
Abstract
Background
The study investigated whether specific ultrasonographically observed endometrial features (including endometrium type and thickness) were linked to ectopic pregnancy after stimulated cycles with fresh embryo transfer.
Method
Of 6246 pregnancy cycles after fresh embryo transfer, 6076 resulted in intrauterine pregnancy and 170 in ectopic pregnancy. The primary outcome of the study was ectopic pregnancy, with the main variables being endometrium type and endometrial thickness. Univariate and subsequent multiple-stepwise logistic regression analyses were used to identify the risk factors of ectopic pregnancy.
Results
1. Compared with patients with an endometrial thickness ≥ 8 mm, the adjusted odds ratio for those with an endometrial thickness < 8 mm was 3.368 (P < 0.001). The adjusted odds ratio for women with a type-C endometrium was 1.897 (P = 0.019) compared with non-type C. 2. A larger dose of gonadotropin used during controlled ovarian hyperstimulation was a protective factor against ectopic pregnancy (P = 0.008). 3. The GnRH antagonist protocol (P = 0.007) was a risk factor for ectopic pregnancy, compared with the use of GnRH agonists.
Conclusion
(1) An endometrial thickness < 8 mm coupled with a type C endometrium significantly increased the risk of ectopic pregnancy after fresh embryo transfer. (2) A thin endometrial thickness and a type C endometrium could be further related to an abnormal endometrial receptivity/peristaltic wave. (3) Patients at a high risk of ectopic pregnancy should therefore be given special attention, with early diagnosis during the peri-transplantation period may assist in the prevention of ectopic pregnancy.
Similar content being viewed by others


Introduction
Ectopic pregnancy (EP) is an anomalous form of pregnancy whereby the embryo is implanted outside the uterine cavity [1]. In developing countries, 1% of maternal deaths can be attributed to this condition, with the figures rising to as high as 5% for developed countries [2]. Thus, EP can represent a significant social and economic burden.
Although Assisted Reproductive Technology (ART) should theoretically reduce the incidence of EP as the fallopian tubes are not involved in fertilization or embryo transfer (ET), it occurs in about 1–2% of spontaneous pregnancies [3] and up to 1.4–5.4% in ART [4, 5]. The risk factors of EP after ART include tubal factor infertility (TFI) [6,7,8,9,10,11], multiple embryos per transfer, [6] and fresh embryo transfer in stimulated cycles in comparison to thawed embryo transfer cycles [12,13,14,15,16,17].
During controlled ovarian stimulation (COS), ultrasound is routinely used to monitor the endometrial thickness (EMT) as well as the type of endometrium, with some studies suggesting that the thicker the EMT, the lower the incidence of EP [18,19,20]. However, to date, no studies have taken the endometrium type into account nor considered possible correlations between combined endometrial features and EP after ART. Furthermore, while previous studies were specifically focused on frozen embryo transfer cycles [18] or undertook a mixed analysis of both fresh and frozen embryo cycles [19, 20], none have analyzed fresh embryo transfers separately. Thus, the main aim of the current work was to investigate whether the endometrium type as well as EMT were related to EP occurrence, especially after stimulated cycles involving fresh embryo transfer.
Methods
Definition of clinical outcomes
The blood β-human chorionic gonadotropin (β-hCG) levels were examined 12 days after ET In this case, they were considered to be negative or positive when their β-hCG levels were respectively below 5 IU/L or above 15 IU/L. Some patients were also considered as indeterminate when their β-hCG amounts were between 5 and 15 IU/L but they were subsequently deemed to be positive if the levels increased after 48 h. All positive women underwent sonography 4–5 weeks after ET.
The possible outcomes encountered after ET included intrauterine pregnancy (IUP), indicating the presence of one or more intrauterine gestational sacs, and EP, defined as the presence of a gestational sac/mass outside the uterine cavity. In contrast, heterotopic pregnancy (HP) was diagnosed when intrauterine gestational sacs and ectopic pregnancy were observed simultaneously.
Study design and patients
This study was performed in accordance with the ethical guidelines of the Declaration of Helsinki, revised in 1983. The participants were recruited from patients who had undergone stimulated cycles with fresh embryo transfer at the Reproductive Medicine Centre of Xiangya Hospital, Central South University, Changsha, China, between January 2014 and November 2021. Patients were examined by sonography at different stages of their menstrual cycles at least twice before the ART procedure. They were then further examined by hysteroscopy and treated when cavity abnormalities were observed.
Clinical information was acquired from the medical records. Patients with the following conditions were excluded: (1) cryopreserved embryos; (2) biochemical pregnancy; (3) heterotopic pregnancy; (4) cesarean scar pregnancy; (5) absence of endometrial data; (6) uterine anomaly; (7) donor oocytes cycles; (8) non-pregnant cycles.
EP was the main outcome examined while the main variables were endometrial type and EMT. Demographic data included age, parity, gravidity, etiology of infertility, infertility duration (years), ovarian stimulation protocol, number of embryo(s) per transfer, number of oocytes retrieved, duration of gonadotrophin (Gn) (days), total Gn dose (IU), method of insemination, basal FSH, and body mass index (BMI) as evaluated by the patient’s doctor in charge. Patients were diagnosed with tubal factor infertility (TFI) if any of the following was noted: hydrosalpinx, previous salpingectomy, previous EP, or tubal scarring, including occlusion. In addition, patients with any two of the following conditions were diagnosed with polycystic ovary syndrome (PCOS): clinical and/or biochemical hyperandrogenism, ovulatory dysfunction, and PCOM (polycystic ovary morphology). Finally, women were considered as presenting diminished ovarian reserve (DOR) if the results of their ovarian reserve test were abnormal (i.e., anti-Mullerian hormone (AMH) < 0.5–1.1 ng/ml or antral follicular count (AFC) < 5–7 follicles), or if any of the risk factors of poor ovarian response (POR) was observed. The follow-up rate in the study was 100%.
Ultrasound measurement
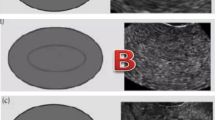
EMT and endometrium type were assessed on the day of HCG injection (trigger day) by transvaginal 8 MHz ultrasonography with Doppler ultrasound (GE Voluson E10, USA). As described by Bredella et al. [21], the EMT was measured by transvaginal sonography, along a sagittal plane and with the maximal anteroposterior thickness used. The morphology of the endometrium was classified into one of three types: type A, with a trilaminar pattern (a triple-line pattern), consisting of outer, hyperechoic middle and hypoechoic inner layers as well as evident echoes at the intrauterine center line; type B, having a relatively homogeneous hyperechoic endometrium, with an obscure intrauterine center line echo and unclear endometrial layers but with clear interfaces between the endometrium and muscular layers; type C, having homogeneous hyperechoic endometrium without an intrauterine center-line echo.
Procedure for inducing ovulation and IVF/ICSI-embryo transfer
The protocols selected for stimulation were tailored to each individual and have been described thoroughly in previous publications [22, 23]. Ovarian stimulation was initiated at the basal state of the ovaries [24] and was performed using human menopausal gonadotrophin (Lebaode) and/or exogenous highly purified follicle-stimulating hormone (FSH, Lishenbao). The starting dose of gonadotrophin (Gn), in this case, ranged from 112.5 to 300 IU, depending on the age of the patient, antral follicular counts (AFC), and basal FSH level (bFSH). HCG (6000-10 000 IU; Profasi; Serono, Italy) was then injected when at least two follicles reached ≥ 18 mm in diameter, with oocytes subsequently retrieved 36 h after the trigger. This was followed by routine in vitro fertilization (IVF)/ intracytoplasmic sperm injection (ICSI) before transferring a maximum of three high-quality embryos with a Cook catheter under transabdominal ultrasound guidance following the standard procedures of our center 72 h after oocyte retrieval. The luteal phase was eventually supported by vaginal micronized progesterone (Utrogestan) using a dose of 200 mg, three times a day, along with oral progesterone capsules (Qining) at a dose of 200 mg once a day, with both treatments simultaneously starting since the day of oocyte retrieval and lasting for 75 days.
Statistics
Variables were selected based on previous studies [25,26,27] and data availability.
SPSS version 23 (IBM, USA) was used for data analysis. For quantitative data, results are presented as mean ± standard deviation (SD) or median (interquartile range) for normally and non-normally distributed data, respectively. Categorical data are presented as the number of cases (percentage).
Univariate analysis was performed using the Pearson Chi-square test for categorical variables, while two-sample t-tests and Mann-Whitney U tests were used where appropriate. Lastly, the independent risk factors for EP were identified based on stepwise multiple logistic regression analysis. Overall, differences were considered statistically significant at P < 0.05.
Results
The cycle selection process used to obtain the final study sample is shown in Fig. 1. The study included 6246 IVF cycles of which 6076 were IUP and 170 were EP cycles.

Flow chart of patients
Single-factor analysis
Table 1 shows the baseline characteristics of the patients together with the ovarian responses. There were no significant differences between patients in terms of BMI, age, previous history of ectopic pregnancy, infertility duration, type of infertility, gravidity, bFSH, duration of Gn, number of oocytes retrieved, and number of embryo(s) per transfer. However, significant differences were observed in terms of the method of insemination, total Gn dose, and ovarian stimulation protocol, as well as the presence or absence of TFI, male factor infertility, and PCOS (P < 0.05).
Compared with IUP patients, patients with EP had significantly thinner EMTs (P < 0.001). Furthermore, the prevalence of EP was significantly higher in women with an EMT < 8 mm (8.4%) compared with those with an EMT of ≥ 8 mm (2.4%) (P < 0.001). At the same time, those with a type C endometrium were significantly more likely to have EP than those with type A or B endometria (5.1% v 2.2% v 2.9%, P = 0.007).
Univariate regression analysis
The univariate analysis showed that for women with an EMT of < 8 mm, the risk of EP was over three times greater than for those with an EMT ≥ 8 mm (OR 3.713; 95% CI 2.421–5.694; P < 0.001). Moreover, the presence of type C endometrium led to a twofold increase in the EP risk compared with non-type C endometria (OR 2.020; 95% CI 1.191–3.424; P = 0.009). The results are summarized in Table 2.
Multivariate stepwise regression analysis
Variables showing P-values < 0.1 in the univariate analysis were subsequently included in the multivariate stepwise regression analysis, with the results provided in Table 3.
After adjusting for confounders, the risk of EP increased more than twofold for women with an EMT of < 8 mm in comparison with those with an EMT of ≥ 8 mm (aOR 3.368; 95% CI 2.184–5.196; P < 0.001). Consistent with the univariate analysis, patients with type C endometria still had a nearly twofold risk of having EP (aOR 1.897; 95% CI 1.110–3.242; P = 0.019) relative to non-type C endometria.
The use of antagonist protocols (aOR 1.748; 95% CI 1.162–2.628; P = 0.007) and TFI (aOR 2.139; 95% CI 1.083–4.225; P = 0.029) were also identified as risk factors. On the other hand, a larger dose of total gonadotrophin (aOR 0.999; 95% CI 0.999-1.000; P = 0.008) was protective against EP.
Discussion
To date, this study represents the first and largest retrospective investigation into the influence of combined endometrial features, namely, the endometrium type and EMT, on the risk of EP after fresh embryo transfer. The results indicated that the risk factors for EP were a thin type C endometrium, with TFI, a smaller Gn dose, and the use of a GnRH antagonist protocol being additional risk factors for EP.
Several studies [18,19,20, 28] have suggested that the presence of a thinner EMT before embryo transfer was more likely to induce EP. However, these studies focused only on freeze-thaw embryo transfer (FET) cycles [18] or confused the use of fresh embryos with FET [19, 20]. Another common feature of previous studies is the absence of information on the endometrial type when investigating EMT. Several researchers have also suggested that the incidence of EP in frozen or donor cycles without ovarian hyperstimulation was lower compared with fresh autologous cycles, thus suggesting that differences in the tubal-uterine environment between cycles contributed to abnormal implantation following embryo transfer [17]. Therefore, the current authors believe that fresh embryo transfer cycles should be analyzed separately.
Consistent with previous studies [6, 7, 9, 18, 19, 26, 29, 30], TFI increased the risk of EP more than twofold. In terms of multiple-embryo transfer, while some studies [18, 20, 26] considered it a risk factor for EP, another [19] suggested that it had no impact. The latter conclusion was supported by the results of the current work, although this could be attributed to the relatively small fraction (728/6246) of the women to whom a single embryo was transferred. Gravidity [18] and previous history of EP [19, 31] represented a similar situation.
Consistent with previous studies, infertility duration [19], method of insemination [18], bFSH [19], BMI [18, 19, 32], infertility type [19], number of oocytes retrieved [19], duration of Gn (days) [19], and age [18, 19] were not found to be risk factors for EP, although one study [20] suggested that age and BMI could independently influence the occurrence of EP. However, unlike the findings of a previous study [19], the current study found a higher Gn dosage to be a protective factor against EP. Furthermore, one study [33] found that the COS cycle was associated with higher uterine peristalsis compared with the natural cycle, with waves mostly moving from the cervix to the fundus. Even at a high level of progesterone, the intensity of the waves did not decrease to natural levels before embryo transfer. Thus, it is evident that COS influences endometrial motility, although the relationship between the Gn dosage and the frequency/direction of endometrial peristalsis wave is yet to be studied.
The risk of EP was found to be higher in when using the GnRH antagonist protocol compared with the GnRH agonist protocol. This result is consistent with previous studies [17, 20], indicating that the incidence of EP can be influenced by the selected protocol.
The present study showed that an EMT of < 8 mm increased the risk of EP more than twofold in comparison with an EMT of ≥ 8 mm. Previous studies [18, 19] have shown a link between thinner EMT and higher EP risk, with one study [18] even reporting an increased EP risk with an EMT of < 12 mm in the frozen embryo cycle. Similarly, a different investigation showed that EP patients had thinner EMTs after a positive pregnancy test [34].
It remains unclear why patients with a thin EMT have a higher risk of EP. This could partly be due to an abnormally high oxygen tension which is known to be detrimental to embryonic development due to the production of reactive oxygen species [35,36,37]. As published by Bartelmez [35], the blood vessels in the endometrium’s basal layer are large spiral arteries, while those in the functional layer are capillaries. Thus, unlike the usual low oxygen tension seen at the endometrial surface, the high oxygen content close to the basal layer could create unfavorable conditions for embryo development. This is because a thin EMT causes the embryo to be much closer to the basal endometrium layer’s spiral arteries, exposing it to higher concentrations of reactive oxygen species. However, in this case, the fallopian tube’s lower oxygen concentration could be more suitable for embryo implantation [38].
Another possible mechanism that could link EP to thin EMT is uterine peristalsis. It has been reported that compared with IUP, the uterine peristaltic wave frequency is increased in patients with EP, although the differences were not significant [39] due to the uneven distribution of the sample size. Patients with a thicker EMT were also reported to have an increased risk of placenta previa [40], and as such, the authors postulated that higher EMT was associated with uterine peristalsis that affected embryo implantation sites. Although the results of the above two studies appear contradictory, it should be noted that neither considered the type and direction of the uterine peristaltic wave, as both factors are important in the assessment of uterine activity [33, 41]. Indeed, embryos can be removed from their original transfer site [42] if the peristaltic waves occur from the fundus to the cervix [33, 39, 43], resulting in the movement of a transferred embryo in an inferior direction that increases the possibility of placenta previa. In contrast, if the waves are in the opposite direction, this may increase the likelihood of EP [39, 44, 45].
A third possible explanation could be endometrial receptivity. Many studies have shown that EMT is associated with uterine receptivity [46,47,48,49,50,51]. In fact, compared with endometria of normal thickness, thin endometria area reported to contain different amounts of cytokines. At the same time, many genes which are related to anti-oxidative stress and metabolism were found to be down-regulated [52]. Currently, there are many criteria for diagnosing endometrial receptivity, including several molecular diagnostic models [53], and thus the associations between EMT characteristics and endometrial receptivity require further investigation.
The other arguably most important finding of the current study was that a type C endometrium increased the risk of EP nearly twofold. The hyperechoic middle line is usually assumed to represent the uterine cavity, with the other two considered to be the junction between the endometrium and myometrium. However, the mechanism of hyperechoic endometrium imaging remains disputable. In this context, Fleischer et al. [54] suggested that, during the late secretory phase, a homogeneous hyperechoic endometrium could indicate a stromal edema [55], referred to as endometrial decidualization when sex hormones cause the endometrium to change from the proliferative phase to a secretory one. The absence of decidualization is related to infertility and recurrent spontaneous abortion (RSA). Some researchers further believe that a premature endometrium secretory pattern is bad for pregnancy [56], while Friedler [57] considered that the type of endometrium could provide valuable predictive information regarding pregnancy. Based on the above, the current authors believe that a type C endometrium could be related to a shift in the embryo implantation window due to early endometrial transformation. Therefore, patients with a type-C endometrium, along with an EMT of < 8 mm on trigger day should be adequately counseled, and their endometrial peristaltic wave/receptivity should also be examined before transfer.
After COS, patients tend to have more frequent uterine peristaltic waves than during natural cycles [33]. However, to date, no study has reported an association between EMT and peristaltic wave frequency, nor between other indicators such as endometrium type and peristaltic wave direction.
The main strength of this work is that, for the first time, the influence of both endometrium type and EMT on EP frequency was determined. Furthermore, unlike previous studies, fresh cycles were studied separately from freeze-thaw transfers. Finally, several previous studies included HP in the EP group even though in HP, one of the embryos is normally implanted in the uterine cavity. Since endometrial characteristics affect EP occurrence, HP should be excluded.
Furthermore, this single study not only included a large sample size but both the EMT and endometrium type were assessed by the same trained sonographers. Similarly, the same trained embryologists cultured and evaluated all embryos. These practices reduced inter-observer and inter-center variations. Finally, almost all the embryos which were transferred during the fresh embryo cycles were of good quality (the fragmentation rates were < 20%) at the cleavage stage on day 3 in our reproductive center. This helped to overcome the influence of confounding factors such as the stage of embryonic development and embryo quality.
However, due to its retrospective design, this study was not without limitations. Confounders which are known [58] to affect pregnancy outcomes, namely, alcohol consumption, smoking, and risky sexual behaviors, were not included, as factors such as smoking and alcohol which could have negatively influenced pregnancy were consciously reduced by couples seeking IVF, thus these factors can be considered to have had little impact.
Conclusions
A type-C endometrium and a thin EMT were linked to a significantly higher risk of EP. Combining information on endometrium type and EMT could be a quantitative marker of uterine peristalsis or even of endometrial receptivity in fresh embryo cycles. Furthermore, patients at high risk of EP, especially if diagnosed with TFI and a thin EMT combined with a type C endometrium, should be further evaluated to determine whether the ET procedure should be carried forward. Finally, prior to ET, EP monitoring can be strengthened for high-risk groups, probably through endometrial peristaltic wave/receptivity examination, and this could be supplemented with medical treatments [59, 60] for controlling peristaltic waves to further prevent EP in high-risk populations.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
ACOG Practice Bulletin No. 191 Summary: Tubal ectopic pregnancy. Obstet Gynecol. 2018;131(2):409–11.
Khan K, Wojdyla D, Say L, Gülmezoglu A, Van Look P. WHO analysis of causes of maternal death: a systematic review. Lancet (London England). 2006;367(9516):1066–74.
Farquhar C. Ectopic pregnancy. Lancet (London England). 2005;366(9485):583–91.
Jurkovic D, Wilkinson H. Diagnosis and management of ectopic pregnancy. BMJ (Clinical research ed). 2011;342:d3397.
Muller V, Makhmadalieva M, Kogan I, Fedorova I, Lesik E, Komarova E, Dzhemlikhanova L, Niauri D, Gzgzyan A, Ailamazyan E. Ectopic pregnancy following in vitro fertilization: meta-analysis and single-center experience during 6 years. Gynecol endocrinology: official J Int Soc Gynecol Endocrinol. 2016;32:69–74.
Clayton H, Schieve L, Peterson H, Jamieson D, Reynolds M, Wright V. Ectopic pregnancy risk with assisted reproductive technology procedures. Obstet Gynecol. 2006;107(3):595–604.
Strandell A, Thorburn J, Hamberger L. Risk factors for ectopic pregnancy in assisted reproduction. Fertil Steril. 1999;71(2):282–6.
Pyrgiotis E, Sultan K, Neal G, Liu H, Grifo J, Rosenwaks Z. Ectopic pregnancies after in vitro fertilization and embryo transfer. J Assist Reprod Genet. 1994;11(2):79–84.
Malak M, Tawfeeq T, Holzer H, Tulandi T. Risk factors for ectopic pregnancy after in vitro fertilization treatment. J Obstet Gynecol Canada: JOGC = Journal d’obstetrique et gynecologie du Can : JOGC. 2011;33(6):617–9.
Kazandi M, Turan V. Ectopic pregnancy; risk factors and comparison of intervention success rates in tubal ectopic pregnancy. Clin Exp Obstet Gynecol. 2011;38(1):67–70.
Refaat B, Dalton E, Ledger W. Ectopic pregnancy secondary to in vitro fertilisation-embryo transfer: pathogenic mechanisms and management strategies. Reproductive biology and endocrinology: RB&E. 2015;13:30.
Huang B, Hu D, Qian K, Ai J, Li Y, Jin L, Zhu G, Zhang H. Is frozen embryo transfer cycle associated with a significantly lower incidence of ectopic pregnancy? An analysis of more than 30,000 cycles. Fertil Steril. 2014;102(5):1345–9.
Shapiro B, Daneshmand S, De Leon L, Garner F, Aguirre M, Hudson C. Frozen-thawed embryo transfer is associated with a significantly reduced incidence of ectopic pregnancy. Fertil Steril. 2012;98(6):1490–4.
Shapiro B, Daneshmand S, Garner F, Aguirre M, Hudson C, Thomas S. Evidence of impaired endometrial receptivity after ovarian stimulation for in vitro fertilization: a prospective randomized trial comparing fresh and frozen-thawed embryo transfer in normal responders. Fertil Steril. 2011;96(2):344–8.
Ishihara O, Kuwahara A, Saitoh H. Frozen-thawed blastocyst transfer reduces ectopic pregnancy risk: an analysis of single embryo transfer cycles in Japan. Fertil Steril. 2011;95(6):1966–9.
Polyzos N, Devroey P. Significantly lower ectopic pregnancy rates after frozen embryo transfer: implications toward segmentation of in vitro fertilization treatment. Fertil Steril. 2012;98(6):1419–20.
Londra L, Moreau C, Strobino D, Garcia J, Zacur H, Zhao Y. Ectopic pregnancy after in vitro fertilization: differences between fresh and frozen-thawed cycles. Fertil Steril. 2015;104(1):110–8.
Liu H, Zhang J, Wang B, Kuang Y. Effect of endometrial thickness on ectopic pregnancy in frozen embryo transfer cycles: an analysis including 17,244 pregnancy cycles. Fertil Steril. 2020;113(1):131–9.
Liu X, Qu P, Bai H, Shi W, Shi J. Endometrial thickness as a predictor of ectopic pregnancy in 1125 in vitro fertilization-embryo transfer cycles: a matched case-control study. Arch Gynecol Obstet. 2019;300(6):1797–803.
Rombauts L, McMaster R, Motteram C, Fernando S. Risk of ectopic pregnancy is linked to endometrial thickness in a retrospective cohort study of 8120 assisted reproduction technology cycles. Hum Reprod (Oxford England). 2015;30(12):2846–52.
Bredella M, Feldstein V, Filly R, Goldstein R, Callen P, Genant H. Measurement of endometrial thickness at US in multicenter drug trials: value of central quality assurance reading. Radiology. 2000;217(2):516–20.
Hou Z, Zhang Q, Zhao J, Xu A, He A, Huang X, Xie S, Fu J, Xiao L, Li Y. Value of endometrial echo pattern transformation after hCG trigger in predicting IVF pregnancy outcome: a prospective cohort study. Reproductive biology and endocrinology: RB&E. 2019;17(1):74.
Qiong Z, Jie H, Yonggang W, Bin X, Jing Z, Yanping L. Clinical validation of pinopode as a marker of endometrial receptivity: a randomized controlled trial. Fertil Steril. 2017;108(3):513–517e512.
Q JZ. Endometrial pattern, thickness and growth in predicting pregnancy outcome following 3319 IVF cycle. Reprod Biomed Online. 2014;29(3):291–8.
Chang H, Suh C. Ectopic pregnancy after assisted reproductive technology: what are the risk factors? Curr Opin Obst Gynecol. 2010;22(3):202–7.
Perkins K, Boulet S, Kissin D, Jamieson D. Risk of ectopic pregnancy associated with assisted reproductive technology in the United States, 2001–2011. Obstet Gynecol. 2015;125(1):70–8.
Li Z, Sullivan E, Chapman M, Farquhar C, Wang Y. Risk of ectopic pregnancy lowest with transfer of single frozen blastocyst. Hum Reprod (Oxford England). 2015;30(9):2048–54.
Fang T, Chen M, Yu W, Ma T, Su Z, Chan D, Zhao M, Zheng Q, Wang W. The predictive value of endometrial thickness in 3117 fresh IVF/ICSI cycles for ectopic pregnancy. J Gynecol Obstet Hum Reprod. 2021;50(8):102072.
Lesny P, Killick S, Robinson J, Maguiness S. Transcervical embryo transfer as a risk factor for ectopic pregnancy. Fertil Steril. 1999;72(2):305–9.
Ribic-Pucelj M, Tomazevic T, Vogler A, Meden-Vrtovec H. Risk factors for ectopic pregnancy after in vitro fertilization and embryo transfer. J Assist Reprod Genet. 1995;12(9):594–8.
Xu Z, Yan L, Liu W, Xu X, Li M, Ding L, Ma J, Chen Z. Effect of treatment of a previous ectopic pregnancy on in vitro fertilization-intracytoplasmic sperm injection outcomes: a retrospective cohort study. Fertil Steril. 2015;104(6):1446–1451e1441.
MacKenna A, Schwarze J, Crosby J, Zegers-Hochschild F. Outcome of assisted reproductive technology in overweight and obese women. JBRA Assist Reprod. 2017;21(2):79–83.
Zhu L, Li Y, Xu A. Influence of controlled ovarian hyperstimulation on uterine peristalsis in infertile women. Hum Reprod (Oxford England). 2012;27(9):2684–9.
Hammoud A, Hammoud I, Bujold E, Gonik B, Diamond M, Johnson S. The role of sonographic endometrial patterns and endometrial thickness in the differential diagnosis of ectopic pregnancy. Am J Obstet Gynecol. 2005;192(5):1370–5.
Casper R. It’s time to pay attention to the endometrium. Fertil Steril. 2011;96(3):519–21.
Yang H, Hwang K, Kwon H, Kim H, Choi K, Oh K. Detection of reactive oxygen species (ROS) and apoptosis in human fragmented embryos. Hum Reprod (Oxford England). 1998;13(4):998–1002.
Catt J, Henman M. Toxic effects of oxygen on human embryo development. Hum Reprod (Oxford England) 2000:199–206.
Bornside G, Donovan W, Myers M. Intracolonic tensions of oxygen and carbon dioxide in germfree, conventional, and gnotobiotic rats. Proc Soc Experimental Biology Med Soc Experimental Biology Med (New York NY). 1976;151(2):437–41.
Zhu L, Che H, Xiao L, Li Y. Uterine peristalsis before embryo transfer affects the chance of clinical pregnancy in fresh and frozen-thawed embryo transfer cycles. Hum Reprod (Oxford England). 2014;29(6):1238–43.
Rombauts L, Motteram C, Berkowitz E, Fernando S. Risk of placenta praevia is linked to endometrial thickness in a retrospective cohort study of 4537 singleton assisted reproduction technology births. Hum Reprod (Oxford England). 2014;29(12):2787–93.
IJland M, Evers J, Dunselman G, Volovics L, Hoogland H. Relation between endometrial wavelike activity and fecundability in spontaneous cycles. Fertil Steril. 1997;67(3):492–6.
Poindexter A, Thompson D, Gibbons W, Findley W, Dodson M, Young R. Residual embryos in failed embryo transfer. Fertil Steril. 1986;46(2):262–7.
Ijland M, Evers J, Dunselman G, van Katwijk C, Lo C, Hoogland H. Endometrial wavelike movements during the menstrual cycle. Fertil Steril. 1996;65(4):746–9.
Eytan O, Elad D. Analysis of intra-uterine fluid motion induced by uterine contractions. Bull Math Biol. 1999;61(2):221–38.
Bulletti C, de Ziegler D, Polli V, Diotallevi L, Del Ferro E, Flamigni C. Uterine contractility during the menstrual cycle. Hum Reprod (Oxford England) 2000:81–9.
McWilliams G, Frattarelli J. Changes in measured endometrial thickness predict in vitro fertilization success. Fertil Steril. 2007;88(1):74–81.
Amir W, Micha B, Ariel H, Liat L, Jehoshua D, Adrian S. Predicting factors for endometrial thickness during treatment with assisted reproductive technology. Fertil Steril. 2007;87(4):799–804.
Richter K, Bugge K, Bromer J, Levy M. Relationship between endometrial thickness and embryo implantation, based on 1,294 cycles of in vitro fertilization with transfer of two blastocyst-stage embryos. Fertil Steril. 2007;87(1):53–9.
Zhang X, Chen C, Confino E, Barnes R, Milad M, Kazer R. Increased endometrial thickness is associated with improved treatment outcome for selected patients undergoing in vitro fertilization-embryo transfer. Fertil Steril. 2005;83(2):336–40.
Zenke U, Chetkowski R. Transfer and uterine factors are the major recipient-related determinants of success with donor eggs. Fertil Steril. 2004;82(4):850–6.
Kovacs P, Matyas S, Boda K, Kaali S. The effect of endometrial thickness on IVF/ICSI outcome. Hum Reprod (Oxford England). 2003;18(11):2337–41.
Maekawa R, Taketani T, Mihara Y, Sato S, Okada M, Tamura I, Jozaki K, Kajimura T, Asada H, Tamura H, et al. Thin endometrium transcriptome analysis reveals a potential mechanism of implantation failure. Reproductive Med biology. 2017;16(2):206–27.
He A, Zou Y, Wan C, Zhao J, Zhang Q, Yao Z, Tian F, Wu H, Huang X, Fu J, et al. The role of transcriptomic biomarkers of endometrial receptivity in personalized embryo transfer for patients with repeated implantation failure. J translational Med. 2021;19(1):176.
Fleischer A, Kalemeris G, Entman S. Sonographic depiction of the endometrium during normal cycles. Ultrasound Med Biol. 1986;12(4):271–7.
Grunfeld L, Walker B, Bergh P, Sandler B, Hofmann G, Navot D. High-resolution endovaginal ultrasonography of the endometrium: a noninvasive test for endometrial adequacy. Obstet Gynecol. 1991;78(2):200–4.
Zhao J, Zhang Q, Li Y. The effect of endometrial thickness and pattern measured by ultrasonography on pregnancy outcomes during IVF-ET cycles. Reproductive biology and endocrinology: RB&E. 2012;10:100.
Friedler S, Schenker J, Herman A, Lewin A. The role of ultrasonography in the evaluation of endometrial receptivity following assisted reproductive treatments: a critical review. Hum Reprod Update. 1996;2(4):323–35.
Gaskins A, Missmer S, Rich-Edwards J, Williams P, Souter I, Chavarro J. Demographic, lifestyle, and reproductive risk factors for ectopic pregnancy. Fertil Steril. 2018;110(7):1328–37.
Xu A, Li Y, Zhu L, Tian T, Hao J, Zhao J, Zhang Q. Inhibition of endometrial fundocervical wave by phloroglucinol and the outcome of in vitro fertilization. Reprod Biol. 2013;13(1):88–91.
Buddhabunyakan N, Sothornwit J, Seejorn K, Buppasiri P, Salang L. Effects of atosiban on uterine peristalsis following frozen embryo transfer: a randomized controlled trial. Eur J Obstet Gynecol Reprod Biol. 2021;265:96–101.
Acknowledgements
The authors thank everyone in the department of Reproductive Medicine in the Xiangya Hospital of Central South University for their scientific advice and friendly help. This study was supported by the National Natural Science Foundation of China (grant no. 8187061497), the Key Project of Research and Development Plan in Hunan Province (2021SK2028), and the National Key Research and Development Program of China (2021YFC2700404).
Funding
This study was supported by the National Natural Science Foundation of China (grant no. 8187061497), the Key Project of Research and Development Plan in Hunan Province (2021SK2028), and the National Key Research and Development Program of China (2021YFC2700404).
Author information
Authors and Affiliations
Contributions
Yanping Li, Ying Zhao and Hongying Tang were contributed to the study conception and design. Material preparation, data collection and analysis were performed by Ying Zhao. The first draft of the manuscript was written by Ying Zhao. All authors commented on previous versions of the manuscript. All authors participated in data analysis and results discussion, reading and approving the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was performed by conforming to the ethical guidelines of the declaration of Helsinki, revised in 1983. Ethical approval was approved by the local Ethics Committee of Xiangya Hospital, Central South University (No. 2022003). For patients who receive ART (IVF/ICSI) treatment in our center, their medical records are allowed to be used for research. All patients received informed consent before ART treatment. All patients were registered in data management system, which is used to store all medical information about patients trying to conceive through ART.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhao, Y., Xu, A., Liu, D. et al. An endometrium of type C along with an endometrial thickness of < 8 mm are risk factors for ectopic pregnancy after stimulated cycles with fresh embryo transfer. BMC Pregnancy Childbirth 23, 713 (2023). https://doi.org/10.1186/s12884-023-05920-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-023-05920-y