
Abstract
Background
Lobar pneumonia caused by Mycoplasma pneumoniae is a relatively difficult-to-treat pneumonia in children. The time of radiographic resolution after treatment is variable, a long recovery time can result in several negative effects, and it has attracted our attention. Therefore, exploring factors associated with delayed radiographic resolution will help to identify these children at an early stage and prepare for early intervention.
Methods
The data of 339 children with lobar pneumonia caused by Mycoplasma pneumoniae were collected from the Department of Pediatrics of Fu Yang People’s Hospital, China from January 2021 to June 2022. After discharge, the children were regularly followed up in the outpatient department and on the WeChat platform for > 8 weeks. According to whether pulmonary imaging (chest radiography or plain chest computed tomography) returned to normal within 8 weeks, the children were divided into the delayed recovery group (DRG) (n = 69) and the normal recovery group (NRG) (n = 270). The children’s general information, laboratory examination findings, bronchoscopy results, and imaging findings were retrospectively analyzed. Single-factor analysis was performed to identify the risk factors for delayed radiographic resolution of lobar pneumonia caused by Mycoplasma pneumoniae, and the factors with statistically significant differences underwent multiple-factor logistic regression analysis. Receiver operating characteristic (ROC) analysis was then performed to calculate the cutoff value of early predictive indicators of delayed radiographic resolution.
Results
Single-factor analysis showed that the following were significantly greater in the DRG than NRG: total fever duration, the hospitalization time, C-reactive protein (CRP) level, lactate dehydrogenase (LDH) level, D-dimer level, pulmonary lesions involving two or more lobes, a large amount of pleural effusion, the time to interventional bronchoscopy, and mucus plugs formation. Multivariate logistic regression analysis showed that the hospitalization time, CRP level, LDH level, pulmonary lesions involving two or more lobes, and a large amount of pleural effusion were independent risk factors for delayed radiographic resolution of lobar pneumonia caused by Mycoplasma pneumoniae. The cutoff values on the receiver operating characteristic curve were a hospitalization time of ≥ 10.5 days, CRP level of ≥ 25.92 mg/L, and LDH level of ≥ 378 U/L.
Conclusion
If patients with lobar pneumonia caused by Mycoplasma pneumoniae have a hospitalization time of ≥ 10.5 days, CRP level of ≥ 25.92 mg/L, and LDH level ≥ 378 U/L, the time of radiographic resolution is highly likely to exceed 8 weeks. Pediatricians must maintain a high level of vigilance for these factors, control the infection as early as possible, strengthen airway management, and follow up closely to avoid complications and sequelae of Mycoplasma pneumoniae pneumonia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lobar pneumonia is a common type of Mycoplasma pneumoniae pneumonia (MPP) in children, and it is typically a mild condition that responds well to macrolide antibiotics (MAs). A follow-up study revealed that in approximately 70% of children’s pulmonary imaging changes can return to normal within 8 weeks when antibiotics and glucocorticoids are used appropriately [1, 2]. In some children, however, the time of radiographic resolution significantly exceeds 8 weeks. When the clinical condition is accompanied by necrotizing pneumonia, the time of radiographic resolution can reach 6 months [3], significantly impacting the patient’s quality of life. Furthermore, children with long-term lung lesions may develop persistent fever, impaired lung function, and worsening of the disease [4, 5].
This study was performed to identify predictors that can be used for early prediction of delayed radiographic resolution of lobar pneumonia caused by Mycoplasma pneumoniae (M. pneumoniae) in children, thus facilitating early interventions to prevent serious complications such as necrotizing pneumonia, bronchiectasis, and bronchial occlusion.
Patients and methods
Patients
We retrospectively analyzed the data of 339 children with lobar pneumonia caused by M. pneumoniae who were admitted to the Department of Pediatrics of Fu Yang People’s Hospital from 1 January 2021 to 30 June 2022. The children were divided into a normal recovery group (NRG) (n = 270) and a delayed recovery group (DRG) (n = 69) (Fig. 1). The research protocol was approved by the Ethical Committee of Fu Yang People’s Hospital (ethical code: 2018 − 167).

Flow chart of patient selection
Inclusion and exclusion criteria
The inclusion criteria were (1) chest radiography or lung computed tomography findings consistent with the imaging characteristics of lobar pneumonia and (2) satisfaction of the diagnostic criteria for MPP in the Expert Consensus on Laboratory Diagnostics and Clinical Practice of Mycoplasma pneumoniae Infection in Children in China (i.e., manifestations of pneumonia and/or imaging changes combined with an MP antibody titer of ≥ 1:160) [6].
The exclusion criteria were (1) infection with other pathogens, (2) immunodeficiency, (3) lack of bronchoscopy with bronchoalveolar lavage, (4) incomplete medical records, and (5) loss to follow-up.
Data collection
The following data were retrospectively collected from the children’s medical records. (1) Clinical data: age, sex, total fever duration, peak body temperature, hospitalization time, season of onset, and time to interventional bronchoscopy ( The “time” refers to the interval from the onset of illness to undergoing bronchoscopy with bronchoalveolar lavage, it is not a treatment time.). (2) Laboratory examination findings: including white blood cell count (WBC), neutrophil ratio (NE%), lymphocyte ratio (LYM%), C-reactive protein (CRP) level, D-dimer level, lactate dehydrogenase (LDH) level, alkaline phosphatase (ALP) level, and immunoglobulins A, M, and G (IgA, IgM, IgG). (3) Other conditions: glucocorticoid resistance, a large amount of pleural effusion, atelectasis, lung lesions involving two or more lobes, and mucus plugs formation as shown by bronchoscopy. A retrospective analysis was performed to understand the relationship between the above factors and delayed radiographic resolution of lobar pneumonia caused by M. pneumoniae in children.
Definitions
(1) According to previous reports, the time of radiographic resolution in most patients with lobar pneumonia caused by M. pneumoniae is 1 to 2 months [7,8,9]. Therefore, we defined delayed radiographic resolution as lack of recovery on chest radiographs or lung computed tomography scans from admission to 8 weeks of treatment. Radiologic follow-up was performed every 4 weeks.
(2) MAs non-responsiveness was defined as a persistent fever in a child with MPP after 72 h of regular MAs treatment, with either no improvement in clinical signs and pulmonary imaging findings or the development of further aggravation [10].
(3) Glucocorticoid resistance was defined as a persistent fever for > 72 h after intravenous administration of methylprednisolone at 1 to 2 mg/kg per day [11, 12].
(4) A large amount of pleural effusion was defined as a total pleural fluid volume of ≥ 500 mL and a low to medium volume of pleural effusion was defined as a total pleural fluid volume of < 500 mL.
Bronchoscopy with bronchoalveolar lavage
All children in this study received routine anti-infection therapy and nebulization for 3 days after admission. If the children still had persistent fever, persistent cough, and no significant improvement in pulmonary signs, bronchoscopy with bronchoalveolar lavage was recommended. The alveolar lavage fluid was reserved for pathogenic nucleic acid detection after obtaining written informed consent from the child’s family. The equipment used for bronchoscopy with alveolar lavage is PENTAX fiber bronchoscopy (device model: EB-1170 K).
Patients were discharged when the rales disappeared, and the body temperature was normal for ≥ 3 consecutive days after completing routine anti-infective and anti-inflammatory treatment and bronchoscopy with bronchoalveolar lavage.
Statistical analysis
The data were analyzed using SPSS 25.0 software (IBM Corp., Armonk, NY, USA). Measurement data conforming to a normal distribution are presented as mean ± standard deviation, and data with a skewed distribution are presented as median with interquartile range (Q25–Q75). Comparisons between groups were performed with the t-test or Mann–Whitney U test [13]. Enumerated data are expressed as rates, and the χ2 test was used for comparison between groups. We conducted a single-factor analysis to identify the risk factors for delayed radiographic resolution. We then conducted a multivariate logistic regression analysis of statistically significant factors to summarize the high-risk factors. Finally, the relevant factors were analyzed using a receiver operating characteristics (ROC) curve, and the early predictors of delayed radiographic resolution were summarized. Two-sided P˗values of < 0.05 were considered statistically significant.
Results
Clinical features
General information
A total 339 children with lobar pneumonia caused by M. pneumoniae were divided into 270 cases with NRG and 69 cases with DRG. The mean age at onset was 7.17 ± 2.37 years in the NRG and 6.86 ± 1.50 years in the DRG. The male: female ratio was approximately 1.4:1.0 (NRG vs. DRG). There was no significant difference in sex, season of onset, or age between the two groups. Total fever duration and hospitalization time were significantly longer in the DRG than NRG (P < 0.05). The time to interventional bronchoscopy was significantly longer in the DRG than NRG (11.06 ± 3.53 vs. 9.03 ± 2.76 days, respectively) (Table 1).
NRG, normal recovery group; DRG, delayed recovery group.
Laboratory test results
Comparison of the laboratory examination results between the two groups showed that the CRP, D˗dimer, and LDH levels were significantly higher in the DRG than NRG (P < 0.05). There were no significant differences in the white blood cell count, neutrophil ratio, lymphocyte ratio, alkaline phosphatase level, or immunoglobulin levels (P > 0.05) (Table 2).
Other conditions
There were statistically significant differences in glucocorticoid resistance, a large amount of pleural effusion, atelectasis, pulmonary lesions involving two or more lung lobes, and mucus plugs formation between the NRG and DRG (P < 0.05). However, the incidence of MAs non-responsiveness was not significantly different between the two groups (Table 3).
Multivariate logistic regression analysis
The statistically significant factors in the above-described univariate analysis were taken as independent variables, and whether delayed recovery had occurred was taken as the dependent variable (no = 0, yes = 1); a binary logistic regression analysis was then performed. The final results showed that the hospitalization time [odds ratio (OR) = 1.584, 95% confidence interval (CI) = 1.082–2.321, P = 0.018], LDH level (OR = 1.022, 95% CI = 1.008–1.036, P = 0.002), CRP level (OR = 1.079, 95% CI = 1.045–1.114, P < 0.001), pulmonary lesions involving two or more lung lobes (OR = 8.997, 95% CI = 1.698–47.682, P = 0.010), and a large amount of pleural effusion (OR = 11.568, 95% CI = 1.767–75.728, P = 0.011) were independent risk factors for delayed radiographic resolution of lobar pneumonia caused by M. pneumoniae in children (P < 0.05) (Table 4).
ROC curve regression analysis
The cutoff values for maximum sensitivity and specificity of predictive indicators were determined according to Youden’s method. The results showed that the cutoff values for predictive indicators were a hospitalization duration of ≥ 10.5 days, CRP level of ≥ 25.92 mg/L, and LDH level of ≥ 378 U/L. The corresponding area under the curve was 0.835, 0.944, and 0.917; the sensitivity was 0.667, 0.913, and 0.812; and the specificity was 0.844, 0.844, and 0.900, respectively (Fig. 2; Table 5).

Receiver operating characteristic curve of predictive value of hospital stay, CRP level, and LDH level on delayed radiographic resolution in children with lobar pneumonia induced by Mycoplasma pneumoniae CRP, C-reactive protein; LDH, lactate dehydrogenase
Prognosis
Comparing the prognosis of two groups of children, it was found that the patients of DGR had an increased risk of adverse prognosis (P < 0.05), such as necrotizing pneumonia, bronchiectasis, obliterative bronchiolitis and recurrent wheezing. The top two are recurrent wheezing and necrotizing pneumonia. They account for 47.8% and 36.2%, respectively (Table 6).
Discussion
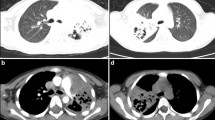
Lobar pneumonia caused by M. pneumoniae in children often presents as pulmonary lobe or segmental consolidation (37%) and slightly less commonly as, infiltration near the hilum or around the bronchus (27%), local reticularis nodule infiltration (21%), and patchy infiltration (15%) [14]. Unilateral pulmonary lobe involvement is more common than bilateral involvement. Imaging examination is one of the main bases for clinical severity and prognosis assessment. In this study, we found that children in the DRG were more likely to have a worsened prognosis. Delayed radiographic resolution may lead to necrotizing pneumonia, bronchiolitis obliterans, bronchiectasis, and recurrent wheezing, their incidence increases in DRG significantly. After the above-mentioned situations occur, almost all patients will experience worsening pulmonary function and decreased exercise tolerance. Therefore, in order to strengthen post-discharge management, early identification of these children is necessary.
This study involved 339 children with MPP who showed lobar changes on lung imaging. The children’s clinical features, laboratory examination findings, and bronchoscopic findings were retrospectively analyzed, and the risk factors for delayed radiographic resolution were summarized. Univariate analysis showed statistically significant differences between the NRG and DRG in the CRP level, LDH level, total fever duration, hospitalization time, glucocorticoid resistance, a large amount of pleural effusion, pulmonary lesions involving two or more lung lobes, and atelectasis (P < 0.05). Further analysis using a multivariate logistic regression model and ROC curve showed that a of hospitalization time of ≥ 10.5 days, CRP level of ≥ 25.92 mg/L, LDH level of ≥ 378 U/L, pulmonary lesions involving two or more lung lobes, and a large amount of pleural effusion were risk factors for delayed radiographic resolution of lobar pneumonia caused by M. pneumoniae in children. Radiographic resolution of pneumonia is affected by multiple factors, which are generally divided into two categories: factors related to the disease severity and factors related to the treatment effect. The more risk factors are combined in the same children, the greater the probability of delayed radiographic recovery.
More severe clinical features and higher laboratory indicators may be associated with delayed radiographic recovery. Lobar pneumonia caused by M. pneumoniae occurs mostly in children aged >5 years, because their immune function is stronger, their autoimmune reaction after M. pneumoniae infection is stronger, and lung tissue damage is more serious than in children aged < 5 years. Zhao et al. [15] found that age had an impact on the prognosis of children with MPP, and the critical age threshold was 4.5 years. The mean age of the children in the NRG and DRG in this study was 7.17 ± 2.37 and 6.86 ± 1.50 years respectively, both were above the threshold of 4.5 years, and there was not find any impact of age on the prognosis of the two groups of patients. Patients in the DRG had a longer hospital stay (12.70 vs. 8.36 days) and a longer fever duration (11.13 vs. 6.34 days) than those in the NRG. Moreover, the levels of CRP (57.18 vs. 10.61 mg/L), LDH (515.00 vs. 307.99 U/L), and D-dimer (3.18 vs. 0.85 mg/L) were higher in the DRG than NRG. These findings suggest that the pulmonary inflammatory reaction or tissue damage was more severe in the DRG [16]. An elevated CRP level is an early indicator of lung tissue necrosis, indicating a systemic inflammatory reaction secondary to severe lung infection. Additionally, studies have suggested that the incidence of pleural effusion, myocardial injury, and liver injury is remarkably increased in children who have MPP with elevated indices [17, 18]. Such findings are consistent with the slower radiographic resolution seen in the children in the DRG of our study. The multivariate logistic regression analysis showed that the CRP and LDH levels were independent risk factors for delayed radiographic resolution, and the ROC curve analysis showed that the CRP and LDH levels (area under the curve = 0.944 and 0.917, respectively) had high predictive value for delayed radiographic resolution.
Several serious complications can lead to delayed radiographic resolution of pneumonia. The most common complications of M. pneumoniae-induced lobar pneumonia include pleural effusion, atelectasis, and mucus plugs formation, which seriously affect the recovery of lung imaging. Kim et al. [19] showed that children who had MPP with pleural effusion had more severe pneumonia lesions and poorer responses to treatment, resulting in prolonged radiographic resolution of lung abnormalities. In other studies, a large amount of pleural effusion was closely associated with the occurrence of necrotic pneumonia [2, 8, 20]. The imaging changes of necrotic pneumonia were characterized by the emergence of voids after destruction of the lung parenchymal structure, and the radiographic resolution of necrotic pneumonia was thus slower than that of common pneumonia. Undoubtedly, children with extensive pulmonary inflammatory lesions had a longer recovery time. In this study, 70% (235/339) of the children had a single pulmonary lobe lesion, and only 30% of the children had lung lesions involving more than two pulmonary lobes. It indicates that lobar pneumonia caused by M. pneumoniae is usually characterized by involvement of a single pulmonary lobe. Notably, however, 72.5% of the children in the DRG had pulmonary lesions involving two or more lobes, suggesting that once inflammatory lesions involve multiple lobes, the recovery period is prolonged. The formation of mucus plugs is an important manifestation of progressive airway mucosal damage, which can lead to irreversible airway dysventilation and atelectasis. Zhang et al. [21] found that children with mucus plugs formation were more likely to have intrapulmonary complications such as pleural effusion and extrapulmonary complications, making treatment more difficult and inflammation more persistent.
Factors related to the treatment effect have slightly different effects on radiographic resolution of pneumonia. Such factors include MAs non-responsiveness, glucocorticoid resistance, and the time to interventional bronchoscopy. Effective antimicrobial and anti-inflammatory therapy helps control disease and shorten the acute phase of disease. MAs therapy is still the first choice for the treatment of M. pneumoniae infection, MAs inhibit protein synthesis to achieve an anti-infection effect by binding to domain II and/or V of 23 S rRNA in the ribosomal subunit of 50 S bacteria. In recent years, however, the rate of resistance to MAs has shown an increasing trend. Wang et al. [22] found that 90.94% (1386/1524) of specimens from 1524 children with MPP were resistant to MAs. Gene mutation in the 23 S rRNA domain V of M. pneumoniae is the main mechanism of MAs resistance, and A2063 G/C, A2064 G/C, and C2617 G/A have been shown to be mutation sites of MAs resistance [23, 24]. In the study, the rate of MAs non-responsiveness was 38.9% and 50.7% in the NRG and DRG, respectively, with no statistically significant difference between the two groups. This finding indicates that MAs non-responsiveness did not affect the radiographic resolution in children with MPP, which is consistent with the results of reported by Deng et al. [25]. Additionally, Chen et al. [26] stated that MAs resistance may prolong fever duration and treatment time, but the chest X-ray examination findings and laboratory test indicators did not change accordingly. Glucocorticoids are used as immunomodulators to suppress overactive host immune responses, reduce the intensity of local inflammation, and promote recovery from disease. Patients with glucocorticoid resistance often have more severe clinical manifestations and imaging abnormalities. A strong cellular immune response will lead to severe ciliary dysfunction, reduce airway immune function, and destroy ciliary mucus clearance ability, these changes will result in large-scale infiltration, atelectasis, and mucus plugs formation, seriously affecting the recovery of lung inflammation. Bronchoscopy with bronchoalveolar lavage is a rapid and effective treatment for relieving clinical symptoms. Many studies have shown that bronchoscopy with bronchoalveolar lavage is beneficial for removing mucus plugs and has significant advantages for patients with pneumonia characterized by persistent atelectasis [27, 28]. Disease remission has been shown to become greatly accelerated after intervention of bronchoalveolar lavage [29]. The study also showed that the time to interventional bronchoscopy was shorter in NRG than DRG, and early treatment with bronchoalveolar lavage was conducive to the improvement of imaging.
No single clinical or biochemical indicator can accurately predict whether delayed radiographic resolution of pulmonary abnormalities will occur. We performed a multiple logistic regression analysis and ROC curve analysis to eliminate the confounding among study factors and objectively examine the clinical factors influencing delayed radiographic resolution in children with lobar pneumonia caused by M. pneumoniae. However, this study also had some limitations; for example, it is a single-center study, some patients were lost to follow-up, and some patients were excluded because of incomplete data or lack of bronchoscopy with bronchoalveolar lavage, which may have biased the results. The sample size should be increased for in further studies. We followed up on the pulmonary function of some patients in the DRG and found that they had varying degrees of decreased pulmonary function. However, pulmonary function tests could not be conducted on young patients (< 6 years old) who were unable to cooperate, preventing an assessment of their pulmonary function. This article also has the shortcoming of not making a comprehensive comparison of pulmonary function.
Conclusion
In the study, we found that delayed radiographic resolution was mainly associated with the development of complications and high levels of inflammatory markers. Patients with lung lesions involving two or more lobes, a large amount of pleural effusion, high levels of inflammatory markers (CRP level of ≥ 25.92 mg/L, LDH level of ≥ 378 U/L), or a long hospital stay (a hospitalization time of ≥ 10.5 days) had longer radiographic resolution. These five factors are closely related to radiographic resolution, and pediatrician should pay attention to them in our clinical work. These findings may help to identify these patients early in the course of their disease and enhance patient management after discharge.
Data availability
Underlying research data and materials can be accessed by contacting the corresponding author.
Abbreviations
- DRG:
-
Delayed recovery group
- NRG:
-
Normal recovery group
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under the curve
- CI:
-
Confidence interval
- OR:
-
Odds ratio
- MPP:
-
Mycoplasma Pneumoniae Pneumonia
- MAs:
-
Macrolide antibiotics
- WBC:
-
White blood cell count
- NE%:
-
Neutrophil ratio
- LYM%:
-
Lymphocyte ratio
- CRP:
-
C-reactive protein
- D-D:
-
D-dimer
- LDH:
-
Lactate dehydrogenase
- ALP:
-
Alkaline phosphatase
- IgA:
-
Immunoglobulin A
- IgM:
-
Immunoglobulin M
- IgG:
-
Immunoglobulin G
References
Huang L, Huang X, Jiang W, Zhang R, Yan Y, Huang L. Independent predictors for longer radiographic resolution in patients with refractory Mycoplasma pneumoniae pneumonia: a prospective cohort study. BMJ Open. 2018;8(12):e023719.
Yang B, Zhang W, Gu W, Zhang X, Wang M, Huang L, et al. Differences of clinical features and prognosis between Mycoplasma pneumoniae necrotizing pneumonia and non-Mycoplasma pneumoniae necrotizing pneumonia in children. BMC Infect Dis. 2021;21(1):797.
Li SR, Mu JH, Chang L, Yan YC, Yuan XY, Chen HZ. [Chest CT features and outcome of necrotizing pneumonia caused by Mycoplasma pneumoniae in children (report of 30 cases)]. Zhonghua Er Ke Za Zhi. 2013;51(3):211–5.
Chen Y, Li L, Wang C, Zhang Y, Zhou Y. Necrotizing Pneumonia in Children: early recognition and management. J Clin Med. 2023;12(6):2256.
Tsai TA, Tsai CK, Kuo KC, Yu HR. Rational stepwise approach for Mycoplasma pneumoniae pneumonia in children. J Microbiol Immunol Infect. 2021;54(4):557–65.
Expert Committee on Rational Use of Medicines for Children Pharmaceutical Group, National Health and Family Planning Commission. [Expert consensus on laboratory diagnostics and clinical practice of Mycoplasma pneumoniae infection in children in China (2019)]. Zhonghua Er Ke Za Zhi. 2020;58(5):366–73.
Luo Y, Dai J, Tang G, He S, Fu W. Development and validation of a simple-to-use nomogram for predicting the delayed radiographic recovery in children with mycoplasma pneumoniae pneumonia complicated with atelectasis. J Investig Med. 2023:10815589231169686.
Wang X, Zhong LJ, Chen ZM, Zhou YL, Ye B, Zhang YY. Necrotizing pneumonia caused by refractory Mycoplasma pneumoniae pneumonia in children. World J Pediatr. 2018;14(4):344–9.
Zhang L, Wang L, Xu S, Li H, Chu C, Liu Q, et al. Low-dose corticosteroid treatment in Children with Mycoplasma pneumoniae Pneumonia: a retrospective cohort study. Front Pediatr. 2020;8:566371.
Bae E, Kim YJ, Kang HM, Jeong DC, Kang JH. Macrolide versus non-macrolide in combination with steroids for the treatment of Lobar or Segmental Mycoplasma pneumoniae Pneumonia unresponsive to initial Macrolide Monotherapy. Antibiot (Basel). 2022;11(9):1233.
Liu J, He R, Zhang X, Zhao F, Liu L, Wang H, et al. Clinical features and early corticosteroid treatment outcome of pediatric mycoplasma pneumoniae pneumonia. Front Cell Infect Microbiol. 2023;13:1135228.
Yan Q, Niu W, Jiang W, Hao C, Chen M, Hua J. Risk factors for delayed radiographic resolution in children with refractory Mycoplasma pneumoniae pneumonia. J Int Med Res. 2021;49(5):3000605211015579.
Lee SW. Methods for testing statistical differences between groups in medical research: statistical standard and guideline of Life Cycle Committee. Life Cycle. 2022;2:e1.
Cho YJ, Han MS, Kim WS, Choi EH, Choi YH, Yun KW, et al. Correlation between chest radiographic findings and clinical features in hospitalized children with Mycoplasma pneumoniae pneumonia. PLoS ONE. 2019;14(8):e0219463.
Zhao Q, Zhang T, Zhu B, Bi Y, Jiang SW, Zhu Y, et al. Increasing age affected Polymorphonuclear neutrophils in Prognosis of Mycoplasma pneumoniae Pneumonia. J Inflamm Res. 2021;14:3933–43.
Lee E, Choi I. Clinical usefulness of serum lactate dehydrogenase levels in Mycoplasma pneumoniae Pneumonia in Children. Indian J Pediatr. 2022;89(10):1003–9.
Fan F, Lv J, Yang Q, Jiang F. Clinical characteristics and serum inflammatory markers of community-acquired mycoplasma pneumonia in children. Clin Respir J. 2023;17(7):607–17.
Qiu J, Ge J, Cao L. D-dimer: the risk factor of children’s severe Mycoplasma Pneumoniae Pneumonia. Front Pediatr. 2022;10:828437.
Kim SH, Lee E, Song ES, Lee YY. Clinical significance of Pleural Effusion in Mycoplasma pneumoniae Pneumonia in Children. Pathogens. 2021;10(9):1075.
Zheng B, Zhao J, Cao L. The clinical characteristics and risk factors for necrotizing pneumonia caused by Mycoplasma pneumoniae in children. BMC Infect Dis. 2020;20(1):391.
Zhang J, Wang T, Li R, Ji W, Yan Y, Sun Z, et al. Prediction of risk factors of bronchial mucus plugs in children with Mycoplasma pneumoniae pneumonia. BMC Infect Dis. 2021;21(1):67.
Wang Y, Xu B, Wu X, Yin Q, Wang Y, Li J, et al. Increased Macrolide Resistance Rate of M3562 Mycoplasma pneumoniae correlated with macrolide usage and genotype shifting. Front Cell Infect Microbiol. 2021;11:675466.
Zhan XW, Deng LP, Wang ZY, Zhang J, Wang MZ, Li SJ. Correlation between Mycoplasma pneumoniae drug resistance and clinical characteristics in bronchoalveolar lavage fluid of children with refractory Mycoplasma pneumoniae pneumonia. Ital J Pediatr. 2022;48(1):190.
Wang N, Xu X, Xiao L, Liu Y. Novel mechanisms of macrolide resistance revealed by in vitro selection and genome analysis in Mycoplasma pneumoniae. Front Cell Infect Microbiol. 2023;13:1186017.
Deng H, Rui J, Zhao D, Liu F. Mycoplasma pneumoniae 23S rRNA A2063G mutation does not influence chest radiography features in children with pneumonia. J Int Med Res. 2018;46(1):150–7.
Chen YC, Hsu WY, Chang TH. Macrolide-resistant Mycoplasma pneumoniae infections in Pediatric Community-Acquired Pneumonia. Emerg Infect Dis. 2020;26(7):1382–91.
Li F, Zhu B, Xie G, Wang Y, Geng J. Effects of bronchoalveolar lavage on pediatric refractory mycoplasma pneumoniae pneumonia complicated with atelectasis: a prospective case-control study. Minerva Pediatr (Torino). 2021;73(4):340–7.
Su DQ, Li JF, Zhuo ZQ. Clinical analysis of 122 cases with Mycoplasma Pneumonia complicated with atelectasis: a retrospective study. Adv Ther. 2020;37(1):265–71.
Wang L, Xie Q, Xu S, Li H, Zhang L, Ai J, et al. The role of flexible bronchoscopy in children with Mycoplasma pneumoniae pneumonia. Pediatr Res. 2023;93(1):198–206.
Acknowledgements
The author thanks all patients enrolled in this study.
Funding
This work was supported by Fu Yang Self-funded Science and Technology Plan Project (FK202081038).
Author information
Authors and Affiliations
Contributions
Y. Z. and Y. Z. were responsible for the conception and design of the paper, statistical processing, analysis and interpretation of the results, and the final writing of the paper. H. D. and G. L. were responsible for bronchoscopic treatment and follow-up observation of patients, and carried out the implementation and feasibility analysis of the study. L. L. and X. C. are responsible for data collection and collation. Y. Z. and G. M. are responsible for the quality control and proofreading of the article, as well as the overall supervision and management of the article. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The performed study’s protocol was following the principles of the declaration of Helsinki and approved by the Ethical Committee of Fu Yang People’s Hospital (2018 − 167). The informed consent was waived by the Ethical Committee of Fu Yang People’s Hospital due to retrospective nature of study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zheng, Y., Mao, G., Dai, H. et al. Early predictors of delayed radiographic resolution of lobar pneumonia caused by Mycoplasma pneumoniae in children: a retrospective study in China. BMC Infect Dis 24, 414 (2024). https://doi.org/10.1186/s12879-024-09289-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09289-x