
Abstract
Background
This study systematically reviewed injury death and causes in the elderly population in China from 2000 to 2020, to prevent or reduce the occurrence of injuries and death.
Methods
The CNKI, VIP, Wan Fang, MEDLINE, Embase, SinoMed, and Web of Science databases were searched to collect epidemiological characteristics of injury death among elderly over 60 years old in China from January 2000 to December 2020. Random effects meta-analysis was performed to pool injury mortality rate and identify publication bias, with study quality assessed using the AHRQ risk of bias tool.
Results
(1) A total of 41 studies with 187 488 subjects were included, covering 125 million elderly. The pooled injury mortality rate was 135.58/105 [95%CI: (113.36 to 162.14)/105], ranking second in the total death cause of the elderly. (2)Subgroup analysis showed that male injury death (146.00/105) was significantly higher than that of females (127.90/105), and overall injury mortality increased exponentially with age (R2 = 0.957), especially in those over 80 years old; the spatial distribution shows that the injury death rate in the central region is higher than that in the east and west and that in the countryside is higher than that in the city; the distribution of death time shows that after entering an aging society (2000–2020) is significantly higher than before (1990–2000). (3) There are more than 12 types of injury death, and the top three are falling, traffic accidents, and suicide.
Conclusions
China's elderly injury death rate is at a high level in the world, with more males than females, especially after the age of 80. There are regional differences. The main types of injury death are falling, traffic, and suicide. During the 14th Five-Year Plan period, for accidental injuries and death, a rectification list for aging and barrier-free environments was issued.
PROSPERO Registration
The systematic review was registered in PROSPERO under protocol number CRD42022359992.
Similar content being viewed by others


Introduction
The proportion of the population over 60 years old is up to 18.7% according to the 7th National Census of China (2020) [1], which means that China has entered a deep aging society. In 2021, the National Bureau of Statistics of China reported that the total number of deaths in the country reached nearly 10.14 million, of which more than 2/3 of the population is over 60 years old [2]. The top three causes of death in China are chronic diseases, injuries, as well as infectious diseases, maternal and infant diseases, and nutritional deficiencies, with injury-related deaths ranking second among the elderly [3]. In addition to death, disability, and personal and family suffering, the consequences of injury will also cause a serious burden of medical care [4]. In this regard, the Chinese Communist Party and government are highly concerned about the death of elderly injuries and have introduced relevant strategies and measures. However, research on injury death of the elderly is still mostly limited to a certain province, prefecture, and city, and there is no comprehensive analysis of the situation In this systematic review, we use big data to conduct a meta-analysis on the types of injury deaths, the characteristics of "population, places, and times" and dynamic changes in the elderly population in China in the past 20 years (2000–2020), and the results can provide a basis for formulating corresponding prevention and control measures, thereby preventing and reducing the occurrence of injuries and deaths.
Material and methods
The systematic review was registered in PROSPERO under protocol number CRD42022359992.
Inclusion and exclusion criteria
Inclusion criteria: (1) Resident senior citizens aged 60 years in China from 2000 to 2020; (2) Injury death as the research outcome goal; (3) Cause of death classified according to ICD-10 code; (4) Provide injury mortality or the number of deaths, sample size, or the required value can be calculated based on the data given in the literature; (5) Source of data from the local death cause monitoring system or authoritative system; (6) Cross-sectional study.
Outcomes
Injury mortality among the elderly
Exclusion criteria: (1) Documents with ambiguous, incomplete, or unconverted data; (2) The quality of the literature is too low (AHRQ score below 3); (3) Repeated publications.
Search strategy
This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and was searched through seven electronic databases without language restriction: Chinese National Knowledge Infrastructure (CNKI), Chongqing VIP Database, WanFang Database, MEDLINE, Embase, SinoMed and Web of Science. To collect epidemiological cross-sectional research papers on injury and death of Chinese people aged ≥ 60 years published in China and abroad, and the search time limit was from January 2000 to December 2020 (including references to the literature to supplement relevant studies). The retrieval takes the combination of subject headings and free words. Chinese search terms include: “中国”, “中国人”, “我国”, “老年人”, “老人”, “老年”, “伤害死亡”, “伤害”, “死因”, “死亡率”, “粗死亡率”, “标化死亡率”, “死因监测”; English search terms include China, Chinese, elderly, elderly people, aged, injury death, injury, death, mortality rate, crude mortality rate, standardized mortality rate, mortality surveillance.
Literature screening and data extraction
All publications that were identified from literature searches were initially extracted by two independent reviewers. Data were stored in a standardized tabular format and the full list was assessed for eligibility by two different reviewers independently. Following the screening, any discrepancies were discussed between the reviewers. Any further conflicts were resolved by reviewing the original publication and additional adjudication. Information from selected literature was extracted as followed: (1) The first author, the area, and time of the investigation; (2) Outcome indicators (injury mortality) and outcome measurement data (sample size, age and gender of patients, place of residence, investigation time and injury type); (3) Key elements of risk assessment for bias.
Quality assessment
Evaluation tools recommended by Agency for Healthcare Research and Quality (AHRQ) tool(www.ahrq.gov) were used to assess the quality of all cross-sectional studies. AHRQ was an 11-item instrument with 3 options: the ‘Yes’ would be scored as ‘1’, ‘No’ or ‘Unclear’ would be scored as ‘0’. The articles were scored as follows: 0–3 = low quality; 4–7 = moderate quality; 8–11 = high quality. The quality of the literature was evaluated by two independent reviewers (Y.SL and T.JX), and a third party was consulted in case of disagreement.
Statistical analysis
All results for the prevalence of injury mortality among 187 488 elderly Chinese were visualized using forest plots. The heterogeneity between the involved studies was assessed using the I2 statistic and Q tests. The fixed effects model was used when the heterogeneity test results were considered to be good(P > 0.1 and I2 < 50%); conversely, the random effects model was utilized when I2 ≥ 50%. Subgroup analysis was carried out according to the characteristics of the population, such as gender, age, region, urban and rural distribution, statistical year, and injury type; sensitivity analysis was carried out by one-by-one elimination method, and Publication bias was assessed using Egger's test and a funnel plot of linear regression of the log ORs on the inverse root of the sample size, and P < 0.05 was considered statistically significant difference. Statistical analysis was performed with the software R (R Project for Statistical Computing, version 4.1.2, http://www.r-project.org/).
Results
Literature screening process and results
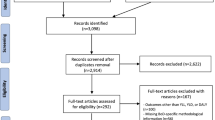
A total of 1864 related pieces of literature were originally identified, and after the layer-by-layer screening, 41 pieces of literature were ultimately incorporated, with a total of 187 488 elderly people who died of injury, comprising a sample population of 124 798 756. The literature screening process and results are shown in Fig. 1.

Flow diagram for systematic review and meta-analysis. Flowchart demonstrating selection of eligible studies. The databases retrieved and the number of the literature identified are as follows: CNKI (N = 91), VIP (N = 63), WanFang Data (N = 389), MEDLINE (N = 193), SinoMed (N = 13), Embase (N = 3), and Web of Science (N = 1112)
Basic characteristics and risk of bias assessment of the included literature
The basic characteristics and risk of bias evaluation of the incorporated literature are demonstrated in Table 1.
Results of the meta-analysis
Literature basic situation and quality
This review collected 41 pieces of literature, and the average AHRQ score was 6.85, demonstrating that the quality of the literature was optimal. The sample involved 124 798 756 elderly people, with 187 488 injury death, in which males (85 119) were slightly more than females (82 300). According to the results of the heterogeneity test (P < 0.001, I2 = 100%), a single-sample rate meta-analysis was performed using a random-effects model, and the results of the forest plot are demonstrated in Fig. 2.

Forest plot of injury mortality point values and interval estimates
Total injury mortality
The results of the random effects model showed that the total injury mortality of the elderly in China was 135.58/105 [95%CI: (113.36 to 162.14)/105].
Subgroup analysis Results (1/10.5 )
The subgroups analyzed the injury mortality rate of different factors such as gender, age, region and time. Due to the large heterogeneity among subgroups, random model analysis was still used. The results showed that the mortality rate of males was higher than that of females (146.00 vs. 127.90, P < 0.05); the author divided the age into six groups, and the mortality rate increased sharply with age, especially in the group over 80 years old (60-year-old: 72.01 < 65-year-old: 91.83 < 70-year-old: 130.05 < 75-year-old: 203.25 < 80-year-old: 384.88 < 85-year-old: 854.42, P for trend < 0.05), see Fig. 3 and Table 2; according to the spatial analysis, the mortality rate in China was as follows: middle: 215.26 > western: 143.84 > east: 130.73, rural (170.35) is higher than urban (131.99); in terms of time, the injury mortality rate was calculated based on the per capita GDP level for 20 years (across four five-year plans), In the first two five-year plans, the overall change demonstrated the same trend as the per capita GDP level, although in the latter two, the trend was the opposite (Fig. 4). According to 41 included literatures, more than 12 types of injuries were involved, and the top three were falling (43.91), traffic accidents (24.49), and suicide (15.88), see in Table 3; and the composition of different causes of death from injuries among the elderly in China from 2000 to 2020 (%) is shown in Fig. 5.

Changes in injury mortality rates among the elderly of different age groups in China, 2000–2020

Columnar diagram of GDP level and elderly injury mortality during the four five-year plans

Composition of different injury causes of death among Chinese elderly from 2000 to 2020 (%)
According to the statistics from 41 literatures, there are more than 12 causes of injury and death in China. They are falling, traffic accidents, suicide, drowning, poisoning, fire, homicide, transportation accidents, electric shock, crushing, accidents caused by the natural environment, suffocation, etc. The first six types accounted for 85.55% of the total causes of death. Falling is the main cause of death (41.36%), followed by traffic and suicide. The death rate of the first two injury types was higher in eastern than in western, and the fall death rate for males was slightly lower than that of females, but the suicide death rate was slightly higher than that of females, and the traffic death rate was 1.79 times higher than that of females.
Sensitivity analysis
The sensitivity analysis was carried out by the one-by-one elimination method, and the results were between 132.40/105 and 143.37/105, which was not much different from the total injury mortality rate, indicating that the results of this study were stable, as shown in Fig. 6.

Forest map after culling one by one
Evaluation of publication bias
The funnel plot of total injury mortality was not significantly asymmetric. Combined with the results of Egger's plot (t = -1.58, P = 0.122), it suggested that there was a small possibility of publication bias, see Fig. 7.

Funnel plot of total injury mortality rate
Discussion
The above results show that the injury mortality rate of the elderly in China after entering the aging period is higher than that before and has broken the original stable situation [46]; it is higher than that of the United States and Brazil in 2000 and is at a medium–high level compared with the EU countries in the early twenty-first century [47,48,49]. Mortality levels indicate that injury mortality in the elderly population varies by country and time. Of course, to more accurately compare this rate with countries, a standardized rate is ideal.
Another prominent feature of injury death in China is that there is a gender difference between males and females, which is consistent with the results of most countries. The mortality rate of different age groups varies significantly. Injuries increase exponentially with age and the rate of falling increases with age. The reason may be the negative impact of aging on the elderly [50], and it is particularly important to prevent falling. The world has become intelligent, and the elderly are not as receptive to intelligent technology as the young and middle-aged. For example, in bad weather, a young man can use his smartphone to solve his lunch while sitting in an office, while an old man needs to go to the street to buy food. It is entirely possible to suffer injury.
2000–2020 was the period from the implementation to the completion of China's four "five-year plans", during which China completed the rapid change from reform to opening up, and the Chinese economy, social environment, family living patterns, and even development policies changed dramatically. This has resulted in large differences in economic development and GDP levels between central, eastern, and western China, which inevitably affect the overall changes in injury mortality among older adults in China. In the first decade, the flow of economic growth led to frequent population movements and traffic, and these phenomena inevitably resulted in a relative increase in traffic accidents and other accidental injuries [51]. GDP growth is largely dependent on industrial production and rising labour levels, which have resulted in increased stress in work and life; these physical to psychological stresses have been reported in other studies in China, so their effects on accidental injuries cannot be ruled out either. GDP growth has a positive impact on increasing the country's economic power, improving people's living standards, and promoting social progress. Meanwhile, from a management and public health perspective, it may play a significant role in reducing the occurrence and prognosis of injuries if the positive effects of GDP are adequately considered.
In the early stage of China’s reform and opening up, the “Seventh Five-Year Plan” divided the entire region into eastern, central, and western regions according to the high, intermediate, and low levels of economic and technological development [52]. The injury mortality in the central region is the highest, which can be explained from the following three aspects. First, compared with the eastern and coastal regions, central China has a cold climate, relatively scarce resources, and relatively lagging economic level [53, 54]. Moreover, diet type and structure, lifestyle, and habits differ among the regions (such as Inner Mongolia, Heilongjiang, Jilin Province, etc.), and the increased risk of death from accidental injuries cannot be excluded as a long-term effect of these factors. Second, the social security development system and speed in the central region are relatively lagging, and the medical and healthcare technology and facilities for elderly special groups are not as ideal as those of the eastern or coastal regions [55]. Lastly, the density of transportation arteries in central China (such as Jiangxi, Hubei, Hunan Province, etc.) is relatively high [56], and many transportation lines are designed to pass through dense areas of urban dwellers due to the regional culture and lifestyle mindset, which to a certain extent are more prone to traffic accidents. While the injury mortality in the eastern region is slightly higher than that in the western region. It is believed that this phenomenon does not rule out the double-edged sword effect of factors such as the aging degree, the higher GDP level, and the more congruent health care system in the eastern region.
After the urbanization development was included in the special key plan in China's "Tenth Five-Year Plan", the level of urbanization has climbed sharply over the past 20 years, from 36% in 2000 to 63.89% in 2020 [2]. This trend has brought about major changes in the rural population, labor force size, and structure –– the average age of agricultural laborers is 48.45 years old, and as many as 75.24% are female. The influx of rural youth and middle-aged labor into cities has considerably accelerated the aging and feminization of the rural population [57], which is also one of the factors that cause rural injuries to be higher than urban ones.
Another feature is that injury mortality in China has raised firstly and then reduced over the past 20 years (2000–2020). Since entering an aging society in 2000, the injury mortality rate has remained high for ten years. With the emergence and popularization of the concept of population aging, the national injury prevention, and control work has been carried out in an all-round way [58], and the Chinese Party and government have issued the "Quality Development Outline (2011–2020)", "National Disability Prevention Action Plan (2016–2020)", "Healthy China 2030 Planning Outline" and a series of strategies or measures such as injury prevention and control, such as road safety-related policies, although the activities of injury prevention, obstacle reduction, and aging-appropriate renovation have been carried out at different levels in China, and achieved certain results, the degree of aging in China Unabated, resulting in a continued increase in injury mortality.
The composition of the cause of injury death still displayed certain characteristics. In terms of period, the top six causes of death in China, including falling, traffic accidents, and suicide, cover 84.1% of the total injury causes, which is substantially higher than that in the EU (64.1%). Among these causes of death, falling is the earliest cause of injury death. Among Chinese people aged 65, an average of 3–4 people in every 10 have fallen. According to this estimate, about 57.192 million to 76.256 million people will fall every year at this stage, and this phenomenon will increase with the acceleration of the aging degree. 40% to 70% of people who fall will suffer from various degrees of injury and receive medical treatment. It is worth mentioning that about 22.34% of those who fall have suffered serious injury or even paralysis [59].
In contemporary China, traffic accidents have virtually become a social problem. Since the beginning of the twenty-first century, the mileage of highways and the number of motor vehicles have raised markedly and have been extensively managed. Road traffic injuries are extremely common, among which injuries involving "people" account for 78.3% ~ 96.5% of all causes, and illegal acts such as speeding are very common [60]. At the same time, frequent and dense population flow leads to traffic jams and traffic accidents.
Compared with the BRICS countries (China, Russia, Brazil, India, and South Africa), the suicide mortality rate among those aged 70 years is the highest in China, and the phenomenon of suicide is severe (2015) [61]. The main reasons for this phenomenon are: first, illness and persistent economic burden. The prevalence of chronic diseases among the elderly in China is 86.23%, of which 76.30% suffer from various chronic diseases at this stage [62, 63]; the second is lack of emotion and loneliness. If it cannot be ruled out that China's "family planning" policy, which was set as a basic national policy in 1982, has led to the emergence of a large number of "4 + 2 + 1 Family", "8 + 2 + 1 Family" and " The Loss of Only Child Family", factors such as widowhood can affect emotions [64].
Because of the current situation of injury and death among the elderly in China, during the "14th Five-Year Plan" period, a list of rectifications such as suitable aging and a barrier-free environment has been issued. However, to achieve Healthy Aging, multiple aspects need to be integrated, such as industrial structure adjustment, improving the elderly's Self-health quality, creating a humanistic environment of government-community-family integration, and reducing the risk of injury and death.
This study has certain limitations. First, the heterogeneity of the included studies is high due to the characteristics of a single rate meta-analysis; second, in the hierarchical analysis, the literature data from different regions are not uniform, and it is also difficult to obtain data standardization background information; third, the analysis of the influencing factors of accidental death is limited to a certain extent, and there is no data on living habits, psychological factors, and post-injury nursing behaviors.
This systematic review objectively reflects the current status of injury deaths and causes of death among the elderly in China. The data is derived from the public security bureaus, death-cause monitoring sites, and CDCs of various provinces and cities in China, which are authentic and authoritative. Sensitivity analysis showed that the results of the meta-analysis of this study were stable, and the publication bias assessment also showed that there was no obvious publication bias, so the results obtained were more representative and reliable than a single study. The results of this study provide an important foundation for future prospective research and the initiation of advanced injury prevention plans in China. Governments and local institutions should consider implementing public health measures to prevent injury death. Examples include reducing income inequality, allocating more resources to vulnerable groups, and implementing targeted group prevention [65].
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due this is a systematic review and meta-analysis of publishing and fully randomized studies but are available from the corresponding author on reasonable request.
Abbreviations
- AHRQ:
-
Agency for Healthcare Research and Quality
- EU:
-
European Union
- CDC:
-
Center for Disease Control and Prevention
References
National Bureau of Statistics. Population Data. (2020–1–30)[2022–2–9].http://www.stats.gov.cn/.
National Bureau of Statistics. Statistical Communiqué of the People's Republic of China on National Economic and Social Development in 2021. (2022–2–28)[2022–2–9].http://www.stats.gov.cn/xxgk/sjfb/zxfb2020/202202/t20220228_1827971.html.
Chinese Center for Disease Control and Prevention chronic non-communicable disease control center, National Health Commission Statistical Information Center. China Cause of Death Surveillance Dataset 2018.Beijing, Science and technology of China press,2019.10:48-49
Ministry of Health's Bureau of Disease Control and Prevention. China Injury Prevention Report. Beijing, People's Medical Publishing House, 2007.
Teng YM, Mao W, Huang JM, et al. Analysis of the causes of injury death among the elderly aged 65 years and above in Guangxi province from 2014 to 2019. Ying yong yu fang yi xue. 2021;27:110–3. https://doi.org/10.3969/j.issn.1673-758X.2021.02.005.
Wei XL, Huang CY, Huang QL, et al. Analysis of injury mortality among the elderly over 60 years old in Suzhou in 2008–2017. Zhonghua Yu Fang Yi Xue Za Zhi. 2020;21:301–5. https://doi.org/10.16506/j.1009-6639.2020.03.015.
Li ZK, Zhang MR, Yang S, et al. Analysis of injury death and change trend of elderly in Kunming from 2010 to 2019. Zhongguo man xing bing yu fang yu kong zhi. 2020;28:945–8. https://doi.org/10.16386/j.cjpccd.issn.1004-6194.2020.12.016.
ZY Liao, QS Yang, LR Fu, et al. Analysis on Injury Death Among the Elderly Aged 60 Years and Above in Langzhong City From 2012 to 2017. Yu fang yi xue qing bao za zhi 2020;36:25–28+33.
Zhang CH, Mao DQ, Xiao YF, et al. Analysis on the characteristics and trend of injury death among the elderly aged 65 and above in Chongqing. Gonggong wei sheng yu yu fang yi xue. 2020;31:79–82.
Huang LL, Cai ZC, Li YL, et al. Analysis of injury death characteristics among registered residents in Zhongshan city, Guangdong province, from 2014 to 2018. Zhongguo she hui yi xue. 2020;37:92–6. https://doi.org/10.3969/j.issn.1006-2483.2020.06.019.
Xu C, Zhang J, Li X, et al. Epidemiological Analysis of Injury Death in Tongjiang County From 2017 to 2019. Zhi ye wei sheng yu bing shang. 2020;35:359–64. https://doi.org/10.3969/j.issn.1673-5625.2020.01.026.
AY Shi, YQ Ni.Characteristic analysis on injury death in elderly in Chongming District of Shanghai, 2005–2014. Journal of environmental & occupational medicine 2019;31:179–182.doi: https://doi.org/10.19428/j.cnki.sjpm.2019.19006.
Yu X. Analysis on injury-related deaths in Haidian district of Beijing, 2010–2015. Ji Bing Jian Ce. 2019;34:166–70. https://doi.org/10.3784/j.issn.1003-9961.2019.02.017.
Zeng C, Liang XD. Analysis of injury and death characteristics of residents in Zhuhai, 2014–2017. Zhongguo man xing bing yu fang yu kong zhi. 2019;27:557–60. https://doi.org/10.16386/j.cjpccd.issn.1004-6194.2019.07.018.
Huang CY, Chen G, Zhang Y, et al. Analysis of changes in causes of death among people over 60 years old in Suzhou from 2002 to 2016. Zhongguo man xing bing yu fang yu kong zhi. 2018;26:713–6. https://doi.org/10.16386/j.cjpccd.issn.1004-6194.2018.09.021.
Xiang YF, Shao Z. Analysis of Resident Injury and Death in Yuyao City from 2011 to 2014. Zhongguo xiang cun yi yao. 2018;25:62–3. https://doi.org/10.19542/j.cnki.1006-5180.001394.
Gong HY, Zhang QJ, Zhang L, et al. Death and the trend of unintentional injury among elderly people in Hubei Province (2008–2015). Gong gong wei sheng yu yu fang yi xue. 2017;28:77–80.
Zhang XY, Hou B, Wu DD, et al. Analysis of the changing trend and influencing factors of injury mortality among the elderly in Xi’an from 2010 to 2015. Zhongguo wei sheng tong ji. 2017;34:632–4.
Zhang DK, Yu J, Zhao XL, et al. Analysis of accidental injury death among the elderly > 65 years old in Gaogang District, Taizhou City from 2011 to 2015. Jiangsu yu fang yi xue. 2017;28:559–60. https://doi.org/10.13668/j.issn.1006-9070.2017.05.26.
Wang HF, Zhao DY. Analysis on the characteristics of injury death among the elderly in Laiwu City from 2010 to 2014. Ying yong yu fang yi xue. 2016;22:219–21.
Dong H, Liu HZ, Lin GZ, et al. Causes of injury-related deaths among the elderly aged 60 years and above in Guangzhou City, 2012–2013. Shi yong yu fang yi xue. 2016;23:483–6. https://doi.org/10.3969/j.issn.1006-3110.2016.04.032.
SC Mu, ZH Liu. Causes on accident death of seniors aged 60 and over of Gaotang, 2013–2015. Xian Dai Yu Fang Yi Xue 2016;43:4328–4331+4353.
Liu ZH, Zheng XF. Analysis on epidemiological characteristics of injury death in Gaotang 2008–2012. Xian Dai Yu Fang Yi Xue. 2015;42:1882–5.
Cai P, Wang XH, Chen ZX, et al. Injury death in old population in Jinhua, Zhejiang, 2006–2013. Ji Bing Jian Ce. 2014;9:995–8. https://doi.org/10.3784/j.issn.1003-9961.2014.12.019.
QP Wan, L Quan, GH Zhang, et al. Study on injury mortality in Zhabei District, Shanghai from 2006 to 2012. Zhongguo jian kang jiao yu 2014;30:605–607+626.doi:https://doi.org/10.16168/j.cnki.issn.1002-9982.2014.07.001.
Qin L, Liu Y. Analysis of injury and death characteristics of urban residents in Dandong City from 2006 to 2011. Zhongguo wei sheng tong ji. 2014;31:1032–4.
Bi SF, Bi JB. Analysis of Unexpected Casualties on the Inhabitants in Chifeng City from 2009 to 2013. Nei Menggu yi xue za zhi. 2014;46:594–6. https://doi.org/10.16096/j.cnki.nmgyxzz.2014.05.002.
Chen HJ. Analysis of accidental injury death among the elderly in Ninghai County from 2006 to 2011. Shanghai yu fang yi xue. 2013;25:96–7. https://doi.org/10.19428/j.cnki.sjpm.2013.02.020.
Li L, Liu QM, Jin DF, et al. Causes of injury death in residents in Hangzhou, 2006–2011. Ji Bing Jian Ce. 2013;28:76–9.
Ying JW. Analysis of the causes of accidental injury death of residents in Xianju County from 2008 to 2012. Zhejiang yu fang yi xue. 2013;25:56–8. https://doi.org/10.19485/j.cnki.issn1007-0931.2013.10.016.
Shao YQ. Analysis of the causes of injury and death of residents in Wenzhou, Zhejiang Province, in 2010. Ji Bing Jian Ce. 2012;27:226–9. https://doi.org/10.3784/j.issn.1003-9961.2012.3.018.
Wang QQ, Bao ZF. Analysis of the causes of injury death of residents in Wuyi County. Zhejiang yu fang yi xue. 2012;24:27–9. https://doi.org/10.19485/j.cnki.issn1007-0931.2012.08.009.
Mei QH, Xu GZ, Ying YY. Causes of injury death and its trend in old population in Ningbo in Zhejiang province, 2002–2010. Ji Bing Jian Ce. 2011;26:723–6. https://doi.org/10.3784/j.issn.1003-9961.2011.09.017.
Xu HF, Xu XJ, Weng F, et al. Epidemiological characteristics on fatal injury among the elder in Guangdong Province, 2004–2005. Hua nan yu fang yi xue. 2011;37:27–30.
Zhang YH, Zhu J, Chen JG. An Analysis of Epidemiological Characteristics of Death Due to Injuries in Qidong, 2000–2009. Yi xue yan jiu. 2011;40:119–22. https://doi.org/10.3969/j.issn.1673-548X.2011.12.040.
HY Xie, XY Xu, WJ Ma, et al. Pattern of injury deaths among residents in Guangdong Province, 2004–2005. Hua nan yu fang yi xue 2011;37:17–21+26.
Liang H, Liang XX, Li W. Analysis of the causes of injury and death of residents in Binyang County, Guangxi Province, in 2008. Internal Medicine of China. 2010;5:293–4. https://doi.org/10.16121/j.cnki.cn45-1347/r.2010.03.001.
Zhou L, Xue CY, Liu F, et al. Analysis on the Deaths of Senior Injury in Xuhui District, Shanghai during 2002–2006. J Environ Occup Med. 2008;25:519–21. https://doi.org/10.3969/j.issn.1006-3617.2008.06.003.
Gong HQ, Zhang MR, Yang S, et al. Analysis of accidental injury death among the elderly in Kunming, 2004. Wei sheng ruan ke xue. 2008;22:452–4. https://doi.org/10.3969/j.issn.1003-2800.2008.06.012.
Bai HZ, Hao E, Fang LP, et al. Analysis of injury and death among the elderly in Qingpu District, Shanghai, 2001–2005. Shanghai yu fang yi xue. 2008;20:615–6. https://doi.org/10.3969/j.issn.1004-9231.2008.12.023.
Ni JH, Huang LM, Chen L, et al. Analysis of injury deaths and potential life loss in Songjiang District, Shanghai, 2002–2006. Zhongguo yu fang yi xue. 2008;20:527–30. https://doi.org/10.3969/j.issn.1009-6639.2008.06.022.
YY Peng, XH Tang. Analysis on Death Cause of Accidental Injury of Elderly Population in Jinshan District. Xian Dai Yu Fang Yi Xue 2007;34:1451–1452+1463.doi:https://doi.org/10.3969/j.issn.1003-8507.2007.08.021.
Hu XQ, He YZ. Analysis of mortality and injuries of residents in Yuyao City. Zhongguo re dai yi xue. 2007;7:476–8. https://doi.org/10.3969/j.issn.1009-9727.2007.03.086.
Yang JZ, Yuan F, Lu ZG, et al. Analysis of Death Causes of the Elderly in Guiyang City, 2002–2004. Zhonghua lao nian yi xue za zhi. 2006;25:930–1. https://doi.org/10.3760/j:issn:0254-9026.2006.12.014.
Sun XK, Liu RH, Xu H. Analysis of injury deaths among residents of Yancheng City in 2005. Jiangsu wei sheng bao jian. 2006;8:8–10. https://doi.org/10.3969/j.issn.1008-7338.2006.05.004.
Yang GH, Zhou MG, Huang ZJ, et al. Study on the trend and disease burden of injury deathes in Chinese population, 1991–2000. Zhonghua Liu Xing Bing Xue Za Zhi. 2004;25:193–8. https://doi.org/10.3760/j.issn:0254-6450.2004.03.004.
Hu G, Baker SP. Recent increases in fatal and non-fatal injury among people aged 65 years and over in the USA. Inj Prev. 2010;16:26–30. https://doi.org/10.1136/ip.2009.023481.
Gawryszewski VP, de Mello Jorge MH, Koizumi MS. Mortes e internações por causas externas entre os idosos no Brasil: o desafio de integrar a saúde coletiva e atenção individual [Injury among the elderly: the challenge to integrate preventive activities in public and individual levels. Rev Assoc Med Bras. 1992;2004(50):97–103. https://doi.org/10.1590/s0104-42302004000100044.
Petridou ET, Dikalioti SK, Dessypris N, et al. The evolution of unintentional injury mortality among elderly in Europe. J Aging Health. 2008;20:159–68. https://doi.org/10.1177/0898264307310467.
He LY, Yang Z, Pang GF, et al. Research Progress on biomarkers of aging and healthy environment for the elderly. Zhongguo lao nian bao jian yi xue. 2020;18:15–8. https://doi.org/10.3969/j.issn.1672-2671.2020.06.005.
Zhang MG, Zhou YB, Li CC, et al. Levels and trends of significant injury-caused deaths in the Chinese population, 2010–2019. Chinese Journal of Epidemiology. 2022;43:871–7.
Xiang KB, Jiang KH, Zhang DL. Social Security Expenditure, Regional Disparities, and Active Aging. East China Economic Management. 2022;36:9–20. https://doi.org/10.19629/j.cnki.34-1014/f.210611004.
Li LL. Analysis of regional differences and influencing factors of population aging in China. Hua Zhong Nong Ye Da Xue Xue Bao. 2017;06:94–102. https://doi.org/10.13300/j.cnki.hnwkxb.2017.06.012.
Yu S. Problems and paths of economic development in Northeast China based on the theory of unbalanced development. Social Scientist. 2021;294:86–92.
Liang BY, Qian S, Zhang WQ. Study of spatial distribution and rationality of medical conditions in Chinese provinces. China Health Statistics. 2017;34:455–8.
Liu JG, Lv GJ. Planning of Zhengzhou railroad hub. J Railway Eng. 2014;31:5–10.
YL Zhang, WC Jing. China has crossed the first Lewis turning point-On China's demographic transition, structural transition and Lewis turning point. The World of Survey and Research 2012;(12):13–16+20. https://doi.org/10.3969/j.issn.1004-7794.2012.12.004.
Liang XF. Promotion and application on the injury prevention strategy research in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2015;36:1–2. https://doi.org/10.3760/cma.j.issn.0254-6450.2015.01.001.
Y Liu, H Mi. Living Environmental Risk Factors Contributing to Falls among Chinese Older Adults: Base on the 2015 SSAPUR Data. Population and Development 2021;27:123–132+109.
Duan LL, Deng X, Zhang R, et al. Analysis of road traffic injuries in China, 1995–2005. Zhongguo wei sheng tong ji. 2007;24:297–9. https://doi.org/10.3969/j.issn.1002-3674.2007.03.025.
Gao X, Wang LH, Jin Y, et al. Disease burden caused by suicide in the Chinese population, in 1990 and 2013. Zhonghua Liu Xing Bing Xue Za Zhi. 2017;38:1325–9. https://doi.org/10.3760/cma.j.issn.0254-6450.2017.10.006.
YN Li, YQ Wang. Prevalence and Patterns of Multimorbidity among Chinese Elderly People. Zhongguo quan ke yi xue 2021;24:3955–3962+3978. https://doi.org/10.12114/j.issn.1007-9572.2021.00.295.
Wang LM, Chen ZH, Zhang M, et al. Study of the prevalence and disease burden of chronic disease in the elderly in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2019;40:277–83. https://doi.org/10.3760/cma.j.issn.0254-6450.2019.03.005.
National Bureau of Statistics. Population development in China presents new characteristics and trends. (2021–5–13)[2022–2–9].http://www.stats.gov.cn/xxgk/jd/sjjd2020/202105/t20210513_1817408.html.
L Zhang, Ding Z, Qiu L, et al. Falls and risk factors of falls for urban and rural community-dwelling older adults in China. BMC Geriatr 2019;19:379. https://doi.org/10.1186/s12877-019-1391-9.
Acknowledgements
N/A.
Funding
This work was supported by the National Natural Science Foundation of China [81960620, 81360446], the Sub-project under National Key Research and Development Program [2020YFC2002901], and the Natural Fund Project of Jiangxi Provincial Department of Science and Technology [20192BAA208005].
Author information
Authors and Affiliations
Contributions
Y.SL analyzed and interpreted the data, and was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, Sl., Zhang, Ll., Zhu, X. et al. Big data on the prevalence of injury deaths among 187 488 elderly Chinese in the past 20 years (2000–2020): a systematic review and meta-analysis. BMC Geriatr 23, 340 (2023). https://doi.org/10.1186/s12877-023-04056-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-023-04056-0