
Abstract
Purpose
To explore the risk factors for cognitive impairment in patients undergoing maintenance hemodialysis (MHD) and construct a predictive model for cognitive impairment.
Methods
A total of 146 patients with end-stage renal disease (ESRD) undergoing MHD were recruited at our hospital between December 2021 and April 2022. Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA), and scores of < 26 were considered indicative of cognitive impairment. Risk factors were identified using a multivariate logistic regression model, and a receiver operating characteristic curve was applied to construct the prediction model. Cognitive impairment risk was categorized using a multifactorial prediction model based on the weight of evidence.
Results
46 patients with cognitive impairment were identified, with a prevalence of 31.5% in ESRD patients undergoing MHD. Multivariate logistic regression analyses indicated that the following factors were associated with an increased risk of cognitive impairment in patients undergoing MHD: aged 55.0–64.0 years (OR:6.24; 95%CI:1.81–21.48; P = 0.001), aged 65.0–74.0 years (OR:16.10; 95%CI:4.03–64.37; P < 0.001), aged ≥ 75.0 years (OR:90.22; 95%CI:16.86-482.86; P < 0.001), duration of dialysis ≥ 5 years (OR:3.99; 95%CI:1.58–10.04; P = 0.003), and current smoker (OR:4.61; 95%CI:1.46–14.57; P = 0.009). The predictive value of the constructed model based on the aforementioned factors for cognitive impairment was 84% (95%CI,77-91%). The prevalence of cognitive impairment for patients at low, moderately low, moderately high, and high risk was 0% (95%CI:0-17%), 10% (95%CI:3-22%), 32% (95%CI:16-52%), and 65% (95%CI:50-78%), respectively.
Conclusions
This study constructed a multifactorial prediction model with a high predictive value for cognitive impairment in patients with ESRD undergoing MHD.
Similar content being viewed by others
Introduction
Chronic kidney disease (CKD) is present in one-eighth of the adult population, and this proportion rises to one-third for individuals aged over 65 years [1, 2]. CKD has been significantly associated with an elevated risk of cardiovascular and cerebrovascular diseases, end-stage renal disease (ESRD), and early mortality [3,4,5]. CKD is an independent risk factor for dementia and cognitive impairment [6]. Studies have found that changes in cognitive impairment begins at the early stage of CKD, and that there is a strong relationship between decreased kidney function and impaired cognition [7, 8]. The prevalence of cognitive impairment in patients with CKD, and ESRD especially, can reach 80% [9, 10]. Informed decisions and compliance with dialysis activities could be affected by cognitive impairment, which is considered an independent risk factor for mortality in ESRD patients undergoing hemodialysis [11,12,13]. Thus, identifying cognitive impairment is particularly important for early prevention and slowing the progression of cognitive decline in patients undergoing maintenance hemodialysis (MHD).
The potential causes of cognitive impairment in patients are multifactorial, including cerebrovascular lesions [14], hypotension [15], serological markers [16], social history [17], and frequency of hemodialysis [18]. Moreover, several studies have illustrated the impact factors for cognitive impairment in patients undergoing hemodialysis and identified predictive factors, including older age, duration of education, undergoing hemodialysis, hemoglobin level, depression, and smoking [19,20,21]. Identifying MHD patients at high risk for cognitive impairment is particularly important; however, no prediction model has been constructed to predict cognitive impairment in MHD patients. Therefore, the current study was performed to identify potential predictive factors for cognitive impairment in patients undergoing MHD, and a prediction model was constructed based on these identified predictive factors. Furthermore, a categorical risk-scoring system was created to evaluate the risk of cognitive impairment in patients undergoing MHD in a specific risk category.
Materials and methods
Population
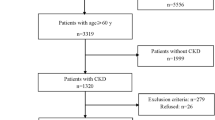
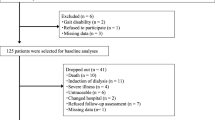
ESRD patients undergoing MHD in our hospital between December 2021 and April 2022 were collected retrospectively. Patients were included if they met the following criteria: (1) age ≥ 18.0 years; (2) regular hemodialysis ≥ 3.0 months; and (3) ability to complete the cognitive function questionnaire. The exclusion criteria were as follows: (1) history of invasive craniocerebral surgery; (2) mental illness, including Alzheimer’s disease or schizophrenia; (3) history of traumatic brain injury; (4) neurological diseases, such as ischemic or hemorrhagic stroke; (5) long-term use of antiepileptic or antipsychotic drugs; (6) chronic alcoholism; and (7) history of acute cardiovascular and cerebrovascular disease, trauma, surgery, acute infection, or other stresses experienced within the past one month. The institutional review board of the hospital approved this study and written informed consent was obtained from the patients after explaining the purpose of the study.
Data collection and variable definition
All data was collected from self-questionnaires, interviews, and medical records, and a total of 23 factors were considered, including sex (male, female), age (< 55.0, 55.0–64.0, 65.0–74.0, ≥ 75.0 years), body mass index (BMI: < 20.0, 20.0–25.0, ≥ 25.0 kg/m2), weight gain proportion (0–5.0%, ≥ 5.0%), duration of dialysis (0–5.0, ≥ 5.0 years), hypertension (yes, no), diabetes mellitus (DM: yes, no), cardiovascular disease (CVD: yes, no), smoking (yes, no), insomnia (yes, no), hemoglobin (low: < 110 g/L; normal:110–130 g/L), albumin (low: < 35.0 g/L; normal:35.0–51.0 g/L), blood urea nitrogen (BUN, high: > 7.0 mmol/L; normal:3.2–7.1 mmol/L), uric acid (high: ≥ 420 umol/L for male and ≥ 360 umol/L for female; normal:180–420 umol/L for male and 120–360 umol/L for female), triglyceride (TG, high: > 1.21 mmol/L; normal:0.20–1.21 mmol/L), total cholesterol (TC, low: < 2.86 mmol/L; normal:2.86–5.98 mmol/L), high density lipoprotein (HDL, low: < 1.08 mmol/L; normal:1.08–1.91 mmol/L), low density lipoprotein (LDL, high: > 3.37 mmol/L; normal: ≤ 3.37 mmol/L), high-sensitive C-reaction protein (hs-CRP, high: > 0.88; normal:0.68–0.88), parathyroid hormone (PTH, high: > 300 pg/mL; normal:150–300 pg/mL), vitamin D (high: > 150.0 nmol/L; normal:50.0-150.0 nmol/L; low: < 50.0 nmol/L), spKt/V (normal: ≥ 1.2; low: < 1.2), alkaline phosphatase (ALP, high: > 120 U/L for male and > 130 U/L for female; normal:45–120 U/L for male and 50–130 U/L for female; low: < 45 U/L for male and < 50 U/L for female), and ferritin (high: > 500.0 ug/L; normal:200–500.0 ug/L; low: < 200 ug/L). Data collection was performed by a clinician and a nurse after training.
Cognitive impairment
The Montreal Cognitive Assessment (MoCA) was applied to assess cognitive function. The MoCA is a 30-point screening tool which takes patients approximately 10 min to complete [22,23,24]. Multiple domains are identified in the MoCA, including memory, visuospatial abilities, executive function, language, attention, concentration, working memory, and orientation to time and place. This cognitive function assessment was administered in a quiet room by medical staff who had been trained by psychologists. MoCA scores are adjusted for educational level, and an additional score should be added to the total score for patients with ≤ 12 years of formal education. The MoCA score system ranges from to 0–31, and the presence of cognitive impairment is determined at scores < 26 [22].
Statistical analysis
The characteristics of patients with and without cognitive impairment were collected as categorical and continuous data, presented as frequencies (proportions) and medians (interquartile ranges), respectively. The differences between groups was assessed using the Kruskal-Wallis method for continuous data, while the Chi-square or Fisher’s test was applied to assess differences in categorical data. Potential predictive factors were identified using univariate logistic regression analysis, and the factors were subjected to multivariate analyses using α = 0.05 and β = 0.10. Multivariate logistic regression was conducted to explore the predictive factors for cognitive impairment after adjusting for potential confounding factors. The weight of evidence was obtained from the regression coefficients for specific factors that were used to construct a categorical risk-scoring system. The numbers rounded to the nearest unit was applied as scoring values. Subsequently, a prediction model was constructed by combining predictive factors, and the predictive value was assessed using the receiver operating characteristic (ROC) curve with the area under the curve (AUC). Statistical significance was defined as a two-tailed P < 0.05. All statistical analyses were performed using SPSS Version 18 for Windows (SPSS Inc., Chicago, IL, USA).
Results
Baseline characteristics of included patients
Of the 146 included patients (96 male and 50 female), 46 patients presented with cognitive impairment (a prevalence of 31.5%). The median age of the patients was 56.0 years. The baseline characteristics of the participants are shown in Table 1. There were significant differences between patients with and without cognitive impairment for the following factors: age (P < 0.001), cardiovascular disease (P = 0.006), low vitamin D level (P = 0.036), and ferritin (P = 0.002). No significant differences were found between groups for: sex, BMI, weight gain, duration of dialysis, hypertension, DM, smoking, insomnia, hemoglobin, albumin, BUN, uric acid, TG, TC, HDL, LDL, hs-CRP, PTH, spKt/V, and ALP.
Multivariate analysis
Multivariate stepwise logistic regression was performed after adjusting for potential confounding factors, and the results are shown in Table 2. The following factors were associated with an increased risk of cognitive impairment in ESRD patients undergoing MHD: aged 55.0–64.0 years (OR:6.24; P = 0.001), aged 65.0–74.0 years (OR:16.10; P < 0.001), aged ≥ 75.0 years (OR:90.22; P < 0.001), duration of dialysis ≥ 5 years (OR:3.99; P = 0.003), and current smoker (OR:4.61; P = 0.009). Subsequently, the above factors were combined to construct the prediction model, and the ROC curve was drawn, with an AUC of 84% (95%CI: 77-91%) (Fig. 1).

Receiver operating characteristic curve for the risk of cognitive impairment in ESRD patients undergoing MHD, including the 3-component risk factor model
Risk scoring system
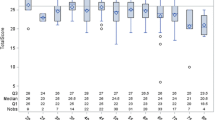
The risk scoring system was established on the basis of a multivariate logistic regression model, and cognitive impairment risk according to four categories is shown in Fig. 2. The number of patients in 1st, 2nd, 3rd, and 4th categories was 20, 49, 28, and 49, respectively, and the prevalence of cognitive impairment was 0% (95%CI:0-17%), 10% (95%CI:3-22%), 32% (95%CI:16-52%), and 65% (95%CI:50-78%), respectively.

Probability of developing cognitive impairment for patients at specific-risk category
Discussion
The current study is the first to construct a multifactorial predictive model for the risk of cognitive impairment in ESRD patients undergoing MHD which can be used as a predictive tool for identifying patients at high risk of cognitive impairment. Consequently, preventive strategies could be used to adjust modifiable risk factors and improve prognosis. A total of 146 patients with ESRD undergoing MHD were identified, and the prevalence of cognitive impairment was 31.5%. The prediction model was constructed based on age, dialysis duration, and smoking status, and the predictive value of the constructed model was high.
The prevalence of cognitive impairment found in this study is consistent with prior studies, which observed cognitive impairment in 30-80% of patients undergoing hemodialysis [9, 25, 26]. In our study, patients with a history of mental illness or neurological disease were excluded, which could partly explain the comparatively lower incidence of cognitive impairment in patients undergoing MHD.
Studies have demonstrated that CKD is associated with an increased risk of cerebrovascular disease, which can in turn induce cognitive impairment [27]. Moreover, cerebral perfusion pressure is related to a decrease in blood flow velocity due to a sharp decrease in blood volume in blood vessels caused by dialysis dehydration, which can cause a decline in cognitive function [28]. Furthermore, repeated cyclic stress of hemodialysis can lead to ischemic brain injury owing to the repeated decrease in cerebral blood flow during hemodialysis, which could induce an accelerated decline in cognitive function [29].
Several studies have identified risk factors for cognitive impairment in patients undergoing hemodialysis [19,20,21]. Drew et al. studied 314 older patients and identified age as the only significant risk factor affecting the rate of executive function decline [19]. Odagiri et al. studied 154 hemodialysis patients and 852 participants from the general population, and found that age and hemodialysis were significantly associated with an increased risk of cognitive impairment [20]. Karakizlis et al. prospectively collected 408 patients and found that sex, hemoglobin level, depression, and smoking could affect the progression of cognitive impairment in patients undergoing hemodialysis [21]. Our study identified risk factors for cognitive impairment, including age, duration of dialysis, and smoking status. Several considerations could explain these results: (1) Older patients have a higher prevalence of cardiovascular risk factors, which are, in turn, stronger risk factors for cognitive impairment [21]. Moreover, aging is related to changes in the brain which could affect cognitive function, including general atrophy (particularly in the hippocampus), imbalance of amyloid-β production and degradation, inflammatory response, and frailty of neurons, [30]. Furthermore, the neuronal metabolism, function and survival could affected by aging, which contributed an important role on the progression of cognitive declie and neurodegenerative diseases [31, 32]; (2) The duration of dialysis is significantly related to the severity of ESRD and kidney function, and cognitive impairment may occur prior to kidney failure [7]. (3) Cigarette smoking could accelerate brain aging, and metals in cigarette smoke could accumulate in tissues and fluids, causing heavy metal toxicity and promoting cognitive impairment [33,34,35,36].
Our study constructed a prediction model for cognitive impairment in patients with ESRD undergoing MHD, and the three risk factors were combined. The AUC of the constructed model was 84% (95%CI:77-91%), which suggests a high predictive value for cognitive impairment. Moreover, a risk scoring system was established, and the prevalence of cognitive impairment was estimated as 0%, 10%, 32%, and 65%. Thus, patients at high risk for cognitive impairment should be carefully monitored, and prevention and early treatment strategies should be applied to prevent the risk of cognitive impairment and improve the prognosis.
Several limitations of this study should be acknowledged. First, it was designed using a retrospective cohort, and the results could be affected by various confounding factors. Second, the severity of ESRD was not addressed, which might have affected the prevalence of cognitive impairment. Third, cognitive impairment contains various domains, which should be further analyzed to determine the potential impacts of MHD. Fourth, the analysis was based on a small sample size, and the constructed model lacked external validation.
Conclusions
Our study constructed a predictive model for cognitive impairment in ESRD patients undergoing MHD. A total of three factors were identified and subjected to the prediction model, including age, duration of dialysis, and smoking status, and the predictive value of the constructed model was high. Thus, the current prediction model should be applied in clinical practice and further large-scale prospective cohort studies should be performed to validate the predictive value of the constructed model.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Stevens LA, Li S, Wang C, et al. Prevalence of CKD and comorbid illness in elderly patients in the United States: results from the kidney early evaluation program (KEEP). Am J Kidney Dis. 2010;55:23–S33.
Cepoi V, Onofriescu M, Segall L, Covic A. The prevalence of chronic kidney disease in the general population in Romania: a study on 60,000 persons. Int Urol Nephrol. 2012;44:213–20.
Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association councils on kidney in Cardiovascular Disease, high blood pressure research, clinical cardiology, and Epidemiology and Prevention. Hypertension. 2003;42:1050–65.
Wilhelm-Leen ER, Hall YN, Tamura K. Frailty and chronic kidney disease: the Third National Health and Nutrition evaluation survey. Am J Med. 2009;122:664–671e2.
Walker SR, Wagner M, Tangri N. Chronic kidney disease, frailty, and unsuccessful aging: a review. J Ren Nutr. 2014;24:364–70.
Kurella Tamura M, Wadley V, Yaffe K, et al. Kidney function and cognitive impairment in US adults: the reasons for Geographic and racial differences in stroke (REGARDS) study. Am J Kidney Dis. 2008;52:227–34.
Yaffe K, Ackerson L, Tamura MK, et al. Chronic kidney disease and cognitive function in older adults: findings from the chronic renal insufficiency cohort (CRIC) cognitive study. J Am Geriatr Soc. 2010;58:338–45.
Darsie B, Shlipak MG, Sarnak MJ, et al. Kidney function and cognitive health in older adults: the Cardiovascular Health Study. Am J Epidemiol. 2014;180:68–75.
Dasgupta I, Patel M, Mohammed N, et al. Cognitive function declines significantly during haemodialysis in a majority of patients: a call for further research. Blood Purif. 2018;45:347–55.
van Zwieten A, Wong G, Ruospo M, et al. Prevalence and patterns of cognitive impairment in adult hemodialysis patients: the COGNITIVE-HD study. Nephrol Dial Transplant. 2018;33:1197–206.
Alosaimi FD, Asiri M, Alsuwayt S, et al. Psychosocial predictors of nonadherence to medical management among patients on maintenance dialysis. Int J Nephrol Renovascular Dis. 2016;9:263–72.
Li P, Ding D, Ma X, et al. Altered intrinsic brain activity and memory performance improvement in patients with end-stage renal disease during a single dialysis session. Brain Imag Behav. 2018;12:1640–9.
Angermann S, Schier J, Baumann M, et al. Cognitive impairment is associated with mortality in hemodialysis patients. J Alzheimer’s Dis. 2018;66:1529–37.
Prohovnik I, Post J, Uribarri J, et al. Cerebrovascular effects of hemodialysis in chronic kidney disease. J Cereb Blood Flow Metab. 2007;27:1861–9.
Mizumasa T, Hirakata H, Yoshimitu T, et al. Dialysis-related hypotension as a cause of progressive frontal lobe atrophy in chronic hemodialysis patients: a 3-year prospective study. Nephron Clin Pract. 2004;97:c23–c30.
Rakowski DA, Caillard S, Agodoa LY, et al. Dementia as a predictor of mortality in dialysis patients. Clin J Am Soc Nephrol. 2006;1:1000–5.
Kurella M, Mapes DL, Port FK, et al. Correlates and outcomes of dementia among dialysis patients: the dialysis outcomes and practice patterns study. Nephrol Dial Transplant. 2006;21:2543–8.
Dahbour SS, Wahbeh AM, Hamdan MZ. Mini mental status examination (MMSE) in stable chronic renal failure patients on hemodialysis: the effects of hemodialysis on the MMSE score. A prospective study. Hemodial Int. 2009;13:80–5.
Drew DA, Weiner DE, Tighiouart H, et al. Cognitive decline and its risk factors in prevalent hemodialysis patients. Am J Kidney Dis. 2017;69:780–7.
Odagiri G, Sugawara N, Kikuchi A, et al. Cognitive function among hemodialysis patients in Japan. Ann Gen Psychiatry. 2011;10:20.
Karakizlis H, Bohl K, Ziemek J, et al. Assessment of cognitive impairment and related risk factors in hemodialysis patients. J Nephrol. 2022;35:931–42.
Nasreddine ZS, Phillips NA, Bedirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53:695–9.
Chen S, Honda T, Narazaki K, et al. Global cognitive performance and frailty in non-demented community-dwelling older adults: findings from the Sasaguri Genkimon Study. Geriatr Gerontol Int. 2016;16:729–36.
Tiffin-Richards FE, Costa AS, Holschbach B, et al. The Montreal Cognitive Assessment (MoCA)- a sensitive screening instrument for detecting cognitive impairment in chronic hemodialysis patients. PLoS ONE. 2014;9:e106700.
van Zwieten A, Wong G, Ruospo M, et al. Associations of cognitive function and education level with all-cause mortality in adults on Hemodialysis: findings from the COGNITIVE-HD study. Am J Kidney Dis. 2019;74:452–62.
Findlay MD, Dawson J, Dickie DA, et al. Investigating the relationship between cerebral blood Flow and cognitive function in Hemodialysis Patients. J Am Soc Nephrol. 2019;30:147–58.
Drew DA, Weiner DE, Sarnak MJ. Cognitive impairment in CKD: Pathophysiology, Management, and Prevention. Am J Kidney Dis. 2019;74:782–90.
Ishida I, Hirakata H, Sugimori H, et al. Hemodialysis causes severe orthostatic reduction in cerebral blood flow velocity in diabetic patients. Am J Kidney Dis. 1999;34:1096–104.
Polinder-Bos HA, García DV, Kuipers J, et al. Hemodialysis induces an Acute decline in cerebral blood Flow in Elderly Patients. J Am Soc Nephrol. 2018;29:1317–25.
Xia X, Jiang Q, McDermott J, et al. Aging and Alzheimer’s disease: comparison and associations from molecular to system level. Aging Cell. 2018;17:e12802.
Hou Y, Dan X, Babbar M, et al. Ageing as a risk factor for neurodegenerative disease. Nat Rev Neurol. 2019;15:565–81.
López-Otín C, Blasco MA, Partridge L, et al. The hallmarks of aging. Cell. 2013;153:1194–217.
Ho YS, Yang X, Yeung SC, et al. Cigarette smoking accelerated brain aging and induced pre-alzheimer-like neuropathology in rats. PLoS ONE. 2012;7:e36752.
Saffari A, Daher N, Ruprecht A, et al. Particulate metals and organic compounds from electronic and tobacco-containing cigarettes: comparison of emission rates and secondhand exposure. Environ Sci Process Impacts. 2014;16:2259–67.
Huat TJ, Camats-Perna J, Newcombe EA, et al. Metal toxicity links to Alzheimer’s disease and neuroinflammation. J Mol Biol. 2019;431:1843–68.
Pamphlett R, Mak R, Lee J, et al. Concentrations of toxic metals and essential trace elements vary among individual neurons in the human locus ceruleus. PLoS ONE. 2020;15:e0233300.
Acknowledgements
Not applicable.
Funding
The author(s) received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
D Chen and X Li mainly participated in literature search, study design, writing and critical revision. C Xiao, W Xiao, L Lou and Z Gao mainly participated in data collection, data analysis and data interpretation. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Air Force Medical Center, PLA(2023-04-PJ01), all methods were performed in accordance with the Declarations of Helsinki and written informed consent was obtained from the patients after explaining the purpose of the study.
Consent for publication
Not applicable.
Disclosure of conflict of interest
The authors declared that there was no conflict of interest associated with the manuscript.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, D., Xiao, C., Xiao, W. et al. Prediction model for cognitive impairment in maintenance hemodialysis patients. BMC Neurol 23, 367 (2023). https://doi.org/10.1186/s12883-023-03407-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-023-03407-z