocol and identify relevant outcomes. Specifically, the older adult partners involved in this project prioritized the inclusion of quality of life and wellbeing as outcomes of primary importance. The partners voiced that older adults’ self-reported functional measures were likely more meaningful to older adults than measures designed to capture physiology or function. We recognize that objective measures are important as benchmarks; however, we propose that subjective ratings represent a personal participant-relevant domain that could be as, or more, important when considering intervention effectiveness. However, very few reviews reported these outcomes separately as they were commonly combined within meta-analyses, thus we are unable to distinguish between self-reported and objectively measured function.
Conclusion
Group and community-based PA interventions that combine aerobic and resistance, general PA, and mind-body exercise can improve mobility measures in older adults. There was no evidence of benefit for nutritional supplementation with physical activity. No reviews focused on group-based nutrition interventions alone, and very few identified quality of life outcomes, highlighting a need for future synthesis work. The results of this umbrella review will be used to inform the co-design of a community-based, mobility-enhancing intervention.
Availability of data and materials
The datasets supporting the conclusions of this article are included within the article and its additional files.
Abbreviations
- AMSTAR 2:
-
A MeaSurement Tool to Assess systematic Reviews
- EMBOLDEN:
-
Enhancing physical and community MoBility in OLDEr adults with health inequities using commuNity co-design trial
- GRADE:
-
Grading of Recommendations Assessment, Development and Evaluation
- JBI:
-
Joanna Briggs Institute
- PA:
-
Physical activity
- RCT:
-
Randomized controlled trial
References
Webber SC, Porter MM, Menec VH. Mobility in older adults: a comprehensive framework. Gerontologist. 2010;50(4):443–50.
Tuscany Regional Health Council. Frailty in elderly people 2013 [cited 2021 May]. Available from: https://www.regione.toscana.it/documents/10180/320308/Frailty+in+elderly+people/9327bb85-6d3c-4e1b-a398-669e76ce5b01?version=1.0.
Wen YC, Chen LK, Hsiao FY. Predicting mortality and hospitalization of older adults by the multimorbidity frailty index. PLoS One. 2017;12(11):e0187825.
Lo AX, Rundle AG, Buys D, Kennedy RE, Sawyer P, Allman RM, et al. Neighborhood disadvantage and life-space mobility are associated with incident falls in community-dwelling older adults. J Am Geriatr Soc. 2016;64(11):2218–25.
Kuspinar A, Verschoor CP, Beauchamp MK, Dushoff J, Ma J, Amster E, et al. Modifiable factors related to life-space mobility in community-dwelling older adults: results from the Canadian longitudinal study on aging. BMC Geriatr. 2020;20(1):35.
Rikli RE, Jones CJ. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical Independence in later years. Gerontologist. 2013;53(2):255–67.
Milaneschi Y, Tanaka T, Ferrucci L. Nutritional determinants of mobility. Curr Opin Clin Nutr Metab Care. 2010;13(6):625–9.
World Health Organization. World Report on Ageing and Health. Geneva: World Health Organization; 2015. [cited 2021 May]. Available from: https://apps.who.int/iris/handle/10665/186463
Ramage-Morin PL, Garriguet D. Nutritional risk among older Canadians. Health Rep. 2013;24(3):3–13.
Bandayrel K, Wong S. Systematic literature review of randomized control trials assessing the effectiveness of nutrition interventions in community-dwelling older adults. J Nutr Educ Behav. 2011;43(4):251–62.
Pahor M, Guralnik JM, Ambrosius WT, Blair S, Bonds DE, Church TS, et al. Effect of structured physical activity on prevention of major mobility disability in older adults: the LIFE study randomized clinical trial. JAMA. 2014;311(23):2387–96.
Young K, Bunn F, Trivedi D, Dickinson A. Nutritional education for community dwelling older people: a systematic review of randomised controlled trials. Int J Nurs Stud. 2011;48(6):751–80.
Landi F, Cesari M, Calvani R, Cherubini A, Di Bari M, Bejuit R, et al. The “sarcopenia and physical fRailty IN older people: multi-componenT treatment strategies” (SPRINTT) randomized controlled trial: design and methods. Aging Clin Exp Res. 2017;29(1):89–100.
Farrance C, Tsofliou F, Clark C. Adherence to community based group exercise interventions for older people: A mixed-methods systematic review. Prev Med. 2016;87:155–66.
Neil-Sztramko SE, Teggart K, Phillips S, Sherifali D, Fitzpatrick-Lewis D, Newbold B, et al. An evidence-informed and stakeholder co-designed physical activity and community mobility intervention for older adults facing health inequities: the EMBOLDEN study. Advances in evidence synthesis: special issue. Cochrane Database Syst Rev. 2020;9:21.
Aromataris E, Fernandez R, Godfrey C, Holly C, Khalil H, Tungpunkom P. Chapter 10: Umbrella Reviews. JBI Manual for Evidence Synthesis; 2020 [cited 2021 May]. Available from. https://doi.org/10.46658/JBIMES-20-11.
Jadczak AD, Makwana N, Luscombe-Marsh N, Visvanathan R, Schultz TJ. Effectiveness of exercise interventions on physical function in community-dwelling frail older people: an umbrella review of systematic reviews. JBI Database System Rev Implement Rep. 2018;16(3):752–75.
Moore SA, Hrisos N, Errington L, Rochester L, Rodgers H, Witham M, et al. Exercise as a treatment for sarcopenia: an umbrella review of systematic review evidence. Physiotherapy. 2020;107:189–201.
Schultz TJ, Roupas P, Wiechula R, Krause D, Gravier S, Tuckett A, et al. Nutritional interventions for optimizing healthy body composition in older adults in the community: an umbrella review of systematic reviews. JBI Database System Rev Implement Rep. 2016;14(8):257–308.
Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100(2):126–31.
Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008.
Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR checklist 2017 [cited 2021 May]. Available from: https://amstar.ca/Amstar_Checklist.php.
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–6.
Santesso N, Glenton C, Dahm P, Garner P, Akl EA, Alper B, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126–35.
Antoniak AE, Greig CA. The effect of combined resistance exercise training and vitamin D3 supplementation on musculoskeletal health and function in older adults: a systematic review and meta-analysis. BMJ Open. 2017;7(7):e014619.
Borde R, Hortobagyi T, Granacher U. Dose-response relationships of resistance training in healthy old adults: A systematic review and Meta-analysis. Sports Med. 2015;45(12):1693–720.
Bouaziz W, Lang PO, Schmitt E, Kaltenbach G, Geny B, Vogel T. Health benefits of multicomponent training programmes in seniors: a systematic review. Int J Clin Pract. 2016;70(7):520–36.
Bouaziz W, Vogel T, Schmitt E, Kaltenbach G, Geny B, Lang PO. Health benefits of aerobic training programs in adults aged 70 and over: a systematic review. Arch Gerontol Geriatr. 2017;69:110–27.
Bouaziz W, Kanagaratnam L, Vogel T, Schmitt E, Drame M, Kaltenbach G, et al. Effect of aerobic training on peak oxygen uptake among seniors aged 70 or older: A Meta-analysis of randomized controlled trials. Rejuvenation Res. 2018;21(4):341–9.
Bruderer-Hofstetter M, Rausch-Osthoff AK, Meichtry A, Munzer T, Niedermann K. Effective multicomponent interventions in comparison to active control and no interventions on physical capacity, cognitive function and instrumental activities of daily living in elderly people with and without mild impaired cognition - A systematic review and network meta-analysis. Ageing Res Rev. 2018;45:1–14.
Bueno de Souza RO, Marcon LF, Arruda ASF, Pontes Junior FL, Melo RC. Effects of mat Pilates on physical functional performance of older adults: A Meta-analysis of randomized controlled trials. Am J Phys Med Rehabil. 2018;97(6):414–25.
Bullo V, Bergamin M, Gobbo S, Sieverdes JC, Zaccaria M, Neunhaeuserer D, et al. The effects of Pilates exercise training on physical fitness and wellbeing in the elderly: A systematic review for future exercise prescription. Prev Med. 2015;75:1–11.
Bullo V, Gobbo S, Vendramin B, Duregon F, Cugusi L, Di Blasio A, et al. Nordic walking can be incorporated in the exercise prescription to increase aerobic capacity, strength, and quality of life for elderly: A systematic review and Meta-analysis. Rejuvenation Res. 2018;21(2):141–61.
Chase JD, Phillips LJ, Brown M. Physical activity intervention effects on physical function among community-dwelling older adults: A systematic review and Meta-analysis. J Aging Phys Act. 2017;25(1):149–70.
da Rosa Orssatto LB, de la Rocha FC, Shield AJ, Silveira Pinto R, Trajano GS. Effects of resistance training concentric velocity on older adults’ functional capacity: A systematic review and meta-analysis of randomised trials. Exp Gerontol. 2019;127:110731.
Devries MC, Phillips SM. Creatine supplementation during resistance training in older adults-a meta-analysis. Med Sci Sports Exerc. 2014;46(6):1194–203.
Ebner SA, Meikis L, Morat M, Held S, Morat T, Donath L. Effects of movement-based mind-body interventions on physical fitness in healthy older adults: A Meta-analytical review. Gerontology. 2021;67(2):125–43.
Elboim-Gabyzon M, Buxbaum R, Klein R. The effects of high-intensity interval training (HIIT) on fall risk factors in healthy older adults: A systematic review. Int J Environ Res Public Health. 2021;18(22):11809.
Fernandez-Arguelles EL, Rodriguez-Mansilla J, Antunez LE, Garrido-Ardila EM, Munoz RP. Effects of dancing on the risk of falling related factors of healthy older adults: a systematic review. Arch Gerontol Geriatr. 2015;60(1):1–8.
Fernandez-Rodriguez R, Alvarez-Bueno C, Ferri-Morales A, Torres-Costoso A, Pozuelo-Carrascosa DP, Martinez-Vizcaino V. Pilates improves physical performance and decreases risk of falls in older adults: a systematic review and meta-analysis. Physiotherapy. 2021;112:163–77.
Finger D, Goltz FR, Umpierre D, Meyer E, Rosa LH, Schneider CD. Effects of protein supplementation in older adults undergoing resistance training: a systematic review and meta-analysis. Sports Med. 2015;45(2):245–55.
Frost R, Belk C, Jovicic A, Ricciardi F, Kharicha K, Gardner B, et al. Health promotion interventions for community-dwelling older people with mild or pre-frailty: a systematic review and meta-analysis. BMC Geriatr. 2017;17(1):157.
Gade J, Pedersen RJ, Beck AM. Effect of protein or essential amino acid supplementation during prolonged resistance exercise training in older adults on body composition, muscle strength, and physical performance parameters: A Systematic Review. Rehabilitation Process Outcome. 2018;7(7):1–12.
Garcia-Hermoso A, Ramirez-Velez R, Saez de Asteasu ML, Martinez-Velilla N, Zambom-Ferraresi F, Valenzuela PL, et al. Safety and effectiveness of long-term exercise interventions in older adults: A systematic review and Meta-analysis of randomized controlled trials. Sports Med. 2020;50(6):1095–106.
Grassler B, Thielmann B, Bockelmann I, Hokelmann A. Effects of different exercise interventions on heart rate variability and cardiovascular health factors in older adults: a systematic review. Eur Rev Aging Phys Act. 2021;18(1):24.
Hanach NI, McCullough F, Avery A. The impact of dairy protein intake on muscle mass, muscle strength, and physical performance in middle-aged to older adults with or without existing sarcopenia: A systematic review and Meta-analysis. Adv Nutr. 2019;10(1):59–69.
Hortobagyi T, Lesinski M, Gabler M, VanSwearingen JM, Malatesta D, Granacher U. Effects of three types of exercise interventions on healthy old Adults’ gait speed: A systematic review and Meta-analysis. Sports Med. 2015;45(12):1627–43.
Hou L, Lei Y, Li X, Huo C, Jia X, Yang J, et al. Effect of protein supplementation combined with resistance training on muscle mass, strength and function in the elderly: A systematic review and Meta-analysis. J Nutr Health Aging. 2019;23(5):451–8.
Howe TE, Rochester L, Neil F, Skelton DA, Ballinger C. Exercise for improving balance in older people. Cochrane Database Syst Rev. 2011;(11):CD004963.
Hurst C, Weston KL, McLaren SJ, Weston M. The effects of same-session combined exercise training on cardiorespiratory and functional fitness in older adults: a systematic review and meta-analysis. Aging Clin Exp Res. 2019;31(12):1701–17.
Hwang PW, Braun KL. The effectiveness of dance interventions to improve older Adults’ health: A systematic literature review. Altern Ther Health Med. 2015;21(5):64–70.
Katsoulis K, Stathokostas L, Amara CE. The effects of high- versus low-intensity power training on muscle power outcomes in healthy, older adults: A systematic review. J Aging Phys Act. 2019;27(3):422–39.
King A, Eitivipart C. Systematic review of published research on aquatic exercise for balance in the elderly. J Aquatic Physical Ther. 2016;24(1):9–21.
Labott BK, Bucht H, Morat M, Morat T, Donath L. Effects of exercise training on handgrip strength in older adults: A Meta-analytical review. Gerontology. 2019;65(6):686–98.
Lesinski M, Hortobagyi T, Muehlbauer T, Gollhofer A, Granacher U. Effects of balance training on balance performance in healthy older adults: A systematic review and Meta-analysis. Sports Med. 2015;45(12):1721–38.
Leung DP, Chan CK, Tsang HW, Tsang WW, Jones A. Tai chi as an intervention to improve balance and reduce falls in older adults: A systematic and meta-analytical review. Altern Ther Health Med. 2011;17(1):40–8.
Levin O, Netz Y, Ziv G. The beneficial effects of different types of exercise interventions on motor and cognitive functions in older age: a systematic review. Eur Rev Aging Phys Act. 2017;14:20.
Liberman K, Forti LN, Beyer I, Bautmans I. The effects of exercise on muscle strength, body composition, physical functioning and the inflammatory profile of older adults: a systematic review. Curr Opin Clin Nutr Metab Care. 2017;20(1):30–53.
Liu H, A. F. Tai chi as a balance improvement exercise for older adults: a systematic review. J Geriatr Phys Ther. 2010;33(3):103–9.
Liu CJ, Chang WP, Araujo de Carvalho I, Savage KEL, Radford LW, Amuthavalli TJ. Effects of physical exercise in older adults with reduced physical capacity: meta-analysis of resistance exercise and multimodal exercise. Int J Rehabil Res. 2017;40(4):303–14.
Liu X, Shen PL, Tsai YS. Dance intervention effects on physical function in healthy older adults: a systematic review and meta-analysis. Aging Clin Exp Res. 2021;33(2):253–63.
Loureiro V, Gomes M, Loureiro N, Aibar-Almazan A, Hita-Contreras F. Multifactorial programs for healthy older adults to reduce falls and improve physical performance: systematic review. Int J Environ Res Public Health. 2021;18(20):10842.
Martin JT, Wolf A, Moore JL, Rolenz E, DiNinno A, Reneker JC. The effectiveness of physical therapist-administered group-based exercise on fall prevention: a systematic review of randomized controlled trials. J Geriatr Phys Ther. 2013;36(4):182–93.
Martins AC, Santos C, Silva C, Baltazar D, Moreira J, Tavares N. Does modified Otago exercise program improves balance in older people? A systematic review Prev Med Rep. 2018;11:231–9.
Meereis-Lemos ECW, Guadagnin EC, CB M. Influence of strength training and multicomponent training on the functionality of older adults: systematic review and meta-analysis. Rev Bras de Cineantropometria & Desempenho Humano. 2020;22:e60707.
Montero D, Diaz-Canestro C. Endurance training and maximal oxygen consumption with ageing: role of maximal cardiac output and oxygen extraction. Eur J Prev Cardiol. 2016;23(7):733–43.
Moore M, Warburton J, O'Halloran PD, Shields N, Kingsley M. Effective community-based physical activity interventions for older adults living in rural and regional areas: A systematic review. J Aging Phys Act. 2016;24(1):158–67.
Moran J, Ramirez-Campillo R, Granacher U. Effects of jumping exercise on muscular power in older adults: A Meta-analysis. Sports Med. 2018;48(12):2843–57.
Nicolson PJA, Duong V, Williamson E, Hopewell S, Lamb SE. The effect of therapeutic exercise interventions on physical and psychosocial outcomes in adults aged 80 years and older: A systematic review and Meta-analysis. J Aging Phys Act. 2022;30(3):517–34.
Plummer P, Zukowski LA, Giuliani C, Hall AM, Zurakowski D. Effects of physical exercise interventions on gait-related dual-task interference in older adults: A systematic review and Meta-analysis. Gerontology. 2015;62(1):94–117.
Qi M, Moyle W, Jones C, Weeks B. Tai chi combined with resistance training for adults aged 50 years and older: A systematic review. J Geriatr Phys Ther. 2020;43(1):32–41.
Raymond MJ, Bramley-Tzerefos RE, Jeffs KJ, Winter A, Holland AE. Systematic review of high-intensity progressive resistance strength training of the lower limb compared with other intensities of strength training in older adults. Arch Phys Med Rehabil. 2013;94(8):1458–72.
Rodrigues-Krause J, Krause M, Reischak-Oliveira A. Dancing for healthy aging: functional and metabolic perspectives. Altern Ther Health Med. 2019;25(1):44–63.
Roland KP, Jakobi JM, GR. J. Does yoga engender fitness in older adults? A critical review. J Aging Phys Act. 2011;19(1):62–79.
Sivaramakrishnan D, Fitzsimons C, Kelly P, Ludwig K, Mutrie N, Saunders DH, et al. The effects of yoga compared to active and inactive controls on physical function and health related quality of life in older adults- systematic review and meta-analysis of randomised controlled trials. Int J Behav Nutr Phys Act. 2019;16(1):33.
Stares A, Bains M. The additive effects of Creatine supplementation and exercise training in an aging population: A systematic review of randomized controlled trials. J Geriatr Phys Ther. 2020;43(2):99–112.
Stathokostas L, Little RM, Vandervoort AA, Paterson DH. Flexibility training and functional ability in older adults: a systematic review. J Aging Res. 2012;2012(306818):1–13.
Straight CR, Lindheimer JB, Brady AO, Dishman RK, Evans EM. Effects of resistance training on lower-extremity muscle power in middle-aged and older adults: A systematic review and Meta-analysis of randomized controlled trials. Sports Med. 2016;46(3):353–64.
Ten Haaf DSM, Nuijten MAH, Maessen MFH, Horstman AMH, Eijsvogels TMH, Hopman MTE. Effects of protein supplementation on lean body mass, muscle strength, and physical performance in nonfrail community-dwelling older adults: a systematic review and meta-analysis. Am J Clin Nutr. 2018;108(5):1043–59.
Tschopp M, Sattelmayer MK, Hilfiker R. Is power training or conventional resistance training better for function in elderly persons? A meta-analysis. Age Ageing. 2011;40(5):549–56.
Van Abbema R, De Greef M, Craje C, Krijnen W, Hobbelen H, Van Der Schans C. What type, or combination of exercise can improve preferred gait speed in older adults? A meta-analysis BMC Geriatr. 2015;15:72.
Vetrovsky T, Steffl M, Stastny P, Tufano JJ. The efficacy and safety of lower-limb plyometric training in older adults: A systematic review. Sports Med. 2019;49(1):113–31.
Waller B, Ogonowska-Słodownik A, Vitor M, Rodionova K, Lambeck J, Heinonen A, et al. The effect of aquatic exercise on physical functioning in the older adult: a systematic review with meta-analysis. Age Ageing. 2016;45(5):593–601.
Wang C, Liang J, Si Y, Li Z, Lu A. The effectiveness of traditional Chinese medicine-based exercise on physical performance, balance and muscle strength among older adults: a systematic review with meta-analysis. Aging Clin Exp Res. 2022;34(4):25–740.
Wirth J, Hillesheim E, Brennan L. The role of protein intake and its timing on body composition and muscle function in healthy adults: A systematic review and Meta-analysis of randomized controlled trials. J Nutr. 2020;150(6):1443–60.
Yang Y-P, Lin H-C, Chen K-M. Functional fitness in older adults. Topics Geriatric Rehabilitation. 2019;35(4):238–47.
McLaughlin EC, El-Kotob R, Chaput JP, Janssen I, Kho ME, Poitras VJ, et al. Balance and functional training and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab. 2020;45(10 (Suppl. 2)):S180–S96.
El-Kotob R, Ponzano M, Chaput JP, Janssen I, Kho ME, Poitras VJ, et al. Resistance training and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab. 2020;45(10 (Suppl. 2)):S165–S79.
Ross R, Chaput JP, Giangregorio LM, Janssen I, Saunders TJ, Kho ME, et al. Canadian 24-hour movement guidelines for adults aged 18-64 years and adults aged 65 years or older: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. 2020;45(10 (Suppl. 2)):S57–S102.
Burton E, Farrier K, Lewin G, Pettigrew S, Hill AM, Airey P, et al. Motivators and barriers for older people participating in resistance training: A systematic review. J Aging Phys Act. 2017;25(2):311–24.
Labudek S, Fleig L, Jansen CP, Kramer-Gmeiner F, Nerz C, Becker C, et al. Applying social cognition models to explain walking duration in older adults: the role of intrinsic motivation. J Aging Phys Act. 2021;29(5):744–52.
Devereux-Fitzgerald A, Powell R, Dewhurst A, French DP. The acceptability of physical activity interventions to older adults: A systematic review and meta-synthesis. Soc Sci Med. 2016;158:14–23.
Steckhan GMA, Warner LM, Fleig L. Preventing falls together: social identification matters for engaging older adults in a group-based exercise program. Act Adapt Aging. 2022;46(1):31–45.
Acknowledgments
Not applicable.
Funding
Funding received from the Labarge Centre for Mobility in Aging within the McMaster Institute for Research on Aging at McMaster University, Canada Research Chairs Program, the Canadian Institutes of Health Research, and in-kind support from the Aging, Community and Health Research Unit at McMaster University. The funders had no role in the study design, conduct, or decision to publish.
Author information
Authors and Affiliations
Contributions
SNS, CM, DS, DFL, SMP, KBN, EA, AK, CCK, PLS, and RG conceptualized and designed the study. SNS, KT, CM, DS, DFL, GC, and RG acquired, analyzed, and interpreted the data. SNS, KT, and RG drafted the manuscript. All authors substantively revised the manuscript and have approved the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
SMP declares that he is a named inventor on a patent held by Exerkine, but receives no fees/payment, and is an unpaid member of the Scientific Advisory Board for Enhanced Recovery.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search Strategy.
Additional file 2.
List of Excluded Studies.
Additional file 3.
AMSTAR 2 Critical Appraisal Results.
Additional file 4.
Aerobic Outcomes.
Additional file 5.
Physical Function Outcomes.
Additional file 6.
Balance Outcomes.
Additional file 7.
Falls and Safety Outcomes.
Additional file 8.
Muscle Strength Outcomes.
Additional file 9.
Health-Related Quality of Life and Wellbeing Outcomes.
Additional file 10.
PRISMA Systematic Reviews and Meta-Analyses Checklist.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Neil-Sztramko, S.E., Teggart, K., Moore, C. et al. Community-based group physical activity and/or nutrition interventions to promote mobility in older adults: an umbrella review. BMC Geriatr 22, 539 (2022). https://doi.org/10.1186/s12877-022-03170-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-022-03170-9